Multisystem Autoimmune Disease | Jaccoud Arthropathy | Multifocal AVN | Perioperative Risk
- SLE arthritis is typically non-erosive but Jaccoud deformity produces reducible swan-neck / ulnar deviation
- AVN in SLE is commonly multifocal (30-50%) - image BOTH hips and knees when one site presents
- Highest AVN risk: cumulative prednisolone greater than 3-5 g, daily dose greater than 20 mg, pulse therapy, Raynaud, vasculitis, antiphospholipid antibodies
- Antiphospholipid syndrome (APS) raises perioperative thromboembolism risk - 10-15% of SLE patients
- Perioperative steroid cover and VTE prophylaxis are mandatory - even for arthroplasty in stable disease
- “Jaccoud = reducible; rheumatoid = fixed and erosive - the differential at the MCP/PIP
- “Multifocal AVN is a SLE signature: ask for MRI of contralateral joint when you see one AVN
- “Always check aPL antibodies (lupus anticoagulant, anti-cardiolipin, anti-beta2 GPI) before theatre
- “Capillaritis, Raynaud, livedo reticularis point to APS - screen for thrombosis history
- “Active lupus nephritis or CNS lupus markedly increases perioperative morbidity - defer elective surgery
Reducible ulnar deviation + swan-neck without bony erosion. Caused by capsuloligamentous laxity from chronic inflammation. Hand function often preserved despite dramatic deformity. Distinguish from RA: Jaccoud has no erosions on X-ray.
30-50% of SLE AVN is bilateral or multifocal. Always obtain MRI of the contralateral joint (most often contralateral hip, then knees, shoulders, talus). Cumulative steroid dose is the dominant modifiable risk factor.
10-15% of SLE patients have aPL antibodies. Triad: thrombosis (arterial/venous), pregnancy morbidity, thrombocytopenia. Perioperative VTE risk is markedly elevated. Bridging anticoagulation may be needed.
Stress-dose steroids for any patient on greater than 5 mg/day prednisolone within 12 months. Stop immunosuppressives (MMF, cyclophosphamide) pre-op. Defer elective surgery during active nephritis, CNS lupus, or severe cytopenia.
- SLE / Jaccoud
- Ulnar deviation, reducible
- Rheumatoid
- Ulnar deviation, fixed
- Key Discriminator
- Jaccoud corrects with passive movement
- SLE / Jaccoud
- Common, reducible
- Rheumatoid
- Common, often fixed
- Key Discriminator
- Jaccoud lacks erosions
- SLE / Jaccoud
- Absent (key)
- Rheumatoid
- Present early
- Key Discriminator
- MRI / ultrasound sensitive in RA
- SLE / Jaccoud
- Mild, often non-erosive
- Rheumatoid
- Marked, pannus, erosions
- Key Discriminator
- Power Doppler may be quiet in SLE
- SLE / Jaccoud
- Often preserved despite deformity
- Rheumatoid
- Loss of function tracks deformity
- Key Discriminator
- Jaccoud hand is more cosmetic than crippling
LACERJaccoud Arthropathy
Hook:Jaccoud LACERs the hand: laxity + reducible + no erosions - looks like RA, behaves like SLE.
STEROIDSLE AVN Risk Factors
Hook:AVN in SLE is driven by STEROIDs and microvascular thrombosis - protect the bone early.
SAFE ORTHOPerioperative SLE Checklist
Hook:Run through SAFE ORTHO before any SLE patient enters theatre.
Overview and Epidemiology
Musculoskeletal complaints are the most common reason a patient with SLE first presents to a clinician, and they remain the leading cause of morbidity through the disease course. The orthopaedic surgeon encounters SLE in three principal scenarios: a hand deformity that mimics rheumatoid arthritis (Jaccoud arthropathy), avascular necrosis of the femoral head in a young patient on steroids, and the perioperative management of an SLE patient listed for arthroplasty or fracture fixation. Each scenario has a defined evidence base and a checklist that examiners love to test.
- Prevalence: SLE affects roughly 30-50 per 100,000 adults worldwide, with a 9:1 female-to-male ratio and peak onset in the second to fourth decade
- MSK involvement: 90-95% of patients develop arthralgia, non-erosive arthritis, or a defined arthropathy during the disease course
- AVN: cumulative incidence of symptomatic AVN in SLE cohorts is 5-15%, with asymptomatic MRI-detected lesions in up to 40%
- Jaccoud arthropathy: 5-12% of SLE patients, increasing with disease duration and severity
- Arthroplasty outcomes: SLE patients have higher perioperative complication rates (infection, VTE, flare) than matched controls
- Wound healing: chronic steroid use impairs collagen synthesis and increases dehiscence risk
- Functional impact: Jaccoud deformity is often more cosmetic than functional; AVN is the dominant MSK cause of disability
- Mortality: periprosthetic joint infection risk in SLE is 1.5-2x matched RA, mainly driven by immunosuppression
Pathophysiology
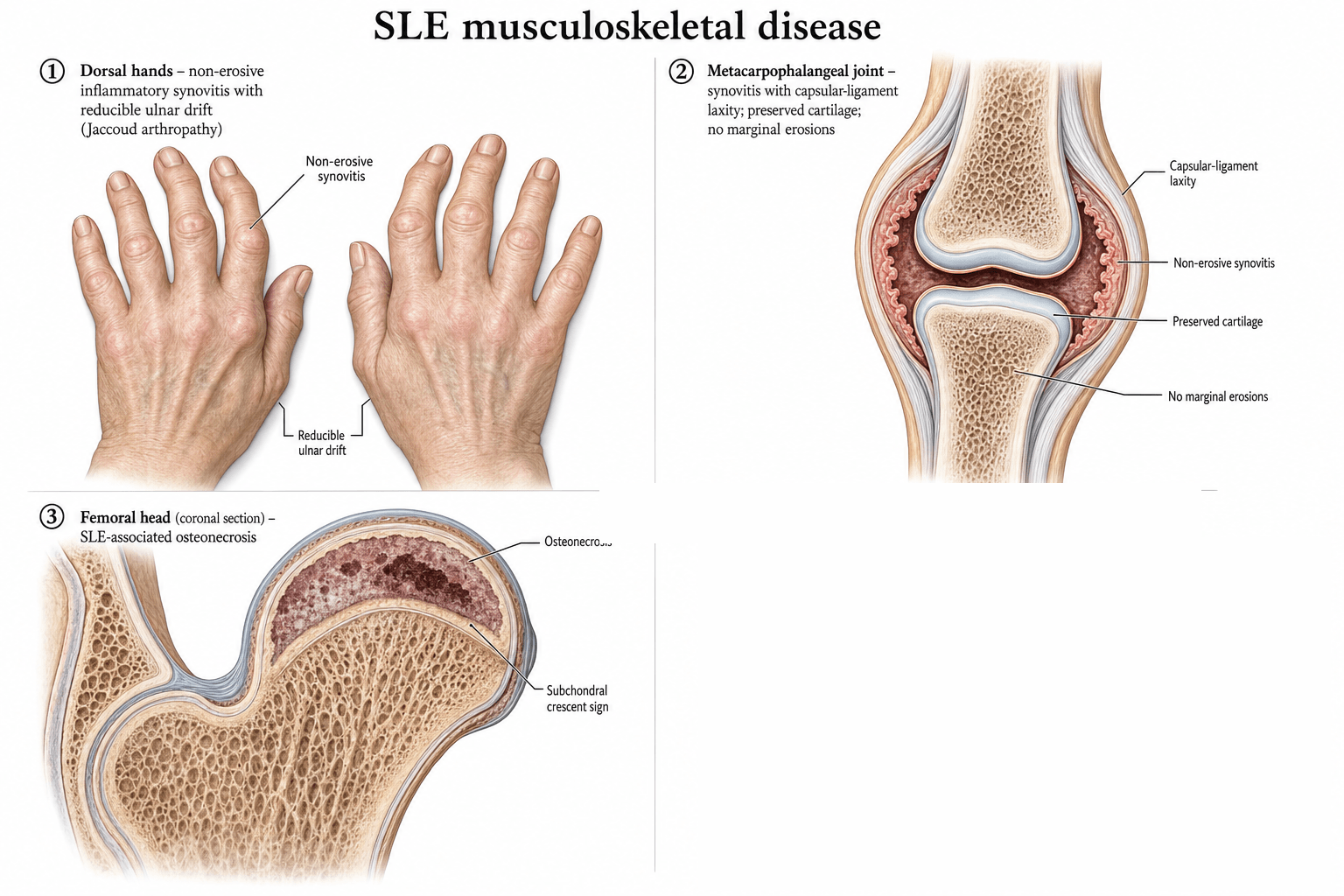
The SLE orthopaedic phenotypes arise from two separable but overlapping mechanisms. Inflammatory capsuloligamentous laxity (immune complex deposition in synovium and peri-articular soft tissues) underlies Jaccoud arthropathy and is the principal driver of hand deformity. Ischaemic bone death (corticosteroid-induced adipocyte hypertrophy, intraosseous pressure rise, and microvascular thrombosis from antiphospholipid antibodies) underlies avascular necrosis. The two mechanisms are not mutually exclusive - a patient may have Jaccoud hands AND bilateral femoral head AVN.
- Driver
- Type III hypersensitivity, complement activation
- Clinical Phenotype
- Non-erosive polyarthritis, tenosynovitis
- Modifiable?
- Yes - immunosuppression (HCQ, MMF, biologics)
- Driver
- Chronic inflammation + fibrotic remodelling
- Clinical Phenotype
- Jaccoud deformity (ulnar deviation, swan neck)
- Modifiable?
- Limited - splints, synovectomy
- Driver
- Intraosseous fat cell hypertrophy, raised pressure
- Clinical Phenotype
- Subchondral ischaemia, AVN
- Modifiable?
- Yes - steroid-sparing regimens
- Driver
- Antiphospholipid antibodies, vasculitis
- Clinical Phenotype
- Bone infarcts, atypical AVN distribution
- Modifiable?
- Yes - anticoagulation where indicated
- Driver
- Autoimmune muscle inflammation (overlap syndromes)
- Clinical Phenotype
- Proximal weakness, raised CK
- Modifiable?
- Yes - immunosuppression
Synovitis: Immune-complex driven, often transient
Capsule + ligament: Chronic inflammation weakens capsuloligamentous structures (MCP volar plate, PIP collateral, extensor hood)
Tendon subluxation: Extensor tendons slip ulnarly at the MCP, intrinsic muscles shorten
Deformity: Ulnar deviation, swan-neck, boutonniere - all passively correctable early
No erosion: Articular cartilage preserved despite deformity
Steroid effect: Adipocyte hypertrophy in marrow raises intraosseous pressure
Apoptosis: Osteocyte and adipocyte apoptosis in subchondral bone
Microvascular compromise: Vasculitis, Raynaud, antiphospholipid-mediated thrombosis
Fat emboli: Possible role of fat emboli from steroid-induced marrow change
Result: Subchondral fracture, femoral head collapse, secondary OA
Classification and Types
Classification of MSK Involvement in SLE
- Prevalence
- Commonest, greater than 80%
- Key Features
- Migratory pain, no swelling
- Management
- NSAIDs, hydroxychloroquine
- Prevalence
- 50-60%
- Key Features
- Symmetrical, reversible
- Management
- DMARDs, short-course steroids
- Prevalence
- 5-12%
- Key Features
- Reducible deformity, no erosion
- Management
- Splints, synovectomy, tendon rebalancing
- Prevalence
- Under 5%
- Key Features
- Erosive arthritis with SLE features
- Management
- Treat as RA; methotrexate often required
- Prevalence
- 5-15% symptomatic
- Key Features
- Multifocal, steroid-related
- Management
- Core decompression, arthroplasty
- Prevalence
- Under 10%
- Key Features
- Overlap with dermatomyositis / polymyositis
- Management
- Immunosuppression, physio
Rhupus is a small but important subgroup - erosive arthritis with SLE serology, behaving clinically like RA.
Clinical Assessment
- SLE features: malar rash, photosensitivity, oral ulcers, serositis, renal disease, cytopenias, neurological
- Current disease activity: SLEDAI score, BILAG index, current immunosuppression
- Joint symptoms: pain, swelling, morning stiffness (usually minutes, not hours as in RA)
- Avascular necrosis symptoms: groin / buttock / knee / shoulder pain, especially after steroid bursts
- Thrombosis history: DVT, PE, stroke, transient ischaemic attack, pregnancy morbidity
- Hands: pattern of deformity (ulnar deviation reducible? swan-neck? boutonniere?), squeeze test, FDS / FDP function
- Skin: periungual erythema, livedo reticularis, digital ulceration, Raynaud
- Hips / knees / shoulders: log roll, FABER, FADIR, ROM, antalgic gait, limb length
- Multifocal AVN screening: examine the contralateral joint and image when one site is identified
- System screen: BP, urine dipstick, fundoscopy, lymphadenopathy
Inspect the hand at rest: ulnar deviation, swan-neck, boutonniere may be obvious.
Test passive correction: in Jaccoud, the examiner can passively correct the deformity - this is the key clinical sign distinguishing it from RA. With RA, fixed deformity resists correction and X-ray shows erosions.
Look for function: despite dramatic-looking deformity, Jaccoud hands often retain good grip and key-pinch. A patient's Jaccoud hand may function better than an RA hand with less obvious deformity.
- What to Look For
- Passive internal/external rotation of hip
- Sensitivity
- Moderate - painful in early AVN
- Notes
- Non-specific but useful screen
- What to Look For
- Impingement signs
- Sensitivity
- Moderate
- Notes
- Differential: labral tear, OA, FAI
- What to Look For
- Image both hips when one is symptomatic
- Sensitivity
- High for multifocal disease
- Notes
- Mandatory in SLE
- What to Look For
- Bone marrow oedema, double-line sign, fat signal
- Sensitivity
- Gold standard
- Notes
- Detects pre-collapse AVN
SLE is one of the classic causes of multifocal AVN. A young patient on steroids with one painful joint should trigger MRI of at least both hips and both knees; some centres add shoulders and ankles. The detection of pre-collapse disease changes management from arthroplasty to joint-preserving core decompression. Missing the contralateral lesion is a recurring exam pitfall.
Investigations
Diagnostic Work-up
Immunology: ANA (sensitive, non-specific), anti-dsDNA (specific, tracks activity), anti-Smith (specific), C3/C4 (low in active disease), anti-SSA/SSB (associated with neonatal lupus, Sjögren)
Antiphospholipid screen: lupus anticoagulant (functional assay), anti-cardiolipin IgG/IgM, anti-beta2 glycoprotein I - confirm positive result after 12 weeks
Inflammatory markers: ESR often raised, CRP variable (often normal even with active disease)
Imaging: X-ray of symptomatic joints (often normal early); MRI of suspected AVN sites
MRI signs: bone marrow oedema, double-line sign on T2 (low signal outer band, high signal inner band), geographic subchondral lesion
Distribution: most common at femoral head (90%), then femoral condyles, humeral head, talus, lunate
Multifocal screening: when one joint AVN confirmed, image at least both hips and both knees
Quantify: ARCO / Ficat stage dictates joint-preserving vs arthroplasty decision
Renal: eGFR, urine protein:creatinine ratio, electrolytes (lupus nephritis flare risk)
Haematology: full blood count (cytopenias common), coagulation, group and save, crossmatch
Cardiac: ECG, echocardiogram if indicated (pericarditis, Libman-Sacks endocarditis, premature atherosclerosis)
Disease activity: SLEDAI / BILAG within 4 weeks of elective surgery
Medication review: prednisolone dose, MMF / azathioprine / cyclophosphamide / belimumab / rituximab timing
SLE can be serologically active with a normal CRP, and CRP can spike with serositis or infection independently of disease activity. A persistently normal CRP with active joint pain points to non-erosive inflammatory arthritis rather than septic arthritis; a sudden CRP rise in a patient on steroids should prompt a search for infection rather than assumed flare.
- Disease Association
- greater than 95% of SLE - sensitive, not specific
- Surgical Implication
- No direct surgical relevance
- Disease Association
- Specific, tracks nephritis activity
- Surgical Implication
- High titre = defer elective surgery, renal risk
- Disease Association
- Highly specific for SLE
- Surgical Implication
- Confirms diagnosis, no direct surgical action
- Disease Association
- Sjögren, neonatal lupus, congenital heart block
- Surgical Implication
- Counsel on pregnancy, neonatal risk
- Disease Association
- Thrombosis risk despite prolonged aPTT in vitro
- Surgical Implication
- Pre-op VTE prophylaxis plan mandatory
- Disease Association
- Thrombosis, pregnancy morbidity
- Surgical Implication
- VTE risk; may need bridging anticoagulation
Management Algorithm
Medical Management of SLE MSK Disease
Treatment Ladder
Hydroxychloroquine (HCQ): cornerstone DMARD, 200-400 mg/day; retinal toxicity screening yearly after 5 years
Lifestyle: sun avoidance, smoking cessation, vitamin D, weight-bearing exercise, infection prevention
NSAIDs: useful for arthralgia but renal and GI risk in lupus nephritis
Short-course oral prednisolone: minimum effective dose, less than 7.5 mg/day where possible
Add DMARD: methotrexate, azathioprine, leflunomide, mycophenolate mofetil
Belimumab: anti-BAFF monoclonal, approved for active SLE with musculoskeletal / cutaneous involvement
Rituximab: B-cell depletion for refractory disease, evidence strongest in vasculitis and haematologic lupus
Anifrolumab: type I interferon receptor antagonist, approved for moderate to severe SLE
Voclosporin / cyclophosphamide: lupus nephritis protocols
Steroid-sparing strategies are central to reducing AVN risk - the goal is the lowest cumulative steroid dose that controls disease.
Complications
- Mechanism
- Steroid + microvascular thrombosis
- Risk Factors
- Cumulative dose greater than 3-5 g, pulses, APS
- Management
- MRI screening, joint-preserving surgery, arthroplasty
- Mechanism
- Immunosuppression, steroid-induced skin fragility
- Risk Factors
- HCQ, MMF, belimumab, rituximab, steroids
- Management
- Pre-op optimisation, antibiotic prophylaxis, surveillance
- Mechanism
- Antiphospholipid antibodies, surgery trigger
- Risk Factors
- Positive lupus anticoagulant, prior thrombosis
- Management
- Bridging anticoagulation, extended prophylaxis
- Mechanism
- Surgical stress, steroid withdrawal
- Risk Factors
- Active disease at operation, abrupt withdrawal
- Management
- Stress-dose steroids, continue DMARDs where safe
- Mechanism
- Steroid-induced collagen impairment
- Risk Factors
- Long-term steroids, poor nutrition
- Management
- Tension-free closure, prolonged antibiotics
- Mechanism
- Active underlying inflammation
- Risk Factors
- Steroid-dependent disease
- Management
- Optimise medical control before surgery
The one-pager lists "tendon rupture" but it deserves its own answer because it is a classic SLE viva trap: a steroid-treated lupus patient who ruptures a major tendon after trivial or no trauma.
- Mechanism: chronic steroid use plus a lupus enthesopathy degrades the tendon-bone junction; ruptures are typically at the insertion and the tendon quality is poor.
- Sites: the extensor mechanism is classic - patellar tendon, quadriceps tendon, Achilles tendon, and finger extensors; bilateral and multiple ruptures are characteristic and a strong clue to the diagnosis.
- Recognition: a sudden extensor lag, palpable gap and inability to straight-leg-raise after a minor stumble; always examine and image the contralateral side because simultaneous/sequential bilateral rupture is described.
- Management: surgical repair is harder than in normal tendon (friable tissue, high re-rupture), so use augmentation/reinforcement, protect with longer immobilisation, and optimise steroid dose first; a missed or late repair retracts and becomes a reconstruction.
Exam point: an atraumatic patellar or quadriceps tendon rupture in a young person on steroids is SLE (or chronic kidney disease/RA) until proven otherwise - and check the other leg.
Catastrophic APS (CAPS) is a rare but greater than 50% mortality syndrome of multi-organ microthrombosis developing over days, often triggered by infection, surgery, or anticoagulation withdrawal. In an SLE patient with positive aPL antibodies who deteriorates rapidly after an operation (renal failure, respiratory distress, neurological signs, skin necrosis), think CAPS, escalate to ICU, and start anticoagulation + plasma exchange + high-dose steroids. Early recognition is the difference between survival and death.
AVN gets the attention, but the same steroids cause glucocorticoid-induced osteoporosis (GIOP) - the commonest cause of secondary osteoporosis and a distinct, examinable MSK complication in SLE that the surgeon must not conflate with AVN.
- Mechanism: glucocorticoids suppress osteoblasts and prolong osteoclast survival, causing rapid bone loss in the first 3-6 months of therapy that disproportionately affects trabecular bone (vertebrae, femoral neck) - so fractures occur at a higher bone-density level than in postmenopausal osteoporosis.
- Consequence: vertebral fragility (often atraumatic/asymptomatic) fractures and hip/wrist fractures; lupus adds inflammation, renal impairment, low vitamin D and reduced mobility on top of the steroid effect.
- Prevention/treatment: lowest effective steroid dose; calcium and vitamin D; assess fracture risk with FRAX (with the glucocorticoid adjustment) and DXA; start a bisphosphonate (or denosumab) for patients on significant ongoing steroids or with a prior fragility fracture, per glucocorticoid-osteoporosis guidance.
- Distinction from AVN: GIOP = generalised low bone mass / fragility fracture (DXA, vertebral imaging); AVN = focal subchondral bone death (MRI double-line sign). Both are steroid-driven and can coexist - a steroid-treated lupus patient needs both a bone-protection plan and AVN vigilance.
Outcomes and Prognosis
- Outcome
- 80-90% achieve quiescent disease
- Complication Rate
- HCQ retinopathy, DMARD toxicity
- Notes
- Multidisciplinary care essential
- Outcome
- 60-80% joint survival at 5 years
- Complication Rate
- Low morbidity, donor site (if graft)
- Notes
- Best in small lesions, young patients
- Outcome
- Good pain relief, 90% 10-year survival
- Complication Rate
- PJI 2-4%, VTE 2-3%
- Notes
- Higher than matched OA - counsel patient
- Outcome
- Variable, mostly cosmetic gain
- Complication Rate
- Recurrence common if disease active
- Notes
- Optimise medical control first
Good prognostic markers: early hydroxychloroquine, low cumulative steroid dose, quiescent disease at time of surgery, normal renal function, no APS antibodies.
Adverse prognostic markers: cumulative prednisolone greater than 5 g, lupus nephritis, positive lupus anticoagulant, multifocal AVN, recurrent infection, active serositis at the time of surgery.
Key message for the exam: the dominant modifiable driver of MSK morbidity in SLE is cumulative steroid exposure - protect the bone by using steroid-sparing agents early.
Guidelines, Registries & Global Practice
- SLE prevalence is 30-50 per 100,000 worldwide, with higher rates and greater severity in women of African, Hispanic, and South Asian ancestry
- MSK involvement is the commonest organ manifestation across all populations - 90-95% of patients report joint symptoms at some point
- AVN rates vary with steroid prescribing practices; studies in the Asia-Pacific and African regions report symptomatic AVN in 5-15% of cohorts
- Antiphospholipid antibodies are found in 30-40% of SLE patients but only 10-15% develop clinical APS
- High-resource: multidisciplinary lupus clinics integrate rheumatology, nephrology, dermatology, orthopaedics, and pharmacy
- Limited-resource: hydroxychloroquine, low-dose steroids, and aspirin form the backbone; access to MRI for AVN screening and to biologics is variable
- Perioperative risk: low-resource settings may not have ready access to perioperative stress-dose steroid protocols or extended VTE prophylaxis
- Arthroplasty access: SLE patients with end-stage AVN may face long waits for joint replacement in publicly funded systems
- MSK focus
- Treat-to-target, HCQ for all unless contraindicated
- Steroid guidance
- Minimise cumulative dose; switch to DMARDs early
- Perioperative guidance
- Multidisciplinary assessment, screen aPL pre-op
- MSK focus
- DMARDs, biologics for refractory disease
- Steroid guidance
- Lowest effective dose; osteoporosis prophylaxis
- Perioperative guidance
- Stress-dose steroids, VTE prophylaxis for APS
- MSK focus
- HCQ, immunosuppressives, biologics by pathway
- Steroid guidance
- Same minimal-dose principle
- Perioperative guidance
- Pre-op assessment in rheumatology clinic
- MSK focus
- Biannual MSK assessment; AVN screening in high risk
- Steroid guidance
- Resource-adapted steroid minimisation
- Perioperative guidance
- Perioperative protocols vary by centre
There is no dedicated arthroplasty registry for SLE AVN, but national joint registries (NJR, AJRR, AOANJRR) capture patients with secondary OA due to AVN, including SLE subgroups. Reported outcomes show higher PJI, VTE, and revision rates than matched primary OA, reinforcing the need for enhanced perioperative protocols. The evidence base for medical management is dominated by RCTs of biologics and DMARDs; surgical evidence is largely case series and cohort studies.
Record in every SLE patient before surgery:
- Cumulative and current prednisolone dose
- aPL antibody status (lupus anticoagulant, anti-cardiolipin, anti-beta2 GPI) with dates of testing
- Disease activity score (SLEDAI or BILAG) within 4 weeks of surgery
- Renal function, urine protein, complement, anti-dsDNA
- Plan for stress-dose steroids, VTE prophylaxis, and antibiotic prophylaxis
- Communication with rheumatology and anaesthesia
A pre-operative checklist protects the patient and demonstrates governance in any jurisdiction.
Controversies & Areas of Uncertainty
Belimumab is a B-lymphocyte stimulator (BLyS) inhibitor. There is no consensus on stopping it perioperatively; many units hold for 4 weeks before and 4 weeks after elective surgery to reduce infection risk, while others continue it. The decision should be individualised with rheumatology.
Rituximab produces B-cell depletion lasting months. Emergency surgery during B-cell depletion carries high infection risk. Elective surgery is usually deferred until B-cell recovery. For trauma or urgent cases, screen for hypogammaglobulinaemia and consider IVIG.
DOACs (rivaroxaban, apixaban) are inferior to warfarin in patients with thrombotic APS, particularly triple-positive disease. Warfarin remains standard for APS-related arterial or recurrent venous thrombosis. The orthopaedic team should be aware when consenting for VTE prophylaxis.
Small studies suggest statins may reduce AVN risk by reducing intraosseous fat, and bisphosphonates may delay collapse in pre-collapse disease. Evidence is not yet strong enough for universal recommendation, but they are reasonable adjuncts in high-risk patients on long-term steroids.
MCQ Practice Points
Q: What is the structural basis of Jaccoud arthropathy? A: Capsuloligamentous laxity without bony erosion. Chronic synovitis in SLE weakens the MCP volar plate, collateral ligaments, and extensor hood, allowing tendon subluxation and reducible deformity. The articular cartilage is preserved - this is the key distinction from RA, where the deformity is fixed and erosive on X-ray.
Q: What is the dominant modifiable risk factor for AVN in SLE? A: Cumulative corticosteroid dose. The risk rises sharply with cumulative prednisolone greater than 3-5 g, daily doses greater than 20 mg, and pulse methylprednisolone. Non-modifiable contributors include Raynaud phenomenon, vasculitis, and antiphospholipid antibodies. Steroid-sparing strategies (azathioprine, MMF, belimumab) are central to AVN prevention.
Q: What is the most appropriate imaging for suspected AVN of the femoral head in a young SLE patient with normal X-rays? A: MRI of both hips and the knees. MRI is the gold standard for pre-collapse AVN, demonstrating bone marrow oedema and the pathognomonic double-line sign on T2. Bilateral imaging is mandatory because 30-50% of SLE AVN is multifocal; contralateral disease is often asymptomatic at presentation.
Q: A patient on 8 mg/day prednisolone is listed for total hip arthroplasty. What is your steroid plan? A: Stress-dose hydrocortisone cover. Continue the morning dose; give 50 mg IV hydrocortisone at induction, then 25 mg IV every 8 hours for 24-48 hours, then taper back to the oral dose. Abrupt withdrawal risks adrenal crisis. Do not stop hydroxychloroquine - it reduces post-operative flare and thrombosis risk.
Q: When is perioperative bridging anticoagulation indicated in SLE? A: Definite antiphospholipid syndrome with prior thrombosis. A single positive aPL test without clinical events is not APS. For patients with lupus anticoagulant, anti-cardiolipin, or anti-beta2 GPI on two occasions 12 weeks apart AND a history of thrombosis, surgery is a high-risk trigger for catastrophic APS and extended anticoagulation (often 4-6 weeks or longer) is indicated. Liaise with haematology.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old woman with SLE on 15 mg/day of prednisolone for 3 years (cumulative dose approximately 18 g) and a history of bilateral DVT presents with bilateral hip and right knee pain. Hip X-rays show subchondral collapse of the right femoral head (Ficat IV) and a sclerotic crescent sign on the left (Ficat III). MRI confirms bilateral femoral head AVN and a 3 cm lesion in the medial femoral condyle. aPL antibodies are positive (lupus anticoagulant and anti-cardiolipin IgG). How would you manage her?”
“A 45-year-old man with SLE controlled on 5 mg/day prednisolone and 200 mg/day hydroxychloroquine is listed for elective total knee arthroplasty for AVN-related secondary OA. He has quiescent disease (SLEDAI 2), normal renal function, and positive anti-cardiolipin IgM at low titre. His GP has stopped his aspirin. What is your perioperative plan?”
Core Definitions
- SLE = multisystem autoimmune disease, 9:1 female predominance, peak onset 20-40 years
- MSK involvement affects 90-95% of patients (arthralgia, non-erosive arthritis, Jaccoud, AVN)
- Jaccoud arthropathy = reducible deformity without bony erosion (5-12%)
- AVN in SLE is multifocal in 30-50% of cases (bilateral hips, knees, shoulders)
Jaccoud vs RA Hand
- Jaccoud: reducible deformity, no erosions on X-ray, function often preserved
- RA: fixed deformity, early erosions, function tracks deformity
- Test by passive correction - examiner can straighten a Jaccoud hand
- Management: hand therapy first, synovectomy or tendon realignment if symptomatic
AVN Risk Factors
- Cumulative prednisolone greater than 3-5 g equivalent
- Daily dose greater than 20 mg or pulse methylprednisolone
- Raynaud phenomenon, vasculitis, antiphospholipid antibodies
- Multifocal AVN is a SLE signature - image contralateral joint and screen both hips and knees
Imaging Algorithm
- X-ray often normal in early AVN (Ficat I-II)
- MRI is gold standard - bone marrow oedema, double-line sign on T2
- Bilateral hips plus knees MRI when one AVN is identified
- ARCO / Ficat stage dictates joint-preserving vs arthroplasty decision
Perioperative Checklist (SAFE ORTHO)
- Stress-dose hydrocortisone for any patient on greater than 5 mg/day prednisolone
- Continue hydroxychloroquine - reduces flare and thrombosis risk
- Screen aPL antibodies (lupus anticoagulant, anti-cardiolipin, anti-beta2 GPI)
- Extended VTE prophylaxis for 4-6 weeks, especially in APS
Antiphospholipid Syndrome Pearls
- APS in 10-15% of SLE; requires clinical event plus persistent aPL on 2 tests 12 weeks apart
- Catastrophic APS - greater than 50% mortality, often surgery-triggered, treat with anticoagulation + plasma exchange + steroids
- Warfarin remains standard for thrombotic APS; DOACs inferior in triple-positive disease
- Positive aPL alone (no events) does not mandate perioperative anticoagulation change
Evidence Base and Key Trials
The 1982 revised criteria for the classification of systemic lupus erythematosus
- Eleven criteria covering mucocutaneous, serosal, renal, neurological, haematological, and immunological features
- Four or more criteria (serially or simultaneously) give 96% sensitivity and 96% specificity for SLE
- Included arthritis as a non-erosive, non-deforming joint involvement pattern - distinguishing it from RA
2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus
- Entry criterion: positive ANA at a titre of 1:80 or greater on HEp-2 cells
- Additive weighted criteria across 10 domains including arthritis, mucocutaneous, renal, neuropsychiatric
- Joint involvement scored 6 points; required to be observed by a clinician with synovitis in 2 or more joints
- Validation cohort achieved 96% sensitivity and 93% specificity for SLE
International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS)
- Definite APS requires at least one clinical (thrombosis or pregnancy morbidity) and one laboratory criterion (aPL antibodies on 2 occasions 12 weeks apart)
- Laboratory panel: lupus anticoagulant, anti-cardiolipin IgG/IgM, anti-beta2 glycoprotein I IgG/IgM
- Stratified by thrombosis type (arterial vs venous) and added obstetric APS as a separate category
Osteonecrosis in patients with SLE
- SLE cohort analysis demonstrating cumulative corticosteroid dose as the dominant predictor of AVN
- Cushingoid habitus, vasculitis, Raynaud phenomenon, and serositis identified as independent risk factors
- Multifocal AVN documented in 30-50% of affected patients - most commonly bilateral femoral heads
Morbidity and mortality in systemic lupus erythematosus during a 10-year period: a comparison of early and late manifestations in a cohort of 1,000 patients
- 1000-patient European cohort followed for 10 years describing cumulative organ damage (SLICC/ACR damage index)
- MSK involvement including AVN, Jaccoud deformity, and tendon rupture contributed substantially to the damage index
- Infection and active lupus were the leading causes of mortality - both relevant to perioperative risk