TGCT | PVNS | GCT-TS | CSF1-Driven Neoplasm | Synovial Proliferation
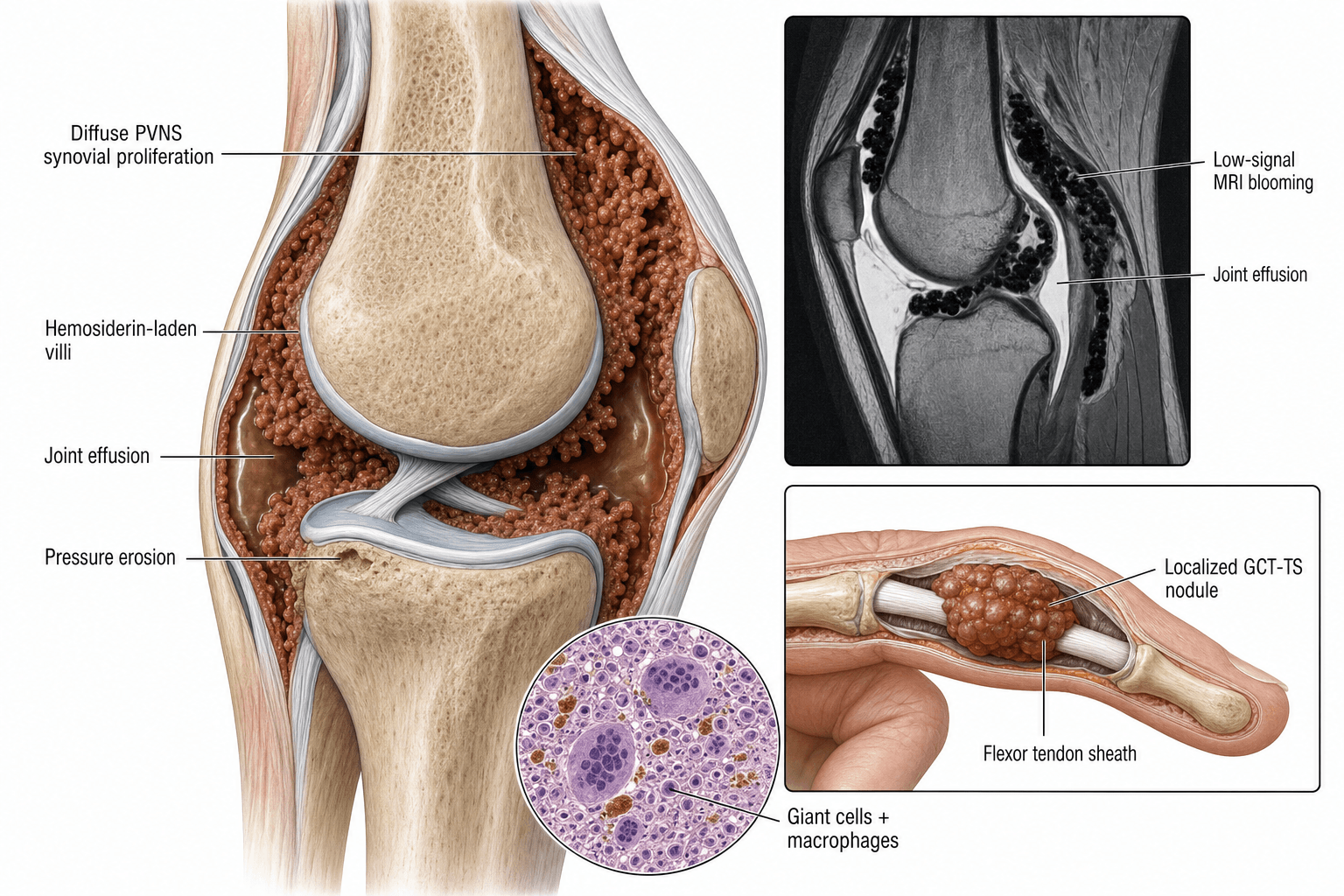
- TGCT is a neoplasm driven by CSF1 overexpression (not an inflammatory condition)
- Localised type (formerly GCT of tendon sheath): firm digital nodule, low recurrence after excision
- Diffuse type (formerly PVNS): infiltrative synovial proliferation of large joints, high recurrence
- MRI shows low T1 and low T2 signal due to haemosiderin, with blooming artefact on gradient echo
- Pexidartinib is a CSF1R tyrosine-kinase inhibitor approved for symptomatic diffuse TGCT not amenable to surgery
- “TGCT = most common synovial tumour of the hand (localised type)
- “Haemosiderin blooming on gradient-echo MRI is pathognomonic
- “CSF1 overexpression recruits CSF1R-positive macrophages (ligand-receptor mechanism)
- “Diffuse PVNS of the knee: anterior then posterior synovectomy for complete clearance
TGCT is the unified WHO term replacing PVNS (diffuse) and GCT of tendon sheath (localised). Both are driven by CSF1 overexpression. "Pigmented villonodular synovitis" is now considered obsolete nomenclature in pathology, though clinicians still use it.
CSF1 overexpression from a chromosomal translocation t(1;2)(p13;q35) fusing CSF1 to COL6A3. A minority of neoplastic cells overexpress CSF1, which recruits a massive population of CSF1R-expressing inflammatory macrophages — the bulk of the tumour mass.
Low T1 + low T2 + blooming on GRE = haemosiderin-laden synovium. This tripathic signal pattern is the imaging hallmark. Differential for low T2 synovial mass includes amyloid arthropathy and gouty tophi (but these do not bloom on GRE).
Localised = marginal excision (low recurrence). Diffuse = complete synovectomy (high recurrence 20-50%). Pexidartinib for symptomatic diffuse TGCT where surgery is not feasible or has failed. Monitor liver function on pexidartinib (hepatotoxicity risk).
- Diagnosis
- Localised TGCT (GCT-TS), MRI confirm
- Treatment
- Marginal excision
- Key Pearl
- Most common synovial tumour of the hand
- Diagnosis
- Diffuse TGCT (PVNS), MRI blooming artefact
- Treatment
- Combined anterior + posterior synovectomy
- Key Pearl
- High recurrence — counsel patient preoperatively
- Diagnosis
- Biopsy confirmation, CSF1R staining
- Treatment
- Pexidartinib (CSF1R inhibitor)
- Key Pearl
- Monitor LFTs monthly; hepatotoxicity black-box warning
BLOOMTGCT MRI Signal Pattern
Hook:When you see BLOOM on MRI, think haemosiderin-laden TGCT!
CLEARDiffuse TGCT Surgical Approach (Knee)
Hook:Get CLEAR margins — incomplete synovectomy guarantees recurrence!
Overview and Epidemiology
Tenosynovial giant cell tumour is the most common synovial neoplasm and a favourite exam topic because it bridges pathology (CSF1 translocation, haemosiderin-laden macrophages), imaging (blooming artefact on MRI), and treatment (surgery versus targeted therapy). The localised and diffuse types behave very differently and must be distinguished. Pexidartinib represents a paradigm shift — targeted therapy against the CSF1R pathway — and is examinable at fellowship level.
- Incidence: approximately 10 per million person-years (diffuse type rarer at 1-2 per million)
- Localised type: most common soft-tissue tumour of the hand (after ganglion cyst)
- Age: 30-50 years peak, slight female predominance for diffuse type
- Joints: knee (approximately 80 percent of diffuse), hip, ankle, shoulder, elbow
- Digits: localised type most common in the fingers (index and middle most frequent)
- Pain and swelling: chronic, progressive joint effusion
- Recurrent haemarthrosis: hallmark of diffuse intra-articular TGCT
- Joint destruction: bone erosions and secondary osteoarthritis if untreated
- Functional impairment: limited range of motion, mechanical symptoms
- Recurrence: the dominant clinical challenge in diffuse disease
Pathophysiology
TGCT is a true neoplasm, not an inflammatory or reactive process. The pathogenesis centres on CSF1 (colony-stimulating factor 1) overexpression. A chromosomal translocation — most commonly t(1;2)(p13;q35) — places the CSF1 gene under the control of the COL6A3 promoter, leading to constitutive CSF1 overexpression. A small population of neoplastic cells (carrying the translocation) secretes abundant CSF1, which recruits CSF1R-expressing monocytes and macrophages. These recruited cells constitute the vast majority (often greater than 90 percent) of the tumour mass. The recruited macrophages differentiate into multinucleated giant cells, haemosiderin-laden macrophages, and foam cells that characterise the histology.
- Localised (GCT-TS)
- Well-circumscribed, encapsulated nodule
- Diffuse (PVNS)
- Infiltrative, sheet-like synovial proliferation
- Localised (GCT-TS)
- Tendon sheath of digits (hand and foot)
- Diffuse (PVNS)
- Large joint synovium (knee, hip, ankle)
- Localised (GCT-TS)
- Focal, discrete attachment
- Diffuse (PVNS)
- Diffuse, villonodular, entire joint
- Localised (GCT-TS)
- Rare (pressure remodelling if large)
- Diffuse (PVNS)
- Common — subchondral cysts and erosions
- Localised (GCT-TS)
- Present but focal
- Diffuse (PVNS)
- Abundant — gives brownish discoloration
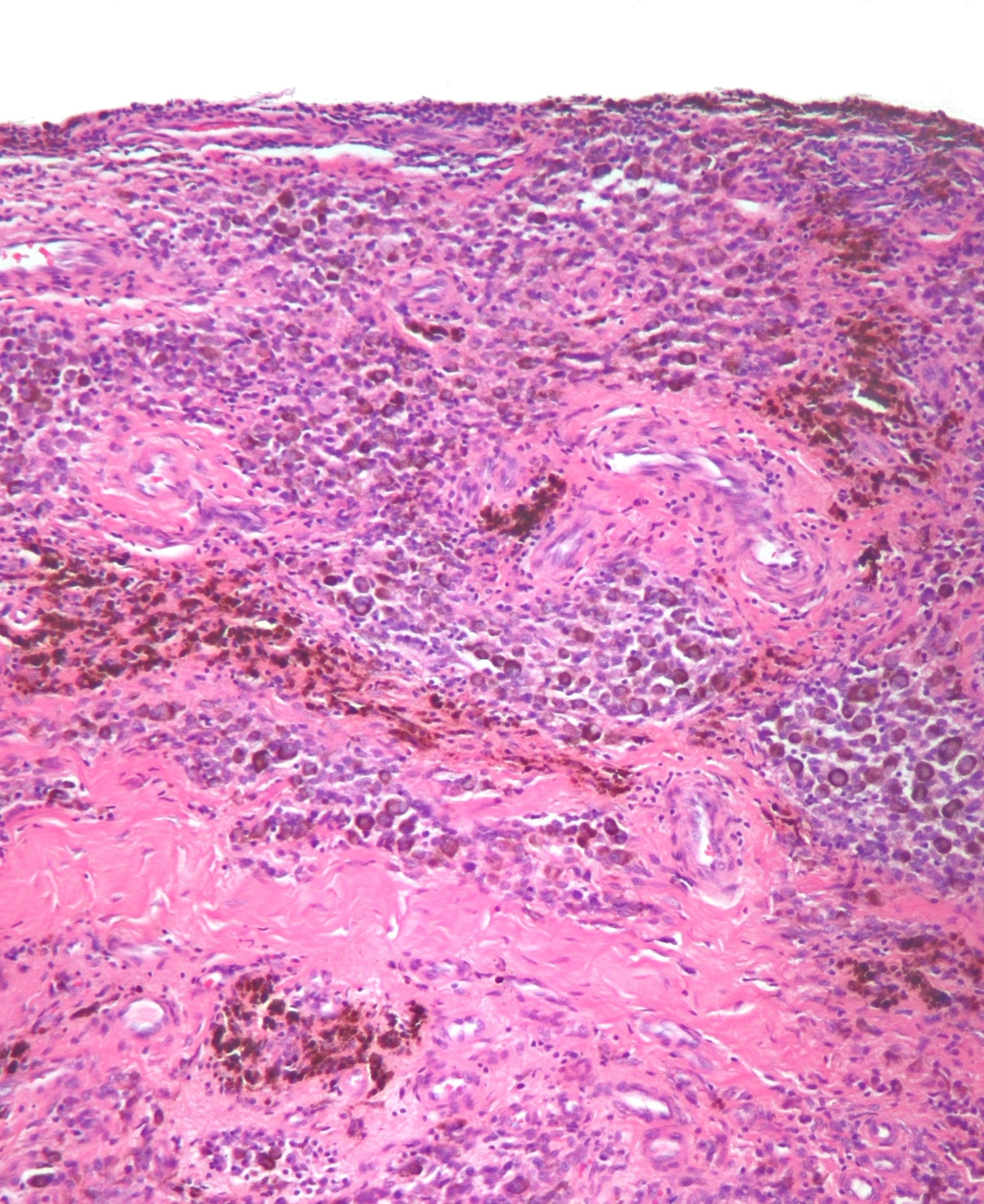
Three characteristic cell populations:
- Mononuclear stromal cells: the neoplastic population (small, round to oval nuclei)
- Multinucleated osteoclast-like giant cells: scattered, 5-50 nuclei per cell
- Haemosiderin-laden macrophages: dark brown pigment, Prussian blue positive
Plus: foam cells (xanthoma cells), inflammatory cells, and fibrosis in varying proportions
CSF1 mechanism:
- Translocation: t(1;2)(p13;q35) in approximately 70 percent of cases
- Fusion gene: CSF1-COL6A3 (COL6A3 promoter drives CSF1)
- Alternative: trisomy 5 and trisomy 7 in some cases
- Key insight: only 2-15 percent of cells carry the translocation
- Paracrine recruitment: neoplastic minority recruits the macrophage majority via CSF1-CSF1R ligand-receptor interaction
DRIVECSF1 Pathogenesis Cascade
Hook:CSF1 is the DRIVE behind TGCT — the translocation recruits the mass!
Classification and Types
Localised TGCT (Formerly Giant Cell Tumour of Tendon Sheath)
Most common soft-tissue tumour of the hand (after ganglion cyst). Presents as a firm, non-tender, slow-growing nodule attached to a tendon sheath, most frequently on the volar surface of the fingers.
- Details
- Volar aspect of index and middle fingers (tendon sheath)
- Details
- Firm, fixed to deep tissues, non-transilluminating, skin freely mobile over it
- Details
- Usually 1-3 cm, well-circumscribed
- Details
- Painless mass, occasionally mild discomfort with flexion, rarely nerve compression
- Details
- 5-15 percent (much lower than diffuse type)
The key clinical distinction is from ganglion cyst (transilluminates, fluctuant) and foreign-body granuloma (history of penetrating injury).
Clinical Assessment
- Duration: months to years of slow growth
- Pain: usually minimal or painless mass
- Location: volar surface of digits
- Function: may cause clicking or limited flexion if large
- Prior history: ask about previous excisions (recurrent nodules)
- Duration: months to years of insidious onset
- Pain: progressive, aching joint pain
- Swelling: recurrent effusions, often blood-stained on aspiration
- Mechanical symptoms: locking, catching, giving way
- Prior surgery: ask about previous synovectomy (recurrence common)
Recurrent unexplained haemarthrosis in a young-to-middle-aged adult with no trauma history must raise suspicion for diffuse TGCT until proven otherwise. The triad of chronic joint swelling, bloody aspiration, and absence of trauma or coagulopathy warrants urgent MRI with gradient-echo sequences.
- Joint Fluid
- Brown / blood-stained
- MRI Signal
- Low T1 + low T2 + blooming
- Key Discriminator
- Diffuse synovial thickening with haemosiderin
- Joint Fluid
- Not usually aspirated
- MRI Signal
- Circumscribed low-T2 nodule
- Key Discriminator
- Well-defined mass on tendon sheath, no joint involvement
- Joint Fluid
- Clear or slightly blood-stained
- MRI Signal
- Multiple loose bodies (calcified rings)
- Key Discriminator
- Radiodense loose bodies on X-ray; T2 bright cartilage nodules
- Joint Fluid
- Variable
- MRI Signal
- Heterogeneous, often near joint but extra-articular
- Key Discriminator
- Aggressive features, calcifications, distant from joint line
- Joint Fluid
- Frank blood
- MRI Signal
- Low T2 haemosiderin but pan-articular destruction
- Key Discriminator
- History of bleeding disorder, multiple joints affected
- Joint Fluid
- Negatively birefringent crystals
- MRI Signal
- Low T2 but no blooming artefact
- Key Discriminator
- Serum urate, clinical gout history, no haemosiderin
- Joint Fluid
- Straw-coloured
- MRI Signal
- Low T2 but no blooming
- Key Discriminator
- Systemic amyloidosis, bilateral, perarticular deposition
Both produce haemosiderin-laden synovium with low T2 signal. However, haemophiliac arthropathy affects multiple joints in a patient with a known bleeding disorder and shows pan-articular destruction (not focal villonodular masses). TGCT is monoarticular without a coagulopathy history. The blooming artefact is present in both but the distribution and clinical context are different.
Investigations
Imaging Protocol
Views: AP and lateral of affected joint; dedicated views for digits
Localised type: usually normal; may show soft-tissue density or pressure remodelling of adjacent bone
Diffuse type: periarticular soft-tissue swelling, subchondral cysts, bone erosions with sclerotic margins (preserved joint space early), late joint space narrowing
Look for: absence of calcification (distinguishes from synovial chondromatosis and synovial sarcoma)
Sequences: T1, T2, fat-saturated T2, proton density, gradient-echo (GRE)
Hallmark findings: low T1 signal (haemosiderin), low T2 signal (haemosiderin and fibrosis), blooming artefact on GRE sequences
Localised: well-circumscribed nodule adjacent to tendon sheath, low T2 signal, homogeneous enhancement
Diffuse: extensive infiltrative synovial thickening, villonodular pattern, joint effusion, bone erosions, low T2 signal with blooming
Staging: assess extent — anterior and posterior compartments, extra-articular extension, popliteal involvement
Indication: atypical presentation, rapid growth, concern for sarcoma, or prior to pexidartinib initiation
Technique: core needle biopsy under imaging guidance, or arthroscopic biopsy
Histology required before systemic therapy: confirm diagnosis and exclude synovial sarcoma
Gradient-echo MRI is the critical sequence for TGCT. Haemosiderin causes magnetic susceptibility artefact that produces dramatic signal loss (blooming) on GRE sequences. This is absent on standard spin-echo T1 and T2. If you suspect TGCT and the MRI protocol does not include GRE, request it specifically. The blooming artefact is the imaging equivalent of Prussian blue staining on histology — it proves haemosiderin is present.
A common viva follow-up is "how does the pathologist confirm it, and how is it told apart from giant cell tumour of bone or a sarcoma?" The key is to separate the two cell populations:
- The neoplastic large mononuclear (dendritic-like) cells: these carry the CSF1 rearrangement and are the diagnostic population. They are typically desmin positive (a dendritic-cell pattern, not smooth-muscle) and clusterin positive; a subset express CD163/CD68. CSF1 over-expression can be shown by in-situ hybridisation, and CSF1 rearrangement by FISH in difficult cases.
- The recruited reactive cells (the bulk): small mononuclear histiocytes and osteoclast-like multinucleated giant cells that are CD68 / CD163 positive (macrophage markers), plus haemosiderin-laden macrophages (Prussian blue positive) and foam (xanthoma) cells.
- Telling it apart: from giant cell tumour of bone (the giant cells look identical, but GCT of bone is centred in epiphyseal bone and carries the H3F3A G34W mutation, not a CSF1 rearrangement); from synovial sarcoma (monophasic spindle cells, SS18-SSX / t(X;18), TLE1 positive); and benign TGCT lacks the marked atypia, atypical mitoses and necrosis of a malignant lesion.
Exam point: TGCT shows a CSF1-driven desmin/clusterin-positive dendritic neoplastic cell within a reactive population of CD68/CD163-positive macrophages, osteoclast-like giant cells and haemosiderin - and the differentiating molecular tests are H3F3A (GCT of bone) and SS18-SSX (synovial sarcoma).
Management Algorithm
Localised TGCT: Marginal Excision
Goal: Complete excision with preservation of surrounding structures (neurovascular bundles, tendons, joint capsule)
Treatment Protocol
Imaging: MRI to delineate extent and relationship to tendons, neurovascular bundles
Counselling: 5-15 percent recurrence rate, transient stiffness expected, physiotherapy post-operatively
Marking: palpate and mark the nodule pre-operatively (may be difficult to find under anaesthesia)
Approach: extensile zigzag (Bruner) or mid-lateral incision over the nodule
Dissection: identify and protect neurovascular bundles, expose tendon sheath, dissect circumferentially around the mass
Excision: remove the nodule with a thin rim of attached tendon sheath (marginal excision)
Send: entire specimen for histology — confirm diagnosis and exclude sarcoma
Splinting: brief immobilisation (3-5 days), then early active mobilisation
Therapy: tendon gliding exercises, scar massage, gradual return to full activity
Follow-up: wound check at 2 weeks, review histology, assess for recurrence at 3 and 12 months
Re-excision: repeat marginal excision is standard for localised recurrence
Re-examine histology: ensure diagnosis is correct and no atypical features
Adjuvant: not routinely indicated for localised type
The most common site for recurrence after localised TGCT excision is the original surgical bed, usually due to incomplete excision or satellite nodules missed at the index procedure. Meticulous circumferential dissection with a thin cuff of normal tendon sheath minimises recurrence without sacrificing tendon function.
Complications
- Incidence
- 5-15 percent after excision
- Risk Factors
- Incomplete excision, satellite nodules
- Management
- Re-excision with margin of normal tissue
- Incidence
- 20-50 percent after synovectomy
- Risk Factors
- Incomplete synovectomy, posterior compartment disease
- Management
- Repeat synovectomy, adjuvant radiotherapy, pexidartinib
- Incidence
- Common in long-standing diffuse TGCT
- Risk Factors
- Chronic bone erosion, delayed diagnosis
- Management
- Joint replacement if end-stage (counselling for recurrence risk)
- Incidence
- Common after extensive synovectomy
- Risk Factors
- Multiple procedures, prolonged immobilisation
- Management
- Early ROM, CPM, intensive physiotherapy
- Incidence
- Less than 5 percent (digit excisions)
- Risk Factors
- Recurrent surgery with scarred anatomy
- Management
- Meticulous dissection, identify structures early
- Incidence
- Elevated LFTs in approximately 10-15 percent
- Risk Factors
- Pre-existing liver disease, concurrent hepatotoxins
- Management
- LFT monitoring, dose reduction or discontinuation
The most significant long-term complication of diffuse TGCT is progressive joint destruction from bone erosions and secondary osteoarthritis. This is preventable with early diagnosis and appropriate management. Delayed diagnosis is common — the mean time from symptom onset to TGCT diagnosis is approximately 2-4 years for diffuse disease. A high index of suspicion for any chronic monoarticular haemarthrosis with bloody aspirate is essential.
Outcomes and Prognosis
- Treatment
- Marginal excision
- Recurrence Rate
- 5-15 percent
- Long-term Function
- Excellent — normal hand function in majority
- Treatment
- Combined synovectomy
- Recurrence Rate
- 20-30 percent
- Long-term Function
- Good to fair — some residual stiffness common
- Treatment
- Arthroscopic anterior synovectomy
- Recurrence Rate
- 40-50 percent
- Long-term Function
- Fair — high recurrence, often needs revision
- Treatment
- Pexidartinib
- Recurrence Rate
- N/A (suppression, not cure)
- Long-term Function
- Good symptom control while on treatment; tumour regrows if stopped
- Treatment
- Joint replacement after tumour control
- Recurrence Rate
- Recurrence around prosthesis possible
- Long-term Function
- Variable — functional improvement, monitor for recurrence
Best prognosis: Localised type, first-time excision, complete margins, digit location
Poor prognosis: Diffuse type, extra-articular extension, multiple prior recurrences, hip or ankle location (harder to access for complete synovectomy)
Key concept: TGCT does not metastasise — it is a locally aggressive neoplasm. However, the morbidity comes from local destruction, functional impairment, and the morbidity of repeated surgical interventions.
Conventional TGCT does not metastasise, but a complete answer must acknowledge the rare malignant tenosynovial giant cell tumour (malignant diffuse-type giant cell tumour) - because it behaves like a sarcoma and the over-simplification "TGCT is always benign" is a trap:
- Definition (Bertoni): either a sarcoma arising in conjunction with a benign TGCT, or a recurrence of a previously typical TGCT as a high-grade sarcoma. The malignant areas show frank cytological atypia, enlarged nucleoli, atypical mitoses, necrosis and a high mitotic rate, with sheets of the mononuclear cells losing the usual admixed giant cells.
- Who/where: typically older adults with large, diffuse, multiply-recurrent lower-limb lesions (knee, foot/ankle, hip) - malignant change in a long-standing or repeatedly recurrent diffuse TGCT.
- Behaviour: genuinely metastasises (lung and regional lymph nodes) and carries a poor prognosis - this is the exception to the "no metastasis" rule.
- Management: wide (oncological) resection rather than synovectomy, regional nodal assessment, and consideration of (neo)adjuvant chemotherapy/radiotherapy in a sarcoma multidisciplinary unit; not a disease for arthroscopic synovectomy or pexidartinib alone.
Exam point: suspect malignant TGCT when a diffuse lesion is large, recurrent, in an older patient, rapidly enlarging, or shows necrosis/atypia/high mitotic activity on biopsy - it can metastasise and needs sarcoma-style wide resection, unlike conventional TGCT.
Guidelines, Registries & Global Practice
- Localised TGCT: most common in the hand, seen across all populations and regions
- Diffuse TGCT: rare tumour, approximately 1-2 per million person-years, no strong geographic or ethnic predilection
- Age distribution: 30-50 years peak, slight female predominance for diffuse type
- Joint distribution: knee overwhelmingly most common for diffuse type (approximately 80 percent)
- High-resource: MRI with GRE sequences standard; arthroscopic combined synovectomy; pexidartinib available through REMS programmes
- Limited-resource: ultrasound-guided diagnosis; open synovectomy more common; pexidartinib access limited by cost
- Universal principle: diagnosis relies on characteristic MRI findings; complete surgical excision remains the gold standard regardless of setting
- Radiotherapy: adjuvant EBRT more commonly used in Europe and Asia than North America for multiply recurrent diffuse TGCT
- Diagnosis
- MRI with GRE; biopsy if atypical; histology mandatory before systemic therapy
- Surgical Treatment
- Complete synovectomy for diffuse; marginal excision for localised
- Medical Therapy
- Pexidartinib for symptomatic diffuse TGCT not amenable to surgery
- Diagnosis
- MRI staging; core biopsy before treatment decisions
- Surgical Treatment
- Combined anterior + posterior synovectomy; adjuvant RT for high-risk
- Medical Therapy
- Pexidartinib or nilotinib (off-label); clinical trial enrolment encouraged
- Diagnosis
- MRI with GRE sequences; aspirate for bloody effusion
- Surgical Treatment
- Surgical excision; combined approach for diffuse knee disease
- Medical Therapy
- Pexidartinib with REMS programme; LFT monitoring mandatory
- Diagnosis
- Unified nomenclature: TGCT (localised and diffuse); CSF1 rearrangement testing
- Surgical Treatment
- Classification guide, treatment recommendations per local practice
- Medical Therapy
- Recognises CSF1R-targeted agents as therapeutic option
There is no dedicated global arthroplasty or implant registry for TGCT as it is not an implant-driven disease. The evidence base consists of the ENLIVEN randomised trial (pexidartinib), multiple institutional surgical series, and systematic reviews of recurrence rates. The WHO 2020 classification unified the nomenclature under "tenosynovial giant cell tumour" with localised and diffuse subtypes, moving away from PVNS and GCT-TS terminology in pathology reporting — though clinicians still widely use the historical terms.
Record in every suspected TGCT case:
- MRI performed with gradient-echo sequences (state whether blooming artefact present or absent)
- Histological confirmation before initiating systemic therapy
- Pre-operative counselling regarding recurrence rates (5-15 percent localised, 20-50 percent diffuse)
- For pexidartinib: baseline LFTs, REMS enrolment documentation, monthly monitoring plan
- Multidisciplinary discussion documented (radiology, pathology, orthopaedic oncology)
TGCT is a rare tumour where delayed diagnosis (mean 2-4 years) and incomplete surgery are recurring themes in medicolegal claims. Thorough documentation of staging, counselling, and surgical planning is essential.
Controversies & Areas of Uncertainty
Arthroscopic combined anterior and posterior synovectomy is increasingly favoured for diffuse knee TGCT, but no randomised trial has directly compared arthroscopic versus open approaches for recurrence rates. Proponents argue arthroscopy allows superior visualisation of posterior recesses; others contend open surgery enables more thorough clearance. Current evidence from institutional series suggests comparable outcomes when arthroscopic technique is meticulous.
External beam radiotherapy (30-40 Gy) is used in some centres as adjuvant treatment after synovectomy for high-risk diffuse TGCT, particularly after multiple recurrences or incomplete resection. Evidence comes from retrospective series showing reduced recurrence, but there is no randomised trial. Concerns include joint stiffness, radiation arthropathy, and theoretical risk of secondary malignancy. Practice varies significantly between continents.
The ENLIVEN extension data show tumour regrowth upon discontinuation of pexidartinib in most patients, suggesting chronic suppressive therapy may be needed. However, long-term safety data beyond 3-4 years are limited, and the hepatotoxicity risk necessitates ongoing monitoring. The optimal duration of therapy — continuous, intermittent, or taper-based — remains undefined.
For end-stage degenerative change secondary to diffuse TGCT, total joint replacement (particularly TKA) is a reasonable option. However, the risk of TGCT recurrence in the prosthetic joint is not well quantified. Some surgeons recommend a disease-free interval before arthroplasty; others proceed with concurrent synovectomy and replacement. No consensus guideline exists.
MCQ Practice Points
Q: What is the molecular driver of TGCT and what is its mechanism? A: CSF1 overexpression due to a translocation (most commonly t(1;2)(p13;q35)) that fuses CSF1 to the COL6A3 promoter. The neoplastic cells (small minority) overexpress CSF1, which recruits CSF1R-expressing macrophages (the bulk of the tumour). This paracrine recruitment mechanism is the basis for CSF1R-targeted therapy with pexidartinib.
Q: What MRI finding is pathognomonic for TGCT? A: Blooming artefact on gradient-echo (GRE) sequences. Haemosiderin within the proliferative synovium causes magnetic susceptibility artefact, producing dramatic signal loss on GRE that appears larger and darker than on spin-echo sequences. The synovium is low signal on both T1 and T2-weighted images. This triad (low T1, low T2, blooming GRE) is characteristic.
Q: How do localised and diffuse TGCT differ in behaviour and management? A: Localised TGCT (formerly GCT of tendon sheath): well-circumscribed digital nodule, marginal excision, 5-15 percent recurrence. Diffuse TGCT (formerly PVNS): infiltrative synovial proliferation of large joints, combined anterior and posterior synovectomy, 20-50 percent recurrence. Pexidartinib is reserved for unresectable diffuse disease.
Q: When is pexidartinib indicated and what monitoring is required? A: Symptomatic diffuse TGCT not amenable to surgical improvement. It is a CSF1R tyrosine-kinase inhibitor that blocks macrophage recruitment. Monitoring requires LFTs at baseline, weekly for the first 2 months, then monthly due to a black-box warning for hepatotoxicity. It is suppressive, not curative — tumour regrows if discontinued.
Q: A 30-year-old presents with recurrent bloody knee aspirates. Name three differential diagnoses and the key discriminator for each. A: Diffuse TGCT — MRI blooming artefact, monoarticular. Haemophiliac arthropathy — polyarticular, known bleeding disorder. Synovial chondromatosis — radiodense loose bodies on X-ray, T2-bright cartilage nodules. Synovial sarcoma — aggressive imaging features, heterogeneous enhancement, often extra-articular.
Q: What is the main driver of recurrence in diffuse TGCT and how is it minimised? A: Incomplete synovectomy — leaving residual disease in the posterior compartment is the most common cause of recurrence in knee TGCT. A combined anterior and posterior synovectomy reduces recurrence from approximately 50 percent (anterior only) to approximately 20-30 percent (combined approach). Adjuvant radiotherapy may be considered for multiply recurrent or high-risk cases.
Clinical Imaging
Imaging Features of TGCT
Imaging is critical for distinguishing localised from diffuse TGCT and planning surgical approach. Plain radiographs may show periarticular lucency, joint space narrowing, or bone erosions in advanced diffuse disease. MRI is the gold standard modality: the hallmark is low signal on both T1- and T2-weighted sequences due to haemosiderin deposition within the proliferative synovium. Gradient-echo (GRE) sequences demonstrate blooming artefact — magnetic susceptibility effect that makes haemosiderin deposits appear larger and darker than on spin-echo sequences — which is virtually pathognomonic for TGCT.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 34-year-old woman presents with a 2-year history of recurrent swelling of her right knee. She has had three episodes of large, blood-stained knee effusions aspirated at her GP. There is no history of trauma or bleeding disorder. Examination reveals a moderate effusion, diffuse synovial thickening, and limited flexion to 100 degrees. X-rays show preserved joint space with subchondral cysts in the medial femoral condyle. What is your differential diagnosis, investigation, and management plan?”
“A 42-year-old man presents with a 1-year history of a slowly enlarging, firm, non-tender mass on the volar surface of his right index finger at the level of the proximal phalanx. It does not transilluminate. He has had one prior excision of a similar lump at the same site 3 years ago which recurred. He is otherwise well. What is the diagnosis, how do you investigate, and what is your management?”
Pathogenesis
- CSF1 overexpression from t(1;2)(p13;q35) translocation (CSF1-COL6A3 fusion)
- Neoplastic minority overexpresses CSF1, recruits CSF1R-positive macrophage majority
- TGCT is a true neoplasm, not an inflammatory condition (WHO 2020 unified nomenclature)
- Does not metastasise — locally aggressive only
Classification
- Localised (GCT-TS): well-circumscribed, digits, marginal excision, 5-15 percent recurrence
- Diffuse (PVNS): infiltrative, large joints (knee 80 percent), synovectomy, 20-50 percent recurrence
- Extra-articular: breaches capsule, highest recurrence, widest excision needed
- WHO 2020 unified both under TGCT — PVNS and GCT-TS are now obsolete pathological terms
Imaging
- Low T1 + low T2 + blooming on GRE = haemosiderin = pathognomonic for TGCT
- Gradient-echo sequence is mandatory — blooming artefact distinguishes from other synovial masses
- X-rays: subchondral cysts with sclerotic margins, preserved joint space early, no calcification
- MRI staging: map anterior and posterior compartments and extra-articular extension before surgery
Surgical Management
- Localised: marginal excision with cuff of tendon sheath, protect neurovascular bundles
- Diffuse knee: combined anterior + posterior synovectomy (arthroscopic or open)
- Anterior-only synovectomy is inadequate — recurrence approaches 50 percent
- Adjuvant radiotherapy considered for multiply recurrent or incomplete resection
Pexidartinib
- CSF1R tyrosine-kinase inhibitor — blocks macrophage recruitment
- FDA approved 2019 for symptomatic diffuse TGCT not amenable to surgery
- Black-box warning: hepatotoxicity — REMS programme, monthly LFT monitoring required
- Suppressive not curative — tumour regrows upon discontinuation
Evidence Base and Key Trials
Pexidartinib for treatment of advanced tenosynovial giant cell tumour (ENLIVEN)
- Randomised, double-blind, placebo-controlled phase 3 trial of pexidartinib in 120 patients with symptomatic diffuse TGCT
- At 24 weeks, 39 percent of pexidartinib patients achieved 50 percent or greater tumour volume reduction versus 0 percent with placebo
- Significant improvements in pain, range of motion, and physical function scores
- Two patients developed serious hepatotoxicity leading to a black-box warning and REMS programme
A landscape effect in tenosynovial giant-cell tumor from activation of CSF1 expression by a translocation in a minority of tumor cells
- Identified CSF1 overexpression as the driver of TGCT via expression profiling
- Demonstrated the t(1;2)(p13;q35) translocation fusing CSF1 to COL6A3
- Showed that only a minority of tumour cells carry the translocation, with the vast majority being recruited CSF1R-positive macrophages
- Established the paracrine recruitment model that underpins CSF1R-targeted therapy
The effect of surgical synovectomy and radiotherapy on the rate of recurrence of pigmented villonodular synovitis of the knee: an individual patient meta-analysis
- Systematic review and meta-analysis of recurrence rates after surgical treatment of diffuse TGCT
- Combined anterior and posterior synovectomy had significantly lower recurrence than anterior-only approach
- Adjuvant radiotherapy reduced recurrence in high-risk diffuse cases
- Hip and ankle locations had higher recurrence rates than knee, attributed to surgical access difficulty
Treatment of tenosynovial giant cell tumor and pigmented villonodular synovitis
- Comprehensive review establishing TGCT as a neoplastic process driven by CSF1 overexpression rather than an inflammatory condition
- Outlined the spectrum from localised to diffuse disease with differing biological behaviour
- Reviewed surgical and emerging medical management strategies
- Emphasised the importance of complete synovectomy and the role of targeted therapy
Long-term outcomes of pexidartinib in tenosynovial giant cell tumors
- Long-term open-label extension data from the ENLIVEN trial with median follow-up exceeding 3 years
- Sustained tumour volume reductions and symptom improvement in patients continuing pexidartinib
- Hepatotoxicity events occurred early (within first 2 months) and were manageable with monitoring and dose adjustments
- Tumour regrowth observed upon treatment discontinuation, suggesting chronic therapy may be needed