Total vs Four-Corner | SLAC/SNAC Staging | Radiolunate Critical | Position Matters
- Total fusion: Pan-carpal arthritis, SLAC/SNAC Stage IV, eliminates all wrist motion
- Four-corner fusion: SLAC/SNAC Stage II-III with INTACT radiolunate joint, preserves 50% motion
- Radiolunate joint assessment critical - any arthritis contraindicates four-corner
- Fusion position: Neutral to 15-20° extension for optimal function
- Complete cartilage removal to bleeding bone is most important technical factor
- “SLAC staging guides treatment: Stage II-III = four-corner or PRC, Stage IV = total fusion
- “Radiolunate joint must be intact for four-corner - assess on X-ray and CT
- “Scaphoidectomy and radial styloidectomy required for four-corner fusion
- “Nonunion most common complication - complete cartilage removal prevents it
Total fusion for pan-carpal arthritis or SLAC/SNAC Stage IV. Four-corner fusion for SLAC/SNAC Stage II-III with INTACT radiolunate joint. Radiolunate arthritis is absolute contraindication to four-corner - must do total fusion. Assess radiolunate joint on X-ray and CT before deciding.
Radiolunate joint must be intact for four-corner fusion. Any arthritis on imaging (X-ray, CT) contraindicates four-corner - patient needs total fusion. This is the most common error: performing four-corner when radiolunate is arthritic, leading to persistent pain and need for revision.
Complete cartilage removal to bleeding subchondral bone is the most important technical factor. Inadequate removal is the leading cause of nonunion. Use rongeur, curette, and burr systematically. Bleeding bone confirms adequate preparation.
Optimal position: Neutral to 15-20° extension, neutral radial/ulnar deviation. This functional position allows hand-to-mouth, perineal care, and writing. Excessive flexion or extension limits function. Position cannot be revised after fusion - get it right first time.
- SLAC Stage
- Stage II-III
- Treatment
- Four-corner fusion or PRC
- Key Consideration
- Preserves 50% motion at radiolunate joint
- SLAC Stage
- Stage IV
- Treatment
- Total wrist fusion
- Key Consideration
- All motion eliminated but reliable pain relief
- SLAC Stage
- Pan-carpal
- Treatment
- Total wrist fusion
- Key Consideration
- Gold standard for end-stage disease
- SLAC Stage
- Instability
- Treatment
- Total wrist fusion
- Key Consideration
- Provides stable pain-free platform
CLEARFour-Corner Fusion Requirements
Hook:CLEAR requirements for four-corner: Cartilage intact, Lunate preserved, Excise scaphoid, Assess preop, Radial styloidectomy.
NEUTRALFusion Position
Hook:NEUTRAL position: Neutral extension, test right first time, immobilize until fusion - position is permanent.
Overview and Epidemiology
Definition: Wrist arthrodesis is a salvage procedure that fuses wrist joints to eliminate motion and provide pain relief. Total wrist fusion eliminates all wrist motion, while four-corner (partial) fusion preserves radiolunate motion. The choice depends on disease extent and radiolunate joint status.
Wrist arthrodesis has evolved from simple pin fixation to modern dorsal plating systems with improved fusion rates. Recognition that radiolunate joint can be preserved in SLAC Stage II-III has made four-corner fusion a motion-preserving alternative to total fusion.
- Pan-carpal arthritis (post-traumatic, inflammatory, degenerative)
- SLAC/SNAC Stage IV (radiolunate arthritis)
- Severe instability (RA, post-traumatic)
- Failed prior salvage procedures
- Paralytic/spastic wrist requiring stable platform
- SLAC/SNAC Stage II-III with intact radiolunate joint
- Scaphoid non-union advanced collapse (SNAC)
- Preserves 50% wrist motion at radiolunate joint
- Frequency: Common in hand surgery (1-2 per month in hand centers)
- Age: Peak 40-60 years (post-traumatic), older for RA
- Gender: Equal distribution (trauma-related), female predominance in RA
- Trend: Four-corner fusion increasing for SLAC Stage II-III
Wrist arthrodesis provides reliable pain relief for end-stage wrist pathology when motion-preserving procedures are not possible or have failed. Total fusion eliminates all motion but provides pain-free stable platform. Four-corner fusion preserves radiolunate motion (~50%) but requires intact radiolunate joint - this is the critical decision point.
Pathophysiology and Mechanisms
- Radioscaphoid fossa: Articulates with scaphoid
- Radiolunate fossa: Articulates with lunate
- Sigmoid notch: Articulates with ulna (DRUJ)
- Scaphocapitate: Scaphoid-capitate articulation
- Capitolunate: Capitate-lunate articulation
- Triquetrohamate: Triquetrum-hamate articulation
- Proximal row: Scaphoid, lunate, triquetrum, pisiform
- Distal row: Trapezium, trapezoid, capitate, hamate
- Carpal height: Critical for four-corner fusion
- Radioscaphocapitate: Primary scaphoid stabilizer
- Radiolunate: Stabilizes lunate
- Dorsal radiocarpal: Dorsal stability
- Scapholunate: Critical for carpal stability
- Lunotriquetral: Ulnar carpal stability
- Branches cross dorsal radial wrist
- Injury causes numbness (10% incidence)
- Must protect during approach
- Ulnar side of incision
- Must protect
Biomechanics
- All wrist motion eliminated
- Compensatory motion at elbow, shoulder
- Grip strength improves (pain relief)
- Functional adaptation required
- 50% wrist motion preserved (radiolunate joint)
- Carpal height maintained
- Better function than total fusion
- Risk of radiolunate arthritis progression
Classification Systems
Scapholunate Advanced Collapse
- Arthritis between radial styloid and scaphoid
- Early disease
- Treatment: Radial styloidectomy, debridement
- Entire radioscaphoid joint involved
- Scaphoid fossa arthritis
- Treatment: Four-corner fusion or PRC (if radiolunate intact)
- Capitolunate arthritis
- Capitate migrates proximally
- Treatment: Four-corner fusion or PRC (if radiolunate intact)
- Radiolunate arthritis
- Pan-carpal involvement
- Treatment: Total wrist fusion (four-corner contraindicated)
SLAC staging guides surgical decision-making and predicts outcomes.
RSCLSLAC Wrist Staging
Hook:RSCL progression: Radial styloid → Scaphoid fossa → Capitolunate → Lunate fossa. Stage IV requires total fusion.
Clinical Assessment
- Pain location (dorsal, radial, ulnar)
- Instability symptoms (giving way, clunking)
- Previous trauma (fractures, ligament injuries)
- Functional limitations (grip, activities)
- Occupation and hand dominance
Physical Examination
- Swelling, deformity
- Carpal collapse (SLAC wrist)
- Muscle atrophy
- Joint line tenderness
- Scapholunate gap (Watson test)
- Instability (ballottement)
- Flexion-extension: Normal 70-80° each direction
- Radial-ulnar deviation: Normal 20-30° each direction
- Pronation-supination: Normal 80° each direction
- Watson test: Scapholunate instability
- Midcarpal shift: Midcarpal instability
- Grip strength: Compare with contralateral
- PA view: Carpal alignment, joint spaces, SLAC stage
- Lateral view: Carpal collapse, DISI/VISI deformity
- CT scan: Cartilage assessment, radiolunate joint evaluation
Investigations
- PA wrist: Carpal alignment, joint spaces, SLAC staging
- Lateral wrist: Carpal collapse, DISI/VISI deformity
- Oblique views: Better visualization of specific joints
- Stress views: Instability assessment
- 3D reconstruction: Essential for planning
- Cartilage assessment: Radiolunate joint evaluation (critical for four-corner)
- Bone stock: Quality for fixation
- Deformity quantification: Carpal collapse, alignment
- Cartilage evaluation: Early changes, radiolunate status
- Ligament integrity: Scapholunate, lunotriquetral
- Avascular necrosis: Scaphoid, lunate
- Diagnostic: Direct cartilage visualization
- Therapeutic: Debridement, limited procedures
- Distinguishing Features
- Scapholunate dissociation, radial-sided pain, positive Watson test
- Key Imaging
- SL gap, radioscaphoid then capitolunate arthritis, lunate dorsiflexed (DISI)
- Implication for Salvage
- Stage-based: PRC or four-corner (radiolunate sparing) vs total fusion
- Distinguishing Features
- Prior scaphoid waist nonunion, radial pain, humpback deformity
- Key Imaging
- Scaphoid nonunion with proximal radioscaphoid then capitolunate arthritis
- Implication for Salvage
- Same staged salvage; distal pole excision an option in early disease
- Distinguishing Features
- Central/dorsal pain, lunate tenderness, often heavy manual workers
- Key Imaging
- Lunate sclerosis, fragmentation and collapse on plain film/MRI
- Implication for Salvage
- Radiolunate often diseased - favours PRC or total fusion, not four-corner
- Distinguishing Features
- Bilateral, polyarticular, soft-tissue swelling, ulnar translocation
- Key Imaging
- Symmetric pan-carpal erosions, carpal collapse, caput ulnae
- Implication for Salvage
- Pan-carpal disease - total fusion or arthroplasty, not partial fusion
- Distinguishing Features
- Prior intra-articular distal radius fracture, focal radiocarpal pain
- Key Imaging
- Radiocarpal joint-space loss and incongruity
- Implication for Salvage
- Radiolunate involvement usually mandates total fusion
- Distinguishing Features
- Pain at base of thumb/distal scaphoid, distinct from radioscaphoid
- Key Imaging
- Isolated STT joint narrowing, radioscaphoid often spared
- Implication for Salvage
- Treated by limited STT fusion or trapeziectomy, not wrist arthrodesis
Management Algorithm

The key decision is total vs four-corner fusion. Total fusion for pan-carpal arthritis or Stage IV. Four-corner for Stage II-III with intact radiolunate. Radiolunate joint assessment is critical - any arthritis contraindicates four-corner.
Decision Tree
Step 1: Assess Disease Extent
- SLAC/SNAC staging (I-IV)
- Radiolunate joint status (critical)
- Pan-carpal vs localized
Step 2: Evaluate Radiolunate Joint
- X-ray: Joint space, alignment
- CT: Cartilage status, subchondral changes
- Any arthritis? → Total fusion
- Intact? → Consider four-corner
Step 3: Patient Factors
- Age, demand, occupation
- Hand dominance
- Functional requirements
Step 4: Surgical Decision
- Stage IV or radiolunate arthritis → Total fusion
- Stage II-III with intact radiolunate → Four-corner or PRC
- Stage I → Joint-sparing procedures
The goal is pain relief with optimal function preservation.
Surgical Technique
Pre-operative Planning Steps
- SLAC/SNAC staging
- Radiolunate joint evaluation (critical)
- Bone quality assessment
- Total vs four-corner fusion
- Radiolunate status determines choice
- Dorsal wrist fusion plate (total)
- Four-corner fusion plate (spider/circular)
- Bone graft (iliac crest or local)
- Fluoroscopy
- Smoking cessation mandatory
- Medical optimization
- Hand dominance consideration
Proper planning ensures correct procedure selection and optimal outcomes.
Construct Choice and Level of Distal Fixation (Total Fusion)
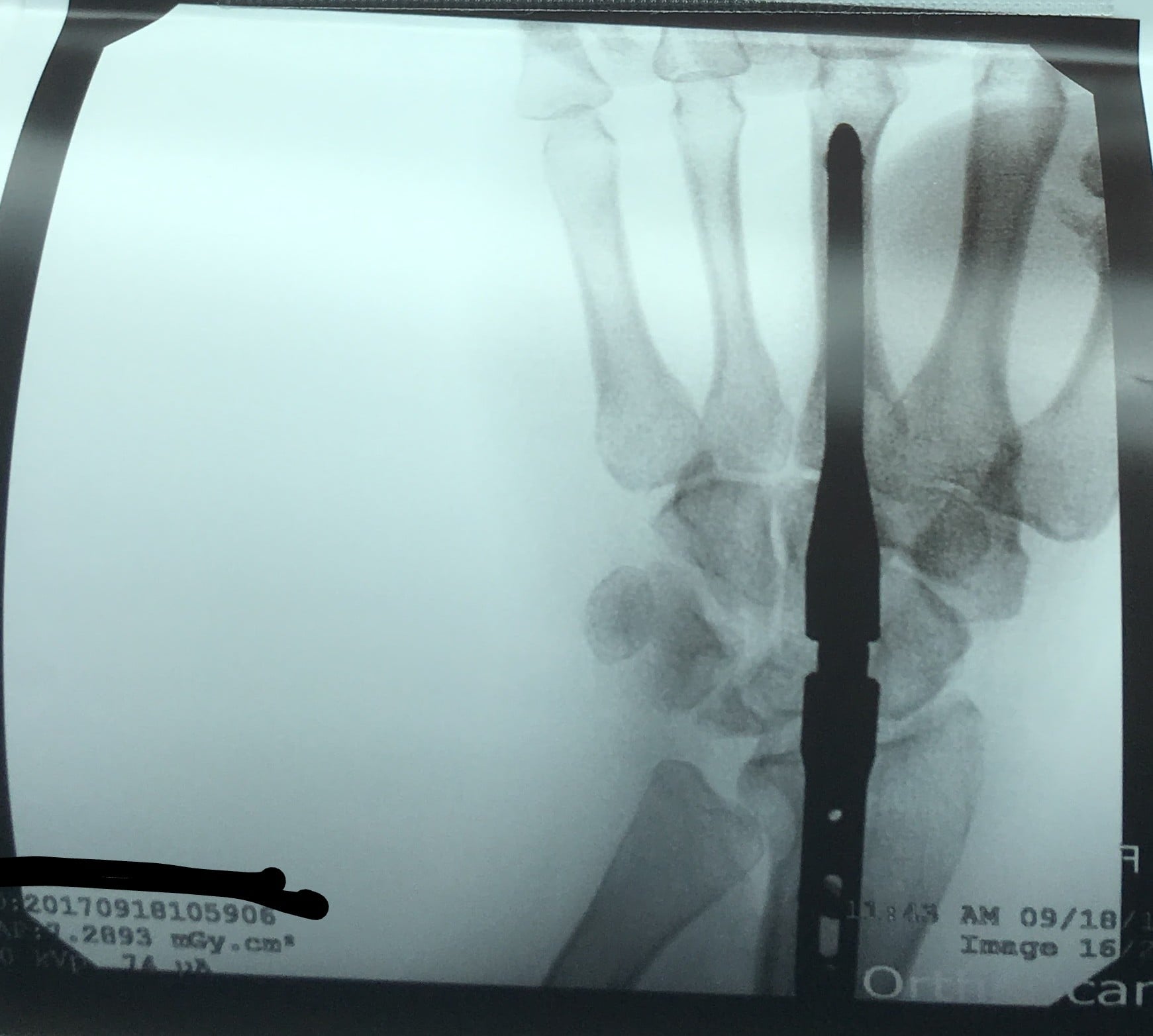
The surgical-technique tabs describe dorsal-plate and Steinmann-pin fixation, but the topic's own total-fusion radiograph shows a third option that is easy to miss - a central intramedullary rod running down the third metacarpal, through the carpus, and into the medullary canal of the distal radius. Understanding the three constructs and where they are anchored is a common viva probe.
- A precontoured, low-profile locking wrist-fusion plate is seated dorsally, usually along the third metacarpal, spanning the third carpometacarpal joint, the carpus and the distal radius.
- Some plate designs (and surgeon preference) seat the distal end on the second metacarpal instead; the second and third carpometacarpal joints are intrinsically near-rigid, so bridging them is well tolerated and they are routinely incorporated in the fusion mass.
- A gentle pre-set extension bend builds the functional position into the plate. Rigid, compressive fixation gives the highest union rates, which is why plating has largely superseded pins.
- A Rush pin or stout Steinmann/Mannerfelt rod is passed retrograde down the third-metacarpal canal into the radial canal, classically supplemented by a staple or additional K-wire to control rotation (an intramedullary rod alone does not resist rotation).
- It is lower-profile than a dorsal plate and needs less soft-tissue stripping, making it attractive where the skin is thin and bone stock is poor (for example the rheumatoid wrist) - the setting in which it was popularised.
- The trade-off is lower rotational and bending stiffness than a locking plate, so it depends on good bony apposition and adjunctive rotation control.
- Two or three retrograde pins are simpler and cheaper but the least stable and most prominent, and are now largely reserved for low-resource or damage-control settings.
Anchoring choice feeds directly into the hardware-prominence complication listed later: a dorsal plate lying over the thin skin of the dorsal wrist and third carpometacarpal region is the usual reason for elective implant removal once the wrist is solidly fused, whereas a buried intramedullary rod is far less often symptomatic.
If a total-wrist-fusion radiograph shows a single central rod spanning the third metacarpal to the radial canal rather than a dorsal plate with transverse screws, name it as an intramedullary (Mannerfelt-type) construct and add that it needs a staple or K-wire for rotational control. Dorsal plating to the second or third metacarpal is the modern default because rigid compression maximises union; the intramedullary rod remains a useful lower-profile alternative in the thin-skinned, poor-bone-stock (often rheumatoid) wrist.
Positioning the Bilateral Total Fusion
The NEUTRAL mnemonic and the position tab describe the ideal fusion angle for a single wrist - neutral to 15 to 20 degrees of extension with neutral deviation - but say nothing about the harder scenario the examiner may escalate to: both wrists requiring total fusion. Because a fused wrist is permanent, symmetric positioning of two stiff wrists can leave a patient unable to reach for perineal care and personal hygiene, a task that requires wrist flexion.
Principle of asymmetric positioning:
- Evidence here is expert opinion and low-level (there is no registry or trial to dictate a formula), so counselling and shared decision-making dominate.
- A widely taught compromise is to fuse the dominant wrist in slight extension (optimising power grip and hand-to-mouth activity) and the non-dominant wrist closer to neutral or in slight flexion, preserving the reach needed for toileting, perineal care and buttoning.
- Where possible, trial the intended positions preoperatively with removable splints so the patient can confirm that both hand-to-mouth feeding and perineal hygiene remain achievable before either wrist is committed.
- Staging the two fusions (rather than simultaneous bilateral surgery) also lets the second wrist's position be tuned to the functional result of the first.
For a unilateral fusion, position in neutral to slight extension. For bilateral fusion, do not simply mirror it: fixing both wrists in extension can make perineal hygiene impossible. Offer to fuse the dominant wrist in slight extension for power and the non-dominant wrist nearer neutral or slight flexion, and trial the positions with splints first - the choice is driven by that patient's priorities, not a fixed number.
Complications
- Incidence
- 5-10% total, 10-20% four-corner
- Risk Factors
- Inadequate cartilage removal, poor fixation, smoking, insufficient graft
- Management
- Revision with better preparation, rigid fixation, bone graft
- Incidence
- 10%
- Risk Factors
- Dorsal plate location, thin skin
- Management
- Removal once fused (18-24 months) if symptomatic
- Incidence
- 10-15%
- Risk Factors
- Nonunion, adjacent joint arthritis, hardware irritation
- Management
- Identify cause, treat accordingly
- Incidence
- 10-20% (four-corner)
- Risk Factors
- Progressive disease, altered biomechanics
- Management
- Conversion to total fusion if symptomatic
- Incidence
- 10% superficial radial
- Risk Factors
- Dorsal approach, nerve branches
- Management
- Observation, most recover
- Incidence
- 5-10% (four-corner)
- Risk Factors
- Inadequate fixation, bone loss
- Management
- Revision with better fixation
- Incidence
- 2-5%
- Risk Factors
- Hardware present, diabetes, smoking
- Management
- Debridement, antibiotics, may need hardware removal
Nonunion is the most common complication: 5-10% for total fusion with plate, 10-20% for four-corner fusion. Leading cause is inadequate cartilage removal. Prevention requires complete denudation to bleeding subchondral bone using rongeur, curette, and burr systematically. Treatment requires revision with better preparation, rigid fixation, and bone graft.
Postoperative Care and Rehabilitation
Total Wrist Fusion Rehabilitation
- Short arm cast or splint
- Immobilize 6-12 weeks until radiographic fusion
- X-rays at 6, 12 weeks assess fusion
- Bridging bone on 3+ cortices indicates fusion
- Remove cast/splint once fused
- Gentle finger ROM exercises
- Strengthening
- NO wrist motion (fused - this is expected)
- Compensatory motion at elbow and shoulder
- Occupational therapy for adaptive techniques
- Most patients adapt well
- Light activities: 3-4 months
- Full activities: 6 months
- Hardware removal: 18-24 months if symptomatic
Total fusion rehabilitation focuses on finger function and adaptation.
Outcomes and Prognosis
- Pain relief: 80-90% achieve good to excellent relief
- Motion: 0° wrist motion (expected and desired)
- Grip strength: 60-80% of opposite side
- Satisfaction: 80-85% satisfied despite motion loss
- Nonunion: 5-10% with plate fixation
- Pain relief: 70-80% achieve good relief
- Motion: ~50% preserved (average 30° arc)
- Grip strength: 75-80% of opposite side
- Satisfaction: 85-90% satisfied
- Nonunion: 10-20% (higher than total)
- Radiolunate arthritis: 10-20% develop over 5-10 years (four-corner)
- Hardware removal: 20-30% require removal for prominence
- Revision: 10-15% require revision (nonunion, complications)
- Adjacent joints: CMC, DRUJ may develop issues
Good outcomes are associated with: complete cartilage removal, rigid fixation (plates), adequate bone graft, proper alignment, smoking cessation, and dedicated therapy. Poor outcomes are associated with: inadequate cartilage removal, poor fixation, smoking, non-compliance, and complications.
Guidelines, Registries & Global Practice
Global Epidemiology:
- SLAC/SNAC is the most common pattern of degenerative wrist arthritis; the radioscaphoid (SLAC) pattern accounts for around 57% of degenerative wrists in the original radiographic series (Watson & Ballet, 1984).
- SNAC arises from untreated scaphoid waist nonunion - relevant worldwide given the high rate of missed scaphoid fractures, particularly in limited-resource settings without early CT/MRI.
- Total wrist arthrodesis is also a major reconstructive option for rheumatoid and post-traumatic pan-carpal disease and for the paralytic/spastic wrist; demand for inflammatory indications has fallen in high-income settings with modern disease-modifying therapy.
Side-by-Side Guidance (no single-country framing):
- Stance on Salvage Choice
- Stage II-III: PRC or four-corner fusion (motion-sparing); Stage IV / pan-carpal: total fusion
- Practical Emphasis
- Radiolunate (and capitolunate for PRC) integrity is the deciding factor
- Stance on Salvage Choice
- PRC and four-corner regarded as broadly equivalent for Stage II-III; total fusion for end-stage
- Practical Emphasis
- Locking-plate fixation preferred over pins for reliable union
- Stance on Salvage Choice
- Rigid internal fixation, complete joint surface preparation, autograft for fusion
- Practical Emphasis
- Compression and stable fixation to bleeding cancellous bone
- Stance on Salvage Choice
- Emphasis on patient-reported outcomes and shared decision-making over a single algorithm
- Practical Emphasis
- Counsel on equivalence of motion-sparing options and durability of total fusion
Registry & Implant Notes:
- There is no large national joint registry for partial carpal fusion or total wrist arthrodesis comparable to hip/knee registries; evidence is dominated by single-centre cohorts and the two PRC-vs-FCA meta-analyses cited above.
- Total wrist arthroplasty registry data (e.g. Norwegian and Australian datasets) show implant survival inferior to lower-limb arthroplasty, which keeps total fusion the more durable salvage in high-demand patients.
Routine preoperative CT for radiolunate cartilage assessment, precontoured locking plates for both total and four-corner fusion, hand-therapy-led rehabilitation, and total wrist arthroplasty offered to selected low-demand or bilateral patients.
Decision often made on plain radiographs alone; K-wire or Steinmann-pin fixation and bridge plating remain valid where dedicated implants are unavailable; total fusion favoured for its reliability and simpler aftercare when follow-up is limited.
Independent of health system, the following protect outcomes:
- Preoperative radiolunate joint assessment (radiograph, CT where available) before committing to four-corner fusion
- Counselling on permanent motion loss (total fusion) versus residual ~50% motion with higher nonunion risk (four-corner)
- Intraoperative confirmation of fusion position (neutral to 15-20° extension) on fluoroscopy - it cannot be revised
- Discussion of motion-sparing alternatives (PRC, four-corner) before total fusion when the disease stage permits
Controversies and Areas of Uncertainty
The longest-running debate. Two meta-analyses (Amer 2020, Ahmadi 2021) find no clinically meaningful difference in motion, grip or pain. PRC is simpler with no hardware-related complications; four-corner is preferred when the capitolunate (proximal capitate) cartilage is degenerate, since PRC depends on a healthy capitate head articulating with the lunate fossa.
Classic teaching cautioned against PRC in younger, high-demand patients (under ~35) due to feared progression of capitate-lunate-fossa arthritis. Longer-term series have challenged this, but the evidence remains low-level and the threshold is not firmly defined.
Dedicated circular/locking plates were introduced to ease fixation but early non-locking designs (e.g. Spider plate) caused dorsal impingement, loosening and reoperation (Reissner 2017). Whether modern locking plates truly outperform headless compression screws or K-wires for union remains debated, with no clear superiority on union rate alone.
Arthroplasty preserves motion but registry-level implant survival lags behind lower-limb arthroplasty, so total fusion remains the durable choice for high-demand or manual workers. Arthroplasty is reserved for low-demand, bilateral, or polyarticular (e.g. rheumatoid) patients who prioritise motion.
The motion-sparing decision (PRC vs four-corner) is genuinely controversial - both are acceptable and outcomes are equivalent in pooled data; articulate your selection criteria (capitate cartilage status, lesion location, hardware avoidance) rather than claiming one is definitively superior. The non-controversial points are: radiolunate arthritis mandates total fusion, complete surface preparation drives union, and fusion position is permanent.
MCQ Practice Points
Q: What is the primary indication for four-corner fusion? A: SLAC/SNAC Stage II-III with INTACT radiolunate joint. The radiolunate joint must have no arthritis on X-ray or CT - any arthritis contraindicates four-corner and requires total fusion.
Q: What is the most important technical factor for successful wrist fusion? A: Complete cartilage removal to bleeding subchondral bone. Inadequate removal is the leading cause of nonunion. Use rongeur, curette, and burr systematically to denude all fusion surfaces.
Q: What is the nonunion rate for four-corner fusion versus total wrist fusion? A: Four-corner fusion has higher nonunion rate (10-20%) compared to total fusion (5-10%). This is due to more fusion interfaces, smaller contact areas, and technically more difficult cartilage removal.
Q: What is the optimal fusion position for total wrist arthrodesis? A: Neutral to 15-20° extension, neutral radial/ulnar deviation. This functional position allows hand-to-mouth, perineal care, and writing. Position cannot be revised after fusion - must be correct initially.
Q: How does SLAC staging guide surgical treatment? A: Stage I: Radial styloidectomy. Stage II-III: Four-corner fusion or PRC (if radiolunate intact). Stage IV: Total wrist fusion (radiolunate arthritis requires total fusion).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old patient presents with SLAC wrist. X-rays show Stage III disease with capitolunate arthritis but radiolunate joint appears preserved. Walk me through your decision-making for total vs four-corner fusion, including how you assess the radiolunate joint and what factors influence your choice.”
“Walk me through the surgical technique for four-corner fusion, including approach, scaphoidectomy, cartilage removal, and fixation.”
“A patient presents 6 months after four-corner fusion with persistent pain. X-rays show no bridging bone and lucency at fusion interfaces. How do you manage this nonunion?”
Key Indications
- Total fusion: pan-carpal arthritis, SLAC/SNAC Stage IV, severe instability
- Four-corner: SLAC/SNAC Stage II-III with intact radiolunate joint
- Radiolunate assessment critical - any arthritis contraindicates four-corner
- Scaphoid non-union advanced collapse (SNAC) similar to SLAC
Surgical Technique
- Dorsal approach: protect superficial radial and dorsal ulnar nerves
- Scaphoidectomy: complete removal, radial styloidectomy 4-6mm
- Cartilage removal: complete to bleeding bone (most important factor)
- Fixation: dorsal plate (total) or four-corner plate (partial)
- Bone graft: iliac crest or local (scaphoid for four-corner)
Fusion Position
- Neutral to 15-20° extension: functional position
- Neutral radial/ulnar deviation
- Test position on fluoro before fixing
- Position cannot be revised after fusion
Complications
- Nonunion: 5-10% total, 10-20% four-corner (most common)
- Hardware prominence: 10% requiring removal
- Radiolunate arthritis: 10-20% over 5-10 years (four-corner)
- Nerve injury: 10% superficial radial (numbness)
Outcomes
- Total fusion: 0° motion, 80-90% pain relief, 60-80% grip
- Four-corner: 50% motion preserved, 70-80% pain relief, 75-80% grip
- Satisfaction: 80-85% total, 85-90% four-corner
- Hardware removal: 20-30% for prominence
Evidence Base and Key Trials
The SLAC Wrist - Original Classification
- Review of 4000 wrist radiographs; 210 cases of degenerative arthritis analysed
- Scaphoid-lunate-radius (SLAC) pattern most common at 57%; STT pattern 27%; combined 15%
- 20 operations in 19 patients: 18 of 19 had less pain, none required analgesia, with improved flexion-extension and deviation
Four-Corner Arthrodesis with Dorsal Locking Plate
- 50 patients (51 wrists), mean 6-year follow-up (range 4-9 years)
- Grip 80% of contralateral side; motion averaged 50° flexion-extension and 30° radioulnar deviation
- Seven nonunions (14%) required repeat arthrodesis; 3 wrists later converted to total fusion for persistent pain
Locking vs Non-Locking Plate for Four-Corner Fusion
- 39 patients with stage II-III SLAC/SNAC; 20 non-locking (Spider) vs 19 locking (Flower) plates, median 4.1-year follow-up
- Non-locking plates had more dorsal impingement and loosening; 5 non-locking patients needed further treatment
- Authors abandoned the non-locking implant and recommend locking-screw fixation
PRC vs Four-Corner Arthrodesis - Meta-analysis
- Systematic review and meta-analysis of 15 studies (incl. 2 randomized trials) comparing PRC and FCA for SLAC/SNAC
- No significant difference between PRC and FCA in motion, grip, pain, complications/reoperation or conversion to total fusion
- Authors favour PRC for its simplicity and absence of hardware-related complications; risk of bias high across studies
PRC vs Four-Corner Arthrodesis - Comparative Meta-analysis
- Meta-analysis of 8 studies, 311 patients comparing FCA and PRC for SLAC
- PRC showed statistically greater flexion-extension arc (by 6.2°), grip (by 1.52%) and slightly less pain
- Differences statistically significant but small and not clinically meaningful - treatments judged equivalent
Arthrodesis vs PRC vs Four-Corner for Advanced Carpal Collapse
- Cohort of 63 patients: 19 total arthrodesis, 26 PRC, 18 scaphoidectomy plus four-corner fusion
- PRC had the best DASH (16); total fusion (DASH 45) and four-corner (DASH 39) did not differ significantly
- PRC and four-corner preserved functional motion (44° and 52° flexion-extension arc); grip remained below the unoperated side in all groups