Posteromedial Impingement | Olecranon Osteophyte | Thrower's Elbow
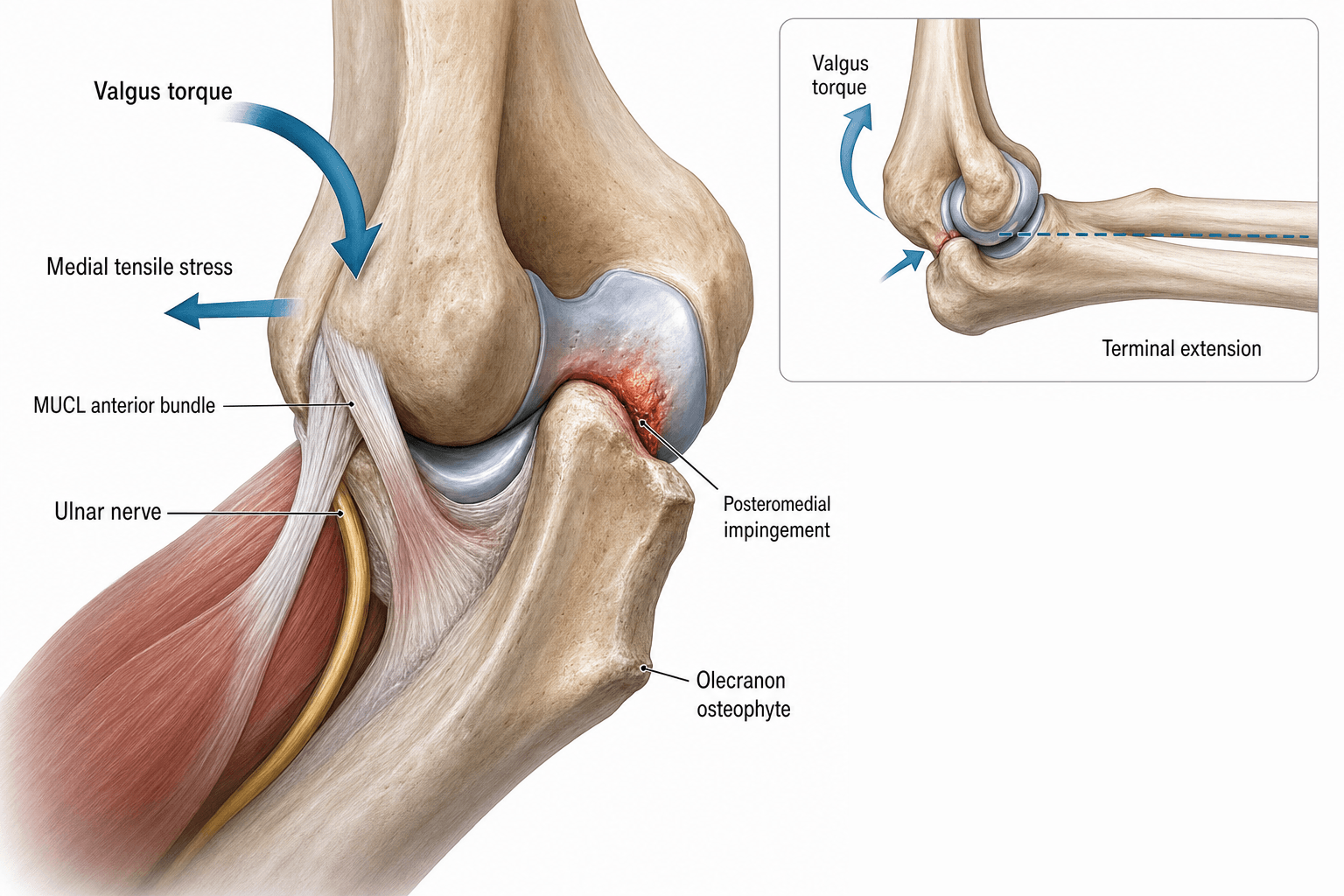
- Valgus extension overload = posteromedial olecranon tip impingement against olecranon fossa during terminal extension
- Repetitive valgus stress in overhead throwing creates shear forces at the posteromedial compartment
- Olecranon osteophyte formation is a reactive response to chronic impingement microtrauma
- UCL insufficiency increases valgus opening, worsening posteromedial impingement
- Isolated osteophyte debridement without addressing UCL insufficiency can DESTROY the elbow
- “VEO is one of the three valgus extension overload pathologies in throwers (with UCL injury and flexor-pronator strain)
- “Posteromedial elbow pain on forced extension = valgus extension overload until proven otherwise
- “Always stress-test the UCL before considering isolated osteophyte debridement
- “The 'valgus extension snap' test reproduces pain at the posteromedial olecranon tip
Valgus torque during the late cocking and early acceleration phases generates compressive forces laterally and tensile forces medially. Terminal extension drives the posteromedial olecranon tip into the medial wall of the olecranon fossa, producing osteophyte formation.
The anterior bundle of the UCL is the primary restraint to valgus stress. If attenuated or torn, valgus opening increases, causing the posteromedial olecranon to impinge earlier and more forcefully. Isolated debridement without UCL reconstruction can remove the osteophyte 'block' and accelerate valgus instability.
AP, lateral, oblique, and axial radiographs may show posteromedial olecranon osteophytes, olecranon fossa sclerosis, and loose bodies. CT is superior for characterising osteophyte size and location. MRI assesses UCL integrity, edema, and chondral damage.
Arthroscopic debridement is indicated ONLY when the UCL is competent or simultaneously reconstructed. Removing the posteromedial osteophyte in the setting of UCL insufficiency removes a secondary stabiliser and can be catastrophic. Always assess UCL integrity before surgery.
- Diagnosis
- Valgus extension snap test positive, UCL stable
- Treatment
- Arthroscopic posteromedial osteophyte debridement
- Key Pearl
- UCL MUST be proven intact before isolated debridement
- Diagnosis
- VEO signs PLUS positive moving valgus stress test
- Treatment
- UCL reconstruction WITH osteophyte debridement
- Key Pearl
- Addressing only the osteophyte will fail
- Diagnosis
- CT shows large osteophytes, MRI shows chondral damage
- Treatment
- Debridement plus loose body removal, manage UCL
- Key Pearl
- May need posteromedial chondral assessment
THROWERThrower's Elbow Differential
Hook:A THROWER's elbow has multiple overlapping pathologies - always assess ALL structures!
SCOPESurgical Decision-Making in VEO
Hook:SCOPE the elbow properly before you scope the elbow surgically!
Overview and Epidemiology
Valgus extension overload (VEO) is one of the most important pathologies in the overhead throwing athlete. During the acceleration phase of throwing, the elbow experiences valgus forces approaching 64 Nm, with the olecranon acting as a fulcrum. Terminal extension drives the posteromedial olecranon tip against the medial wall of the olecranon fossa. Over time, this repetitive microtrauma generates posteromedial osteophytes, chondral damage, and loose bodies. Critically, the UCL relationship means that isolated osteophyte debridement in the setting of UCL insufficiency can convert a stable but painful elbow into an unstable and catastrophically damaged one.
- Sport-specific: Predominantly overhead throwing athletes (baseball pitchers, javelin, cricket fast bowlers)
- Age: Typically ages 18-35 (peak competitive years)
- Incidence: Up to 90 percent of professional baseball pitchers have radiographic evidence of posteromedial osteophytes
- Bilateral: Dominant arm affected; non-dominant arm may show similar but milder changes
- Late cocking phase: Peak valgus torque of 50-74 Nm at the elbow
- Early acceleration: Maximum angular velocity and valgus stress
- Terminal extension: Olecranon tip engages in fossa at terminal 10-20 degrees
- Posteromedial shear: Valgus combined with extension concentrates force on medial olecranon
Pathophysiology
The anterior bundle of the ulnar collateral ligament (UCL) is the primary restraint to valgus stress at the elbow, providing approximately 55 percent of valgus stability. When the UCL is intact, the posteromedial olecranon tip experiences controlled contact with the olecranon fossa during terminal extension. However, when the UCL becomes attenuated or tears, valgus opening increases, driving the olecranon tip more medially and more forcefully into the fossa wall. This creates a vicious cycle: UCL insufficiency worsens posteromedial impingement, which generates osteophytes and chondral damage, which in turn produces loose bodies and inflammation that further compromise elbow mechanics.
The posteromedial osteophyte acts as a SECONDARY stabiliser against valgus stress when the UCL is insufficient. Surgical removal of this osteophyte without addressing UCL insufficiency removes this secondary restraint and can result in catastrophic valgus instability.
- Valgus Force
- Low
- Medial Tension
- Minimal
- Lateral Compression
- Low
- Posteromedial Shear
- Minimal
- Valgus Force
- Peak (50-74 Nm)
- Medial Tension
- Maximum UCL tension
- Lateral Compression
- High radiocapitellar
- Posteromedial Shear
- Increasing
- Valgus Force
- High
- Medial Tension
- UCL at limit
- Lateral Compression
- High
- Posteromedial Shear
- Peak posteromedial
- Valgus Force
- Decreasing
- Medial Tension
- Eccentric flexor-pronator
- Lateral Compression
- Moderate
- Posteromedial Shear
- Terminal impingement
Mechanism: Repetitive posteromedial impaction between olecranon tip and medial olecranon fossa wall
Location: Posteromedial aspect of olecranon tip (specific, not lateral)
Progression: Cartilage fibrillation leads to subchondral sclerosis, then osteophyte formation, then loose body generation
Key fact: The osteophyte is NOT the primary problem - it is a secondary response to the underlying biomechanical pathology
Stage 1: Posteromedial chondral softening from impaction
Stage 2: Chondral fibrillation and partial-thickness loss
Stage 3: Full-thickness chondral defect exposing subchondral bone
Stage 4: Loose body formation from delaminated cartilage and fractured osteophytes
End stage: Postero-medial compartment degenerative arthritis
IMPINGEValgus Extension Overload Pathology
Hook:IMPINGE reminds you that posteromedial osteophytes in VEO are a LOAD BEARING secondary stabiliser when the UCL is incompetent!
Classification and Types
Classification by Pathoanatomy
- Key Pathology
- Posteromedial osteophyte only
- UCL Status
- Intact (stable)
- Typical Findings
- Pain on terminal extension, no valgus laxity
- Treatment Principle
- Arthroscopic debridement alone is appropriate
- Key Pathology
- Osteophyte plus UCL attenuation/tear
- UCL Status
- Insufficient (lax)
- Typical Findings
- Valgus laxity on stress testing, medial pain
- Treatment Principle
- UCL reconstruction PLUS osteophyte debridement
- Key Pathology
- Osteophyte with fragmentation
- UCL Status
- Variable (assess individually)
- Typical Findings
- Mechanical locking, catching, effusions
- Treatment Principle
- Loose body removal plus address osteophyte and UCL
- Key Pathology
- Osteophyte compressing cubital tunnel
- UCL Status
- Variable
- Typical Findings
- Medial hand tingling, positive Tinel, nerve subluxation
- Treatment Principle
- Nerve transposition may be needed alongside debridement
The posteromedial impingement osteophyte in throwers must always be evaluated in the context of overall medial elbow stability.
Valgus throwing load is a tension medially (UCL/VEO) but a compression laterally at the radiocapitellar joint - and the classic examinable lateral lesion is osteochondritis dissecans (OCD) of the capitellum. It affects the adolescent or young thrower or gymnast (typically 11-16 years), presents with lateral elbow pain, an effusion, a flexion contracture (loss of terminal extension) and mechanical catching/locking if a fragment loosens, and is graded by stability: a stable lesion with an open capitellar physis is treated non-operatively (rest from throwing, often 3-6 months) with good healing, whereas an unstable lesion, a loose body, or a lesion in a closing or closed physis needs arthroscopic management (drilling, fixation, microfracture, or fragment removal with osteochondral grafting/OATS). Distinguish it from Panner disease - a self-limiting osteochondrosis of the whole capitellar ossific nucleus in the younger child (under about 10 years) that remodels with rest and does not form loose bodies. So the thrower's elbow has matched medial-tension (VEO/UCL) and lateral-compression (capitellar OCD) pathologies - always assess both compartments.
Clinical Assessment
- Sport: Overhead throwing (baseball pitcher, javelin, cricket fast bowler, tennis serve)
- Symptom: Posteromedial elbow pain during terminal extension
- Mechanical symptoms: Clicking, catching, locking (suggest loose bodies)
- Velocity loss: Decreased throwing velocity or accuracy
- Duration: Insidious onset over months to seasons (chronic)
- Medial symptoms: Tingling in ring and small fingers raises concern for ulnar neuritis
- Inspect: Carrying angle, medial swelling, muscle atrophy
- Palpate: Posteromedial olecranon tip tenderness (key finding), medial epicondyle, UCL
- Range of motion: Terminal extension painful, possible mechanical block
- Valgus stress testing: Moving valgus stress test, gravity valgus test, milking test
- Special test: Valgus extension snap test (reproduces posteromedial pain)
Technique: The patient's arm is stabilised while the examiner applies a valgus stress and quickly extends the elbow from 30 degrees of flexion to full extension.
Positive test: Pain at the posteromedial olecranon tip reproduced during terminal extension with valgus load.
Significance: Reproduces the impingement mechanism and localises pathology to the posteromedial compartment.
Critical caveat: A positive test does NOT exclude UCL insufficiency. Always perform the moving valgus stress test in addition. The moving valgus stress test is performed by applying a valgus torque as the elbow is flexed and extended through its range; pain between 120 and 70 degrees of flexion indicates UCL insufficiency.
- Technique
- Valgus stress applied while extending elbow rapidly
- Positive Finding
- Posteromedial pain at terminal extension
- Structure Tested
- Posteromedial olecranon impingement (VEO)
- Technique
- Valgus torque applied while flexing/extending through range
- Positive Finding
- Pain between 120 and 70 degrees flexion
- Structure Tested
- UCL anterior bundle insufficiency
- Technique
- Patient pulls thumb with elbow at 90 degrees, valgus applied
- Positive Finding
- Medial pain at UCL
- Structure Tested
- UCL insufficiency
- Technique
- Passive extension with direct posteromedial palpation
- Positive Finding
- Crepitus and pain at posteromedial tip
- Structure Tested
- Osteophyte or loose body in posteromedial gutter
- Key Localising Feature
- Pain specifically on terminal extension with valgus
- Discriminating Test
- Positive valgus extension snap test
- Key Imaging Finding
- Posteromedial olecranon osteophyte on CT/axial radiograph
- Key Localising Feature
- Medial pain during late cocking / early acceleration
- Discriminating Test
- Positive moving valgus stress test
- Key Imaging Finding
- UCL discontinuity or thickening with surrounding edema on MRI
- Key Localising Feature
- Medial epicondyle origin tenderness, pain on resisted wrist flexion
- Discriminating Test
- Resisted pronation reproduces pain
- Key Imaging Finding
- Flexor-pronator tendon thickening or partial tear on MRI
- Key Localising Feature
- Tingling in ring and small fingers, positive Tinel at cubital tunnel
- Discriminating Test
- Nerve conduction studies if equivocal
- Key Imaging Finding
- Ulnar nerve edema or subluxation on MRI
- Key Localising Feature
- Medial epicondyle pain in skeletally immature thrower
- Discriminating Test
- Pain on resisted flexion-pronation, open physis on X-ray
- Key Imaging Finding
- Widened medial epicondyle physis on AP radiograph
- Key Localising Feature
- Posterior pain, worse with throwing, night pain possible
- Discriminating Test
- Direct olecranon tenderness, positive resisted extension test
- Key Imaging Finding
- Olecranon fracture line on CT or MRI
VEO produces pain at terminal extension with a positive valgus extension snap test. UCL insufficiency produces pain during the mid-range (120-70 degrees) on the moving valgus stress test. Both frequently coexist. Missing the UCL component and performing isolated osteophyte debridement is a well-documented cause of surgical failure and accelerated elbow destruction.
The posterior-pain differential that must not be missed alongside VEO is an olecranon stress fracture. The same repetitive valgus-extension throwing load that drives posteromedial impingement also stresses the olecranon itself, producing a stress fracture (classically an oblique or transverse line, often physeal/metaphyseal in adolescents). Clues that it is a stress fracture rather than VEO: pain reproduced by resisted elbow extension (triceps loading) and focal olecranon tenderness rather than the terminal-extension valgus snap, sometimes with night pain. Plain films are often normal early - MRI (marrow oedema) or CT (the fracture line) confirms it, and it commonly coexists with UCL insufficiency and VEO because valgus laxity raises olecranon stress. Management is activity cessation for low-risk patterns, but a displaced or sclerotic non-union, or a persistent symptomatic line in a high-demand thrower, is fixed with an intramedullary screw (with bone grafting of a non-union) - and the underlying UCL/VEO problem must be addressed. Crucially, debriding a posteromedial osteophyte will not treat a coexisting olecranon stress fracture - image for it before operating.
Investigations
Imaging Protocol
Views: AP, lateral, oblique, and axial (45 degrees flexion) views of the elbow
Look for: Posteromedial olecranon osteophyte (best seen on axial view), olecranon fossa sclerosis, loose bodies, medial epicondyle calcification, joint space narrowing
Clinical correlation: Up to 90 percent of professional pitchers have radiographic osteophytes; correlate clinically before attributing symptoms to osteophytes
Indication: Characterise osteophyte size, location, and fossa depth; plan debridement extent
Superior to MRI for bone detail: Defines exact osteophyte morphology and any olecranon fossa involvement
Surgical planning: Determines how much bone can safely be removed without destabilising the elbow
Indication: Assess UCL integrity in EVERY patient with VEO findings
UCL assessment: Look for ligament thickening, partial-thickness undersurface tear, full-thickness tear, surrounding edema
Additional findings: Chondral damage, loose bodies, flexor-pronator pathology, ulnar nerve signal, bone marrow edema
Indication: Assess UCL laxity under valgus stress in real-time
Advantage: Shows dynamic joint space opening; can compare to contralateral side
Limitation: Operator-dependent; does not visualise deep chondral surfaces
The axial radiograph at 45 degrees of flexion is the single most valuable plain film view for VEO, as it profiles the posteromedial olecranon tip and clearly demonstrates osteophytes that may be hidden on standard AP and lateral views. If you suspect VEO, always request or perform this specific view. CT with 3D reconstruction is the gold standard for operative planning. MRI is mandatory to rule out UCL insufficiency before any surgical intervention.
Management Algorithm
Non-Operative Management
Goal: Reduce posteromedial impingement through biomechanical modification, inflammation control, and progressive rehabilitation
Rehabilitation Protocol
Rest: Complete throwing cessation (6-12 weeks minimum)
Anti-inflammatory measures: NSAIDs, ice, activity modification
Physical therapy: Address flexor-pronator strengthening, forearm pronation exercises
Biomechanical analysis: Video analysis of throwing mechanics to identify fault patterns
Progressive strengthening: Flexor-pronator mass, triceps, biceps
Range of motion: Gentle terminal extension stretching (avoid forceful extension)
Core and scapular stabilisation: Address proximal kinetic chain deficits
Gradual return to activity: Begin tossing program when pain-free
Interval throwing program: Graduated distance and intensity
Mechanics correction: Maintain corrected throwing pattern
Monitor symptoms: Any posteromedial pain = stop and reassess
Decision point: Failure at 12 weeks of conservative management indicates surgical evaluation
The most common cause of VEO is poor throwing mechanics, particularly inadequate trunk rotation, late trunk rotation, or dropping the elbow below shoulder height during the cocking phase. Biomechanical coaching and video analysis are essential components of non-operative management. Without correcting the underlying mechanics, the osteophyte will recur even after successful surgery.
Complications
- Incidence
- Reported in cases of debridement without UCL reconstruction
- Risk Factors
- Missed UCL insufficiency, aggressive resection
- Management
- Urgent UCL reconstruction; may need hinged external fixator
- Incidence
- Up to 30 percent without mechanics correction
- Risk Factors
- Return to throwing without biomechanical coaching
- Management
- Revision debridement only if mechanics addressed
- Incidence
- Progressive over career in throwers
- Risk Factors
- Chronic impingement, loose bodies, UCL laxity
- Management
- Arthroscopic chondral management; activity modification
- Incidence
- 5-15 percent association with VEO
- Risk Factors
- Osteophyte encroachment on cubital tunnel, traction
- Management
- Cubital tunnel release or anterior transposition
- Incidence
- Common in advanced VEO
- Risk Factors
- Osteophyte fragmentation, chondral delamination
- Management
- Arthroscopic removal; address underlying impingement
The most important complication to prevent is iatrogenic instability from inappropriate debridement. This is entirely preventable by: (1) performing a thorough pre-operative UCL assessment with physical examination and MRI, (2) planning osteophyte resection limits on CT, and (3) reconstructing the UCL whenever there is any question about ligament integrity. A conservative approach of leaving a small residual osteophyte is far preferable to over-resection and instability.
Outcomes and Prognosis
- Population
- Early VEO, UCL intact, willing to modify mechanics
- Expected Outcome
- 60-70 percent return to throwing with mechanics correction
- Return to Throwing
- 3-4 months with interval throwing program
- Population
- Symptomatic osteophyte, confirmed stable UCL
- Expected Outcome
- 85-90 percent return to prior level of competition
- Return to Throwing
- 3-6 months post-operatively
- Population
- VEO with UCL insufficiency
- Expected Outcome
- 80-90 percent return to throwing (professional athletes)
- Return to Throwing
- 12-18 months post-operatively
- Population
- UCL insufficient but not recognised
- Expected Outcome
- Poor; recurrent pain, instability, accelerated degeneration
- Return to Throwing
- Requires revision UCL reconstruction; outcomes inferior
Best prognosis: Isolated VEO with intact UCL, early intervention, good biomechanical coaching, arthroscopic debridement limited to osteophyte
Poor prognosis: Unrecognised UCL insufficiency treated with isolated debridement, chronic posteromedial chondral damage, multiple prior surgeries, inability to correct throwing mechanics
Key principle: The single greatest predictor of surgical success is accurate pre-operative assessment of UCL integrity.
Guidelines, Registries & Global Practice
- Baseball pitchers: Highest incidence worldwide (USA, Japan, Korea, Caribbean, Latin America)
- Javelin throwers: Significant prevalence in European and Commonwealth nations
- Cricket fast bowlers: Increasingly recognised in cricket-playing nations worldwide (England, South Asia, the West Indies, Australia)
- Other overhead sports: Tennis serve, volleyball spike, handball throwing motion
- Up to 90 percent of professional baseball pitchers have radiographic posteromedial osteophytes
- High-resource (USA, Japan, Australia): MRI and dynamic ultrasound for UCL assessment; advanced arthroscopic techniques with throwing mechanics analysis and biomechanical labs
- Limited-resource: Radiographs and clinical examination for diagnosis; open debridement when arthroscopy unavailable; rehabilitation-based management emphasised
- Universal principle: UCL integrity assessment is mandatory regardless of resource setting - the clinical examination (moving valgus stress test) is the most important tool
- Return-to-sport protocols: Standardised interval throwing programs are used globally regardless of resource level
- Diagnosis Emphasis
- Moving valgus stress test plus MRI for UCL; CT for osteophyte characterisation
- Acute Management
- Minimum 3 months rest, biomechanical coaching, flexor-pronator rehabilitation
- Surgical Approach
- Arthroscopic debridement if UCL intact; combined UCL reconstruction if insufficient
- Diagnosis Emphasis
- Clinical examination first; radiographs including axial view; MRI for UCL assessment
- Acute Management
- Structured physiotherapy and throwing modification; consider PRP injection adjunct
- Surgical Approach
- Arthroscopic debridement with careful patient selection; UCL reconstruction in specialist centres
- Diagnosis Emphasis
- Systematic assessment of all medial elbow structures; CT for surgical planning
- Acute Management
- Rehabilitation protocol with graduated return; biomechanical analysis essential
- Surgical Approach
- Arthroscopic technique with defined resection limits; combined procedures as indicated
- Diagnosis Emphasis
- High clinical suspicion in throwing athletes; ultrasound increasingly used for dynamic UCL assessment
- Acute Management
- Prolonged conservative management favoured before surgical intervention
- Surgical Approach
- Arthroscopic debridement standard; UCL reconstruction in specialist elbow centres
There is no dedicated global registry for VEO outcomes. Evidence comes primarily from retrospective case series from major throwing sports centres (American Sports Medicine Institute, Kerlan-Jobe Orthopaedic Clinic, and similar institutions). The evidence base is dominated by Level 4 studies, with biomechanical cadaveric studies providing the strongest support for the principle that osteophytes are secondary stabilisers. The return-to-play data after UCL reconstruction (approximately 83-90 percent in professional baseball) is among the best-studied outcomes in sports elbow surgery.
Record in every throwing athlete with posteromedial elbow pain:
- Moving valgus stress test result (positive or negative for UCL insufficiency)
- Valgus extension snap test result (positive or negative for VEO)
- UCL integrity on MRI (intact, partial tear, full tear)
- Osteophyte characterisation on CT (size, location, fossa involvement)
- Throwing mechanics assessment performed or referred
- Discussion of surgical risk if UCL insufficient: debridement alone is contraindicated
Missing the UCL component in a patient who proceeds to isolated osteophyte debridement is a well-documented source of surgical failure and medicolegal claims. Document the UCL assessment in every case.
Controversies & Areas of Uncertainty
Partial undersurface UCL tears pose a dilemma: some can be managed with rehabilitation and augmented repair, while others progress to require reconstruction. No consensus exists on the threshold for reconstruction versus repair in the context of simultaneous VEO. Decision-making is individualised based on sport, level of competition, and biomechanical demands.
The safe limit of posteromedial olecranon resection is debated. Biomechanical studies suggest that resection exceeding 4-6 mm of normal olecranon beyond the osteophyte may compromise stability. Intra-operative fluoroscopy and CT-based templating are recommended, but the exact limits vary by individual anatomy.
Internal brace augmentation (collagen-coated tape) during UCL reconstruction may allow accelerated rehabilitation, but long-term outcome data specific to VEO patients is limited. This technique is gaining acceptance in high-level throwing athletes.
PRP and stem cell injections for partial UCL tears and chondral damage associated with VEO remain investigational. Some centres report promising early results, but high-quality trials are lacking. These adjuncts should not replace established surgical principles.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old professional baseball pitcher presents with posteromedial right elbow pain for 4 months. The pain occurs during the late acceleration phase and is worse on terminal extension. He reports occasional clicking but no locking. Physical examination reveals tenderness at the posteromedial olecranon tip, a positive valgus extension snap test, and a negative moving valgus stress test. His UCL feels stable. Radiographs show a posteromedial olecranon osteophyte. What is your diagnosis and management?”
“A 28-year-old javelin thrower presents with medial and posteromedial elbow pain for 8 months. He has lost throwing distance and reports a 'pop' sensation. Examination reveals posteromedial olecranon tenderness, a positive valgus extension snap test, AND a positive moving valgus stress test with pain between 120 and 70 degrees. MRI shows a partial-thickness undersurface tear of the UCL with surrounding edema and a posteromedial osteophyte. How would you manage this?”
Key Pathomechanics
- Repetitive valgus stress during throwing drives posteromedial olecranon tip into olecranon fossa
- Terminal extension in valgus concentrates force on posteromedial compartment
- Osteophyte forms as reactive response to chronic impingement microtrauma
- UCL insufficiency increases valgus opening, worsening posteromedial impingement
- Posteromedial osteophyte acts as secondary valgus stabiliser when UCL is insufficient
Diagnosis
- Posteromedial elbow pain on terminal extension in overhead throwing athlete
- Valgus extension snap test positive (reproduces posteromedial pain at terminal extension)
- Axial radiograph at 45 degrees flexion shows posteromedial osteophyte best
- MRI mandatory to assess UCL integrity before any surgical intervention
- CT superior for characterising osteophyte size and planning resection limits
Treatment Algorithm
- Conservative first: rest, biomechanical coaching, flexor-pronator rehab (3 months trial)
- UCL intact with persistent VEO: arthroscopic osteophyte debridement and loose body removal
- UCL insufficient with VEO: UCL reconstruction PLUS osteophyte debridement (combined)
- NEVER debride osteophyte in UCL-insufficient elbow without simultaneous reconstruction
- Throwing mechanics correction is mandatory to prevent recurrence
Critical Pitfalls
- Missed UCL insufficiency is the most dangerous error in VEO management
- Isolated debridement with unrecognised UCL tear causes catastrophic instability
- Over-resection of olecranon beyond the osteophyte risks iatrogenic instability
- Failure to address throwing mechanics leads to osteophyte recurrence
- Ulnar nerve assessment is essential: osteophytes may compress the nerve in the cubital tunnel
Outcomes
- Conservative management: 60-70 percent return with mechanics correction
- Arthroscopic debridement (UCL intact): 85-90 percent return to competition
- UCL reconstruction plus debridement: 80-90 percent return to throwing
- Failed isolated debridement (missed UCL): poor outcomes, requires revision surgery
- Return to throwing timeline: 3-6 months (debridement alone) or 12-18 months (UCL reconstruction)
Evidence Base and Key Trials
Valgus extension overload in the pitching elbow
- Seminal paper describing the clinical syndrome of posteromedial olecranon impingement in throwing athletes
- Identified the relationship between valgus stress during throwing and posteromedial osteophyte formation
- Reported successful outcomes with osteophyte debridement in athletes with intact medial stabilisers
- Warned against debridement when valgus instability is present
Outcome of elbow surgery in professional baseball players
- Reported outcomes of arthroscopic osteophyte debridement in professional baseball players
- Demonstrated that concomitant UCL pathology was common and required simultaneous treatment
- Found that isolated debridement in the setting of UCL insufficiency led to poor outcomes
- Emphasised pre-operative assessment of valgus stability
Medial collateral ligament strain with partial posteromedial olecranon resection: a biomechanical study
- Cadaveric study quantifying the contribution of the posteromedial olecranon to valgus stability
- Demonstrated that the olecranon acts as a secondary stabiliser to valgus stress when the UCL is insufficient
- Showed that osteophyte resection in UCL-deficient elbows significantly increases valgus opening
- Recommended that any debridement in the setting of UCL insufficiency must be accompanied by ligament reconstruction
Outcome of ulnar collateral ligament reconstruction of the elbow in 1281 athletes: Results in 743 athletes with minimum 2-year follow-up
- Large retrospective review of over 1,200 overhead athletes treated surgically for medial elbow pathology
- Found that VEO was present in a significant proportion of athletes undergoing UCL reconstruction
- Outcomes were best when both UCL insufficiency and posteromedial impingement were addressed simultaneously
- Reported return-to-play rates of approximately 83 percent in professional baseball players after combined procedures
Arthroscopy of the elbow: a long-term clinical review
- Evaluated outcomes of isolated arthroscopic debridement in throwing athletes with VEO
- Demonstrated that careful patient selection (UCL intact) is critical for successful outcomes
- Reported that athletes who failed conservative management had good results with arthroscopic intervention
- Identified that pre-operative CT was more useful than MRI for surgical planning of osteophyte resection