Article summary
A practical evidence-based guide to cervical disc replacement versus ACDF. Compare reoperation risk, adjacent segment concerns, patient selection, and the decision points that matter in real spine practice.
Educational content is reviewed for source visibility, editorial coherence, and correction readiness.
No individual clinician credential is claimed unless a named person is shown.
Verify before clinical use; this is not medical advice or a substitute for local guidance.
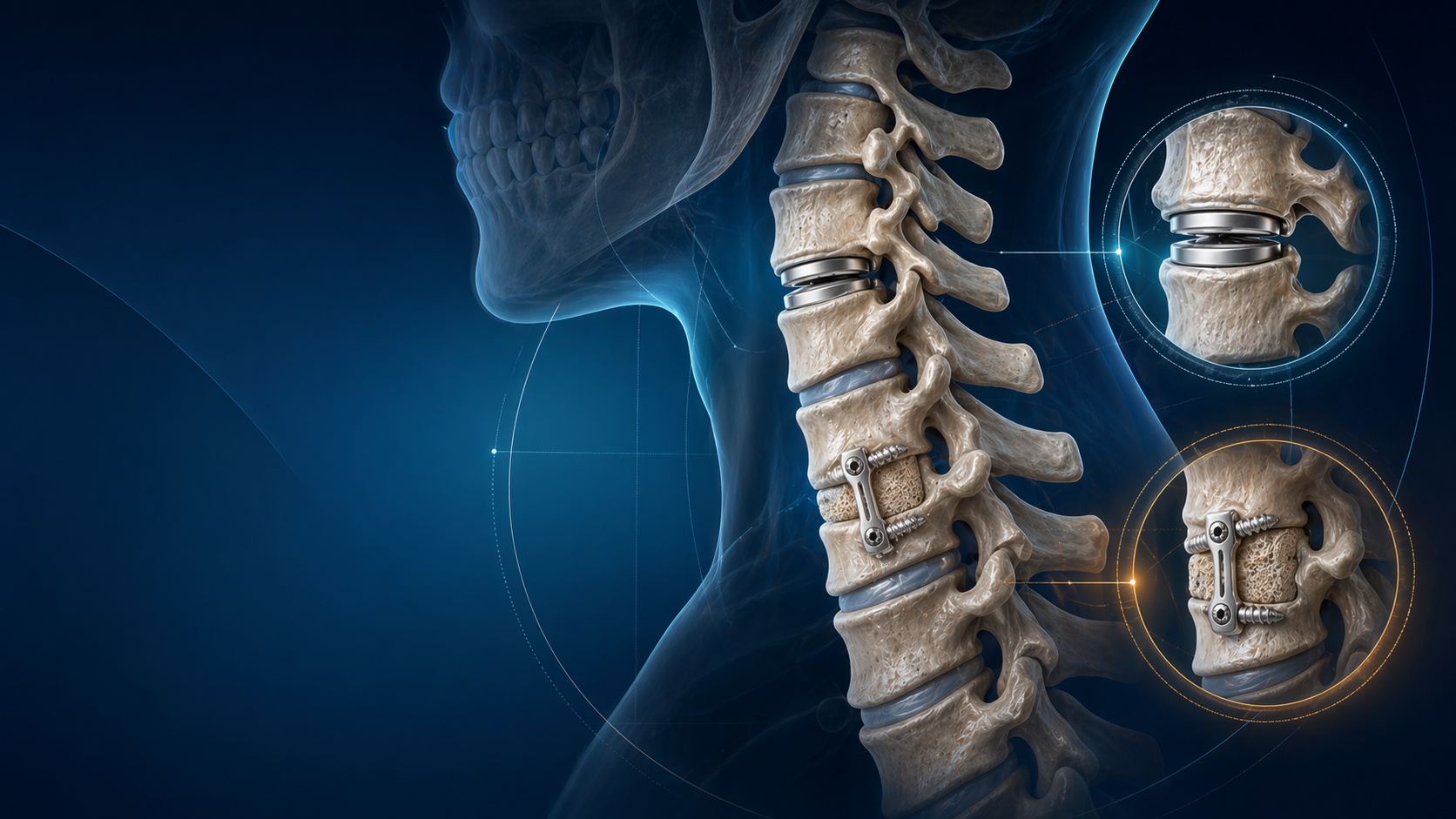
Cervical Disc Replacement vs ACDF in 2026: Who Actually Benefits?
Cervical disc arthroplasty has matured from “interesting new option” to a genuine alternative to anterior cervical discectomy and fusion in selected patients. The temptation is to flatten the argument into a slogan: motion preservation good, fusion old. That is not how good spine surgery works. The better question is narrower and more useful: which patients actually benefit from disc replacement, and which patients are still better served by ACDF?
Fast Takeaways
- In appropriately selected one-level disease, cervical disc replacement and ACDF often produce similar pain and functional outcomes.
- Reoperation rates tend to favour arthroplasty in several comparative datasets.
- Disc replacement is not a default upgrade. Facet degeneration, instability, deformity, and poor indication selection can erase any theoretical benefit.
- The correct operation is the one that matches pathology, alignment, and the patient’s goals.
- Two-level arthroplasty requires more careful indication discipline than marketing usually acknowledges.
Why This Matters in 2026
The 2023 AHRQ systematic review is a useful anchor because it avoids implant marketing and looks broadly at the comparative evidence. Its main message is nuanced: cervical arthroplasty can reduce reoperation risk in selected patients, but it does not produce a dramatic universal advantage in pain or function over ACDF for single-level disease.
That is probably the most clinically honest summary of the field. Arthroplasty is not magic. It is a well-supported option when the anatomy, pathology, and motion segment are right.
The Core Decision Points
1. Pathology first, implant second
Disc replacement is best considered in patients with symptomatic cervical degenerative disc disease where the pathology is primarily disc-level and motion preservation is biologically plausible. It becomes less attractive when the problem is dominated by:
- advanced facet arthrosis
- marked segmental instability
- major deformity or kyphosis
- severe spondylosis with poor motion to preserve
- multilevel disease beyond the implant’s evidence base or regulatory comfort zone
This is why “young patient equals disc replacement” is too simplistic.
2. Pain and function are not the whole story
One reason the debate persists is that both operations work well for the right patient. If you only look at short-term pain relief, the distinction can seem small. The real comparative edge of arthroplasty shows up more clearly in reoperation patterns and some adjacent-segment outcomes in selected series and meta-analyses.
That still needs cautious interpretation. Lower reoperation is meaningful, but it does not make every radiculopathy patient a disc candidate.
3. Motion preservation only matters if the segment can still behave like a good motion segment
The theoretical advantage of disc replacement is straightforward: maintain motion, reduce stress concentration, and potentially reduce adjacent segment burden. But a degenerative segment with advanced facet wear, collapse, or deformity is not a healthy motion segment waiting to be rescued. In those patients, fusion may be more biomechanically honest.
4. Two-level disease is a different conversation
The evidence for two-level arthroplasty is growing, but it is still not as simple as multiplying the one-level indication by two. The stronger the pathology burden, the more important it becomes to assess alignment, facet condition, and whether motion preservation is likely to be a benefit or a liability.
The best candidates for cervical disc replacement are not merely younger patients. They are patients with the right pathology at the right segment, with preserved enough local mechanics for motion preservation to be worth pursuing.
Common Pitfalls
Calling CDA “better” when the evidence is actually more selective
The more defensible statement is that CDA is a strong alternative to ACDF in selected patients and may reduce reoperation risk. That is much more accurate than saying it is simply superior.
Ignoring the facets
Facet degeneration can turn a motion-preserving idea into a disappointing operation. A preserved implant does not help if the pain generator is no longer mainly the disc.
Underestimating alignment
Good implant choice cannot fully compensate for poor overall cervical mechanics. The operation has to fit the spine, not just the disc space.
Overselling adjacent-segment protection
Arthroplasty may help reduce some adjacent-segment problems, but it does not abolish degeneration elsewhere in the cervical spine.
Exam and Practice Pearls
- Mention cervical disc arthroplasty and ACDF as operations with overlapping but not identical candidate groups.
- In a viva, say that clinical outcomes are often similar, but reoperation may favour arthroplasty in selected patients.
- If asked for contraindications to CDA, discuss facet disease, instability, deformity, and advanced spondylosis before listing implant trivia.
- Do not forget that cervical disc disease is a pathology spectrum, not a single operation.
References
- Selph SS, Skelly AC, Jungbauer RM, et al. Cervical Degenerative Disease Treatment: A Systematic Review. AHRQ Comparative Effectiveness Review. 2023.
- Ten-Year Outcomes of Cervical Disc Arthroplasty Versus Anterior Cervical Discectomy and Fusion: A Systematic Review With Meta-Analysis. 2024.
- Comparison of cervical disc arthroplasty versus ACDF for single-segment disease with a minimum of 4-year follow-up. 2025.
- Anterior cervical discectomy and fusion versus cervical disc arthroplasty: an epidemiological review of 433,660 surgical patients from 2011 to 2021. 2024.
Related topics
Share this article
Useful for a journal club, study list, or teaching session.


