Partial Knee | Medial vs Lateral | Oxford vs Fixed Bearing
- Strict Indication Criteria: Essential for success. 50% of revisions are due to poor selection.
- ACL Requirement: Must be intact and functional for UKA kinematics.
- Oxford Criteria: Bone-on-bone medial, Full thickness lateral/PF, Correctable varus, FFD under 15 deg.
- Inflammatory Arthritis: Absolute contraindication (disease will progress).
- Outcomes: Faster recovery and better function than TKA, but 2-3x higher revision rate.
- “Oxford criteria: intact ACL, correctable deformity, isolated compartment
- “Mobile bearing: lower wear, higher dislocation
- “Medial UKA most common
- “Good for active younger patients
ACL Must Be Intact. An ACL deficient knee has altered kinematics (anterior translation) that causes early failure of UKA (rocking horse phenomenon).
Deformity Must Be Correctable. Intra-articular deformity only. Does not fix extra-articular deformity.
Revision Rate Artifact. Registers show higher revision rates partly because UKA is easier to revise to TKA than TKA is to revise.
Do NOT Overcorrect. Aim for native alignment or slight under-correction. Overcorrection unloads the UKA and accelerates lateral wear.
- UKA Candidate
- Intact & Functional
- TKA Candidate
- Intact or Ruptured
- UKA Candidate
- Isolated Medial (or Lateral)
- TKA Candidate
- Multicompartmental
- UKA Candidate
- Correctable, under 15 deg
- TKA Candidate
- Fixed, Severe deviation
- UKA Candidate
- Under 15 degrees
- TKA Candidate
- Any degree
- UKA Candidate
- No (Contraindicated)
- TKA Candidate
- Yes (Indicated)
- UKA Candidate
- BMI under 35 (Relative)
- TKA Candidate
- Any BMI
Overview and Epidemiology
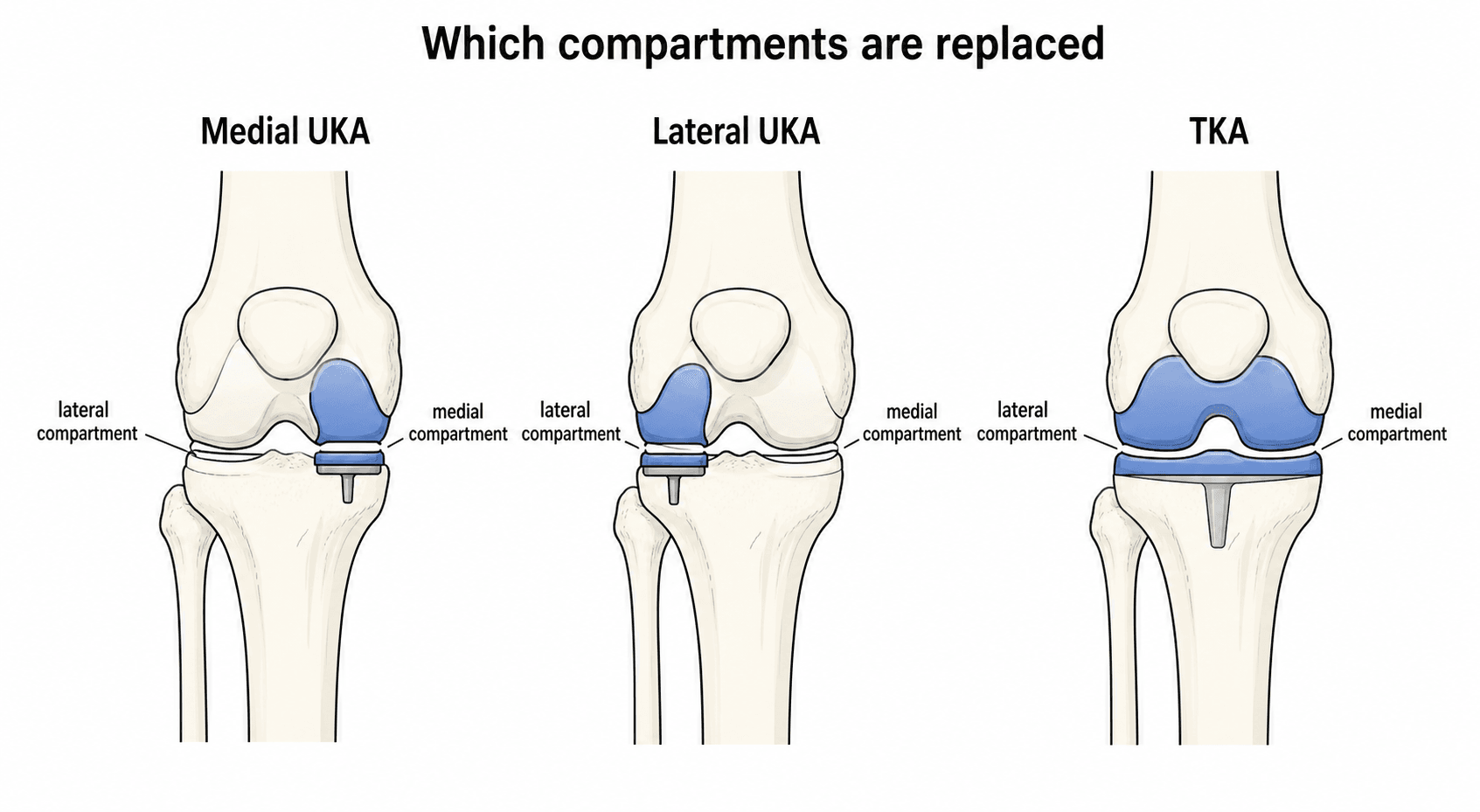
Definition: Unicompartmental Knee Arthroplasty (UKA) involves replacing only the damaged compartment of the knee (medial or lateral), preserving the cruciate ligaments and the healthy compartments.
Epidemiology:
- Prevalence: Accounts for 10-15% of all knee replacements in most developed registries.
- Utilization: Highly variable. Usage ranges from under 5% to over 40% depending on surgeon philosophy and country, with most large registries clustering around 8-12% of primary knee arthroplasties.
- Gender: Equal distribution.
- Age: Bimodal distribution.
- Young Active: Under 55. Goal is bone preservation and high function.
- Elderly Frail: Over 80. Goal is less morbidity, quicker recovery, and lower risk of medical complications (MI/Stroke) compared to TKA.
Rationale: By preserving the ACL and PCL, UKA maintains near-normal knee kinematics and proprioception. This translates to a "forgotten knee" feeling more often than TKA.
- Kinematics: Retains the screw-home mechanism and femoral rollback.
- Function: Patients walk faster and have better gait analysis scores than TKA patients.
- Recovery: Shorter length of stay and faster return to work.
Indications and Contraindications
Indications (Kozinn and Scott / Oxford)
- Age greater than 60
- Weight less than 82kg (180lbs)
- Low activity demand
- Minimal rest pain
- ROM greater than 90 degrees
- Flexion contracture less than 5 degrees
- Angular deformity less than 10 degrees (varus)
- Pathology: Anteromedial OA (bone-on-bone)
- Ligaments: Functionally intact ACL/MCL
- Deformity: Correctable intra-articular varus
- Status: Full thickness cartilage in Lateral compartment
- Age and Weight: Ignored. Criteria applied to all.
Result: Modern usage has expanded to younger, heavier, and more active patients with good results, provided the anatomical criteria are met.
ABCDEUKA Indications (Oxford Criteria)
Hook:ABCDE for UKA eligibility!
FAILUKA Contraindications
Hook:FAIL criteria = don't do UKA!
Mobile vs Fixed Bearing
Design Philosophy
- Mobile Bearing (e.g., Oxford)
- Polyethylene moves on tibia
- Fixed Bearing (e.g., Miller-Galante)
- Polyethylene locked to tibia
- Mobile Bearing (e.g., Oxford)
- High (Conformity)
- Fixed Bearing (e.g., Miller-Galante)
- Low (Point loading)
- Mobile Bearing (e.g., Oxford)
- Low (Linear)
- Fixed Bearing (e.g., Miller-Galante)
- High (Point stress)
- Mobile Bearing (e.g., Oxford)
- Soft tissue dependent
- Fixed Bearing (e.g., Miller-Galante)
- Implant dependent
- Mobile Bearing (e.g., Oxford)
- Risk (1-2%)
- Fixed Bearing (e.g., Miller-Galante)
- No risk
- Mobile Bearing (e.g., Oxford)
- Must be intact/tensioned
- Fixed Bearing (e.g., Miller-Galante)
- Tolerates some laxity
- Mobile Bearing (e.g., Oxford)
- Excellent long term
- Fixed Bearing (e.g., Miller-Galante)
- Excellent long term
Fixed vs Mobile Bearing — Systematic Review & Meta-analysis
- 44 studies, 9,463 medial UKA knees pooled.
- Crude revision rate: fixed bearing 0.90 vs mobile bearing 1.51 per 100 component-years.
- After stratifying for follow-up duration and age, revision rates were NOT substantially different.
- No essential difference in survivorship between the two designs.
Pathophysiology and Mechanisms
The Medial Compartment:
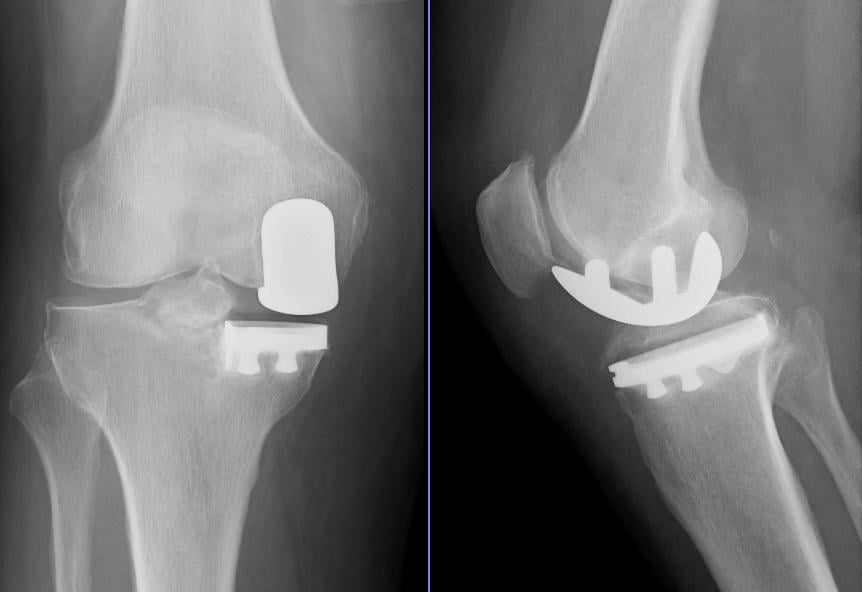
- Wear Pattern: Anteromedial wear is typical in varus OA with an intact ACL. The femoral wear is on the distal condyle, and tibial wear is central/posterior (often with a 'cup' defect).
- Obligatory Rotation: The tibia internally rotates during flexion. UKA designs must accommodate this screw-home mechanism.
- Meniscus: The medial meniscus is excised. The implant (polyethylene) effectively replaces meniscal function.
Kinematics (The ACL):
- Anterior Translation: The ACL prevents anterior tibial translation.
- In UKA: Without an ACL, the tibia subluxes anteriorly, causing eccentric loading on the posterior aspect of the UKA insert ("Rocking Horse").
- Result: Early loosening and failure. Hence, ACL integrity is non-negotiable.
Alignment Goals:
- Resurfacing: The goal is to resurface the joint line to its pre-disease state (constitutional varus).
- Coronal Plane: Tibial cut usually perpendicular to tibial mechanical axis. Femoral component aligned to restore joint line height.
- Sagittal Plane: Tibial slope must match native slope (usually 7 degrees posterior) to balance the flexion gap.
Classification Systems
Ahlback Classification (Radiographic OA)
Useful for quantifying bone loss and suitability for UKA vs HTO.
Grade 1: Joint space narrowing (less than 3mm).
Grade 2: Joint space obliteration.
Grade 3: Minor bone attrition (0-5mm).
Grade 4: Moderate bone attrition (5-10mm).
Grade 5: Severe subluxation of tibia.
Relevance: UKA is ideal for Grade 2-4. Grade 5 may imply excessive deformity/instability that requires TKA.
Keys to Classification for UKA:
- "Kissing Lesion": Bone-on-bone contact is ideal (confirms full thickness loss). Pain relief is more predictable when bone-on-bone is present than when some cartilage remains.
- "Anteromedial Wear": On lateral X-ray, wear should be anterior. Posterior wear suggests ACL deficiency.
Clinical Assessment
History:
- Pain Location: "One finger test". Patient should point directly to the medial joint line. Generalized pain or retropatellar pain is a "red flag".
- Start Up Pain: Typical of OA.
- Mechanical Symptoms: Locking/Catching (meniscal) fits with UKA pathology.
- Instability: Giving way? (Suggests ACL deficiency - Contraindication).
- Patellofemoral Symptoms: Significant pain on stairs or rising from a chair? (Relative contraindication if severe).
Physical Examination:
- Gait: Antalgic? Varus thrust? (Thrust suggests dynamic instability).
- Alignment: Standing varus. Is it mild/moderate or severe?
- Range of Motion:
- Check extension (FFD under 15 deg?). Fixed flexion is hard to correct.
- Check flexion (Need greater than 110 deg for surgery exposure).
- Ligaments:
- Lachman/Anterior Drawer: MUST be stable. A firm endpoint is required.
- MCL: Valgus stress test. Must be competent (especially for mobile bearing). Open at 30 deg flexion but solid endpoint.
- Correctability: With knee in 20 deg flexion, apply valgus stress. Does the varus correct to neutral? If rigid, TKA is better.
- Other Compartments: Palpate lateral joint line and PF joint. Should be pain-free. Crepitus in PF joint with pain is concerning.
- Distinguishing Feature
- One-finger medial joint-line pain, intact ACL, correctable varus, anterior wear on lateral X-ray
- Why it Matters for UKA
- The target pathology — predictable UKA result
- Distinguishing Feature
- Diffuse pain, lateral or retropatellar symptoms, lateral/PF narrowing on X-ray
- Why it Matters for UKA
- Contraindicates UKA — pain persists; needs TKA
- Distinguishing Feature
- History of giving-way, positive Lachman, posterior tibial wear on lateral X-ray
- Why it Matters for UKA
- Absolute contraindication to standard UKA (edge loading)
- Distinguishing Feature
- Inflammatory pattern, effusion, raised CRP/ESR, pan-compartment changes
- Why it Matters for UKA
- Absolute contraindication — disease progresses to other compartments
- Distinguishing Feature
- Sudden severe pain, focal medial femoral condyle lesion on MRI, often older female
- Why it Matters for UKA
- May be a UKA indication if confined and ACL intact; confirm extent on MRI
- Distinguishing Feature
- Mechanical symptoms, preserved joint space, normal alignment
- Why it Matters for UKA
- Arthroplasty not indicated — arthroscopic/conservative management
- Distinguishing Feature
- Groin or thigh pain, restricted hip rotation, normal knee X-ray
- Why it Matters for UKA
- Wrong joint — examine the hip and spine before listing for knee surgery
Investigations
Standard Series:
- Weight-Bearing AP: Assess medial joint space narrowing. Look for "bone-on-bone".
- Lateral: Assess posterior wear (ACL status) and patellofemoral osteophytes.
- Skyline: Assess PF joint. Lateral facet wear? (Lateral facet wear is contraindication. Medial facet is debatable).
- 45-Degree PA (Rosenberg): Most sensitive view for posterior wear.
Stress Views:
- Valgus Stress X-ray: Confirms lateral compartment cartilage thickness is maintained. Confirms correctability of varus. This is the "Gold Standard" investigation for candidacy.
- Varus Stress X-ray: To check if medial gap opens (MCL integrity) - less common.
MRI:
- Not routinely needed if X-rays are classic.
- Role: Verify ACL integrity if Lachman is equivocal. Check lateral cartilage if stress view not available. Check PF cartilage.
- Pearl: MRI often "over-calls" damage. Normal aging cartilage changes in lateral compartment on MRI do not necessarily preclude UKA if X-ray is normal.
Bone Scan (Spect-CT):
- Can help identifying the "pain generator" if X-rays are mild (e.g., Grade 2 OA with unexplained severe pain).
Management Algorithm
The Decision Matrix
- Symptoms are mechanical and localized to one compartment.
- Radiographs show bone-on-bone in that compartment ONLY.
- ACL is clinically and radiographically intact.
- Deformity is mild and passively correctable.
- Patient accepts slightly higher revision risk for better function.
- Pain is diffuse or patellofemoral.
- ACL is deficient.
- Deformity is fixed or severe (greater than 15 deg).
- Inflammatory arthritis present.
- Obesity (BMI greater than 40) - though relative.
Summary: Select the right patient for the right reasons.
Surgical Technique
Core Principles of UKA
- Restoration of Constitutional Alignment: Do not aim for 0 degrees mechanical axis. Aim for the patient's pre-disease alignment (usually slight varus).
- Ligament Sparing: ACL and PCL are preserved. MCL is preserved (not released).
- Minimal Bone Resection: Take only enough bone to fit the implant (usually 6-8mm).
- Gap Balancing: Flexion and Extension gaps must be equal (especially for mobile bearing).
Intra-operative ACL Check: Even if MRI was normal, you MUST visualize and probe the ACL. Chronic attenuation or mucinous degeneration may not show on MRI. If the ACL is floppy or absent, you must abandon the UKA and perform a TKA.
RRRSurgical Goals
Hook:RRR: Resurface, Realign, Retain.
Complications
- Specific to UKA?
- Yes (Mobile)
- Incidence
- 1-2%
- Management
- Closed reduction or Revision
- Specific to UKA?
- Yes
- Incidence
- 5-10% (10y)
- Management
- Revision to TKA
- Specific to UKA?
- Yes (Exposure)
- Incidence
- Rare
- Management
- Repair + Brace or Convert to TKA
- Specific to UKA?
- Yes (Stress)
- Incidence
- less than 1%
- Management
- Fixation or Revision
- Specific to UKA?
- No (Common)
- Incidence
- 5-10%
- Management
- Revision
- Specific to UKA?
- No
- Incidence
- 0.5-1%
- Management
- DAIR or 2-stage Revision
Bearing Dislocation (Mobile Bearing):
- Cause: Flexion gap too loose, or MCL injury, or impingement on osteophytes.
- Presentation: Sudden pain, locking, lump.
- Treatment: Operative. Exchange bearing for thicker one (if loose).
Periprosthetic Fracture:
- Tibial: Vertical shear fracture through the keel slot. Usually intra-operative or stress fracture post-op.
Progression of OA:
- The most common "late" cause of failure. Lateral compartment wears out over 10-15 years.
- Requires conversion to TKA.
POLICEComplications of UKA
Hook:Call the POLICE when the UKA fails!
Postoperative Care
Rehabilitation Protocol
Patient mobilizes Full Weight Bearing (FWB) immediately. Crutches for comfort.
Most patients discharged DOS (Day Surgery) or Day 1. Criteria: Safe ambulation, pain control.
Clip removal. ROM should be 0-90 degrees minimum.
Wean crutches. Driving permitted. ROM 0-120.
Return to low-impact sports (Golf, Doubles Tennis, Cycling).
UKA vs TKA Recovery: UKA is significantly faster (weeks vs months). Less pain, less bleeding, less swelling. This is a key selling point for working patients.
Outcomes and Prognosis
Survival:
- Excellent survivorship in designer series (Oxford greater than 95% at 10 years).
- Registry data shows lower survivorship (85-90% at 10 years) compared to TKA.
- Why?: Lower threshold to revise (painful UKA is easily revised to TKA). TKA revision is a bigger deal, so surgeons/patients tolerate more pain before revising.
Function:
- UKA consistently scores better on Forgotten Knee Score (FKS).
- Better ROM (usually greater than 120 compared to 110 for TKA).
- More normal gait pattern.
Lateral UKA and Revision
Lateral Unicompartmental Knee Arthroplasty
Lateral UKA accounts for only about 10% of UKAs and is technically more demanding than medial — examiners expect you to know why it is different, not just that it exists.
- Indications: isolated lateral compartment OA (often post-traumatic or following lateral meniscectomy), a correctable valgus deformity, intact ACL, and preserved medial/patellofemoral compartments.
- Why it is different — kinematics: the lateral compartment is normally lax in flexion with greater femoral rollback and the femur lifts off, so a flat mobile bearing has a much higher dislocation/"spin-out" rate laterally (historically ~10%) than medially.
- Bearing solution: this is why a domed (biconcave) tibial bearing (which increases entrapment — see Yang) or a fixed-bearing design is generally preferred for lateral UKA; if intra-operative bearing stability is unacceptable, convert a mobile to a fixed bearing.
- Approach: usually a lateral parapatellar approach; beware over-correction (correct the valgus only to neutral, not into varus).
Guidelines, Registries & Global Practice
Global epidemiology & utilisation:
- UKA accounts for roughly 8-12% of primary knee arthroplasty in most major registries, but usage varies enormously (under 5% to over 40%) between surgeons and health systems — a function of surgeon selection philosophy rather than disease prevalence.
- Isolated anteromedial OA with an intact ACL — the ideal UKA substrate — is present in a substantial minority of patients otherwise listed for TKA, so most registries report UKA as "under-used" relative to the ideal indication pool.
Registry evidence (side by side):
- Region
- England & Wales
- Key UKA signal
- UKA revision ~2x TKA at 8 yrs, but lower mortality/complications (Liddle 2014); revision lowest at 40-60% surgeon usage (Liddle 2015)
- Region
- Australia
- Key UKA signal
- Higher cumulative revision than TKA; aseptic loosening and disease progression are leading revision diagnoses
- Region
- New Zealand
- Key UKA signal
- Higher revision rate than TKA; revision strongly volume-dependent
- Region
- Sweden
- Key UKA signal
- Long-standing data; mobile-bearing dislocation and loosening as failure modes; survival improves with experience
Guideline positions (side by side):
- Position on UKA
- Offer partial OR total knee replacement for single-compartment OA where appropriate; discuss higher revision but faster recovery of UKA
- Position on UKA
- Recognises UKA as an option for isolated unicompartmental OA with strict selection; emphasises patient selection over age/weight cut-offs
- Position on UKA
- UKA appropriate for anteromedial OA with functional ACL, correctable deformity, intact lateral/PF compartments
- Position on UKA
- Supports broadened modern indications (Oxford group) when anatomical criteria met; cautions on low-volume practice
Historical selection criteria (Kozinn & Scott):
- The classic restrictive criteria (age over 60, weight under 82 kg, low activity, deformity under 10-15 degrees) were popularised by Kozinn & Scott. Modern evidence (TOPKAT, designer series) shows these age/weight limits are NOT independent predictors of failure when anatomical criteria are met — the field has moved toward anatomical, not demographic, selection.
High- vs limited-resource practice variation:
- High-resource settings: robotic/navigated UKA increasingly used to improve component positioning; early registry signals suggest comparable-to-lower short-term revision, but long-term and cost-effectiveness data remain immature. Day-case/outpatient UKA is well established.
- Limited-resource settings: UKA's smaller implant, shorter stay, lower transfusion need and faster rehabilitation are attractive, but the technique-sensitivity and need for adequate UKA volume mean outcomes depend heavily on surgeon experience; in low-volume centres TKA may be the more reproducible choice.
Controversies and Areas of Uncertainty
1. The registry-versus-designer-series paradox:
- Designer centres report ~96-99% 10-year survival (Pandit 2011), while national registries report ~85-90%. The gap is partly real (case selection, learning curve, low-volume surgeons) and partly an artefact: a painful UKA is far easier to revise to a primary TKA than to revise a TKA, so the threshold to "revise" is lower. Revision should not be read as a pure measure of clinical failure.
2. Cemented vs cementless fixation:
- Cementless mobile-bearing UKA was introduced to reduce radiolucent lines and aseptic loosening. Some series and registry signals suggest lower revision for cementless designs, but the evidence is not yet definitive and cementing errors remain a recognised cause of early failure.
3. Robotic / navigated UKA:
- Robotic assistance improves component-positioning accuracy and reduces outliers; early registry data hint at lower short-term revision. However, long-term survival benefit and cost-effectiveness are unproven, and the dominant determinant of outcome remains correct patient selection.
4. Patellofemoral OA as a contraindication:
- Historically any PFJ disease excluded UKA. The Oxford group's work suggests that medial PFJ changes and even some lateral facet damage WITHOUT severe lateral grooving do not compromise medial UKA outcome. Severe lateral PFJ facet wear with grooving remains a contraindication. This area is genuinely debated.
5. UKA vs HTO in the young, active patient:
- For the young heavy labourer, HTO preserves bone and permits unrestricted activity but has a longer recovery and complicates future arthroplasty. UKA offers faster, more predictable pain relief. A prior HTO markedly worsens later UKA survival (66% vs 96% at 10 years; Rees 2001), so sequencing matters.
6. Expanding indications:
- Modern anatomical (rather than demographic) selection has extended UKA to younger, heavier and more active patients. Whether this broadening will hold up in long-term registry survival — or simply shift more revisions into the data — is still being resolved.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“question: Discuss the options of UKA vs HTO vs TKA.”
“question: How do you manage this?”
“question: Can you perform a UKA in this patient?”
MCQ Practice Points
Q: Which UKA design absolutely requires a competent MCL? A: Mobile Bearing (Oxford). Without a competent MCL, the bearing will spin out or dislocate. Fixed bearing is more tolerant of mild laxity.
Q: Is ACL deficiency a relative or absolute contraindication for Mobile Bearing UKA? A: Absolute Contraindication. ACL deficiency allows anterior tibial translation, causing posterior edge loading and rapid failure.
Q: What is the most common cause of re-operation after UKA in the first 5 years? A: Aseptic Loosening or Bearing Dislocation (depending on series/bearing). Late failure is usually Progression of OA.
Q: What is the upper limit of Fixed Flexion Deformity (FFD) for UKA? A: 15 degrees. Beyond this, the posterior capsule cannot be released sufficiently through a UKA approach to achieve extension.
Q: What is the 10-year survival rate of UKA in registry data? A: 90-95% (slightly lower than TKA). Designer series report higher (98%). UKA has 2-3x higher revision rate than TKA.
Q: What is the alignment goal in UKA? A: Constitutional varus (pre-disease alignment). Do NOT aim for 0 degrees mechanical axis - this overcorrects and overloads the lateral compartment.
Indications (ABCDE)
- A: ACL Intact
- B: Bone-on-bone medial
- C: Correctable deformity
- D: Deformity (FFD) under 15 deg
- E: Exclude lateral/PF
Contraindications
- Inflammatory Arthritis
- ACL deficiency
- Fixed Varus greater than 15 deg
- BMI greater than 40 (Relative)
Complications
- Bearing Dislocation (Mobile)
- Fracture (Tibial plateau)
- Loosening
- Progression of OA
Key Numbers
- 10-15% of all knees
- 90% 10-year survival
- 1-2% dislocation rate
- 2-3x revision vs TKA
Evidence
- TOPKAT (RCT): OKS equal to TKA at 5y
- Liddle NJR: UKA 2x revision, lower mortality
- Liddle 2015: optimal usage 40-60%
- Pandit: 96% survival at 10y (designer)
Pearl
- Don't overcorrect valgus
- Respect the ACL
- One finger pain test
- Avoid overstuffing (tight gap)
Evidence Base and Key Studies
TOPKAT — Total or Partial Knee Arthroplasty Trial
- 528 patients randomised to partial (PKR/UKA) or total knee replacement for medial OA across 27 UK centres.
- No difference in Oxford Knee Score at 5 years (mean difference 1.04, 95% CI minus 0.42 to 2.50; p=0.159).
- PKR was both more effective (0.240 additional QALYs) and less expensive (minus 910 pounds) over 5 years.
- Similar incidence of re-operations and complications between groups.
Adverse Outcomes UKA vs TKA — National Joint Registry
- 25,334 UKRs propensity-matched to 75,996 TKRs (101,330 total) in the NJR for England and Wales.
- UKA had worse implant survival: revision subhazard ratio 2.12 (95% CI 1.99-2.26) at 8 years.
- Mortality was significantly LOWER for UKA at every timepoint (8-year HR 0.85, 95% CI 0.79-0.92).
- UKA had fewer complications (VTE, MI, stroke), shorter stay and fewer readmissions.
- Per 100 patients switched from TKA to UKA: about one fewer death but three more re-operations within 4 years.
Oxford Phase 3 UKR — 1000 Cases (Designer-Centre Series)
- First 1000 minimally invasive medial Oxford UKRs by two surgeons, independently reviewed (mean 5.6 years).
- 10-year survival 96% (95% CI 92.5-99.5) counting all implant-related re-operations as failure.
- 10-year survival 99.8% if only revisions needing revision components are counted as failure.
- Commonest causes of re-operation: lateral OA progression (0.9%), bearing dislocation (0.6%), unexplained pain (0.6%).
- Mean maximum flexion 130 degrees; function better than standard open approach.
Optimal UKA Usage & the Volume Effect — NJR
- 41,986 UKAs from the NJR for England and Wales analysed.
- Non-linear relationship between a surgeon's UKA usage and revision risk.
- Optimal results when UKA constitutes 40-60% of knee arthroplasty practice; acceptable at 20% or more.
- 5-year survival 96% with optimal usage vs 90% for low-usage surgeons (about 5% of practice).
- Lowest usage surgeons have the HIGHEST revision rates — implying overly narrow, inappropriate selection.
UKA After Failed High Tibial Osteotomy
- 631 medial Oxford UKAs pooled from three series; 18 had a previous HTO.
- 10-year cumulative survival 96% for primary UKA vs only 66% after failed HTO (p less than 0.0001).
- 27.8% of post-HTO UKAs were revised vs 3.1% of primary UKAs.
Lateral UKA Bearing Dislocation — Domed vs Flat Tibia
- 9 studies, 937 lateral Oxford UKR knees (3 flat, 6 domed tibia).
- Bearing dislocation fell from 17% (flat) to 3.7% (domed biconcave) tibial design.
- 10-year survival excluding dislocation rose to 93% with the domed design.
- Most dislocations occurred at ~16 months; medial dislocations most common.