Preserve Sensation and Length | Functional Priorities | Prosthetic Integration | Targeted Muscle Reinnervation
- Functional priority in upper limb: Sensation greater than motion greater than length (opposite to lower limb)
- Preserve elbow joint whenever possible - essential for prosthetic function and ADLs
- Replantation vs amputation: Consider indications including thumb, multiple digits, child, clean sharp amputation
- TMR (Targeted Muscle Reinnervation): Improves myoelectric prosthetic control and reduces neuroma pain
- Body-powered vs myoelectric prostheses: Different advantages - body-powered provides sensory feedback
- “Upper limb amputees use prostheses less than lower limb amputees - functional adaptation common
- “Replant thumb at all costs - worth the entire hand functionally
- “Transradial amputation maintains pronation-supination if distal radioulnar joint preserved
- “Phantom limb pain affects up to 80% of upper limb amputees - early intervention essential
Upper limb priorities differ from lower limb. The sensate hand is critical for function - a shorter stump with preserved sensation may be more functional than a longer insensate stump. Always preserve sensate tissue where possible. This contrasts with lower limb where length for weight-bearing and prosthetic fitting is paramount.
Know the replantation indications: Thumb (most important single digit), multiple digits, hand through wrist, pediatric (any level), clean sharp amputation. Contraindications: Multi-level injury, severe crush/avulsion, prolonged warm ischaemia (greater than 6 hours for digits), life-threatening injuries, severe comorbidities.
Body-powered prostheses provide proprioceptive feedback and are more durable. Myoelectric prostheses offer cosmesis and grip strength but lack sensory feedback. Many upper limb amputees reject prostheses and adapt functionally. Elbow preservation is essential for any prosthetic control.
TMR (Targeted Muscle Reinnervation) is an emerging technique where transected nerves are transferred to nearby muscle targets. This provides intuitive myoelectric control, reduces phantom pain, and prevents neuroma formation. Know this as a contemporary technique for transradial and transhumeral levels.
- Key Considerations
- Preserve length, preserve insertion of FDS/FDP
- Functional Outcome
- Good function, cosmesis concern
- Prosthetic Options
- Passive cosmetic, rarely active
- Key Considerations
- Improves grip for adjacent digits, cosmesis
- Functional Outcome
- Narrower hand, may improve function
- Prosthetic Options
- Cosmetic finger prosthesis
- Key Considerations
- Preserves pronation-supination, long lever arm
- Functional Outcome
- Excellent residual function
- Prosthetic Options
- Body-powered or myoelectric
- Key Considerations
- Preserve elbow, minimum 5cm for pronation
- Functional Outcome
- Good prosthetic control with elbow intact
- Prosthetic Options
- Myoelectric with multiple grip patterns
- Key Considerations
- Long lever arm, no bone cut
- Functional Outcome
- Bulky prosthetic elbow, limited cosmesis
- Prosthetic Options
- External locking elbow
- Key Considerations
- Preserve length for prosthetic suspension
- Functional Outcome
- Major functional loss, reduced prosthetic use
- Prosthetic Options
- Myoelectric with TMR, body-powered
- Key Considerations
- Oncological indication most common
- Functional Outcome
- Very limited prosthetic use
- Prosthetic Options
- Cosmetic shoulder cap
SENSEUpper Limb Amputation Priorities
Hook:Upper limb makes SENSE - Sensation and Elbow preservation are the priorities
THUMB PLUSReplantation Indications
Hook:THUMB PLUS all its fingers equals replantation success
Overview and Epidemiology
Upper limb amputation is the surgical removal of part or all of the upper extremity. Unlike lower limb amputation where weight-bearing function is paramount, upper limb amputation surgery must prioritize preservation of sensation and fine motor function to maximize hand utility.
Epidemiology:
- Upper limb amputations are approximately 5 times less common than lower limb
- Trauma is the most common indication (80%) - industrial accidents, motor vehicle trauma
- Males predominate (3:1 ratio) due to occupational exposure
- Mean age is younger than lower limb amputees (occupational injury)
- Finger and partial hand amputations are most common
Upper limb amputation differs fundamentally from lower limb. In the lower limb, the goal is weight-bearing and locomotion - length and prosthetic fitting are priorities. In the upper limb, sensation and fine motor control are essential for hand function. A shorter sensate stump may be more functional than a longer insensate one. Many upper limb amputees adapt without prostheses.
Indications:
- Industrial accidents: Crush, avulsion, saw injuries
- Motor vehicle trauma: Mangled extremity
- Burns: Electrical, thermal with vascular compromise
- Frostbite: Severe cold injury with gangrene
- Failed replantation or reconstruction
- Malignancy: Primary bone/soft tissue sarcoma
- Infection: Gas gangrene, necrotizing fasciitis, refractory osteomyelitis
- Vascular: Rare in upper limb (brachial artery occlusion, Buerger's disease)
- Congenital: Constriction band syndrome, amniotic band syndrome
Contraindications to Replantation (Favour Amputation):
- Multi-level or avulsion injury (poor prognosis)
- Severe crush injury with tissue destruction
- Warm ischaemia time greater than 6 hours for digits (12 hours if cooled)
- Life-threatening associated injuries requiring resuscitation
- Severe medical comorbidities precluding prolonged surgery
- Self-inflicted injuries (relative - psychiatric assessment needed)
Pathophysiology and Functional Considerations
Functional Anatomy Considerations
Understanding the functional requirements at each level is essential for amputation planning in the upper limb.
- Function Lost
- Fine pinch, sensation at fingertip
- Function Preserved
- Power grip, adjacent finger function
- Prosthetic Potential
- Limited - cosmetic mainly
- Function Lost
- All grip patterns, opposition
- Function Preserved
- Wrist motion, pronation-supination
- Prosthetic Potential
- Partial hand prosthesis
- Function Lost
- Grip, wrist motion
- Function Preserved
- Full pronation-supination (50 degrees each)
- Prosthetic Potential
- Good terminal device control
- Function Lost
- Grip, wrist, partial forearm rotation
- Function Preserved
- Elbow flexion-extension
- Prosthetic Potential
- Excellent myoelectric control
- Function Lost
- All below-elbow function
- Function Preserved
- Shoulder motion only
- Prosthetic Potential
- Limited - major functional loss
- Function Lost
- All arm function
- Function Preserved
- Trunk and scapular motion
- Prosthetic Potential
- Very limited prosthetic use
Nerve Handling and Neuroma Prevention
Neuroma Formation:
- Inevitable after nerve transection - regenerating axons form disorganized mass
- Painful neuroma develops when nerve end is in mobile or pressure-bearing area
- Upper limb neuromas are particularly problematic due to constant use
- Prevention is key - proper nerve management at initial surgery
Targeted Muscle Reinnervation (TMR):
TMR involves transferring transected nerves to nearby muscle motor points. The muscle serves as a biological amplifier - when the patient thinks of moving their missing hand, the reinnervated muscle contracts, providing strong EMG signals for myoelectric prosthetic control. TMR also prevents neuroma formation and reduces phantom pain by providing the transected nerve a target.
TMR Nerve Transfers by Level:
- Transradial: Median and ulnar nerves to remaining forearm muscle motor points
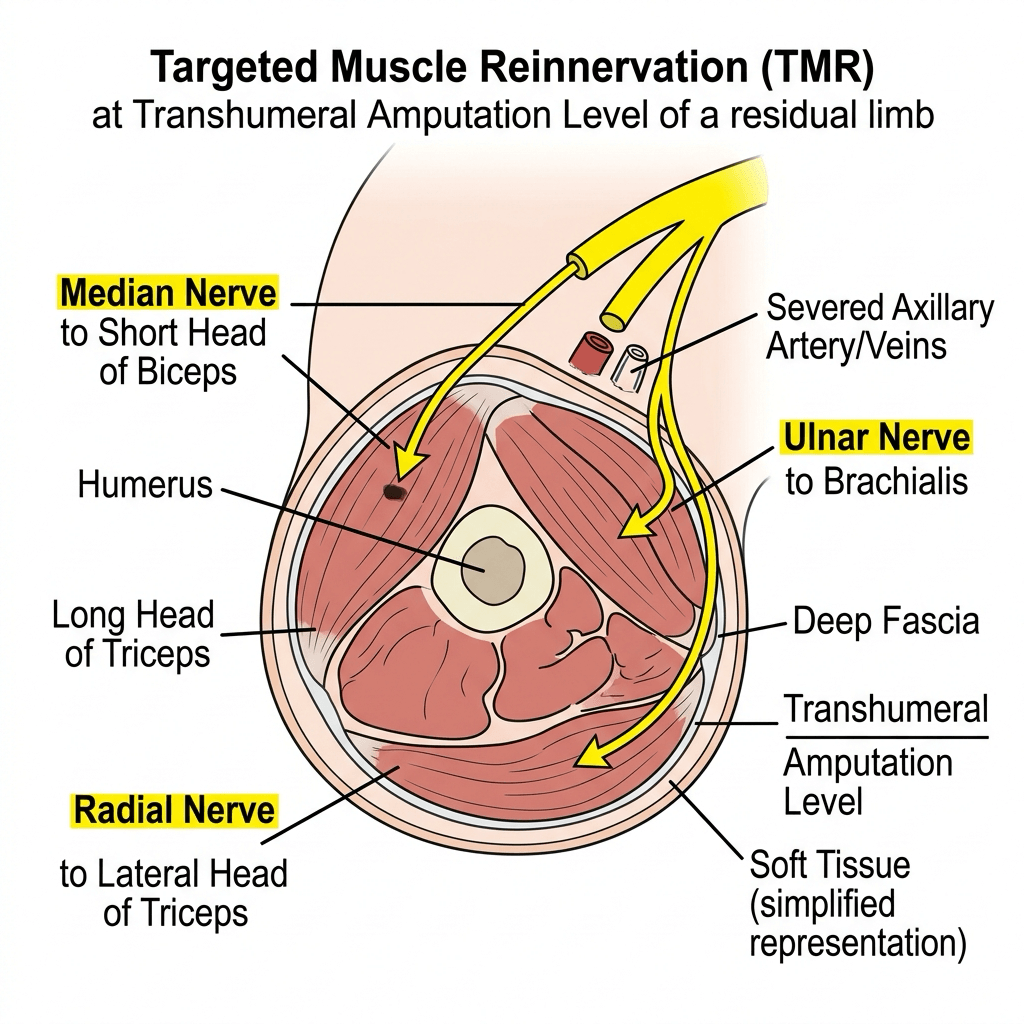
- Transhumeral: Median to short head biceps, ulnar to brachialis, radial to lateral triceps
- Shoulder: Musculocutaneous to clavicular pectoralis major, median/ulnar to sternal pectoralis
Phantom Limb Phenomena
- Nearly universal after upper limb amputation
- Non-painful awareness of missing limb
- Typically diminishes over time
- Affects 50-80% of upper limb amputees
- Character: Burning, cramping, shooting, electric
- Risk factors: Pre-amputation pain, traumatic mechanism, anxiety/depression
- Prevention: Perioperative nerve blocks, TMR at initial surgery
Early intervention is key for phantom limb pain. Perioperative regional anaesthesia (brachial plexus block, epidural) may reduce incidence. TMR at primary amputation reduces both neuroma pain and phantom pain. Mirror therapy should be initiated early in rehabilitation.
Clinical Presentation and Assessment
Indications by Level
Finger and Ray Amputation
- Irreparable crush or avulsion injury to digit
- Failed replantation
- Severe infection (septic arthritis, osteomyelitis)
- Tumour requiring local excision
- Painful non-functional digit (neuroma, cold intolerance)
- Vascularity of adjacent tissue
- Tendon and nerve integrity
- Level of injury (through bone vs joint)
- Replantation candidacy (thumb prioritized)
- Thumb: Most important digit - 50% of hand function. Replant at all costs
- Index finger: Precision pinch, pointing. Loss well compensated by long finger
- Long finger: Central pillar of grip. Loss affects both power and precision
- Ring finger: Power grip contribution. Ray amputation may improve function
- Little finger: Ulnar border, power grip. Preserve for cupping function
Replantation Decision-Making
- Favours Replantation
- Clean, sharp cut (guillotine)
- Favours Amputation
- Crush, avulsion, multi-level
- Favours Replantation
- Less than 6 hours (digit), less than 12 hours (major limb)
- Favours Amputation
- Prolonged warm ischaemia
- Favours Replantation
- Thumb, multiple digits, proximal (wrist/forearm)
- Favours Amputation
- Single digit (index, long, ring)
- Favours Replantation
- Pediatric (excellent regeneration), young adult
- Favours Amputation
- Elderly with comorbidities
- Favours Replantation
- Non-smoker, compliant, motivated
- Favours Amputation
- Smoker, non-compliant, unrealistic expectations
- Favours Replantation
- Isolated limb injury, stable patient
- Favours Amputation
- Polytrauma, life-threatening injuries

Investigations
Investigation Protocol for Upper Limb Amputation Planning
Essential for all cases:
- AP and lateral of affected limb segment
- Assess bone level, fracture pattern, foreign bodies
- For trauma: Full trauma series if indicated
- Chest radiograph if oncological (metastatic workup)
When vascular injury suspected:
- Hand-held Doppler assessment of radial, ulnar, digital arteries
- Allen test for palmar arch competency
- CT angiography if revascularization being considered
- Warm ischaemia time documentation critical
Selected cases:
- MRI: Tumour staging, soft tissue extent
- CT: Bone detail, fracture pattern, foreign bodies
- PET-CT: Oncological staging if sarcoma suspected
Preoperative baseline:
- Full blood count, coagulation studies
- Group and hold (cross-match if major amputation)
- Urea, electrolytes, glucose
- CRP if infection suspected
- Muscle enzymes if crush injury (rhabdomyolysis risk)
For potential replantation, investigations are time-critical. Obtain X-rays of both amputated part and stump. Document exact ischaemia time. Cool the amputated part correctly (wrapped in saline-moistened gauze, in plastic bag, on ice - not directly on ice or in water). Activate replantation team while investigations proceed.

Management Principles
Level Selection Principles
Goals in Upper Limb Amputation:
- Preserve sensation wherever possible
- Preserve elbow joint (critical for function)
- Preserve length for prosthetic fitting
- Ensure durable soft tissue coverage
- Prevent neuroma formation (TMR when possible)
- Optimize for prosthetic or functional adaptation
- Length Requirements
- Maximum length through bone
- Key Structures to Preserve
- Preserve FDS/FDP insertions if possible
- Prosthetic Implications
- Cosmetic prosthesis only
- Length Requirements
- Through metacarpal base
- Key Structures to Preserve
- Adjacent finger tendons and nerves
- Prosthetic Implications
- Improves grip, cosmetic option
- Length Requirements
- Through radiocarpal joint
- Key Structures to Preserve
- Distal radioulnar joint (pronation-supination)
- Prosthetic Implications
- Excellent control, bulbous end
- Length Requirements
- Minimum 5cm from olecranon
- Key Structures to Preserve
- Elbow joint, biceps/brachialis insertions
- Prosthetic Implications
- Ideal for myoelectric, TMR possible
- Length Requirements
- Through joint, preserve condyles
- Key Structures to Preserve
- Humeral length, epicondyles for suspension
- Prosthetic Implications
- External elbow lock, bulky
- Length Requirements
- Minimum 10cm from acromion
- Key Structures to Preserve
- Deltoid insertion if possible
- Prosthetic Implications
- TMR improves control significantly
- Length Requirements
- At glenohumeral joint
- Key Structures to Preserve
- Scapula, clavicle for cosmetic cap
- Prosthetic Implications
- Limited prosthetic use
Surgical Management
Digital Amputation Technique
- Irreparable trauma to digit
- Severe infection (septic arthritis, osteomyelitis)
- Non-viable replant
- Tumour requiring excision
- Preserve maximum length
- Through bone preferred to through joint (cosmesis)
- Preserve FDP/FDS insertions when possible
Digital Amputation Steps
Fish-mouth or lateral incisions:
Create volar and dorsal flaps of equal length, or lateral flaps for side-to-side closure. Volar flap slightly longer provides better coverage.
Identify and protect structures:
Divide flexor and extensor tendons proximal to skin level. Identify digital nerves and arteries.
Ligate vessels, handle nerves:
Ligate or cauterize digital arteries. Apply gentle traction to digital nerves, transect sharply, allow retraction.
Divide bone smoothly:
Use bone cutter or saw. Rongueur to smooth edges. Bone level proximal to skin level for tension-free closure.
Tension-free skin closure:
Close volar to dorsal skin with interrupted nylon. Bulky dressing with aluminium finger splint protection.
Technical Pearls:
- Thumb: Preserve maximum length - every millimeter counts
- Index ray amputation: Improves cosmesis and grip width
- Ring ray amputation: Narrows hand, may improve power grip
- Volar flap: More durable than dorsal skin for tip coverage
Prosthetic Considerations
Prosthetic Options by Level
- Prosthetic Type
- Passive cosmetic silicone
- Terminal Device
- Cosmetic fingers
- Control Mechanism
- None - passive
- Prosthetic Type
- Body-powered or myoelectric
- Terminal Device
- Hook or hand
- Control Mechanism
- Cable or EMG
- Prosthetic Type
- Myoelectric multi-articulating hand
- Terminal Device
- i-Limb, bebionic, TASKA
- Control Mechanism
- 2-site EMG or pattern recognition
- Prosthetic Type
- Body-powered or hybrid
- Terminal Device
- Hook or hand with external elbow
- Control Mechanism
- Cable for elbow, EMG for TD
- Prosthetic Type
- Myoelectric with TMR
- Terminal Device
- Multi-articulating hand and elbow
- Control Mechanism
- Pattern recognition optimal
- Prosthetic Type
- Cosmetic cap
- Terminal Device
- None functional
- Control Mechanism
- Cosmetic restoration only
Body-Powered vs Myoelectric Prostheses
- Provides proprioceptive feedback through cable
- More durable, reliable
- Lower cost and maintenance
- Works in wet and dirty environments
- Lighter weight
- Limited grip strength
- Less cosmetic
- Requires harness (uncomfortable for some)
- Fatiguing with prolonged use
- Better cosmesis
- Higher grip strength
- Multiple grip patterns (modern hands)
- No harness required
- Less physical effort for operation
- No sensory feedback
- Battery dependent
- Cannot use in wet environments
- Higher cost and maintenance
- Heavier
Upper limb amputees reject prostheses more often than lower limb amputees (30-50% rejection rate). Many adapt functionally using their residual limb and contralateral hand. Body-powered prostheses are rejected less often than myoelectric due to feedback and reliability. Early prosthetic fitting improves long-term use. Patient goals and occupation should guide prosthetic selection.
GRASPProsthetic Selection Factors
Hook:Help patients GRASP their prosthetic options - matching function to need
Complications
Wound-Related Complications
- Incidence
- 5-10%
- Risk Factors
- Diabetes, contamination, crush injury
- Management
- Antibiotics, debridement, revision if needed
- Incidence
- 5%
- Risk Factors
- Tension, poor vascularity, malnutrition
- Management
- VAC therapy, revision, skin graft if needed
- Incidence
- Variable
- Risk Factors
- Crush injury, arterial disease, tension
- Management
- Debridement, revision to higher level
- Incidence
- 5%
- Risk Factors
- Anticoagulation, inadequate hemostasis
- Management
- Aspiration or evacuation
Prevention:
- Tension-free closure
- Adequate hemostasis
- Avoid closure over bone prominences
- Proper flap design
The Krukenberg Kineplastic Forearm Reconstruction
The topic repeatedly stresses that sensation is prized over length, that roughly a third of upper-limb amputees reject prostheses and adapt without them, and that limited-resource settings rely on function rather than technology - but it never mentions the one operation that delivers sensate prehension without any prosthesis: the Krukenberg procedure.
- What it is. A kineplastic (cineplastic) reconstruction of the transradial stump that splits the residual forearm into two sensate, independently mobile "pincers" - a radial ray (radius and its muscles) and an ulnar ray (ulna and its muscles) - separated down the interosseous space, with the pronator teres and other forearm muscles powering the opening and closing of the pincers.
- Why it is unique. The pincer tips are covered by the patient's own sensate skin, so grasp has intact sensation and proprioception that no prosthesis provides - the very qualities this topic says matter most in the upper limb. It is self-powered and self-suspending: no socket, battery, harness or maintenance.
- Who it is for. Classically the bilateral transradial amputee (on at least one side), the blind amputee (sensate grasp substitutes for lost vision), and low-resource settings where durable prostheses are unavailable. It needs an adequate residual forearm length and good soft tissue.
- The trade-off. The result is cosmetically confronting (a "lobster-claw" forearm), which limits acceptance for many patients; it can still be fitted with a prosthesis over it if desired, so it does not preclude later prosthetic use. Consider it when function without technology is the priority, not as a routine primary amputation.
Q: How can a transradial amputee achieve sensate grasp without any prosthesis? A: The Krukenberg procedure - a kineplastic reconstruction that splits the forearm stump into two sensate, muscle-powered pincers (a radial ray and an ulnar ray) that open and close for prehension with the patient's own skin sensation and no socket, battery or harness. It is classically used for the bilateral transradial amputee, the blind amputee, and limited-resource settings, needs adequate forearm length, and - despite a "lobster-claw" appearance that limits acceptance - can still be fitted with a prosthesis later.
Reconstructing the Unreplantable Thumb
The single most-repeated message in this topic is that the thumb is worth roughly half of hand function and should be replanted "at all costs", and "failed replantation" is listed as an indication for amputation - yet the topic never says what to do when the thumb is lost or unreplantable: reconstruct it.
- Why reconstruct at all. A hand without a thumb loses opposition, pinch and most grip; restoring even a mobile, sensate post to oppose against transforms function - so an unreplantable thumb is not simply "closed" but reconstructed up a ladder according to the level of loss and the available donors.
- Pollicization. For loss at or proximal to the metacarpophalangeal level (or a congenitally absent thumb), an adjacent digit - usually the index (or an already-injured, stiff finger) - is transposed onto the thumb axis, shortened and rotated into roughly 40-50 degrees of pronation/opposition with its intrinsics re-tensioned, converting a finger into a thumb in a single-stage, non-microsurgical operation that brings its own nerves and vessels.
- Microvascular toe-to-thumb transfer. When the other digits must be preserved, a free toe transfer (great toe, second toe, or a "wrap-around" great-toe flap) reconstructs the thumb with a growing, sensate, mobile digit and a nail - the workhorse for the amputated thumb on an otherwise healthy hand, at the cost of microsurgery and donor-foot morbidity.
- Simpler options. For lesser loss, length and stability are restored by distraction lengthening of the metacarpal, deepening of the first web space (Z-plasty/release), or osteoplastic reconstruction - lower-tech steps on the same ladder.
Q: The thumb is amputated and cannot be replanted - what are the reconstructive options? A: Reconstruct it up a ladder by level and donor availability. For loss at/proximal to the MCP joint, pollicization transposes an adjacent digit (usually the index) onto the thumb axis in ~40-50 degrees of opposition - single-stage, non-microsurgical, bringing its own nerves and vessels. When the other digits must be kept, a microvascular toe-to-thumb transfer (great or second toe) gives a growing, sensate, nailed digit. Lesser loss is managed by metacarpal distraction lengthening, first-web deepening, or osteoplastic reconstruction. A restored sensate, mobile, opposable post transforms hand function.
Guidelines, Registries & Global Practice
Global Epidemiology
- Upper-limb amputation is roughly 5 times less common than lower-limb amputation; in high-income settings the leading cause is trauma (occupational and machinery injury), whereas dysvascular and diabetic causes dominate the lower limb.
- Male predominance (~3:1) and a younger mean age than lower-limb amputees, reflecting occupational mechanism.
- In low- and middle-income countries, agricultural and industrial machinery, road trauma and conflict/blast injury are major contributors, often with delayed presentation that reduces replantation viability.
Guidelines and Society Guidance (side by side)
- Emphasis
- Major trauma network triage; specialist hand/replant transfer
- Practical recommendation
- Potentially replantable injuries routed early to a replantation-capable unit; correct cooling and transfer
- Emphasis
- Function-first level selection, early prosthetic referral
- Practical recommendation
- Preserve elbow and sensate length; multidisciplinary limb-loss rehabilitation pathways
- Emphasis
- Selective, evidence-based replantation
- Practical recommendation
- Always salvage thumb and multiple digits; selective approach to borderline single digits
- Emphasis
- Appropriate, sustainable prosthetic provision
- Practical recommendation
- Match device to need and resource setting; body-powered devices remain first line where service support is limited
Registry and Outcome Data
- Upper-limb amputation and replantation lack the mature implant registries that exist for arthroplasty (NJR, AJRR, AOANJRR); evidence comes mainly from national administrative databases and large single-centre series (e.g. replantation volume-outcome relationships).
- Volume matters: higher institutional replantation volume is associated with higher digit-survival rates, supporting regionalised referral to specialist units.
- Emerging osseointegration outcome registries are beginning to capture infection and implant-survival data for bone-anchored upper-limb prostheses.
High- vs Limited-Resource Practice Variation
- High-resource: 24/7 microsurgical replantation, multi-articulating myoelectric hands, TMR/RPNI and osseointegration available in tertiary centres; structured limb-loss rehabilitation and peer support.
- Limited-resource: emphasis on durable revision amputation, sensate length preservation and robust body-powered or appropriate-technology prostheses; replantation reserved for the highest-yield cases (thumb, multiple digits) where microsurgical capacity exists.
- The functional priority (sensation greater than motion greater than length) and the imperative to preserve the elbow hold across all settings - they are decisions, not resources.
Controversies and Areas of Uncertainty
Performing TMR or regenerative peripheral nerve interfaces (RPNI) at the time of amputation is increasingly advocated to prevent neuroma and phantom pain, but the highest-quality RCT evidence (Dumanian 2019) studied delayed/established pain. Whether routine prophylactic TMR in every amputee changes long-term outcomes - versus added operative time and cost - remains unproven.
Both convert cut nerves into a target. TMR transfers a nerve to a motor point (also yielding control signals); RPNI wraps the nerve end in a free muscle graft and is technically simpler with no donor muscle sacrifice. Comparative trials are lacking - choice is largely surgeon preference and whether myoelectric control sites are also wanted.
Level III data (Zhu 2018) show no functional benefit of replanting small, ring (proximal) or distal long-finger amputations, at higher cost. Yet patient preference, occupation, cultural factors and bilateral injury may still justify attempts. The "replant everything" reflex is being replaced by selective, evidence-based salvage.
Bone-anchored implants abolish socket discomfort and improve range and proprioception, but carry superficial/deep infection and mechanical failure risk and require staged surgery. Long-term comparative outcome data versus modern sockets are still maturing; uptake is selective and level-dependent.
Despite advanced multi-articulating myoelectric hands, no consistent functional superiority over durable body-powered devices is shown in everyday tasks, and abandonment rates are similar. Sensory feedback restoration (sensorised prostheses, targeted sensory reinnervation) is an active research frontier.
Lower-limb scores (MESS) translate poorly to the upper limb, where a partially functional, sensate hand often outperforms any prosthesis. There is no validated upper-limb-specific decision score; the threshold for salvage is generally lower (more aggressive) than in the leg.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old right-hand dominant male presents to the emergency department after his right hand was caught in an industrial press. Examination reveals crush injury to all fingers at the level of the proximal phalanges with devitalized tissue. The thumb metacarpal is fractured but the thumb itself is intact. There is no distal circulation to the fingers. The amputated finger segments have been retrieved but are severely crushed. How would you manage this patient?”
“You are performing a transradial amputation for a 45-year-old woman with sarcoma of the distal radius. The oncology team requires a margin of 5cm proximal to the tumour, which leaves approximately 12cm of forearm from the elbow. Describe your surgical technique, focusing on nerve management and optimization for prosthetic function.”
“A 16-year-old boy presents 4 hours after a clean guillotine amputation of his right thumb at the level of the proximal phalanx from a circular saw accident at his father's workshop. The amputated part has been kept in a plastic bag on ice. What are the indications for replantation here, and describe your management approach.”
Key Priorities
- Sensation GREATER THAN motion GREATER THAN length (opposite to lower limb)
- Preserve elbow - loses 50% function if amputated above
- Replant thumb at all costs - 50% of hand function
- TMR prevents neuroma and phantom pain, improves prosthetic control
Replantation Indications (THUMB PLUS)
- Thumb - single most important digit
- Multiple digits, hand/wrist level
- Pediatric patients (any level)
- Clean sharp mechanism, short ischaemia time
Level-Specific Pearls
- Finger: Preserve FDS/FDP insertion, volar flap for coverage
- Wrist disarticulation: Preserves pronation-supination (DRUJ intact)
- Transradial: Minimum 5cm from elbow, ideal for TMR and myoelectric
- Transhumeral: Preserve deltoid insertion, TMR essential for function
Nerve Management
- Standard: Traction neurectomy - pull, sharp transection, allow retraction
- TMR: Transfer median to biceps, ulnar to brachialis, radial to triceps
- Position nerves away from scar and pressure areas
- TMR reduces both neuroma AND phantom limb pain
Prosthetic Considerations
- Body-powered: Proprioceptive feedback, durable, works wet
- Myoelectric: Cosmesis, grip strength, multiple patterns, no feedback
- 30-50% upper limb amputees reject prostheses - functional adaptation common
- Early fitting improves long-term acceptance
Complications to Know
- Phantom limb pain: 50-80%, mirror therapy effective, gabapentinoids
- Neuroma: Prevented by TMR or traction neurectomy
- Contracture: Elbow flexion (transhumeral) - early ROM essential
- Prosthetic rejection: Common - address patient goals and expectations
Evidence Base and Key Studies
TMR Treats Neuroma and Phantom Pain in Major Amputees (Landmark RCT)
- First randomised surgical trial for post-amputation pain - 28 major limb amputees randomised to TMR versus standard neuroma excision with burying in muscle
- In longitudinal mixed-model analysis, reduction in phantom limb pain was significantly greater with TMR (between-group difference 3.5 on the 0-10 NRS, P=0.03)
- Residual (neuroma) limb pain trended in favour of TMR (difference 1.9, P=0.10 to 0.15)
- Results continued to favour TMR at longest follow-up including crossover patients
- Multicentre design (Northwestern and Walter Reed)
TMR Enables Real-Time Myoelectric Control of Multifunction Arms
- 5 patients with shoulder-disarticulation or transhumeral amputation after TMR, compared with 5 able-bodied controls
- Pattern-recognition decoding of surface EMG allowed reliable performance of 10 distinct elbow, wrist and hand motions
- TMR patients completed 96.3% of elbow/wrist movements and 86.9% of hand movements within 5 seconds (controls 100% and 96.7%)
- Three patients demonstrated control of advanced motorised shoulder, elbow, wrist and hand prostheses
- Established TMR as a biological amplifier for intuitive prosthetic control
Single-Digit Replantation vs Revision Amputation by Tamai Level
- 1023 patients with single-digit traumatic amputation - successful replantation versus revision amputation, stratified by Tamai level and digit
- Replantation gave NO functional benefit (Michigan Hand Questionnaire at 1 year) for small finger (levels I-V), ring finger (I-III) and long finger (level I)
- Replantation outperformed revision for thumb (all levels I-V), index (I-V), long finger (II-V) and ring finger (IV-V)
- Replantation cost more and lengthened hospital stay and sick leave
- Provides a digit- and level-specific evidence base for the replantation decision
Upper Limb Prosthesis Use and Abandonment
- Analytical review of ~200 articles (40 reporting rejection) across 25 years of upper-limb prosthesis literature
- Adult rejection: body-powered 26%, electric (myoelectric) 23%
- Paediatric rejection markedly higher: body-powered 45%, electric 35%
- Average non-wear similar in adults (20%) and children (16%)
- Wide variance reflects heterogeneous samples and non-standardised outcome measures
Mirror Therapy Reverses Cortical Reorganisation in Phantom Limb Pain
- 13 chronic phantom limb pain patients after unilateral arm amputation completed 4 weeks of daily mirror therapy
- Mean phantom pain fell by 27%
- fMRI showed pain reduction tracked with reversal of dysfunctional reorganisation in primary somatosensory cortex
- Telescoping of the phantom predicted poorer response
- Mechanistic link between body representation and analgesic effect
Patient Perspectives on Upper-Limb Osseointegration
- National survey of US veterans with upper-limb amputation on attitudes to bone-anchored (osseointegrated) prostheses
- 28% of unilateral and 13% of bilateral amputees were willing to consider osseointegration surgery
- Transhumeral level was associated with greater willingness; older age and better mental-health scores with less
- Durability/reliability, ability to do more activities and comfort were the most valued benefits
- Chronic pain, loss of nerve function and device failure were the least acceptable risks