MSIS/ICM Criteria | DAIR vs Two-Stage | Organism-Specific Treatment
TIMEFRAME CLASSIFICATION
Critical Must-Knows
- MSIS/ICM 2018 criteria - major and minor criteria for PJI diagnosis
- Two-stage revision is gold standard for chronic PJI (90% success)
- DAIR indications: acute (under 3 weeks), stable implant, sensitive organism
- Never use cement spacer as permanent implant - toxicity risk
- Organism identification critical - culture before antibiotics when possible
Clinical Pearls
- "MSIS 2018: 1 major criterion OR 4 minor criteria = definite PJI
- "Synovial alpha-defensin has best diagnostic accuracy (sens 97%, spec 97%)
- "DAIR success under 50% - use strict criteria
- "Biofilm formation makes eradication without removal very difficult
- "S. aureus and resistant organisms require more aggressive treatment
Critical PJI Exam Points
Know MSIS Criteria
Major criteria (1 equals PJI): two positive cultures of same organism OR sinus tract communicating with joint. Minor criteria (4 equals PJI): elevated serum markers, elevated synovial markers, positive histology, single positive culture. This is exam gold.
DAIR Is Not Magic
DAIR success is under 50% overall. Only use in acute infections (under 3 weeks), stable implants, and sensitive organisms. Most chronic PJI requires implant removal. Choosing wrong treatment leads to failure and patient harm.
Two-Stage Gold Standard
Two-stage revision remains the gold standard for chronic PJI with success rates over 90% for sensitive organisms. Stage 1: resection, spacer, antibiotics. Stage 2: reimplantation after infection clearance (typically 6-12 weeks).
Culture Before Antibiotics
Always attempt to identify the organism before starting antibiotics. Hold antibiotics for 2 weeks before aspiration if possible. Culture-negative PJI has worse outcomes - harder to target treatment.
Quick Decision Guide - PJI Treatment Algorithm
| Timing | Clinical Features | Implant Status | First-Line Treatment |
|---|---|---|---|
| Acute postop (under 3 weeks) | Acute symptoms, single organism | Well-fixed components | DAIR (debridement, antibiotics, implant retention) |
| Subacute/chronic (over 3 weeks) | Indolent symptoms or late presentation | Any implant fixation | Two-stage revision (resection, spacer, reimplantation) |
| Acute hematogenous (over 2 years) | Acute symptoms, identifiable source | Well-fixed, no prior infection | DAIR possible if under 3 weeks from symptom onset |
| Any timing | Resistant organism (MRSA, fungi) | Any implant status | Two-stage or resection arthroplasty (salvage) |
| Any timing | Sinus tract present | Any implant status | Implant removal mandatory (two-stage or resection) |
MSIS 2018 - MMSIS 2018 - Major Criteria
| S | Sinus tract Communicating with prosthesis |
| I | Identical organisms Two positive cultures of same organism |
| N | Need only ONE Single major criterion = definite PJI |
| U | Unambiguous diagnosis Clear-cut infection if present |
| S | Sufficient alone Don't need minor criteria if major present |
| S | Sinus tract Communicating with prosthesis | U | Unambiguous diagnosis Clear-cut infection if present |
| I | Identical organisms Two positive cultures of same organism | S | Sufficient alone Don't need minor criteria if major present |
| N | Need only ONE Single major criterion = definite PJI |
Hook:SINUS - one major criterion is sufficient for definite PJI diagnosis
PJIMSIS 2018 - Minor Criteria (Need 4 for Definite PJI)
| M | Markers elevated serum CRP over 10 mg/L AND ESR over 30 mm/hr |
| I | Intra-articular markers Synovial WBC, PMN%, alpha-defensin, LE |
| N | Neutrophils on histology Over 10 PMN per HPF (5 fields at 400x) |
| O | One positive culture Single positive periprosthetic culture |
| R | Requires FOUR total Need 4 minor criteria for definite PJI |
| M | Markers elevated serum CRP over 10 mg/L AND ESR over 30 mm/hr | O | One positive culture Single positive periprosthetic culture |
| I | Intra-articular markers Synovial WBC, PMN%, alpha-defensin, LE | R | Requires FOUR total Need 4 minor criteria for definite PJI |
| N | Neutrophils on histology Over 10 PMN per HPF (5 fields at 400x) |
Hook:MINOR - need 4 minor criteria to diagnose PJI without major criteria
DAIR - SDAIR - Strict Criteria for Success
| D | Duration under 3 weeks Acute infection or acute hematogenous |
| A | Adequate debridement Thorough synovectomy, all modular exchange |
| I | Implant well-fixed Stable components, no loosening |
| R | Right organism Sensitive organism (avoid MRSA, resistant) |
| D | Duration under 3 weeks Acute infection or acute hematogenous | I | Implant well-fixed Stable components, no loosening |
| A | Adequate debridement Thorough synovectomy, all modular exchange | R | Right organism Sensitive organism (avoid MRSA, resistant) |
Hook:DAIR has strict indications - if not met, use two-stage revision
PJITWO-STAGE - Gold Standard for Chronic PJI
| T | Take out implants Complete component removal, radical debridement |
| W | Wait for clearance 6-12 weeks antibiotics, normalize markers |
| O | Organism-specific antibiotics IV then oral based on sensitivities |
| S | Spacer placement Antibiotic-impregnated cement spacer (temporary) |
| T | Test before reimplantation Aspirate off antibiotics, check markers |
| A | After clearance, reimplant Stage 2 surgery with new components |
| G | Good success rate 90%+ for sensitive organisms |
| E | Expect long treatment Total process 3-6 months minimum |
| T | Take out implants Complete component removal, radical debridement | S | Spacer placement Antibiotic-impregnated cement spacer (temporary) | G | Good success rate 90%+ for sensitive organisms |
| W | Wait for clearance 6-12 weeks antibiotics, normalize markers | T | Test before reimplantation Aspirate off antibiotics, check markers | E | Expect long treatment Total process 3-6 months minimum |
| O | Organism-specific antibiotics IV then oral based on sensitivities | A | After clearance, reimplant Stage 2 surgery with new components |
Hook:TWO-STAGE is comprehensive and time-intensive but has best success rates
Overview and Epidemiology
Periprosthetic joint infection (PJI) is one of the most devastating complications following total hip arthroplasty. Despite advances in prevention, PJI remains a leading cause of early revision and has profound impact on patient outcomes.
Epidemiology:
- Primary THA: 1-2% infection rate
- Revision THA: 3-5% infection rate (higher risk)
- Increasing incidence despite improved prevention strategies (likely due to higher-risk patients)
- Costs: PJI treatment costs 3-4 times more than primary arthroplasty
Risk factors:
Modifiable:
- Obesity (BMI over 35)
- Diabetes (HbA1c over 7%)
- Smoking
- Malnutrition (albumin under 3.5 g/dL)
- Immunosuppression (steroids, biologics)
- Active infection elsewhere
Non-modifiable:
- Rheumatoid arthritis
- Prior surgery at same site
- Male gender
- Advanced age
These patient factors should trigger optimization protocols preoperatively.
The Biofilm Problem
Biofilm formation is the key pathophysiology of PJI. Bacteria adhere to implant surface and produce extracellular matrix (biofilm). This protects bacteria from antibiotics (1000x higher MIC) and immune system. This is why implant removal is usually necessary for chronic PJI - antibiotics cannot penetrate established biofilm.
Pathophysiology and Microbiology
Routes of infection:
-
Direct inoculation (most common for early PJI)
- Intraoperative contamination
- Postoperative wound complications
- Accounts for majority of early infections
-
Hematogenous spread (late PJI)
- Dental procedures
- Urinary tract infections
- Skin/soft tissue infections
- GI sources (endoscopy, diverticulitis)
-
Contiguous spread (rare)
- Adjacent osteomyelitis
- Septic hip (pre-existing)
Biofilm development stages:
- Bacteria adhere to implant surface
- Mediated by surface proteins and conditioning layer
- Critical window for prevention
- Bacterial multiplication
- Microcolony formation
- Begin extracellular matrix production
- Mature biofilm with complex architecture
- Protective extracellular matrix
- Drastically reduced antibiotic penetration
- Bacteria shed from biofilm
- Can seed new locations
- Chronic inflammation and bone resorption
Biofilm Timeframe
Biofilm maturation takes 3-4 weeks. This is why DAIR (implant retention) only works in acute infections (under 3 weeks). After biofilm matures, antibiotics cannot effectively penetrate, and implant removal becomes necessary.
Organism-specific considerations:
Organism Characteristics and Treatment Implications
| Organism | Virulence | Biofilm | Treatment Challenge |
|---|---|---|---|
| S. aureus (MSSA) | High | Strong | Aggressive, often needs implant removal |
| MRSA | High | Very strong | Two-stage mandatory, prolonged antibiotics |
| CoNS (S. epidermidis) | Low | Very strong | Indolent presentation, strong biofilm producer |
| Streptococcus | Moderate | Weak | Better success with DAIR if caught early |
| Enterococcus | Low-Moderate | Moderate | Often resistant, difficult to treat |
| Gram-negatives | Variable | Variable | Often resistant, polymicrobial common |
| Fungi (Candida) | Low | Moderate | Requires antifungals, often two-stage or resection |
Classification Systems
Temporal classification (Tsukayama/Fitzgerald & Steinberg):
| Type | Timing | Presentation | Typical Organisms |
|---|---|---|---|
| I. Early postoperative | Under 3 months | Acute wound inflammation | S. aureus, Gram-negatives |
| II. Delayed/chronic | 3-24 months | Indolent, pain, loosening | CoNS, P. acnes |
| III. Late hematogenous | Over 24 months | Acute symptoms, well-fixed implant | S. aureus, Streptococcus |
| IV. Positive intraoperative | During revision | Unexpected positive cultures | Variable |
Classification Guides Treatment
The temporal classification directly guides treatment choice. Early (Type I) and acute hematogenous (Type III, if under 3 weeks symptoms) may be suitable for DAIR. Delayed/chronic (Type II) almost always requires two-stage revision.
McPherson staging (host and extremity factors):
A (Good host):
- Healthy, no comorbidities
- Good nutrition, no immunosuppression
- Best prognosis
B (Compromised host):
- Diabetes, obesity, smoking
- Local wound issues
- Intermediate prognosis
C (Severe compromise):
- Significant immunosuppression
- Active malignancy, ESRD
- Multiple failed surgeries
- Poor prognosis, consider salvage
Host grade affects antibiotic duration and treatment aggressiveness.
Clinical Presentation and Assessment
Clinical presentation varies by timing:
Clinical Presentations
| Timing | Symptoms | Key Features |
|---|---|---|
| Acute (under 3 months) | Fever, wound drainage, erythema | Clear signs of infection, systemic symptoms |
| Subacute (3-24 months) | Pain, stiffness, mechanical symptoms | May mimic aseptic loosening, subtle presentation |
| Chronic (over 24 months, hematogenous) | Acute pain in previously well-functioning THA | Identifiable infection source elsewhere |
History taking:
- Timing of symptoms relative to surgery
- Previous function of the THA (was it ever pain-free?)
- Wound complications postoperatively
- Recent infections or procedures (dental, UTI)
- Risk factors: diabetes, immunosuppression, prior surgery
- Prior antibiotic use (affects culture yield)
Physical examination:
Sinus Tract = Infection
A sinus tract communicating with the prosthesis is pathognomonic for infection (MSIS major criterion). Even without other signs, this mandates treatment for PJI.
Examination findings:
- Wound erythema, warmth, swelling
- Sinus tract or wound drainage
- Pain with ROM (even passive)
- Reduced ROM (contracture from chronic inflammation)
- Previous surgical scars
- Systemic signs (fever, sepsis in severe cases)
Subtle Chronic PJI
Chronic PJI can mimic aseptic loosening. Any patient with painful THA (especially if never pain-free postop or pain after pain-free interval) should be worked up for infection. Don't assume aseptic loosening without ruling out PJI.
Differential diagnosis of the painful THA:
Differential Diagnosis - Painful THA (Distinguishing PJI)
| Diagnosis | Key Features | Discriminating Test |
|---|---|---|
| Periprosthetic joint infection | Rest pain, never pain-free, sinus/drainage, raised ESR/CRP | Aspiration (cell count, alpha-defensin, culture); MSIS score 6 or more |
| Aseptic loosening | Start-up/activity pain, progressive radiolucent lines, normal CRP | Normal aspiration cell count and markers; radiographic migration |
| Adverse local tissue reaction (MoM/trunnionosis) | Groin pain, effusion, metal-on-metal or large-head MoP bearing | Serum cobalt/chromium, MARS-MRI showing pseudotumour; bland aspirate |
| Instability / recurrent dislocation | Mechanical giving-way, positional pain, dislocation history | Radiographs/dynamic exam; markers normal |
| Periprosthetic fracture | Acute pain after trauma, deformity, inability to weight-bear | Radiographs (Vancouver classification); markers normal |
| Referred pain (spine, vascular, hernia) | Pain not reproduced by hip movement, neuro/vascular signs | Spinal/vascular workup; normal hip aspiration and markers |
Always Exclude Infection First
Before attributing a painful THA to a mechanical cause, exclude PJI with serum ESR/CRP and, if elevated or suspicion is high, off-antibiotic aspiration. Missing low-grade infection before a revision converts a one-stage mechanical revision into a failed, contaminated reconstruction.
Diagnostic Investigations
MSIS/ICM 2018 Criteria for PJI:
Major criteria (ONE required for definite PJI):
- Two positive cultures of the same organism from separate samples
- Sinus tract communicating with the prosthesis
Minor criteria (FOUR required for definite PJI if no major criteria):
| Minor Criterion | Threshold | Points if met |
|---|---|---|
| Elevated serum CRP | Over 10 mg/L | 1 |
| Elevated serum ESR | Over 30 mm/hr | 1 |
| Elevated synovial WBC | Over 3000 cells/µL | 2 |
| Elevated synovial PMN% | Over 70% | 1 |
| Positive alpha-defensin | Qualitative positive | 3 |
| Positive leukocyte esterase | ++ or +++ | 3 |
| Elevated synovial CRP | Over 6.9 mg/L | 1 |
| Single positive culture | One organism | 2 |
| Positive histology | Over 10 PMN/HPF (5 HPF) | 3 |
Scoring System
The 2018 MSIS criteria use a scoring system: score of 6 or more = definite PJI. Alpha-defensin, LE (at ++ or +++), and histology are worth 3 points each. Synovial WBC over 3000 is worth 2 points. This is exam-critical knowledge.
Diagnostic workup algorithm:
First-line blood tests:
- ESR (over 30 mm/hr suggestive)
- CRP (over 10 mg/L suggestive)
- CBC with differential (leukocytosis less sensitive)
- D-dimer (research, not yet standard)
Limitations:
- ESR/CRP can be elevated in aseptic inflammation
- Sensitivity 80-90%, specificity 70-80%
- More useful for monitoring treatment response
Utility:
- Elevated markers prompt further workup
- Normal markers don't rule out PJI (especially low-virulence)
- Trending markers guides treatment response
Serum markers are screening tests but not diagnostic alone.
Diagnostic algorithm summary:
- Clinical suspicion → Serum ESR/CRP
- If elevated or high suspicion → Hip aspiration (off antibiotics if possible)
- Aspiration: cell count, culture, alpha-defensin
- Apply MSIS criteria for diagnosis
- If diagnosis confirmed → Plan treatment based on timing and organism
- Intraoperative cultures confirm and guide antibiotic therapy
Management Algorithm
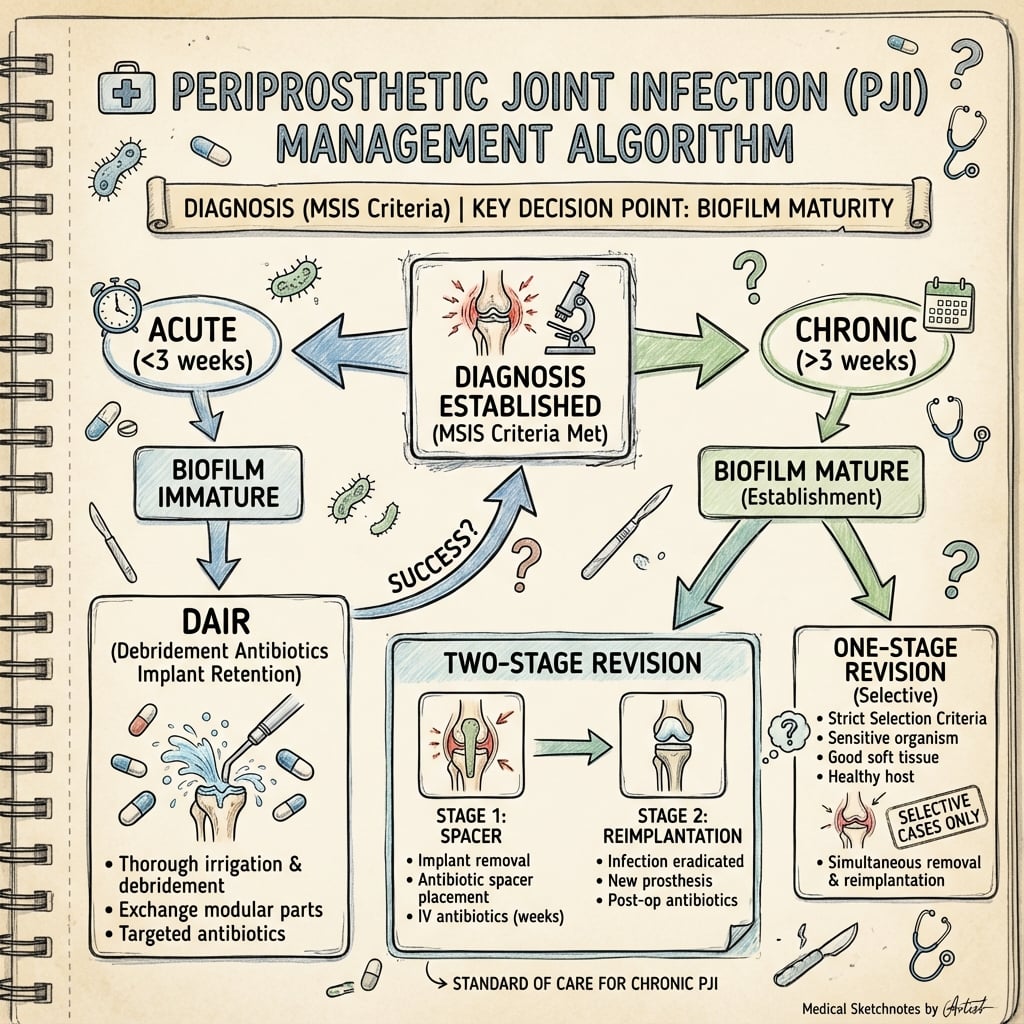
PJI treatment options:
-
Debridement, Antibiotics, Implant Retention (DAIR)
- Acute infection (under 3 weeks)
- Stable implant
- Sensitive organism
-
One-stage revision
- Single surgery: remove components, debride, reimplant
- Selective use (Europe more than US)
- Known sensitive organism
-
Two-stage revision (GOLD STANDARD)
- Stage 1: resection, debridement, spacer
- Antibiotics 6-12 weeks
- Stage 2: reimplantation
- Highest success rate for chronic PJI
-
Resection arthroplasty (salvage)
- Permanent spacer or Girdlestone
- Multiple failed revisions
- Non-reconstructable bone loss
- Severe medical comorbidities
-
Suppressive antibiotics only
- Medically unfit for surgery
- Patient refuses surgery
- Palliative intent
Treatment choice depends on timing, organism, implant fixation, and host factors.
Surgical Technique
Debridement, Antibiotics, Implant Retention (DAIR)
Surgical steps:
- Approach: Use previous surgical incision
- Exposure: Full capsulotomy, inspect entire joint
- Debridement:
- Complete synovectomy (remove ALL synovium)
- Debride any necrotic tissue
- Inspect component-bone interfaces
- Remove loose debris
- Component assessment:
- Test stability (push-pull test)
- Inspect for loosening, wear
- If loose - convert to two-stage
- Modular exchange (critical):
- Remove femoral head
- Remove acetabular liner
- New head and liner (do NOT reuse)
- Check neck-liner impingement
- Irrigation:
- Copious irrigation (minimum 6 liters)
- Normal saline (no additives)
- Pulsatile lavage for deeper areas
- Cultures: Minimum 5 tissue samples from different locations
- Closure: Layered closure over drain
Modular Exchange Essential
Always exchange ALL modular components during DAIR (head and liner). Biofilm forms on these surfaces. Reusing modular components dramatically increases DAIR failure rate.

Antibiotic Therapy
Organism-specific antibiotic selection:
First-Line Antibiotic Choices by Organism
| Organism | First-Line IV | Oral Suppression | Duration |
|---|---|---|---|
| MSSA | Flucloxacillin or cefazolin | Cefalexin + rifampicin | IV 4-6 weeks, oral 3-6 months |
| MRSA | Vancomycin | Linezolid, cotrimoxazole, or doxycycline | IV 6 weeks minimum, oral 6-12 months |
| CoNS | Vancomycin (often resistant to beta-lactams) | Cefalexin (if sensitive) + rifampicin | IV 4-6 weeks, oral 3-6 months |
| Streptococcus | Penicillin or ceftriaxone | Amoxicillin | IV 2-4 weeks, oral 3 months |
| Enterococcus | Ampicillin + gentamicin (synergy) | Amoxicillin | IV 4-6 weeks, oral 3-6 months |
| Gram-negative rods | Fluoroquinolone (ciprofloxacin) | Ciprofloxacin + rifampicin | IV 4 weeks, oral 6 months minimum |
| Polymicrobial | Broad-spectrum (vancomycin + pip-tazo) | Based on sensitivities | Extended duration, tailored to organisms |
Key antibiotic principles:
Rifampicin Rules
Rifampicin enhances biofilm penetration and should be used for Staph infections (MSSA, MRSA, CoNS) when implant is retained (DAIR) or after reimplantation. Never use rifampicin monotherapy - resistance develops rapidly. Always combine with another active agent.
General antibiotic protocol:
-
Stage 1 (resection) to Stage 2 (reimplantation):
- IV antibiotics: 4-6 weeks post-stage 1
- Oral antibiotics: Continue until stage 2 (or stop 2-6 weeks before for antibiotic holiday)
- Choice based on culture and sensitivities
-
After Stage 2 (reimplantation):
- IV antibiotics: 2-4 weeks
- Oral suppression: 3-6 months minimum
- Some advocate 12 months for S. aureus/MRSA
- Infectious disease consultation recommended
Antimicrobial stewardship (global principle):
- Reserve agents such as linezolid, daptomycin and newer cephalosporins for resistant Gram-positives (MRSA/VRE) per local sensitivities
- Therapeutic drug monitoring for vancomycin and aminoglycosides
- Engage antimicrobial stewardship and infectious-diseases teams in every case
Culture-Negative PJI
Culture-negative PJI (7-10% of cases) has worse outcomes. Causes: prior antibiotics, fastidious organisms, biofilm. Treat empirically with broad-spectrum (vancomycin + pip-tazo or meropenem) and consider extended culture incubation, molecular diagnostics, or fungal cultures.
Complications
Complications of PJI and Treatment
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Recurrent infection | 10-20% (two-stage), 20-40% (DAIR) | Adequate debridement, appropriate antibiotics, good host optimization |
| Bone loss | Common in chronic PJI | Staged reconstruction, impaction grafting, revision components |
| Spacer complications | 10-15% (fracture, dislocation) | Articulating spacer preferred, patient education on weight-bearing |
| Antibiotic toxicity | 5-15% (renal, hepatic, GI) | Drug level monitoring, renal function checks, ID consultation |
| Persistent pain | 20-30% even after successful treatment | Set realistic expectations, consider salvage if infection cleared |
| Death | 1-2% (higher in elderly, comorbid) | Early recognition, aggressive treatment, optimize comorbidities |
Recurrent infection:
- Most devastating complication
- Risk factors: resistant organisms, immunocompromised host, inadequate debridement
- Management: repeat two-stage, consider salvage (resection arthroplasty)
Antibiotic-related complications:
- Vancomycin: nephrotoxicity (monitor trough levels, creatinine)
- Aminoglycosides: oto- and nephrotoxicity (avoid in renal impairment)
- Rifampicin: hepatotoxicity, drug interactions (LFTs monitoring)
- Fluoroquinolones: tendon rupture, avoid in elderly if possible
Postoperative Care and Rehabilitation
After DAIR:
- Standard THA precautions
- Early mobilization (POD 1-2)
- IV antibiotics
- Monitor wound closely
- Continue IV antibiotics (home IV via PICC if stable)
- Transition to oral antibiotics at 4-6 weeks
- Progressive weight-bearing
- Outpatient physiotherapy
- Oral suppressive antibiotics
- Continue mobilization and strengthening
- Monitor inflammatory markers monthly
- Continue oral antibiotics (per ID)
- Monitor for recurrence
- Gradual return to activities
After Two-Stage Revision:
Stage 1 (resection/spacer):
- Weight-bearing: protected (PWB with walker/crutches)
- Articulating spacer allows mobilization
- IV antibiotics in hospital then home PICC
- Manage expectations - significant disability during this phase
- Spacer is temporary - not a permanent solution
Interval between stages:
- Continue antibiotics per protocol
- Monitor inflammatory markers
- Aspirate hip off antibiotics before stage 2
- Optimize medical comorbidities
- Nutritional optimization (albumin, vitamin D)
Stage 2 (reimplantation):
- Standard THA precautions
- Early mobilization (POD 1-2)
- WBAT if stable fixation
- IV antibiotics 2-4 weeks
- Transition to oral suppression 3-6 months
Long-term surveillance:
- Monitor inflammatory markers at 3, 6, 12 months
- Annual clinical and radiographic review
- Any new pain/symptoms → rule out recurrence
- Patient education on dental prophylaxis
Outcomes and Prognosis
Treatment-specific outcomes:
| Treatment | Success Rate | Functional Outcome | Complications |
|---|---|---|---|
| DAIR | 30-60% | Good if successful | High reinfection |
| One-stage | 80-85% | Good | Moderate reinfection |
| Two-stage | 90-95% (sensitive) | Good to fair | Lowest reinfection |
| Resection | 95% infection control | Poor function | Pain, instability |
Prognostic factors for success:
Favorable:
- Sensitive organisms (Streptococcus best)
- Healthy host (no immunosuppression)
- Early diagnosis and treatment
- Good soft tissue envelope
- Adequate bone stock
Unfavorable:
- MRSA, resistant Gram-negatives, fungi
- Immunosuppressed host (steroids, biologics)
- Multiple prior surgeries
- Extensive bone loss
- Polymicrobial infection
- Culture-negative PJI
Function After Two-Stage
Even with successful infection eradication, functional outcomes after two-stage revision are inferior to primary THA. Patients have longer recovery, more pain, worse ROM, and lower satisfaction scores. Setting realistic expectations is critical.
Long-term considerations:
- PJI survivors have increased mortality compared to matched controls
- Quality of life significantly impacted
- Economic burden substantial (lost work, caregiver needs)
- Psychological impact (depression, anxiety common)
Controversies and Areas of Uncertainty
The evidence base in PJI is evolving, and several management questions remain genuinely contested - high-yield discussion points for vivas.
One-stage vs two-stage
Two-stage is the traditional "gold standard," but the INFORM RCT (BMJ 2022) and the Kunutsor meta-analysis show comparable re-infection with faster recovery, fewer intraoperative events and lower cost for single-stage in selected hips. The debate is shifting from "which is better" to "which patient for which strategy."
Optimal antibiotic duration
The OVIVA trial (NEJM 2019) showed oral therapy was non-inferior to IV for bone and joint infection in the first 6 weeks, challenging routine prolonged IV courses. Total duration (6 weeks vs 12 weeks vs lifelong suppression) remains unsettled and is being tested in ongoing trials.
DAIR criteria and timing
The "3-week biofilm window" is a useful heuristic, not a hard rule. Reported success varies widely with organism, host, and debridement quality. Whether a single thorough DAIR or planned repeat debridement is optimal is debated.
Diagnostic thresholds
Alpha-defensin, synovial CRP, leukocyte esterase, D-dimer and next-generation sequencing each add value but lack universal cut-offs. Culture-negative PJI and the significance of low-virulence organisms (e.g. Cutibacterium) remain difficult areas.
Spacer type and dosing
Articulating versus static spacers, and high-dose antibiotic cement loading, are supported mainly by cohort data; the systemic toxicity ceiling and ideal elution profile are not standardised.
Suppression vs eradication
In frail or multiply-revised patients, long-term suppressive antibiotics with implant retention may be preferable to repeated major surgery, but durability and resistance risk are uncertain.
Prevention Strategies
Preoperative optimization:
Target thresholds:
- HbA1c under 7% (diabetics)
- BMI under 35 (consider weight loss if over 40)
- Albumin over 3.5 g/dL (nutritional status)
- Smoking cessation 4+ weeks preop
- Optimize RA/inflammatory disease (minimize steroids)
Screening and treatment:
- Screen and treat MRSA colonization (nasal mupirocin)
- Clear remote infections (dental, skin, UTI)
- Optimize immunosuppression (hold biologics perioperatively per protocol)
Medical optimization reduces infection risk by 50% or more in high-risk patients.
System-level prevention (global):
- National surgical site infection surveillance programmes (e.g. NHSN in the US, the UK SSI surveillance service, ECDC HAI-Net) benchmark and drive down rates
- Standardised perioperative antibiotic prophylaxis protocols and WHO Surgical Safety Checklist
- Preoperative optimisation pathways (glycaemic control, MRSA decolonisation, nutrition, smoking cessation) in high-volume arthroplasty centres
Evidence Base
- Multi-institutional development and external validation of an updated scoring-based PJI definition (n=1504 development cohort, 422 validation). Major criteria: two positive cultures of the same organism OR a sinus tract. Preoperative minor criteria weighted: serum CRP and D-dimer 2 points each, ESR 1; synovial WBC 3, alpha-defensin 3, leukocyte esterase 3, PMN% 2, synovial CRP 1. Score 6 or more equals infected. New criteria sensitivity 97.7% versus MSIS 79.3% and ICM 86.9%, specificity 99.5%.
- Meta-analysis of 38 one-stage studies (2,536 patients) and 60 two-stage studies (3,288 patients) for infected THA. Pooled re-infection rate 8.2% (95% CI 6.0-10.8) after one-stage versus 7.9% (95% CI 6.2-9.7) after two-stage, with no significant difference and rates similar across subgroups. No randomised trials existed at the time.
- Pragmatic RCT of 140 adults with hip PJI (65 single-stage, 75 two-stage) across the UK and Sweden. No difference in WOMAC pain/function at 18 months (mean difference 0.13, 95% CI -8.2 to 8.5), but single-stage was better at 3 months and had fewer intraoperative events (8% vs 27%). Markers of possible ongoing infection at 18 months: 14% vs 11% (NS). Single-stage was cost-effective.
- Prospective study of 331 explanted hip/knee prostheses (79 infected). Culture of sonicate fluid (which dislodges biofilm bacteria) was more sensitive than periprosthetic-tissue culture: 78.5% vs 60.8% overall (p less than 0.001), and 75.0% vs 45.0% in patients given antibiotics within 14 days before surgery. Specificity ~99% for both.
- Infectious Diseases Society of America guidelines covering DAIR, resection with staged reimplantation, one-stage exchange, and amputation. Recommend 2-6 weeks of pathogen-directed IV (or highly bioavailable oral) therapy, addition of rifampin for staphylococcal infection when the implant is retained or reimplanted, and routine infectious-diseases involvement.
- Largest cohort of Staphylococcus aureus PJI treated with DAIR: 345 episodes (81 MRSA). Overall success 55%; failure 45%, often early. No overall prognostic difference between MSSA and MRSA. Rifampin-based combinations had an independent protective effect. Predictors of failure: polymicrobial, inflammatory and bacteraemic infection, need for more than one debridement, immunosuppression, and not exchanging modular components.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Early Postoperative PJI
"A 68-year-old man is 10 days post-primary THA. He develops increasing hip pain, fevers to 38.5°C, and the wound has serous drainage. ESR 65, CRP 120. What is your assessment and management?"
Scenario 2: Chronic PJI - Two-Stage Candidate
"A 72-year-old woman had a primary THA 18 months ago. She has had persistent pain since surgery, never pain-free. X-rays show subtle periosteal reaction and focal osteolysis. ESR 45, CRP 35. Hip aspiration grows coagulase-negative Staphylococcus (CoNS) from 2 of 3 samples. How do you manage this?"
Scenario 3: Late Hematogenous PJI
"A 65-year-old man had a well-functioning THA 5 years ago (pain-free until now). He presents with 1 week of acute severe hip pain and fever following a dental extraction 2 weeks ago. ESR 75, CRP 95. X-rays show well-fixed components with no loosening. Hip aspiration grows Streptococcus viridans. What is your management?"
Timing Critical
MCQ Practice Points
MSIS 2018 Major Criteria
Q: What are the two major criteria for PJI diagnosis in MSIS 2018? A: (1) Sinus tract communicating with the prosthesis, OR (2) Two positive cultures of the same organism from separate samples. Either ONE major criterion is sufficient for definite PJI diagnosis.
MSIS Minor Criteria Scoring
Q: Which minor criteria are worth 3 points each in the MSIS 2018 scoring system? A: (1) Alpha-defensin (qualitative positive), (2) Leukocyte esterase (++ or +++), (3) Histology (over 10 PMN/HPF in 5 high-power fields). Score of 6 or more equals definite PJI.
DAIR Indications
Q: What are the strict criteria that must ALL be met for DAIR to be appropriate? A: (1) Acute infection (under 3 weeks symptoms OR under 3 months from surgery), (2) Stable/well-fixed implant, (3) Known organism with sensitivities, (4) No sinus tract, (5) Reasonable host (not severely immunocompromised).
Two-Stage Success Rates
Q: What are the success rates for two-stage revision based on organism? A: Sensitive organisms (Strep, MSSA): 90-95%. S. aureus: 85-90%. Resistant organisms (MRSA, resistant GNR): 70-80%. Fungi: under 70%. Two-stage has highest success of all treatments.
Biofilm Timing
Q: Why does DAIR only work in acute infections (under 3 weeks)? A: Biofilm maturation takes 3-4 weeks. Mature biofilm protects bacteria from antibiotics (increases MIC by 1000-fold) and immune system. Before biofilm matures, antibiotics can penetrate. After maturation, implant removal is required for eradication.
Rifampicin Use
Q: When should rifampicin be used in PJI treatment? A: For Staphylococcus species (S. aureus, MRSA, CoNS) when implant is retained (DAIR or after reimplantation). Rifampicin enhances biofilm penetration. Never use as monotherapy - always combine with another active agent to prevent resistance.
Culture-Negative PJI
Q: What are the main causes of culture-negative PJI and how is it managed? A: Causes: (1) Prior antibiotics (most common), (2) Fastidious organisms (slow-growing), (3) Biofilm (organisms in biofilm less culturable). Manage with: extended culture incubation (14 days), molecular diagnostics, sonication of removed implants, empiric broad-spectrum antibiotics (vancomycin + broad Gram-negative coverage).
Guidelines, Registries & Global Practice
Global epidemiology:
- Primary THA PJI incidence ~1-2%; revision THA 3-5%
- Infection is consistently among the top 3 indications for THA revision worldwide, alongside aseptic loosening and dislocation/instability
- Absolute case numbers are rising as arthroplasty volume and patient age/comorbidity increase, even where the percentage rate is stable
Registry evidence (cumulative revision for infection):
| Registry | Region | Notable finding |
|---|---|---|
| NJR | England, Wales, NI | Infection a leading early-revision cause; rising as a proportion of revisions over time |
| AJRR | United States | Infection among top reported revision indications, especially within 2 years of index surgery |
| AOANJRR | Australia/New Zealand | Primary THA revision for infection ~1% at 10 years; higher after revision surgery |
| SHAR (Swedish) | Sweden | Long-term data underpin prophylaxis and bearing-related infection-risk analyses |
| Norwegian / NZJR | Norway / New Zealand | Confirm antibiotic-loaded cement and prophylaxis associations with lower infection-related revision |
Side-by-side guideline comparison:
| Body | Diagnosis | DAIR | Exchange strategy |
|---|---|---|---|
| MSIS/ICM (2018) | Scoring-based definition (score 6 or more) | Acute infection, stable implant, susceptible organism | Two-stage default; one-stage in selected cases |
| IDSA (2013) | Clinical + culture + histology | DAIR acceptable for early/acute with stable implant | Staged or one-stage exchange; rifampin for staphylococci |
| BOA/BOAST / UK | MDT-led, off-antibiotics aspiration | DAIR for acute, well-fixed implant | Increasing single-stage use (INFORM RCT support) |
| EBJIS (European) | Tiered "confirmed/likely/unlikely" definition | Early acute, susceptible organism | Two-stage or one-stage by host/organism |
Resource-setting variation:
- High-resource: dedicated bone-infection MDTs (orthopaedics, ID, microbiology, plastics), sonication, molecular/next-generation sequencing, articulating spacers, and single-stage exchange programmes
- Limited-resource: reliance on serum markers and aspiration without alpha-defensin or sonication; two-stage and resection arthroplasty (Girdlestone) more frequently used where revision implants, prolonged IV antibiotics, or spacer fabrication are constrained
Exam Context
Be prepared to discuss MSIS/ICM 2018 diagnostic criteria (major and minor with scoring). Know the treatment algorithm: DAIR for acute with strict criteria; staged or one-stage exchange for chronic. Cite the INFORM RCT showing single-stage non-inferiority for the hip. Understand organism-specific management (especially S. aureus vs Streptococcus) and rifampicin use for staphylococci with retained or reimplanted components.
PERIPROSTHETIC JOINT INFECTION (PJI) AFTER THA
Clinical summary
MSIS 2018 MAJOR CRITERIA (ONE = DEFINITE PJI)
- •1. Sinus tract communicating with prosthesis
- •2. Two positive cultures of same organism (separate samples)
- •Either ONE major criterion alone = definite PJI diagnosis
- •No further workup required if major criterion present
MSIS 2018 MINOR CRITERIA (SCORE 6+ = DEFINITE PJI)
- •Elevated serum CRP (over 10 mg/L) = 1 point
- •Elevated serum ESR (over 30 mm/hr) = 1 point
- •Elevated synovial WBC (over 3000) = 2 points
- •Elevated synovial PMN% (over 70%) = 1 point
- •Positive alpha-defensin = 3 points (HIGHEST)
- •Positive LE (++ or +++) = 3 points
- •Elevated synovial CRP (over 6.9 mg/L) = 1 point
- •Single positive culture = 2 points
- •Positive histology (over 10 PMN/HPF, 5 fields) = 3 points
DAIR STRICT CRITERIA (ALL MUST BE MET)
- •Acute: under 3 weeks symptoms OR under 3 months from surgery
- •Stable/well-fixed implant (no loosening)
- •Known organism with sensitivities
- •No sinus tract present
- •Healthy host (not severely immunocompromised)
TWO-STAGE REVISION (GOLD STANDARD)
- •Stage 1: Complete removal, debridement, antibiotic spacer
- •IV antibiotics 4-6 weeks, oral until stage 2
- •Antibiotic holiday 2-6 weeks before stage 2
- •Aspirate off antibiotics before stage 2
- •Stage 2: Reimplant when infection cleared (normal markers, negative aspirate)
- •Success: 90-95% sensitive organisms, 85% MSSA, 70-75% resistant
ORGANISM-SPECIFIC TREATMENT
- •MSSA: Flucloxacillin IV → cefalexin + rifampicin PO
- •MRSA: Vancomycin IV → linezolid/cotrimoxazole PO (longer duration)
- •Streptococcus: Penicillin/ceftriaxone (best DAIR success 70-80%)
- •Enterococcus: Ampicillin + gentamicin (synergy)
- •Gram-negatives: Ciprofloxacin + rifampicin
- •Culture-negative: Vancomycin + pip-tazo (broad empiric)
KEY PEARLS AND TRAPS
- •Biofilm matures in 3-4 weeks → why DAIR only works early
- •Rifampicin for Staph with retained implants (never monotherapy)
- •DAIR success 30-60% overall (organism-dependent)
- •Culture before antibiotics (2 weeks off if possible)
- •Never use spacer as permanent implant (cement toxicity)
- •Alpha-defensin best single test (sens 97%, spec 97%)
- •Chronic PJI can mimic aseptic loosening - always rule out infection