Virchow's Triad | Risk Stratification | Prophylaxis Protocols | Prevention & Treatment
- Virchow's triad is the pathophysiological foundation: Stasis + Hypercoagulability + Endothelial injury
- Risk stratification is mandatory: Use Caprini score or NICE guidelines to determine prophylaxis intensity
- Extended prophylaxis for 35 days is standard after THA, TKA, and hip fracture surgery (ACCP Grade 1B)
- LMWH and DOACs are superior to aspirin alone for VTE prevention but aspirin is acceptable for lower-risk patients
- DVT diagnosis: Compression ultrasound (sensitivity over 95% for proximal DVT)
- PE diagnosis: CTPA is gold standard; V/Q scan if contrast contraindicated
- “Virchow's triad explains why ALL orthopaedic surgery patients are at VTE risk
- “Caprini score 5 or higher = high risk requiring chemical prophylaxis
- “LMWH started 12h preop (European) or 12-24h postop (North American) - know both protocols
- “DOACs (rivaroxaban, apixaban) are non-inferior to LMWH with better compliance
- “Post-thrombotic syndrome affects 20-50% of DVT patients - compression reduces risk
You MUST know the triad. Stasis (immobility), Hypercoagulability (trauma response, inherited disorders), Endothelial injury (surgery, fractures). Examiners expect you to explain how each component contributes to VTE risk in orthopaedic patients and how your prophylaxis strategy addresses each element.
Know Caprini Score cutoffs: Score 0-1 = low risk (early ambulation), 2 = moderate (mechanical), 3-4 = high (mechanical + chemical), 5 or higher = highest (extended prophylaxis 35 days). NICE guidelines are alternative. Must individualize based on bleeding risk.
Critical timing knowledge: LMWH 12h before surgery (European) OR 12-24h after surgery (North American). DOACs started 6-12h postop (rivaroxaban 6-10h, apixaban 12-24h). Never give before spinal/epidural - risk of epidural hematoma. Know contraindications.
35 days is the standard for THA, TKA, hip fracture (ACCP Grade 1B). VTE risk persists 6-12 weeks postop. Stopping at hospital discharge is suboptimal. Aspirin alone may be used for extended phase if LMWH used perioperatively (AAOS).
| Agent | Mechanism | Dosing | Advantages | Disadvantages |
|---|---|---|---|---|
| Enoxaparin (LMWH) | Anti-Xa and anti-IIa inhibition | 40mg SC daily or 30mg BD | Gold standard, reversible with protamine, renal dosing available | Injection required, HIT risk (0.5%), monitoring if renal impairment |
| Rivaroxaban (DOAC) | Direct Factor Xa inhibitor | 10mg PO daily | Oral, fixed dose, no monitoring, non-inferior to LMWH | No reversal agent (andexanet expensive), avoid CrCl less than 15 |
| Apixaban (DOAC) | Direct Factor Xa inhibitor | 2.5mg PO BD | Oral, renal-safe (less than 25% renal), low bleeding | Twice daily dosing, no reversal widely available |
| Aspirin | COX-1 inhibition (antiplatelet) | 100-300mg PO daily | Cheap, oral, low bleeding, patient familiarity | Inferior efficacy vs LMWH/DOAC, consider only for lower-risk or extended phase |
| Warfarin | Vitamin K antagonist | Target INR 2-3 | Oral, reversible with vitamin K/FFP, cheap | Requires INR monitoring, interactions, slow onset, bridging needed |
| UFH | Anti-IIa greater than anti-Xa | 5000 units SC BD-TDS | Fully reversible, short half-life, safe in renal failure | Highest HIT risk (2-3%), requires more frequent dosing |
SHEVirchow's Triad
Hook:SHE is at risk for VTE - Stasis, Hypercoagulability, Endothelial injury. All three present in major orthopaedic surgery!
HIPSCaprini Risk Factors (5-point items)
Hook:HIPS fractures and these factors score 5 points each on Caprini - automatic high-risk status!
CLOTDVT Clinical Features
Hook:Look for a CLOT - Calf pain, Leg swelling, Observable veins, Temperature change. But remember: 50% of DVTs are asymptomatic!
Overview and Epidemiology
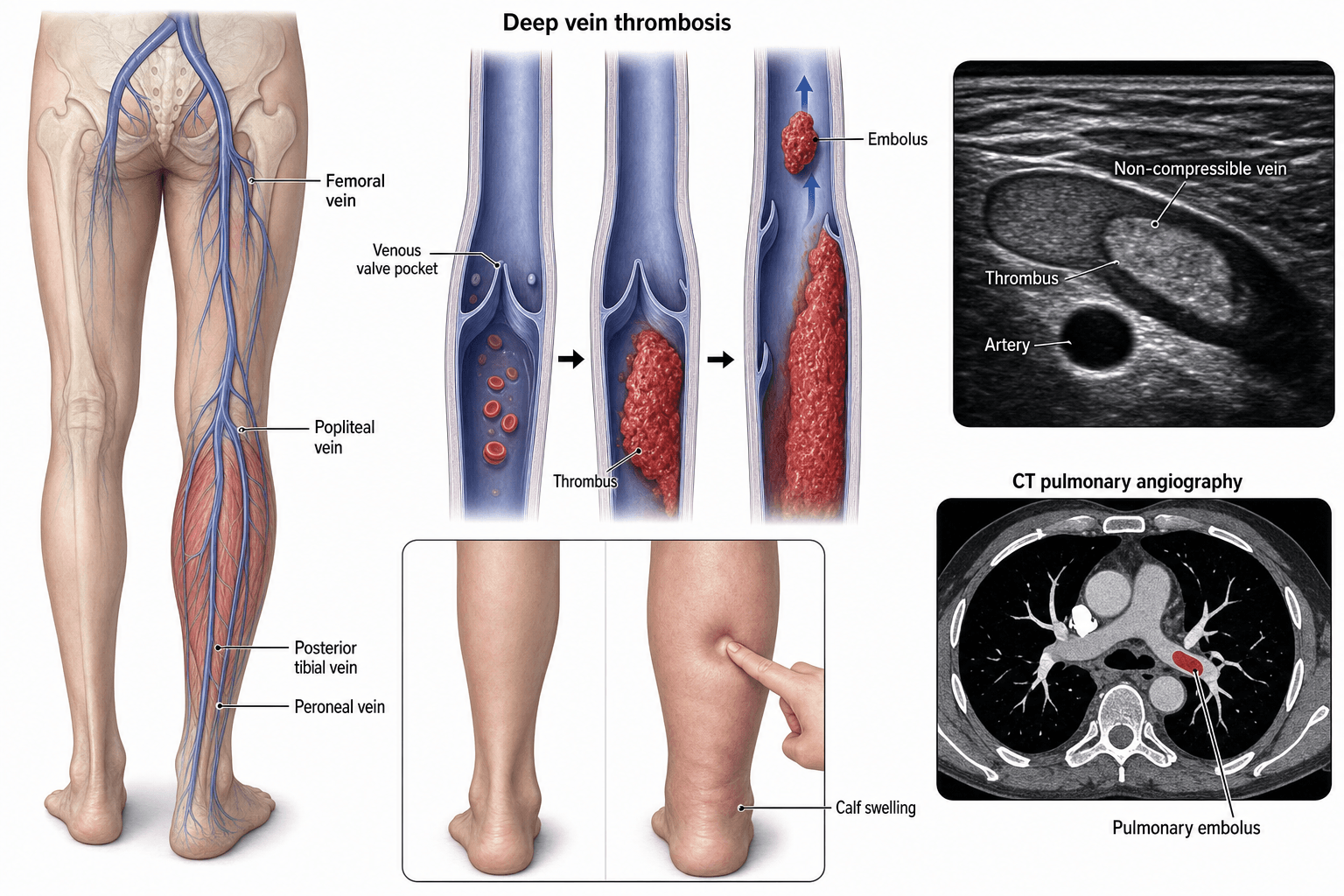
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), represents one of the most significant preventable complications in orthopaedic surgery. Understanding VTE pathophysiology, risk stratification, and evidence-based prophylaxis is mandatory knowledge for fellowship examinations.
Definition:
- DVT: Thrombus formation in the deep venous system, most commonly in lower extremity (iliac, femoral, popliteal, calf veins)
- PE: Embolization of thrombus to pulmonary arterial circulation, causing ventilation-perfusion mismatch
- VTE: Umbrella term encompassing the spectrum from asymptomatic calf DVT to fatal massive PE
Epidemiology in Orthopaedic Surgery:
| Procedure | DVT Rate | Proximal DVT | Fatal PE |
|---|---|---|---|
| Total hip arthroplasty | 40-60% | 15-25% | 0.5-2% |
| Total knee arthroplasty | 40-84% | 10-20% | 0.5-1.5% |
| Hip fracture surgery | 40-60% | 15-30% | 2-7% |
| Knee arthroscopy | 5-15% | 1-2% | Less than 0.1% |
| Spine surgery | 15-40% | 5-10% | 0.3-0.5% |
| Lower limb trauma | 40-80% | 10-20% | 1-2% |
With Prophylaxis:
- DVT rates reduced to 10-20% (mechanical only) or 1-5% (mechanical + chemical)
- Fatal PE reduced to less than 0.5% with adequate prophylaxis
- NNT (number needed to treat) approximately 7 to prevent one symptomatic VTE
VTE remains a leading cause of preventable hospital death in Australia. The Australian Commission on Safety and Quality in Health Care mandates VTE risk assessment for all hospital admissions. Compliance with prophylaxis protocols is a key hospital performance indicator.
Pathophysiology - Virchow's Triad
Rudolf Virchow described his famous triad in 1856, identifying three factors that predispose to venous thrombosis. All three are present in major orthopaedic surgery, explaining the extremely high VTE risk in this population.
Venous Stasis
Mechanism:
- Normal venous return depends on calf muscle pump action and competent venous valves
- Immobility eliminates calf muscle pump function
- Venous pooling allows activated clotting factors to accumulate locally
- Reduced clearance of activated factors overwhelms natural anticoagulant systems
Orthopaedic Causes:
- Preoperative immobility (hip fracture, multiple trauma)
- Intraoperative positioning (hip flexion, rotation)
- Postoperative bed rest and reduced mobility
- Cast immobilization
- Lower limb paralysis (stroke, spinal cord injury)
- Tourniquet application (distal stasis during inflation)
Prevention Strategies:
- Early mobilization (day 0-1 post-surgery when safe)
- Mechanical prophylaxis (IPC devices, GCS)
- Ankle exercises and calf pump activation
- Avoiding prolonged hip flexion
- Physiotherapy protocols
The calf muscle pump generates pressures of 200-300 mmHg during contraction, propelling blood centrally through competent valves. Loss of this pump (immobility) reduces venous velocity by 50% and allows thrombus formation in valve pockets.
Combined Effect in Orthopaedic Surgery:
All three elements of Virchow's triad are present simultaneously in major orthopaedic procedures, creating a "perfect storm" for VTE:
- Preoperative immobility (stasis)
- Surgical trauma and tissue factor release (hypercoagulability)
- Direct vessel injury and manipulation (endothelial injury)
This explains why THA and TKA have the highest VTE risk of any elective surgical procedures and why prophylaxis is mandatory.
Clinical Presentation
Deep Vein Thrombosis - Clinical Features
Important: Up to 50% of DVTs are asymptomatic, detected only on screening ultrasound. Clinical diagnosis is unreliable (sensitivity 50-60%, specificity 50%).
Symptoms:
- Calf pain (most common) - often described as "cramping" or "tightness"
- Leg swelling - may be acute or insidious onset
- Warmth and redness over affected area
- Heaviness or aching in leg
- Pain worse with standing or walking
Signs:
- Unilateral leg edema (more than 3cm difference significant)
- Pitting edema
- Calf tenderness on palpation
- Increased warmth
- Erythema (may be subtle)
- Superficial venous distension
- Homans' sign (calf pain on forced dorsiflexion) - unreliable, only 50% sensitive
| Clinical Feature | Points |
|---|---|
| Active cancer (treatment within 6 months or palliative) | +1 |
| Paralysis, paresis, or recent lower limb immobilization | +1 |
| Bedridden more than 3 days or major surgery within 12 weeks | +1 |
| Localized tenderness along deep venous system | +1 |
| Entire leg swollen | +1 |
| Calf swelling more than 3cm compared to other leg | +1 |
| Pitting edema confined to symptomatic leg | +1 |
| Collateral superficial veins (non-varicose) | +1 |
| Previously documented DVT | +1 |
| Alternative diagnosis at least as likely | -2 |
Wells Score Interpretation:
- 0 or less: Low probability (5% DVT prevalence)
- 1-2: Moderate probability (17% DVT prevalence)
- 3 or more: High probability (53% DVT prevalence)
In postoperative orthopaedic patients, the Wells score has limited utility because multiple risk factors are already present (recent surgery, immobility). Have a LOW threshold for imaging. If clinical suspicion exists, proceed directly to compression ultrasound regardless of Wells score.
Differential Diagnosis of the Painful, Swollen Postoperative Leg
| Condition | Distinguishing Features | Key Investigation |
|---|---|---|
| Deep vein thrombosis | Unilateral calf swelling more than 3cm, calf tenderness, warmth; often asymptomatic postop | Compression ultrasound (non-compressible vein) |
| Cellulitis | Erythema with well-defined advancing margin, fever, raised inflammatory markers, possible portal of entry | Clinical; ultrasound to exclude coexisting DVT |
| Ruptured Baker's cyst | Sudden calf pain, crescent bruise around malleolus, history of knee effusion or arthritis | Ultrasound (fluid tracking from popliteal cyst) |
| Superficial thrombophlebitis | Tender, palpable cord along a superficial vein, localised erythema | Ultrasound (superficial vein thrombus, deep system patent) |
| Postoperative haematoma | Localised swelling and bruising near wound, recent surgery, possible falling haemoglobin | Ultrasound or CT; assess coagulation |
| Compartment syndrome | Pain out of proportion, pain on passive stretch, tense compartment, paraesthesia | Clinical diagnosis; compartment pressures |
| Lymphoedema / chronic venous insufficiency | Bilateral or chronic, non-pitting (lymphoedema) or pitting with skin changes, no acute onset | Clinical; ultrasound if acute change |
| Calf muscle tear / gastrocnemius strain | Sudden pain during activity, localised tenderness at musculotendinous junction | Clinical; ultrasound if uncertain |
Investigations
DVT Diagnostic Pathway
D-dimer:
- Highly sensitive (95%) but poorly specific (50%)
- Elevated in: surgery, trauma, pregnancy, cancer, infection, inflammation
- Negative D-dimer reliably excludes DVT in LOW pretest probability patients
- In postoperative orthopaedic patients: D-dimer is almost always elevated - DO NOT use to rule out DVT
D-dimer has NO role in ruling out DVT in postoperative orthopaedic patients. It will be elevated from surgery and does not add diagnostic value. Proceed directly to imaging if DVT is suspected.
Compression Ultrasound (Gold Standard):
- Sensitivity: 95% for proximal DVT, 70-80% for calf DVT
- Specificity: 98%
- Technique: Inability to fully compress vein with probe pressure is diagnostic
- Also visualizes thrombus echogenicity and venous flow patterns
- Advantages: Non-invasive, no radiation, bedside available
When to Image:
- Any clinical suspicion of DVT postoperatively
- Unexplained leg swelling, pain, or warmth
- Before anticoagulation cessation if DVT was diagnosed
- PE diagnosed - evaluate for DVT source
Other Imaging:
- CT venography: For pelvic and IVC extension, if US non-diagnostic
- MR venography: Alternative for pelvic veins, no radiation
- Contrast venography: Historical gold standard, rarely used now (invasive)
| Probability | D-dimer | Ultrasound | Interpretation |
|---|---|---|---|
| Low (Wells 0 or less) | If negative: DVT excluded | If D-dimer positive: proceed to US | Serial US if negative but high suspicion |
| Moderate (Wells 1-2) | Not reliable | Proceed directly | Consider repeat US in 5-7 days if negative |
| High (Wells 3+) | Do not use | Proceed directly | Consider venography if negative and high suspicion |
| Postoperative ortho | Do not use | Proceed directly | Low threshold for imaging |
Management
Risk Stratification Systems
Caprini Score: The Caprini Risk Assessment Model is the most widely used tool for VTE risk stratification in surgical patients.
| 1 Point Each | 2 Points Each | 3 Points Each | 5 Points Each |
|---|---|---|---|
| Age 41-60 | Age 61-74 | Age 75 or more | Hip, pelvis, leg fracture |
| Minor surgery | Arthroscopic surgery | Prior VTE | Stroke (less than 1 month) |
| BMI over 25 | Major surgery over 45 min | Family history VTE | Spinal cord injury |
| Varicose veins | Malignancy | Positive thrombophilia | Elective arthroplasty |
| OCP/HRT | Bed rest over 72h |
Caprini Score Interpretation:
- 0: Very low risk (0.5% VTE) - Early ambulation only
- 1-2: Low risk (1.5% VTE) - Mechanical prophylaxis
- 3-4: Moderate risk (3% VTE) - Mechanical + chemical prophylaxis
- 5 or more: High risk (6% VTE) - Mechanical + chemical + extended prophylaxis (35 days)
NICE Guidelines: UK National Institute for Health and Care Excellence provides alternative risk assessment.
Key Principles:
- ALL orthopaedic inpatients require VTE risk assessment
- ALL patients undergoing THA, TKA, hip fracture surgery are automatically HIGH RISK
- Must also assess bleeding risk to balance prophylaxis
Prophylaxis must balance VTE risk against bleeding risk. Consider bleeding risk factors: active bleeding, severe thrombocytopenia (platelets less than 50), coagulopathy, high-bleeding-risk surgery (spine, intracranial), recent major bleeding. If bleeding risk is high, use mechanical prophylaxis only until bleeding risk diminishes.
Surgical Management - IVC Filters
Inferior Vena Cava (IVC) Filter Indications
Absolute Indications:
- Acute proximal DVT or PE with absolute contraindication to anticoagulation
- Recurrent PE despite adequate anticoagulation
- Complications of anticoagulation requiring cessation (major bleeding)
Relative Indications (Controversial):
- Prophylactic filter in very high-risk trauma (controversial, not recommended routinely)
- Free-floating iliofemoral thrombus (some advocate, others anticoagulate)
- Massive PE with residual DVT where further embolization would be fatal
- Poor cardiopulmonary reserve where any PE would be catastrophic
NOT Indicated:
- Routine prophylaxis in trauma or orthopaedic surgery
- As alternative to anticoagulation when anticoagulation is feasible
- For calf DVT only
Do NOT place IVC filters for VTE prophylaxis in trauma or orthopaedic patients who can receive anticoagulation. The PREPIC-2 trial showed no benefit of prophylactic filters in addition to anticoagulation, with increased DVT rates in filter group. Filters are for patients who CANNOT be anticoagulated.
Complications
| Complication | Incidence | Presentation | Management |
|---|---|---|---|
| Post-thrombotic syndrome | 20-50% after proximal DVT | Chronic leg swelling, pain, skin changes, ulceration | Prevention: compression stockings for 2 years. Treatment: compression, elevation, wound care for ulcers |
| Recurrent VTE | 5-10% at 1 year on anticoagulation | New DVT or PE symptoms | Ensure therapeutic anticoagulation, consider extended/indefinite therapy |
| Chronic thromboembolic pulmonary hypertension (CTEPH) | 2-4% after PE | Persistent dyspnea 6+ months post-PE | Referral to pulmonary hypertension centre, pulmonary endarterectomy |
| Phlegmasia cerulea dolens | Rare | Massive iliofemoral DVT, cyanotic limb, compartment syndrome risk | Urgent surgical thrombectomy or catheter-directed thrombolysis, fasciotomy if compartment syndrome |
| Anticoagulation bleeding | 3-5% major bleeding on therapeutic anticoagulation | GI bleed, intracranial hemorrhage, surgical site bleeding | Hold anticoagulation, reversal agents, transfusion, surgical hemostasis if needed |
| Heparin-induced thrombocytopenia (HIT) | 0.5% with LMWH, 2-3% with UFH | Platelet drop more than 50% at 5-14 days, paradoxical thrombosis | Stop all heparin, switch to non-heparin anticoagulant (argatroban, fondaparinux) |
Heparin-Induced Thrombocytopenia is a prothrombotic emergency despite low platelets. 4Ts score (Thrombocytopenia, Timing, Thrombosis, oTher causes) helps assess probability. If HIT suspected: (1) Stop ALL heparin immediately, (2) Start alternative anticoagulant (argatroban, fondaparinux - NOT warfarin alone), (3) Send HIT antibody testing. HIT can cause limb loss, stroke, PE, and death.
Evidence Base
RECORD Trials (2008)
- Rivaroxaban 10mg daily superior to enoxaparin 40mg for VTE prevention after THA and TKA
- RECORD1 (THA, PMID 18579811): total VTE 1.1% vs 3.7%; major VTE 0.2% vs 2.0% (rivaroxaban vs enoxaparin)
- RECORD3 (TKA, PMID 18579812): total VTE 9.6% vs 18.9% (rivaroxaban vs enoxaparin)
- No significant difference in major bleeding in either trial
ADVANCE Trials (2010)
- Apixaban 2.5mg BD at least non-inferior to enoxaparin 40mg for VTE prevention after arthroplasty
- ADVANCE-2 (TKA, Lancet, PMID 20206776): total VTE 15% apixaban vs 24% enoxaparin (RR 0.62)
- ADVANCE-3 (THA, N Engl J Med, PMID 21175312): total VTE 1.4% vs 3.9% (RR 0.36, superior)
- Major or clinically relevant non-major bleeding not increased (and numerically lower) with apixaban
EPCAT II Trial (2018)
- Aspirin 81mg daily non-inferior to rivaroxaban 10mg for extended prophylaxis after THA/TKA
- Symptomatic VTE: 0.64% aspirin (11/1707) vs 0.70% rivaroxaban (12/1717) at 90 days
- ALL patients received rivaroxaban 10mg daily for first 5 days postoperatively before randomisation
- Major and clinically relevant bleeding similar between groups
PREPIC-2 Trial (2015)
- Retrievable IVC filter plus anticoagulation vs anticoagulation alone in 399 patients with high-risk acute PE
- No reduction in symptomatic recurrent PE at 3 months: 6 patients (3.0%) with filter vs 3 (1.5%) control (RR 2.00, p=0.50)
- No significant difference in recurrent DVT, major bleeding or death; filter thrombosis in 3 patients
- Filters added to anticoagulation showed no benefit
SOX Trial - Compression Stockings for PTS Prevention (2014)
- Multicentre randomised placebo-controlled trial of active vs placebo elastic compression stockings worn for 2 years after a first proximal DVT (806 patients)
- Cumulative incidence of post-thrombotic syndrome 14.2% active vs 12.7% placebo (adjusted HR 1.13, 95% CI 0.73-1.76, p=0.58)
- No benefit even in the per-protocol analysis of frequent stocking users
- Findings do not support routine elastic compression stockings to prevent PTS after DVT
Global Burden of VTE (2014)
- Systematic review of the global disease burden of VTE across low-, middle- and high-income countries
- Annual VTE incidence 0.75-2.69 per 1000 population in Western Europe, North America, Australia and Southern Latin America
- Incidence rises to 2-7 per 1000 in those aged 70 years or more; lower in Chinese and Korean populations but burden remains high due to ageing
- Hospital-associated VTE was the leading cause of disability-adjusted life-years lost in low- and middle-income countries and second in high-income countries
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman is scheduled for elective total hip arthroplasty for osteoarthritis. She has well-controlled hypertension and type 2 diabetes. What is your VTE prophylaxis strategy?”
“A 72-year-old man is 5 days post total knee arthroplasty. He develops sudden onset dyspnea, pleuritic chest pain, and is tachycardic at 110 bpm. SpO2 is 88% on room air. What is your management?”
“A 58-year-old man with hip fracture also has active GI bleeding from a peptic ulcer. He requires surgery within 24-48 hours. How do you manage VTE prophylaxis?”
Guidelines, Registries & Global Practice
Global Epidemiology:
VTE is a major global cause of preventable death and disability. A systematic review for the International Society on Thrombosis and Haemostasis (Raskob et al, Arterioscler Thromb Vasc Biol 2014, PMID 25304324) reported an annual VTE incidence of 0.75-2.69 per 1000 population across Western Europe, North America, Australia and Southern Latin America, rising to 2-7 per 1000 in those aged 70 years or more. Incidence is lower in Chinese and Korean populations, but the disease burden remains high because of population ageing. Hospital-associated VTE - including surgery and major lower-limb trauma - is the dominant contributor and the leading cause of disability-adjusted life-years lost in low- and middle-income countries. This global burden underpins the worldwide convergence on systematic risk assessment and prophylaxis.
Side-by-Side Guideline Comparison:
| Body (region) | First-line agent | Aspirin role | Extended duration (THA/TKA) | Mechanical prophylaxis |
|---|---|---|---|---|
| ACCP / CHEST (North America) | LMWH preferred; DOAC, fondaparinux, warfarin or aspirin acceptable | Acceptable alternative (Grade 1B vs no prophylaxis) | At least 10-14 days, extend to 35 days (Grade 2B) | Add IPC during hospital stay (Grade 2C) |
| AAOS (USA) | Pharmacological + mechanical; agent at surgeon discretion | Endorsed as acceptable, supported by EPCAT II | Recommends prophylaxis but no single duration mandated | Recommended in addition to chemical prophylaxis |
| NICE NG89 (UK) | LMWH (or LMWH then aspirin) for THA; aspirin or LMWH or DOAC for TKA | Explicitly offered as an option (NG89) | THA up to 28-35 days; TKA up to 14 days | Offer mechanical (IPC or stockings) on admission |
| ESVS / EFORT (Europe) | LMWH or DOAC | Reserved for lower-risk or extended phase | Up to 35 days for THA and hip fracture | Combine with mechanical methods |
| eTG / NHMRC (Australia) | LMWH or DOAC; aligns with ACCP | Used for lower-risk patients or extended phase | 35 days for THA, TKA and hip fracture | IPC and early mobilisation |
The major guidelines now broadly agree on three principles: every major-orthopaedic patient is high-risk and needs combined mechanical plus pharmacological prophylaxis; LMWH and DOACs are the most effective agents; and aspirin is an acceptable option in selected (lower-risk or extended-phase) patients following the EPCAT II evidence. The main practice variation is around aspirin's prominence (greater in North America and the UK) and the precise extended duration.
Registry and System-Level Evidence:
National joint registries (the Australian AOANJRR, the National Joint Registry for England, Wales, Northern Ireland and the Isle of Man, and the American Joint Replacement Registry) capture arthroplasty volumes, implant survival and, increasingly, 90-day readmissions including symptomatic VTE, providing real-world denominators for prophylaxis policy. At the system level, the World Health Organization, the UK NHS (which mandated risk assessment of admitted patients), and the Australian Commission on Safety and Quality in Health Care all classify hospital-acquired VTE as a reportable patient-safety indicator, driving mandatory risk-assessment and prophylaxis bundles.
Practice Variation and Access:
Access to specific agents varies by jurisdiction. In Australia, enoxaparin, rivaroxaban and apixaban are subsidised through the Pharmaceutical Benefits Scheme for arthroplasty prophylaxis, and dabigatran is not currently approved for this indication; aspirin is available without prescription. In lower-income settings, LMWH cost and the lack of monitoring infrastructure for warfarin make low-cost oral options (including aspirin) and mechanical prophylaxis especially important. Across all systems, smoking is an independent, modifiable VTE risk factor: preoperative cessation (Australian patients can be referred to Quitline on 13 7848) for four or more weeks reduces perioperative complications.
For the viva, frame VTE prophylaxis as a globally standardised process: mandatory risk assessment, combined mechanical and pharmacological prophylaxis for all major-orthopaedic patients, extended duration (up to 35 days) after hip and knee replacement and hip fracture, with LMWH or a DOAC first-line and aspirin acceptable in selected patients. Hospital-acquired VTE is a reportable patient-safety indicator in most health systems, making prophylaxis a medicolegal as well as clinical obligation.
Virchow's Triad (SHE)
- Stasis: Immobility, venous pooling - treat with mechanical prophylaxis, early mobilization
- Hypercoagulability: Trauma, surgery, inherited thrombophilia - treat with chemical prophylaxis
- Endothelial injury: Surgery, fractures, cement - minimize with gentle technique
- All three present in major orthopaedic surgery - explains high VTE risk
Risk Stratification (Caprini)
- Score 0: Very low risk (0.5%) - early ambulation only
- Score 1-2: Low risk (1.5%) - mechanical prophylaxis
- Score 3-4: Moderate risk (3%) - mechanical + chemical prophylaxis
- Score 5+: High risk (6%) - mechanical + chemical + extended prophylaxis (35 days)
- 5-point factors: Hip/pelvis/leg fracture, prior VTE, stroke, spinal cord injury, arthroplasty
Chemical Prophylaxis Agents
- Enoxaparin: 40mg SC daily, start 12-24h postop, gold standard LMWH
- Rivaroxaban: 10mg PO daily, start 6-10h postop, Factor Xa inhibitor
- Apixaban: 2.5mg PO BD, start 12-24h postop, renal-safe DOAC
- Aspirin: 100-300mg daily, acceptable for extended phase or lower-risk patients
- All THA/TKA/hip fracture: 35 days extended prophylaxis (ACCP Grade 1B)
DVT Diagnosis
- Wells Score: 3+ = high probability (53% prevalence)
- D-dimer: DO NOT use postoperatively (always elevated)
- Compression ultrasound: Gold standard, 95% sensitive for proximal DVT
- Clinical features: Calf pain, unilateral leg swelling, warmth (CLOT mnemonic)
- 50% of DVTs are asymptomatic
PE Diagnosis and Severity
- CTPA: Gold standard (95% sensitivity and specificity)
- Low risk PE: Stable, no RV dysfunction - anticoagulation, consider outpatient
- Intermediate PE: Stable, RV dysfunction - anticoagulation, close monitoring
- Massive PE: Hemodynamic instability (SBP less than 90) - thrombolysis, embolectomy, ECMO
- Biomarkers: Troponin and BNP for risk stratification
Key Timing Points
- LMWH: 12h before (European) or 12-24h after surgery (North American)
- Rivaroxaban: 6-10 hours postoperatively
- Apixaban: 12-24 hours postoperatively
- Neuraxial: LMWH 12h before and 4h after epidural manipulation
- DOACs: 24-48h washout before neuraxial procedures
Key Trials
- RECORD trials: Rivaroxaban superior to enoxaparin for THA/TKA prophylaxis
- ADVANCE trials: Apixaban non-inferior to enoxaparin with lower bleeding
- EPCAT II: Aspirin non-inferior to rivaroxaban for extended prophylaxis (after initial DOAC)
- PREPIC-2: IVC filters do not reduce PE when anticoagulation given
- SOX trial: Compression stockings showed no PTS benefit (controversial)
Contraindications to Chemical Prophylaxis
- Active bleeding or high bleeding risk
- Severe thrombocytopenia (platelets less than 50)
- Recent intracranial hemorrhage or neurosurgery
- Epidural/spinal within timing window
- HIT (for heparin products)
- If contraindicated: maximize mechanical prophylaxis, consider IVC filter