Inadequate 25-OH Vitamin D | Rickets in Children | Osteomalacia in Adults
- Vitamin D deficiency causes rickets in children (growth plate abnormalities) and osteomalacia in adults (defective mineralization)
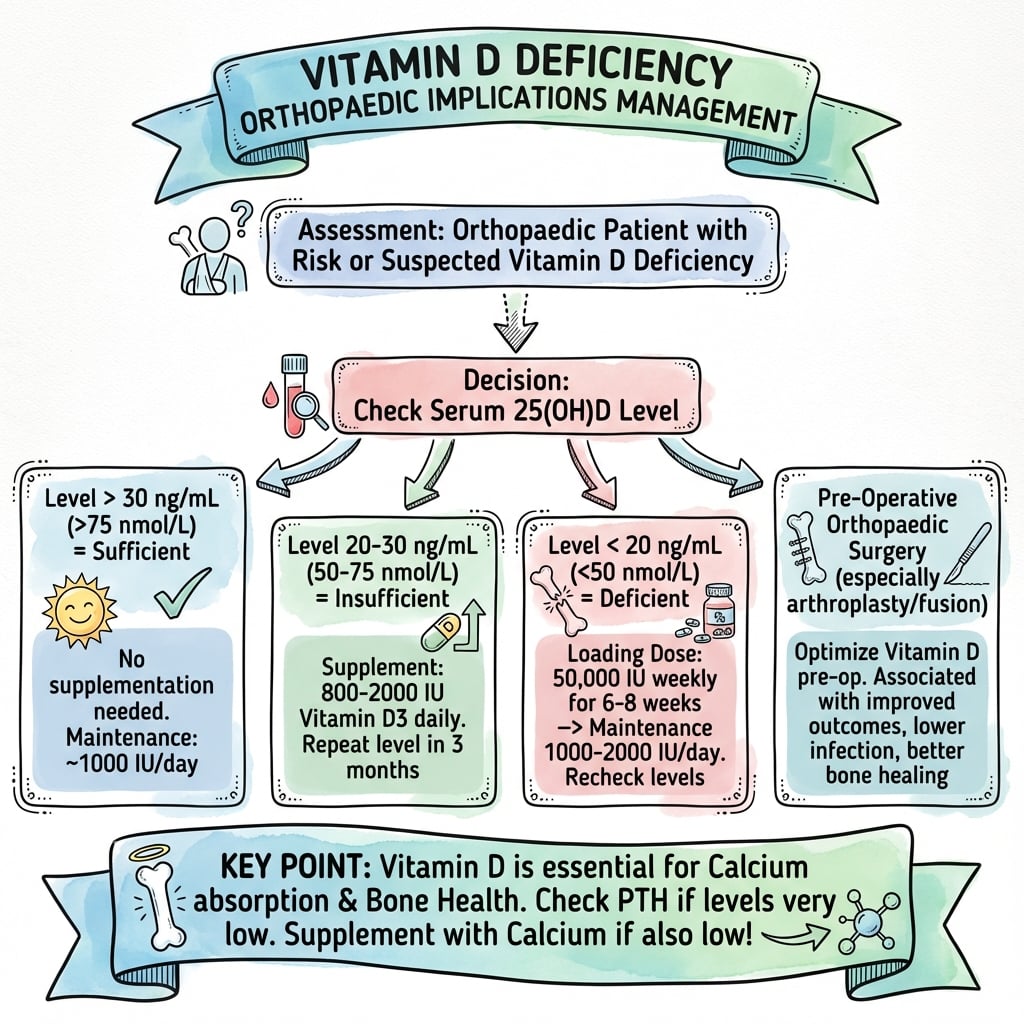
- 25-OH vitamin D less than 25 nmol/L = severe deficiency requiring urgent replacement
- Proximal myopathy (waddling gait, difficulty rising) is a key clinical feature
- Replacement protocol: 50,000 IU weekly for 6-8 weeks, then 800-2000 IU daily maintenance
- Orthopaedic implications: delayed fracture healing, aseptic loosening, periprosthetic fracture risk
- “Vitamin D deficiency is a PUBLIC HEALTH PROBLEM - screen high-risk populations preoperatively
- “Target 25-OH vitamin D greater than 75 nmol/L before elective arthroplasty
- “Vitamin D receptors in muscle - deficiency causes proximal muscle weakness independent of bone disease
- “Secondary hyperparathyroidism develops as compensatory response to hypocalcemia
Clinical Imaging
Imaging Atlas




Same disease, different age. Rickets occurs in children (open growth plates) with bowing deformities, widened epiphyses, and growth retardation. Osteomalacia occurs in adults (closed growth plates) with bone pain, proximal myopathy, and Looser zones. Both caused by vitamin D deficiency.
Severe deficiency: less than 25 nmol/L (less than 10 ng/mL). Deficiency: 25-50 nmol/L. Insufficiency: 50-75 nmol/L. Optimal: 75-125 nmol/L. Treatment intensity escalates with severity. Most osteomalacia occurs with levels less than 25 nmol/L.
Vitamin D receptors in skeletal muscle regulate calcium-dependent muscle contraction. Deficiency impairs muscle function causing proximal weakness (hip flexors, shoulder abductors), waddling gait, and difficulty rising from chair. Resolves with replacement.
Roughly one-third of arthroplasty patients are vitamin D deficient preoperatively, and deficiency is markedly more frequent in periprosthetic joint infection. Many units screen and optimize to greater than 50-75 nmol/L before elective surgery, although high-quality outcome trials are still lacking.
At a Glance
Vitamin D deficiency causes rickets in children (growth plate abnormalities, bowing, widened epiphyses) and osteomalacia in adults (defective mineralization, Looser zones, bone pain). Severe deficiency is defined as 25-OH vitamin D under 25 nmol/L (under 10 ng/mL); target for bone health is over 50 nmol/L, with over 75 nmol/L optimal before elective arthroplasty. A key clinical feature is proximal myopathy (waddling gait, difficulty rising from chair) due to vitamin D receptors in muscle affecting calcium-dependent contraction. Causes include inadequate sunlight, malabsorption (celiac, bariatric surgery), and CKD (impaired 1-alpha hydroxylation). Treatment: 50,000 IU weekly for 6-8 weeks loading, then 800-2000 IU daily maintenance. 30% of arthroplasty patients are deficient preoperatively, increasing infection risk (OR 2.4) and delayed healing.
SUNLIGHTCauses of Vitamin D Deficiency
Hook:Without SUNLIGHT, you can't make vitamin D!
RICKETSClinical Features of Vitamin D Deficiency
Hook:Remember RICKETS for the classic childhood presentation!
LOADINGVitamin D Replacement Protocol
Hook:LOADING dose first, then maintenance - just like LOADING a gun!
Overview and Epidemiology
Definition
Vitamin D deficiency is defined by inadequate serum 25-hydroxyvitamin D (25-OH vitamin D), the major circulating form and best marker of vitamin D status. Deficiency leads to impaired intestinal calcium absorption, compensatory secondary hyperparathyroidism, and ultimately skeletal disease: rickets in children (affecting growth plates) and osteomalacia in adults (defective bone mineralization).
Epidemiology
Global burden:
- 1 billion people worldwide have vitamin D deficiency or insufficiency
- 30-50% of community-dwelling elderly have levels less than 50 nmol/L
- 50-70% of hip fracture patients are vitamin D deficient
- Dark-skinned populations in high latitudes have 5-10 times higher risk
Global practice variation:
- Prevalence rises with latitude - populations above 35 degrees North/South have winter UVB too weak for cutaneous synthesis
- Institutionalized elderly - 40-60% deficient across high-income countries
- Post-bariatric surgery - 25-40% develop deficiency without supplementation
- South Asian, Middle Eastern and East African migrants to high-latitude countries are a recognized high-risk group (skin pigmentation plus concealing dress)
Risk factors:
- Age - elderly have reduced skin synthesis capacity
- Dark skin - melanin blocks UVB absorption (requires 3-5 times longer sun exposure)
- Institutionalized or homebound - inadequate sunlight exposure
- Malabsorption syndromes - celiac disease, Crohn's disease, post-bariatric surgery
- Chronic kidney disease - impaired activation of vitamin D
- Medications - anticonvulsants (phenytoin, phenobarbital), rifampicin
Vitamin D Metabolism and Physiology
Synthesis and Activation
UVB radiation (290-315 nm) converts 7-dehydrocholesterol in skin to pre-vitamin D3, which isomerizes to vitamin D3 (cholecalciferol). Requires adequate sun exposure - 10-15 minutes midday sun on arms and legs, 2-3 times weekly. Dark skin requires 3-5 times longer exposure.
Natural sources: Fatty fish (salmon, mackerel), fish liver oils, egg yolks. Fortified foods: Milk, cereals, orange juice. Dietary contribution typically provides 200-400 IU daily - insufficient without supplementation in high-risk groups.
Activation pathway:
- Liver (25-hydroxylation): Vitamin D3 converted to 25-OH vitamin D by 25-hydroxylase (primary storage form, half-life 2-3 weeks)
- Kidney (1-alpha hydroxylation): 25-OH vitamin D converted to 1,25-dihydroxy vitamin D (calcitriol) by 1-alpha hydroxylase (active hormone, tightly regulated by PTH, calcium, phosphate)
Physiological Actions
Primary role - calcium homeostasis:
- Intestinal calcium absorption - upregulates calcium-binding proteins in small intestine
- Bone mineralization - provides adequate calcium and phosphate for hydroxyapatite formation
- Renal calcium reabsorption - enhances distal tubular calcium reabsorption
- PTH regulation - suppresses PTH secretion when calcium adequate
Extra-skeletal effects:
- Muscle function - vitamin D receptors in skeletal muscle regulate calcium-dependent contraction
- Immune function - modulates innate and adaptive immunity (deficiency increases infection risk)
- Cell proliferation - anti-proliferative effects in many tissues
Q: Why is 25-OH vitamin D the best marker of vitamin D status?
A: 25-OH vitamin D has a long half-life (2-3 weeks) and reflects total body vitamin D stores from both cutaneous synthesis and dietary intake. 1,25-dihydroxy vitamin D (active form) has a short half-life (4-6 hours) and is tightly regulated by PTH, calcium, and phosphate - it can be normal or even elevated in vitamin D deficiency due to compensatory secondary hyperparathyroidism stimulating 1-alpha hydroxylase. Therefore, 25-OH vitamin D is the appropriate screening and monitoring test.
Pathophysiology of Deficiency
Cascade of Metabolic Derangements
Progressive pathophysiology:
- Vitamin D deficiency (25-OH vitamin D less than 50 nmol/L)
- Reduced intestinal calcium absorption (efficiency drops from 30-40% to 10-15%)
- Mild hypocalcemia triggers parathyroid glands
- Secondary hyperparathyroidism (compensatory PTH elevation to maintain calcium)
- PTH-mediated bone resorption releases calcium from skeleton
- Renal phosphate wasting (PTH inhibits proximal tubular phosphate reabsorption)
- Hypophosphatemia impairs mineralization
- Defective bone mineralization - osteoid accumulates but cannot mineralize (osteomalacia)
- Skeletal deformities and fractures in severe, prolonged deficiency
The PTH elevation in vitamin D deficiency is an appropriate physiological response to maintain serum calcium in the normal range. It is NOT primary hyperparathyroidism (autonomous PTH secretion). Once vitamin D is repleted, PTH normalizes. Do not treat PTH elevation - treat the underlying vitamin D deficiency.
Skeletal Manifestations
| Feature | Rickets (Children) | Osteomalacia (Adults) |
|---|---|---|
| Growth plate status | Open (actively growing) | Closed (growth complete) |
| Primary pathology | Defective growth plate mineralization | Defective osteoid mineralization |
| Skeletal deformities | Bowing (genu varum or valgum), frontal bossing, rachitic rosary | Looser zones, vertebral compression, kyphosis |
| Growth | Stunted growth, delayed milestones | Normal (growth complete) |
| Clinical presentation | Bowing, wrist/ankle widening, delayed walking | Bone pain, proximal myopathy, fractures |
| Radiographic findings | Widened metaphyses, cupping, fraying, coarse trabeculae | Looser zones, osteopenia, pathological fractures |
Neuromuscular Effects
Proximal myopathy mechanism:
- Vitamin D receptors (VDR) in skeletal muscle regulate calcium homeostasis within myocytes
- Deficiency impairs calcium-dependent muscle contraction
- Results in proximal muscle weakness (hip flexors, shoulder abductors greater than distal muscles)
- Type II muscle fiber atrophy on biopsy (fast-twitch fibers)
Clinical manifestations:
- Waddling gait (Trendelenburg due to hip abductor weakness)
- Difficulty rising from chair (hip flexor and knee extensor weakness)
- Difficulty climbing stairs (quadriceps weakness)
- Difficulty reaching overhead (shoulder abductor weakness)
Muscle weakness is independent of bone disease and can occur without osteomalacia.
Classification
Vitamin D Status Classification
Based on 25-OH Vitamin D Levels:
| Category | nmol/L | ng/mL | Clinical Action |
|---|---|---|---|
| Severe deficiency | Less than 25 | Less than 10 | Urgent replacement, osteomalacia risk |
| Deficiency | 25-50 | 10-20 | Replacement therapy required |
| Insufficiency | 50-75 | 20-30 | Supplementation recommended |
| Optimal | 75-125 | 30-50 | Target for bone health |
| Excess | Greater than 250 | Greater than 100 | Toxicity risk |
Clinical Presentation
Symptoms
Skeletal symptoms:
- Diffuse bone pain - worse with weight-bearing, pressure on sternum, ribs, pelvis
- Bone tenderness - palpation of sternum, ribs, tibia, pelvis elicits pain
- Pathological fractures - minimal trauma, often at sites of Looser zones
- Skeletal deformities - kyphosis, leg bowing (in severe, prolonged deficiency)
Neuromuscular symptoms:
- Proximal muscle weakness - difficulty rising from chair, climbing stairs
- Myalgias - diffuse muscle pain and cramping
- Fatigue - pervasive tiredness and reduced exercise tolerance
- Waddling gait - Trendelenburg gait from hip abductor weakness
Hypocalcemia symptoms (if severe):
- Paresthesias - perioral, fingers, toes
- Muscle cramps and spasms
- Tetany - carpopedal spasm, laryngospasm (rare, severe deficiency)
Many patients are asymptomatic until pathological fracture or incidental biochemical detection.
Examination Findings
Musculoskeletal:
- Antalgic or waddling gait - pain avoidance or Trendelenburg
- Bone tenderness - sternal pressure, rib compression, pelvic compression painful
- Skeletal deformities - leg bowing, kyphosis (chronic cases)
- Reduced muscle power - hip flexion (iliopsoas) and knee extension (quadriceps) grade 3-4 out of 5
Neurological:
- Proximal muscle weakness - cannot rise from squat without using hands
- Hyporeflexia - reduced deep tendon reflexes
- Tetany signs (if severe hypocalcemia):
- Chvostek's sign - facial twitch with tapping facial nerve
- Trousseau's sign - carpopedal spasm with blood pressure cuff inflation
General:
- Pallor (anemia of chronic disease in severe deficiency)
- Poor dentition (delayed eruption, enamel defects in rickets)
Investigations
Laboratory Investigations
Primary screening test:
- 25-hydroxyvitamin D (25-OH vitamin D) - best marker of vitamin D status
- Reflects total body vitamin D stores (cutaneous synthesis plus dietary intake)
- Long half-life (2-3 weeks) - stable marker
- Measure in all patients with suspected deficiency, bone disease, or preoperatively before arthroplasty
Supportive biochemistry:
- Serum calcium - may be low-normal or low (secondary hyperparathyroidism compensates initially)
- Serum phosphate - typically low (PTH-mediated renal phosphate wasting)
- Parathyroid hormone (PTH) - elevated (secondary hyperparathyroidism)
- Alkaline phosphatase (ALP) - elevated (osteoblast activity in osteomalacia)
- 1,25-dihydroxy vitamin D - NOT useful for screening (normal or elevated due to PTH stimulation)
Urine studies:
- 24-hour urine calcium - low (less than 2.5 mmol per 24 hours)
- Calcium-creatinine clearance ratio - helps exclude familial hypocalciuric hypercalcemia
Additional investigations if indicated:
- Creatinine and eGFR - assess for chronic kidney disease
- Liver function tests - screen for cholestatic disease (impairs 25-hydroxylation)
- Celiac serology (anti-TTG, anti-endomysial antibodies) - if malabsorption suspected
- Inflammatory markers - if inflammatory bowel disease suspected
Imaging Studies
Classic findings:
- Looser zones (pseudofractures) - pathognomonic
- Radiolucent bands perpendicular to cortex
- Bilateral, symmetric
- No periosteal reaction
- Common sites: femoral neck, pubic rami, ribs, scapula, proximal ulna
- Generalized osteopenia
- Cortical thinning
- Coarsened trabecular pattern
- Pathological fractures at sites of Looser zones
Advanced imaging if needed:
- Bone scan (nuclear medicine) - multiple symmetric hot spots at Looser zones
- MRI - bone marrow edema at pseudofracture sites
- CT - assess fracture risk, surgical planning
Looser zones at the medial femoral neck, pubic rami and lateral scapular border are the most exam-relevant sites; they are characteristically bilateral and symmetric, which distinguishes them from stress fractures.
DEXA scan (bone densitometry):
- Low bone mineral density (T-score less than -2.5 at spine or hip)
- Cannot distinguish osteomalacia from osteoporosis on DEXA alone
- Biochemistry essential for diagnosis
Bone Biopsy (Gold Standard)
Indications:
- Diagnostic uncertainty after clinical, biochemical, radiographic evaluation
- Suspected hypophosphatasia or rare mineralization disorder
- Exclude other bone diseases (renal osteodystrophy, osteopetrosis)
Technique:
- Iliac crest biopsy with tetracycline double-labeling
- Undecalcified sections for histomorphometry
Findings in vitamin D deficiency osteomalacia:
- Increased osteoid volume (greater than 15% vs normal less than 5%)
- Widened osteoid seams (greater than 12 micrometers thick)
- Prolonged mineralization lag time (greater than 100 days vs normal less than 25 days)
- Reduced mineralization surface
- Tetracycline double-labeling shows delayed mineralization front
Bone biopsy is rarely needed in practice - diagnosis typically made on clinical, biochemical, and radiographic grounds.
Diagnosis and Differential
The Diagnostic Biochemical Pattern
Diagnosis rests on a low 25-OH vitamin D plus the classic supporting pattern (see the Investigations and Classification sections for full thresholds and biochemistry): low-normal calcium, low phosphate, high PTH and high ALP, with normal or elevated 1,25-dihydroxy vitamin D. Looser zones on radiographs confirm osteomalacia, but DEXA cannot distinguish osteomalacia from osteoporosis - biochemistry is essential.
Q: Why is alkaline phosphatase elevated in vitamin D deficiency osteomalacia?
A: Osteoblast hyperactivity. In osteomalacia, osteoblasts continue to produce osteoid (unmineralized bone matrix) but cannot mineralize it due to lack of calcium and phosphate. This results in accumulation of large amounts of osteoid and elevated osteoblast activity. Alkaline phosphatase is an osteoblast enzyme, so levels rise markedly. In contrast, osteoporosis has normal ALP because there is simply reduced bone formation, not excess osteoid production.
Differential Diagnosis
Several conditions mimic vitamin D deficiency osteomalacia, especially when biochemistry is only partly typical. The pattern of calcium, phosphate, ALP, PTH and 25-OH vitamin D usually separates them.
| Condition | Calcium | Phosphate | ALP / PTH | Discriminating feature |
|---|---|---|---|---|
| Vitamin D deficiency osteomalacia | Low-normal or low | Low | ALP high, PTH high | Low 25-OH vitamin D, Looser zones, responds to D |
| Osteoporosis | Normal | Normal | ALP normal, PTH normal | Normal biochemistry; fragility fractures, low BMD |
| Primary hyperparathyroidism | High | Low | ALP high, PTH high | Hypercalcaemia with non-suppressed PTH |
| Renal osteodystrophy (CKD-MBD) | Low or high | High | ALP high, PTH very high | Reduced eGFR, high phosphate, low calcitriol |
| X-linked / tumour-induced hypophosphataemia | Normal | Low | ALP high, PTH normal | Normal 25-OH vitamin D, high renal phosphate wasting (FGF23) |
| Hypophosphatasia | Normal or high | Normal or high | ALP LOW, PTH normal | Low ALP (the key clue), elevated pyridoxal-5-phosphate |
| Paget disease | Normal | Normal | ALP very high, PTH normal | Focal disease, normal calcium/phosphate, classic radiology |
Hypophosphatasia is the trap when ALP is low rather than high - never give bisphosphonates. Hypophosphataemic rickets/osteomalacia (XLH, tumour-induced) has a normal 25-OH vitamin D with isolated renal phosphate wasting and will NOT respond to standard cholecalciferol; it needs phosphate plus active vitamin D (or burosumab for FGF23-driven disease).
Management
Treatment Protocol
Vitamin D Replacement Phases
For 25-OH vitamin D less than 25 nmol/L:
- Cholecalciferol (vitamin D3) 50,000 IU weekly for 6-8 weeks
- Oral calcium 1000-1500 mg daily (divided doses with meals)
Alternative daily dosing:
- Cholecalciferol 4000-6000 IU daily for 8-12 weeks
For moderate deficiency (25-50 nmol/L):
- Cholecalciferol 3000-5000 IU daily for 8-12 weeks
- Or 20,000 IU weekly for 8-12 weeks
- Cholecalciferol 800-2000 IU daily (lifelong if risk persists)
- Calcium 1000-1200 mg daily (dietary plus supplements if needed)
- Recheck 25-OH vitamin D at 3 months - target greater than 75 nmol/L
- Annual monitoring once stable
- Calcium and phosphate at 1, 3, 6 months then annually
- PTH and alkaline phosphatase - should normalize by 6 months
- Annual 25-OH vitamin D to ensure maintenance
- Bone density (DEXA) at 2 years to assess response
In severe, prolonged vitamin D deficiency with marked secondary hyperparathyroidism, rapid vitamin D and calcium replacement can cause hungry bone syndrome - profound hypocalcemia and hypophosphatemia as the demineralized skeleton avidly takes up minerals. Risk factors: PTH greater than 150 pg/mL, very low vitamin D (less than 12.5 nmol/L), prolonged deficiency. Monitor calcium closely in first 2 weeks. May require IV calcium gluconate if symptomatic tetany develops.
Special Populations
Malabsorption (celiac, Crohn's, post-bariatric):
- Higher doses required: 50,000 IU weekly long-term, or 3000-6000 IU daily
- Monitor absorption: Check 25-OH vitamin D at 3 months to ensure adequate rise
- Consider IM or IV if severe malabsorption (rare)
Chronic kidney disease:
- Activated vitamin D (calcitriol) required if eGFR less than 30 mL/min
- Standard cholecalciferol ineffective (impaired 1-alpha hydroxylation)
- Dose: Calcitriol 0.25-1 microgram daily, titrated to PTH and calcium
- Monitor for hypercalcemia and hyperphosphatemia
Elderly institutionalized:
- Universal supplementation recommended: 800-1000 IU daily
- Calcium 1200 mg daily
- Reduces fracture risk in institutionalized elderly when combined with calcium
Orthopaedic Implications
Fracture Healing
Vitamin D deficiency impairs fracture healing:
- Delayed union or nonunion - inadequate mineralization of callus
- Reduced mechanical strength of healing bone
- Prolonged time to union (50-100% longer than vitamin D-replete patients)
Mechanism:
- Insufficient calcium and phosphate for mineralization
- Impaired osteoblast function and differentiation
- Reduced angiogenesis (vitamin D regulates VEGF)
Management:
- Optimize vitamin D preoperatively for elective fracture fixation
- Aggressive replacement in acute fractures (50,000 IU weekly)
- Monitor union - may require longer protected weight-bearing
- Consider bone stimulation if delayed union persists
Arthroplasty Considerations
Preoperative screening:
- Consider 25-OH vitamin D measurement before elective arthroplasty, especially in high-risk patients
- Optimize to greater than 50-75 nmol/L before surgery where deficiency is found
- Delay elective surgery if severe deficiency (less than 25 nmol/L) until repleted
Intraoperative considerations:
- Poor bone quality - soft bone, reduced screw purchase
- Risk of periprosthetic fracture during insertion (especially press-fit stems)
- Consider cemented fixation if bone very osteopenic
Postoperative complications:
- Increased infection risk (OR 2.4) - vitamin D modulates immune function
- Delayed mobilization - proximal myopathy impairs rehabilitation
- Prolonged hospital stay
- Aseptic loosening risk - impaired osseointegration of uncemented implants
- Periprosthetic fracture with minimal trauma
Management:
- Continue vitamin D and calcium indefinitely
- Aggressive physiotherapy to overcome muscle weakness
- Thromboprophylaxis (prolonged immobilization risk)
Pathological Fractures
High-risk sites in osteomalacia:
- Femoral neck - often bilateral, at sites of Looser zones
- Proximal femur - subtrochanteric, intertrochanteric
- Pelvis - pubic rami, sacrum
- Ribs - multiple, painful
- Vertebrae - compression fractures
Management principles:
- Optimize medical management FIRST - vitamin D and calcium replacement
- Prophylactic fixation for impending fractures (Looser zones greater than 50% cortical width, symptomatic)
- Fracture fixation with caution - bone is soft, screw purchase poor
- Longer plates with more screws for load distribution
- Locking plates to minimize screw toggle
- Cement augmentation in proximal femur fractures
- Protected weight-bearing for 3-6 months (delayed healing)
- Aggressive vitamin D replacement perioperatively to accelerate healing
Surgical Considerations
Intraoperative Considerations
Bone Quality:
- Osteomalacic bone is soft and poorly mineralized
- Reduced screw purchase and holding power
- Higher risk of intraoperative fracture
Fixation Strategies:
- Use cemented implants in arthroplasty
- Longer plates with more screws
- Locking plate constructs preferred
- Cement augmentation for screw purchase
| Issue | Standard Bone | Osteomalacic Bone |
|---|---|---|
| Screw purchase | Good | Poor - use locking screws |
| Plate length | Standard | Extended with more screws |
| THA fixation | Uncemented | Cemented preferred |
| Protected WB | 6-8 weeks | 12+ weeks |
Complications
Complications of Deficiency
Skeletal:
- Pathological fractures (Looser zones)
- Delayed/non-union of fractures
- Progressive skeletal deformity (bowing)
- Accelerated osteoporosis
Surgical Complications:
- Implant loosening (poor bone integration)
- Periprosthetic fracture
- Surgical site infection (OR 2.4)
- Delayed mobilization
| Complication | Mechanism | Prevention |
|---|---|---|
| Delayed union | Poor mineralization | Optimize vitamin D |
| Infection | Immune dysfunction | Level greater than 75 nmol/L |
| Loosening | Poor osseointegration | Cemented implants |
Postoperative Care
Postoperative Protocol
Immediate:
- Continue vitamin D replacement (50,000 IU weekly)
- Calcium supplementation (1200 mg daily)
- Protected weight-bearing (extended in osteomalacia)
Monitoring:
- Check calcium at 1 week, 1 month
- Vitamin D at 3 months post-op
- PTH and ALP should normalize
| Phase | Normal Bone | Osteomalacic Bone |
|---|---|---|
| Protected WB | 6 weeks | 12+ weeks |
| Union expected | 8-12 weeks | 16-24 weeks |
| Full activity | 3 months | 6+ months |
Prognosis and Outcomes
Expected Response to Treatment
Biochemical:
- Calcium and phosphate normalize by 4-12 weeks
- PTH decreases by 3-6 months (may take longer if severe secondary hyperparathyroidism)
- Alkaline phosphatase declines by 6-12 months (may initially rise as bone heals)
- 25-OH vitamin D rises by 3 months to target (greater than 75 nmol/L)
Clinical:
- Bone pain improves by 6-12 weeks
- Muscle weakness reverses by 3-6 months (proximal myopathy resolves)
- Looser zones heal by 6-12 months (radiographic evidence of mineralization)
- Fracture risk decreases once vitamin D greater than 50 nmol/L
Poor prognostic factors:
- Severe, prolonged deficiency - may have permanent skeletal deformities
- Uncontrolled underlying cause (malabsorption, chronic kidney disease)
- Non-compliance with supplementation
- Concurrent osteoporosis - may require additional antiresorptive therapy
Evidence Base and Key Studies
Vitamin D and Fracture Prevention
- Meta-analysis of double-blind RCTs in adults aged 60 and over (5 RCTs for hip fracture, n=9294; 7 RCTs for nonvertebral fracture, n=9820)
- Cholecalciferol 700-800 IU daily reduced hip fracture by 26% (pooled RR 0.74) and any nonvertebral fracture by 23% (pooled RR 0.77) vs calcium or placebo
- Low-dose 400 IU daily showed no significant fracture benefit (hip RR 1.15)
- All included trials used cholecalciferol; benefit seen in both ambulatory and institutionalized elderly
Vitamin D Deficiency and Periprosthetic Joint Infection
- Single-centre study measuring serum 25-OH vitamin D across primary arthroplasty (n=109), aseptic loosening (n=31) and periprosthetic joint infection (n=50)
- Low vitamin D levels were common in all subgroups, reflecting high baseline prevalence in arthroplasty patients
- 25-OH vitamin D was significantly lower in periprosthetic joint infection than in primary arthroplasty or aseptic loosening (p less than 0.001)
- Vitamin D was framed as a modifiable immune mediator potentially relevant to infection risk
Metabolic and Endocrine Abnormalities in Nonunions
- Case series: 37 nonunion patients meeting screening criteria (unexplained nonunion, multiple low-energy fractures, or non-displaced pubic rami/sacral nonunion) referred to endocrinology
- 31 of 37 (84%) had at least one new metabolic or endocrine diagnosis
- Vitamin D deficiency was the most common new finding (25 of 37 patients, 68%)
- 8 patients achieved union with medical treatment alone (no further surgery), at a mean of 7.6 months
Low Vitamin D, High PTH and Sarcopenia
- Prospective population study (Longitudinal Aging Study Amsterdam), adults aged 65 and over, 3-year follow-up (grip strength n=1008; muscle mass n=331)
- Baseline 25-OH vitamin D under 25 nmol/L conferred a 2.57-fold higher risk of sarcopenia by grip strength vs levels over 50 nmol/L
- High PTH (4.0 pmol/L or more) was independently associated with sarcopenia (OR ~1.7-2.4)
- Associations persisted after adjustment for activity, season, chronic disease, smoking and BMI
Endocrine Society Guideline: Diagnosis and Treatment
- Recommends serum 25-OH vitamin D by a reliable assay as the initial test in patients at risk of deficiency
- Defines deficiency as under 50 nmol/L (20 ng/mL) and insufficiency as 52-72 nmol/L (21-29 ng/mL)
- Either vitamin D2 or D3 is acceptable for treating deficiency
- Recommends against population-wide screening of low-risk individuals
Global Consensus on Nutritional Rickets
- International, GRADE-based consensus from 11 scientific organisations defining and managing nutritional rickets
- Rickets results from vitamin D and/or dietary calcium deficiency; diagnosis requires biochemical plus radiographic confirmation
- Recommends infant supplementation (400 IU daily) and population food fortification to prevent rickets
- Frames nutritional rickets and osteomalacia as preventable global public-health problems
VITAL: Supplemental Vitamin D and Incident Fractures
- Randomized, double-blind, placebo-controlled trial: 25,871 generally healthy US adults, vitamin D3 2000 IU daily vs placebo, median follow-up 5.3 years
- Participants were NOT selected for vitamin D deficiency, low bone mass or osteoporosis
- No reduction in total (HR 0.98), nonvertebral (HR 0.97) or hip fractures (HR 1.01)
- No benefit even in subgroups with lower baseline 25-OH vitamin D
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman is listed for total knee arthroplasty. Preoperative blood tests show 25-OH vitamin D 22 nmol/L, calcium 2.1 mmol/L, PTH 145 pg/mL, alkaline phosphatase 180 U/L. What is your assessment and management?”
“A 52-year-old man presents with tibial shaft fracture nonunion 9 months post-intramedullary nailing. Initial fracture was low-energy. He smokes 10 cigarettes daily. Blood tests show 25-OH vitamin D 28 nmol/L. How do you assess and manage this nonunion?”
“A 14-month-old child presents with delayed walking and bowing of the legs. X-rays show widened metaphyses with cupping and fraying at the distal femur and proximal tibia. Blood tests show 25-OH vitamin D 18 nmol/L, calcium 1.9 mmol/L, phosphate 0.8 mmol/L, PTH 220 pg/mL, alkaline phosphatase 650 U/L. How do you diagnose and manage this child?”
MCQ Practice Points
Q: What is the threshold for severe vitamin D deficiency?
A: 25-OH vitamin D less than 25 nmol/L (less than 10 ng/mL). This level is associated with high risk of osteomalacia, rickets, secondary hyperparathyroidism, and pathological fractures. Requires urgent replacement with high-dose cholecalciferol (50,000 IU weekly for 6-8 weeks).
Q: What is the appropriate vitamin D replacement regimen for severe deficiency (25-OH vitamin D less than 25 nmol/L)?
A: Cholecalciferol 50,000 IU weekly for 6-8 weeks, followed by maintenance 800-2000 IU daily. Alternative: 4000-6000 IU daily for 8-12 weeks. Always add calcium 1000-1500 mg daily. Recheck 25-OH vitamin D at 3 months - target greater than 75 nmol/L for optimal bone health.
Q: Why does vitamin D deficiency cause proximal muscle weakness?
A: Vitamin D receptors (VDR) in skeletal muscle regulate calcium-dependent muscle contraction. Deficiency impairs myocyte calcium homeostasis, causing Type II muscle fiber atrophy (fast-twitch fibers). Clinical manifestations: waddling gait, difficulty rising from chair, difficulty climbing stairs. Resolves with vitamin D replacement over 3-6 months.
Q: Why should you screen for vitamin D deficiency before elective arthroplasty?
A: Roughly one-third of arthroplasty patients are vitamin D deficient preoperatively, and 25-OH vitamin D is significantly lower in patients with periprosthetic joint infection. Deficiency is associated with delayed mobilization and is biologically linked to impaired osseointegration and immune function. Many units screen and optimize to over 50-75 nmol/L before surgery, though high-quality RCT evidence that correction improves implant outcomes is still lacking.
Q: What is hungry bone syndrome and when does it occur in vitamin D deficiency treatment?
A: Hungry bone syndrome occurs when rapid vitamin D and calcium replacement in severe, prolonged deficiency causes profound hypocalcemia and hypophosphatemia as the demineralized skeleton avidly takes up minerals. Risk factors: marked secondary hyperparathyroidism (PTH greater than 150 pg/mL), very low vitamin D (less than 12.5 nmol/L), prolonged disease. Monitor calcium closely in first 2 weeks of treatment. May require IV calcium gluconate if symptomatic tetany develops.
Controversies and Areas of Uncertainty
The exam-relevant debates in vitamin D centre on who to test, what level to aim for, and when supplementation actually helps.
Societies disagree. The US Institute of Medicine treats 50 nmol/L (20 ng/mL) as adequate for the population, whereas the Endocrine Society and many bone specialists favour over 75 nmol/L for at-risk patients. Higher targets risk over-treatment; lower targets risk under-treating true skeletal disease.
The VITAL trial (25,871 unselected US adults) found vitamin D 2000 IU daily did not reduce fractures, falls or cancer in people who were not deficient. The benefit seen in older meta-analyses is concentrated in deficient, institutionalized or co-supplemented (calcium) populations - argue against blanket supplementation.
Deficiency is common before arthroplasty and is associated with infection, but there is no high-quality RCT proving that correcting it improves implant outcomes. Practice ranges from routine screening to risk-based testing only.
Weekly loading (e.g. 50,000 IU weekly) is standard, but single very large annual boluses (e.g. 500,000 IU) have been associated with a paradoxical increase in falls and fractures and are now discouraged.
Guidelines, Registries & Global Practice
Global Epidemiology
- Vitamin D deficiency or insufficiency affects an estimated 1 billion people worldwide
- Highest burden at high latitudes in winter, in darker-skinned populations, and in concealed-dress and institutionalized groups
- Nutritional rickets remains common in parts of South Asia, the Middle East and sub-Saharan Africa, and persists in migrant communities at high latitude
Side-by-Side Guidance
| Body | Sufficiency target | Key position |
|---|---|---|
| Endocrine Society (2011) | Over 75 nmol/L (at-risk) | Risk-based testing; treat deficiency with D2 or D3; no universal screening |
| US Institute of Medicine / NAM | 50 nmol/L (population) | 50 nmol/L meets needs of 97.5% of population; cautions against higher targets |
| UK NOS / NICE & SACN | Over 50 nmol/L; 400 IU/day intake | Population intake advice; treat symptomatic deficiency |
| Global Consensus on Rickets (2016) | Infants 400 IU/day | Supplementation plus food fortification to eradicate nutritional rickets |
High- vs Limited-Resource Practice
- High-resource settings: ready 25-OH vitamin D assays, fortified foods, and cholecalciferol availability; debate is about screening intensity and targets.
- Limited-resource settings: assays may be unavailable and diagnosis is clinical plus radiographic; emphasis shifts to public-health prevention (food fortification, antenatal and infant supplementation) over individual testing.
- Calcium deficiency (low dietary intake) is a co-driver of rickets in some low-income regions, so calcium as well as vitamin D may be needed.
Be able to state the controversy: thresholds differ between the Endocrine Society (over 75 nmol/L) and the IOM (50 nmol/L), and large RCTs (VITAL) show no fracture benefit in replete adults - so target treatment to genuine deficiency, not the whole population.
Key Pathophysiology
- Vitamin D deficiency leads to reduced intestinal calcium absorption
- Compensatory secondary hyperparathyroidism (PTH elevates to maintain calcium)
- PTH causes bone resorption and renal phosphate wasting (hypophosphatemia)
- Inadequate calcium and phosphate impairs mineralization - osteomalacia (adults) or rickets (children)
Vitamin D Thresholds
- Severe deficiency: less than 25 nmol/L (less than 10 ng/mL)
- Deficiency: 25-50 nmol/L
- Insufficiency: 50-75 nmol/L
- Optimal for bone health: 75-125 nmol/L
- Target for arthroplasty: greater than 75 nmol/L
Clinical Features
- Adults: Bone pain, proximal myopathy (waddling gait, difficulty rising), fractures
- Children: Bowing deformities, rachitic rosary, delayed milestones, craniotabes
- Proximal muscle weakness: hip flexors, shoulder abductors (vitamin D receptors in muscle)
- Looser zones (pseudofractures): bilateral, symmetric, perpendicular to cortex
Replacement Protocol
- Severe deficiency (less than 25 nmol/L): Cholecalciferol 50,000 IU weekly for 6-8 weeks
- Maintenance: 800-2000 IU daily (lifelong if risk persists)
- Always add calcium 1000-1500 mg daily
- Recheck 25-OH vitamin D at 3 months - target greater than 75 nmol/L
- Special populations: malabsorption requires higher doses (3000-6000 IU daily), CKD requires calcitriol
Orthopaedic Implications
- Delayed fracture healing - prolonged by 50-100%, risk of nonunion
- Arthroplasty complications: increased infection (OR 2.4), delayed mobilization, aseptic loosening
- Screen preoperatively - optimize to greater than 75 nmol/L before elective surgery
- Pathological fractures: prophylactic fixation for Looser zones greater than 50% cortex
- Soft bone - poor screw purchase, consider cemented fixation, cement augmentation
Complications
- Hungry bone syndrome: rapid replacement causes profound hypocalcemia (demineralized skeleton avidly takes up minerals)
- Risk factors: PTH greater than 150, vitamin D less than 12.5 nmol/L, prolonged deficiency
- Monitor calcium closely first 2 weeks, may require IV calcium gluconate
- Secondary hyperparathyroidism: appropriate response to hypocalcemia (not primary HPT)