Trabecular Metal and Porous Structure
- Definition: A highly porous transition metal (Element 73) often referred to as 'Trabecular Metal' or 'Tantalum Foam'
- Definition: Used as a coating or bulk implant for acetabular cups, cones, and augments
- Mechanism: Manufactured by Chemical Vapour Deposition (CVD) of pure Tantalum onto a vitreous carbon skeleton
- Management: Ideal for revision situations with bone loss
- “Young's Modulus: ~3 GPa (Very close to cancellous bone)
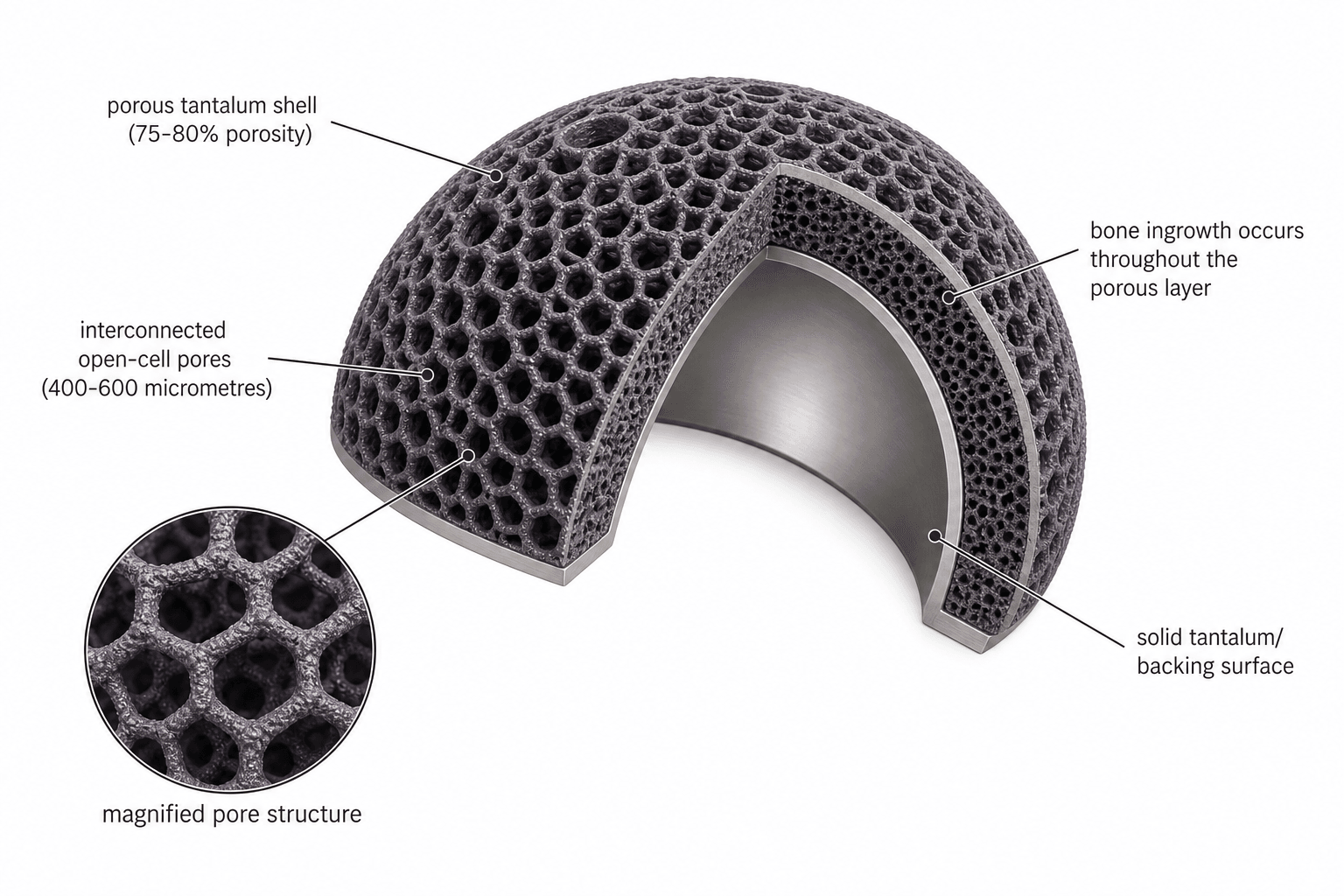
- “Porosity: 75-80% (Higher than any other porous coating)
- “Excellent osseointegration
- “Biological fixation occurs rapidly
Tantalum
The key features of Tantalum are its High Porosity (80%) and Low Modulus (3 GPa - similar to cancellous bone). This minimises stress shielding and maximises biological ingrowth potential. It also has a High Coefficient of Friction (~0.88-0.98 against bone), making it grip bone like velcro for superb initial stability.
CAMP-FTantalum Properties
Hook:Picture a CAMP-Fire made of bone-coloured foam: porous, soft (low modulus) and sticky.
Composition & Structure
Tantalum (Ta, atomic number 73) is a hard, ductile, corrosion-resistant transition metal. In orthopaedics it is used as a highly porous open-cell structure marketed as Trabecular Metal (Zimmer Biomet), nicknamed "tantalum foam."
- Porosity 75-80% — the highest of any clinically used porous metal (sintered titanium/cobalt-chrome beads achieve only 30-40 percent). High volumetric porosity gives an enormous surface area and an interconnected pore network for three-dimensional bone ingrowth.
- Low elastic modulus (~3 GPa) — close to cancellous bone (0.1-2 GPa) and far below titanium alloy (~110 GPa) or stainless steel (~200 GPa). This minimises stress shielding and encourages physiological load transfer.
- High coefficient of friction (~0.88-0.98 against bone/trabecular metal) — much higher than titanium beads (~0.6). This "scratch-fit" gives immediate mechanical stability with minimal supplementary fixation.
- Self-passivating oxide layer — tantalum pentoxide forms spontaneously, giving excellent biocompatibility and bioactivity (forms a bone-like apatite layer in vivo). Tantalum has a long safety record as pacemaker electrodes, cranioplasty plates and radiopaque markers.
Manufacturing (CVD)
- A skeleton (scaffold) of Reticulated Vitreous Carbon is placed in a vacuum chamber.
- Tantalum gas is deposited onto the skeleton.
- Result: 99% Pure Tantalum surface with a carbon core.
- Cellular: Resembles trabecular bone (dodecahedron shape).
- Porosity: 75-80% (Standard sintered beads are only ~30-40% porous).
- Pore Size: 400-600 microns (Ideal for osteoblast ingrowth).
Tantalum vs Titanium Beads
Applications in Revision
-
Acetabular Revision:
- "Paprosky" defects.
- Tantalum Cones/Wedges fill large bone voids.
- Trabecular Metal cups bridge defects with minimal screws due to high friction.
-
Knee Revision:
- Metaphyseal Cones (Femur and Tibia).
- Provide structural support where cancellous bone is lost.
-
Spine:
- Cages (interbody fusion).
- Bioactive surface + Radiolucent properties (sort of - less artifact than steel).
Tantalum implants become extremely difficult to remove once osseointegration occurs. Bone grows deep into the 80% porous structure, creating a biological weld. Plan carefully before using tantalum - it's essentially a permanent solution.
Biomechanics & Stress Shielding
- Cortical bone: 15-20 GPa
- Cancellous bone: 0.1-2 GPa
- Tantalum: 3 GPa ✓ Closest match to cancellous bone
- Titanium alloy: 110 GPa (excessive stiffness)
- Stainless steel: 200 GPa (severe stress shielding)
- Minimizes stress shielding
- Promotes physiological load transfer
- Stimulates bone remodeling
- Reduces risk of peri-implant bone loss
How Tantalum Osseointegrates: Ingrowth vs Ongrowth
The topic repeatedly invokes "excellent osseointegration," "rapid biological fixation" and the "biological weld," but the mechanism — and especially the distinction between bone ingrowth and ongrowth — is worth making explicit, because it is what sets tantalum apart from older porous coatings.
- Ongrowth is bone apposition onto a roughened or thinly textured surface (grit-blasted or plasma-sprayed titanium, hydroxyapatite coatings). Fixation is essentially two-dimensional — bone bonds to the outer surface only.
- Ingrowth is bone growing into a three-dimensional, interconnected pore network. Sintered beads and fibre-mesh allow only limited ingrowth into a thin surface layer (typically less than 1 mm deep). Tantalum differs in degree: its 75 to 80 percent open-cell structure lets bone grow throughout the full thickness of the construct — which is exactly why an ingrown tantalum implant behaves like a "biological weld" and is so destructive to remove.
haematoma and fibrin scaffold within the pores, then osteoprogenitor recruitment with the self-passivating tantalum-oxide surface supporting apatite deposition (osteoconduction), then woven bone laid down on the pore walls, then remodelling to lamellar bone — with Haversian systems eventually seen deep within the pores. The general biology of the bone–implant interface is developed in the dedicated osseointegration topic.
Prerequisites — why the scratch-fit and the ingrowth are inseparable. Ingrowth is not automatic; it requires:
- Initial mechanical stability — interface micromotion must stay low (broadly under about 40 micrometres; motion of roughly 150 micrometres or more provokes fibrous encapsulation rather than bone). Tantalum's high friction coefficient delivers precisely this immediate stability, so the scratch-fit and the biological fixation are two halves of one story.
- Small gaps / close apposition — large bone–implant gaps fill with fibrous tissue, so press-fit that minimises them is essential.
- Appropriate pore size — the 400 to 600 micrometre window covered above, together with an osteoconductive surface.
- A viable, uninfected host bed — which is why infection, not loosening, is the dominant failure mode in the published cone and cup series.
100-400-600Pore Size for Ingrowth
Hook:Climb 100 to 400 to 600: too small = scar, just right = bone, too big = weak.
Management Algorithm
Choosing a strategy for severe periarticular bone loss
Tantalum vs 3D-Printed (Additive) Porous Titanium
The comparison table above, the controversies below, and a stock viva follow-up ("how does it compare to 3D-printed titanium?") all set tantalum against printed titanium — so it is worth stating what additive-manufactured porous titanium actually is and where the two genuinely differ.
Two different ways to make a porous metal:
- Tantalum (CVD). Pure tantalum is vapour-deposited onto a reticulated vitreous-carbon skeleton, reproducing a trabecular, dodecahedral open-cell architecture around a residual carbon core. The pore pattern is a property of the carbon scaffold, not individually designed.
- 3D-printed titanium (additive manufacturing). Selective laser melting (SLM/DMLS) or electron-beam melting (EBM) fuses titanium-alloy powder layer by layer to build a computationally designed lattice. Pore size, shape, gradient and even regional stiffness can be specified in the CAD file. The titanium metallurgy itself is covered in the dedicated titanium-alloys topic.
Where they actually differ:
- Porous tantalum
- CVD onto carbon scaffold
- 3D-printed titanium
- Layer-by-layer powder fusion (SLM/EBM)
- Porous tantalum
- Fixed trabecular pattern
- 3D-printed titanium
- Designed, tunable lattice
- Porous tantalum
- 75 to 80 percent
- 3D-printed titanium
- Comparable (design-dependent)
- Porous tantalum
- Around 3 GPa
- 3D-printed titanium
- Higher than tantalum, but tunable by lattice design (far below solid titanium)
- Porous tantalum
- Very high (around 0.88 to 0.98)
- 3D-printed titanium
- High; gives reliable press-fit
- Porous tantalum
- High (roughly 3 to 5 times standard)
- 3D-printed titanium
- Generally lower than tantalum
- Porous tantalum
- Longer clinical follow-up
- 3D-printed titanium
- Newer; survivorship comparable in pooled data
The practical bottom line. Both achieve cementless fixation by the same biological route — three-dimensional ingrowth plus scratch-fit. Pooled meta-analysis shows no significant survivorship difference between tantalum and printed-titanium cones, so the choice is increasingly driven by cost, on-shelf availability and design flexibility rather than any true biological superiority. This is exactly why the historical "tantalum is uniquely osteoconductive" framing is softening.
80-3-1Tantalum vs Titanium Beads — the Numbers
Hook:80-3-1: eighty percent holes, three giga-pascals, friction near one.
Guidelines, Registries & Global Practice
Global epidemiology of use. Tantalum is a niche but high-value biomaterial used almost exclusively in revision (and selected complex primary) arthroplasty for managing acetabular and metaphyseal bone loss. Demand is rising worldwide as the volume of revision hip and knee surgery grows with an ageing arthroplasty population.
Guideline / consensus positions (side by side):
- Position on highly porous metal for bone loss
- Endorses highly porous ingrowth surfaces (tantalum, printed titanium) for cementless revision fixation
- Position on highly porous metal for bone loss
- Supports trabecular metal augments/cups for severe acetabular defects within a reconstruction algorithm
- Position on highly porous metal for bone loss
- Teaches scratch-fit metaphyseal/acetabular fixation over large structural allograft where host contact allows
- Position on highly porous metal for bone loss
- Recognises porous metals as standard for cavitary and contained segmental defects; reserves cages/cup-cage for discontinuity
Registry signal. National joint registries (NJR England/Wales, AJRR USA, AOANJRR Australia, Swedish and Norwegian registries) record increasing use of trabecular-metal acetabular components in revision and report mid-term revision rates consistent with the published cohort and meta-analysis data above. Registries do not yet show a clear divergence between tantalum and 3D-printed titanium constructs.
High- vs limited-resource practice. In well-resourced centres, tantalum cones, augments and cups are kept on the shelf for complex revision and chosen for immediate scratch-fit stability in poor bone. In cost-constrained settings the 3-5x price premium drives greater reliance on impaction/structural allograft, cages, or cheaper modular components, and complex bone-loss cases are often centralised to tertiary referral units. Selection everywhere balances ingrowth potential, modulus matching, host-bone availability and the difficulty of any future extraction.
Controversies & Areas of Uncertainty
- Tantalum vs 3D-printed titanium. Additive-manufactured highly porous titanium now matches tantalum's porosity and pore architecture at lower cost and stiffness intermediate between the two. Pooled meta-analysis shows no significant survivorship difference between tantalum and printed-titanium cones, so the historical "tantalum is unique" framing is weakening.
- Cost-effectiveness. Tantalum costs roughly 3-5 times a standard component. Whether the ingrowth advantage justifies this over cheaper printed-titanium or graft strategies is unresolved and varies by health system.
- Extraction burden. Deep ingrowth into an 80 percent porous structure makes removal at re-revision difficult and bone-destructive. This is a genuine downside in younger patients who may face multiple future revisions.
- Failure mode. Contemporary data show aseptic loosening of cones is exceedingly rare (under 1 percent); infection is now the dominant reason for cone removal, shifting the research focus from fixation to infection prevention.
- Long-term data. Most acetabular and cone series report 5-10 year follow-up; 20-year data and performance in patients under 40 remain limited.
Limitations & Disadvantages
- Significantly more expensive than traditional implants
- 3-5 times the cost of standard titanium components
- Economic consideration in public hospital systems
- Extensive bone ingrowth makes revision extremely challenging
- May require extended trochanteric osteotomy or acetabular osteotomy
- Bone loss inevitable during removal
- Consider carefully before use in young patients
- More radiopaque than titanium
- Can obscure radiographic assessment of bone-implant interface
- May create artifact on CT imaging (though less than stainless steel)
- MRI compatible but creates some artifact
- Cannot substitute for massive bone loss without structural support
- Still requires reasonable host bone contact
- Pelvic discontinuity may still require additional fixation (plates, THA cage)
- Most studies have 5-10 year follow-up
- 20+ year data still emerging
- Uncertain performance in very young patients (less than 40 years old)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the material characteristics of the implant you would use for a Paprosky 3B acetabular defect in a revision hip replacement.”
“A 68-year-old woman needs revision TKA with a large metaphyseal tibial defect. How would you manage the bone loss? What biomaterial properties are important?”
“An examiner asks: 'Why is tantalum superior to sintered titanium beads for porous coating?' Walk me through the key differences.”
The Numbers
- Porosity: 80%
- Modulus: 3 GPa
- Friction: 0.98
Clinical Use
- Revision Hip (Cups/Augments)
- Revision Knee (Cones)
- Spine Cages
Evidence Base
Foundational bone-ingrowth study (canine transcortical model)
- Porous tantalum was 75-80% porous with dodecahedral pores averaging 430 and 650 microns
- Pore bone filling rose from 13% at 2 weeks to 63-80% by 16-52 weeks
- Minimum shear (push-out) fixation strength was 18.5 MPa at 4 weeks, substantially higher than other porous materials with lower porosity
- Haversian remodelling was seen within the pores at later timepoints
Biomaterial properties review — porous tantalum in orthopaedics
- Open-cell dodecahedral structure produced by CVD/infiltration of pure tantalum onto a vitreous carbon scaffold
- High volumetric porosity (70-80%), low elastic modulus and high frictional characteristics
- Self-passivating tantalum oxide layer drives apatite formation and excellent biocompatibility
- Applications span hip, knee, spine surgery and bone graft substitution
Trabecular metal cup for Paprosky IIIB defect with pelvic discontinuity
- 13 hips with type IIIB defect plus pelvic discontinuity treated with a trabecular metal cup +/- augment
- At mean 2.6 years, 12 of 13 hips were radiographically stable; only 1 showed possible loosening
- No patient required repeat surgery during follow-up
- Merle d'Aubigne score improved from 6.1 to 10.3
Porous tantalum tibial cones for large metaphyseal defects (revision TKA)
- 16 revision TKAs with AORI T2-T3B tibial defects reconstructed with porous tantalum cones
- At mean 31 months, 14 of 16 reconstructions functioned well with no reoperation
- The 2 failures were recurrent infection requiring removal of a well-fixed cone
- Radiographs showed restored joint line, neutral axis and stable osseointegration
Porous implants vs grafts for knee bone loss — meta-analysis
- Systematic review and meta-analysis of 77 studies and 4,391 knees
- No significant difference in 10-year failure between porous implants and grafting (OR 0.91, 95% CI 0.70-1.19)
- Larger functional improvement (standardised mean difference) for tantalum cones than for porous sleeves
- Grafts remained a reasonable option in younger patients with less constrained implants
Contemporary metaphyseal cones (tantalum vs 3D-printed titanium) — meta-analysis
- 63 studies, 4,433 patients and 5,435 cones; most defects were AORI 2B or 3
- Radiographic osseointegration achieved in 96.0% (95% CI 92.5-98.5)
- All-cause re-revision 13.5% at mean 49.7 months, driven by infection; cone removal only 3.6%
- No significant survivorship difference between tantalum and 3D-printed titanium cones (3.7% vs 2.2%, P = 0.199)
AAOS / AO biomaterials selection in revision arthroplasty
- Highly porous metals (tantalum, 3D-printed titanium) are endorsed for cementless fixation in cavitary and segmental bone loss
- Scratch-fit metaphyseal/acetabular fixation is preferred over large structural allograft where adequate host contact exists
- Implant selection should balance modulus matching, ingrowth potential and the difficulty of future extraction
References
- Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J Bone Joint Surg Br. 1999;81(5):907-14. PMID 10530861.
- Levine BR, Sporer S, Poggie RA, Della Valle CJ, Jacobs JJ. Experimental and clinical performance of porous tantalum in orthopedic surgery. Biomaterials. 2006;27(27):4671-81. PMID 16737737.
- Sporer SM, Paprosky WG. Acetabular revision using a trabecular metal acetabular component for severe acetabular bone loss associated with a pelvic discontinuity. J Arthroplasty. 2006;21(6 Suppl 2):87-90. PMID 16950068.
- Long WJ, Scuderi GR. Porous tantalum cones for large metaphyseal tibial defects in revision total knee arthroplasty: a minimum 2-year follow-up. J Arthroplasty. 2009;24(7):1086-92. PMID 18823749.
- Byttebier P, Dhont T, Pintelon S, Rajgopal A, Burssens A, Victor J. Comparison of different strategies in revision arthroplasty of the knee with severe bone loss: a systematic review and meta-analysis. J Arthroplasty. 2022;37(6S):S371-S381. PMID 35271982.
- Goh GS, Lee S, Singh K, et al. Contemporary outcomes of highly porous metaphyseal cones in revision total knee arthroplasty: a systematic review and meta-analysis. J Arthroplasty. 2026. PMID 41513075.