Adductor-Related Groin Pain
- Adductor (groin) strain is the COMMONEST cause of acute groin pain in athletes, and the muscle most often injured is the ADDUCTOR LONGUS, typically at its musculotendinous junction or its proximal enthesis on the pubis; it is especially common in sports involving cutting, kicking and rapid change of direction such as soccer/football, ice hockey and Australian football.
- The MECHANISM is a forceful ECCENTRIC contraction of the adductors - the muscle contracting while being lengthened - during cutting, change of direction, kicking or reaching/lunging for a ball; large eccentric contractions are known to cause or exacerbate the strain (for example during run-to-cut manoeuvres), which is the basis for eccentric-focused prevention and rehabilitation.
- The CLINICAL picture is acute medial GROIN pain (sometimes with a tearing sensation), tenderness over the adductor origin/musculotendinous junction, and pain reproduced by RESISTED ADDUCTION and by the adductor 'SQUEEZE TEST' (pain/weakness on squeezing the examiner's fist or a ball between the knees); strains are graded I-III by severity (I minor, II partial tear with weakness, III complete tear/avulsion).
- The Doha agreement on terminology places this within ADDUCTOR-RELATED groin pain, one of the defined clinical entities of groin pain in athletes (alongside iliopsoas-related, inguinal-related and pubic-related groin pain, plus hip-joint causes), which encourages a systematic approach and recognition that more than one entity may coexist.
- IMAGING is used to confirm and grade and to exclude other causes: ULTRASOUND and MRI show the site and grade of the adductor strain (and any avulsion or proximal tendon tear), while assessment should also consider the differential of groin pain - osteitis pubis, iliopsoas, sports hernia/inguinal disruption, hip-joint pathology (FAI/labral tear) and, importantly in adolescents, an apophyseal avulsion rather than a muscle strain.
- MANAGEMENT is predominantly CONSERVATIVE with a HIGH REINJURY RATE that makes rehabilitation quality critical: initial relative rest/ice/analgesia, then a PROGRESSIVE, ECCENTRIC-based strengthening and reconditioning programme (e.g. Copenhagen-adduction-type exercises) restoring adductor strength and the adductor-to-abductor ratio, with a criteria-based return to sport; validated rehab/reconditioning programmes can return professional players in around two weeks for lower-grade injuries, while complete tears/avulsions or refractory cases occasionally need surgery (tenotomy/repair).
- “Adductor strain = commonest acute groin injury; ADDUCTOR LONGUS the usual muscle (musculotendinous junction/enthesis); ECCENTRIC contraction during cutting/kicking.
- “Acute medial groin pain; pain on RESISTED ADDUCTION and the SQUEEZE test; graded I-III; Doha 'adductor-related groin pain'. Exclude apophyseal avulsion in adolescents, osteitis pubis, sports hernia, hip pathology.
- “Conservative with HIGH reinjury rate - progressive ECCENTRIC strengthening (Copenhagen adduction), criteria-based return; surgery only for complete tear/avulsion or refractory cases.
Acute medial groin pain after cutting/kicking; tenderness over the adductor longus origin/musculotendinous junction; pain on resisted adduction and the squeeze test.
High reinjury rate - rehabilitate with progressive eccentric strengthening and a criteria-based return. Exclude apophyseal avulsion (adolescents) and other groin-pain causes.
Epidemiology, Risk Factors and Prevention
- Burden. Groin injuries account for a reported 4-19% of all time-loss injuries in male football, and adductor-related groin pain is the commonest subtype. The problem concentrates in the change-of-direction and kicking sports - football (soccer), ice hockey, Australian rules and handball - and in in-season play, when exposure to sprinting, cutting and kicking is highest.
- The dominant modifiable risk factor is adductor weakness. A low adductor strength, and particularly a low adductor-to-abductor strength ratio, is the most consistently reported predictor of subsequent groin injury - which is why it is both the screening measure and the rehabilitation target.
- Previous injury is the strongest non-modifiable predictor. A prior groin injury markedly raises the risk of a further one, and incomplete rehabilitation is the mechanism.
- Other contributors repeatedly cited: pre-season deconditioning, reduced hip range of motion, higher exposure/match load, and core/lumbopelvic control deficits that increase the demand on the adductors during single-leg loading.
- Prevention works. Adductor-strengthening programmes built around the Copenhagen adduction exercise reduce groin-injury rates at squad level, and are most effective when maintained through the season rather than performed only pre-season. Screening with hand-held dynamometry identifies the athletes to target.
If asked "how would you reduce groin injuries in a football squad?", answer with adductor strengthening (Copenhagen adduction), maintained in-season, plus dynamometry screening for low adductor strength and a low adductor-to-abductor ratio - and identify previous groin injury as the strongest risk marker.
Adductor Compartment Anatomy: Why the Adductor Longus
- The group. The hip adductors are the adductor longus, adductor brevis, adductor magnus, gracilis and pectineus, arising from the pubis/ischium and inserting along the linea aspera (gracilis onto the pes anserinus, the adductor magnus also to the adductor tubercle). They adduct the hip, contribute to flexion/rotation, and - crucially in sport - eccentrically control the limb and stabilise the pelvis during cutting and kicking.
- Why the adductor longus. Its proximal origin is a narrow, largely tendinous attachment to the body of the pubis (relatively poorly vascularised), so the musculotendinous junction and the pubic enthesis are the weak points that fail under eccentric load - which is why it is the most commonly strained adductor.
- Innervation. Mostly the obturator nerve (L2-4) (longus, brevis, gracilis and the adductor part of magnus); the adductor magnus hamstring portion is supplied by the tibial division of the sciatic and the pectineus by the femoral nerve - the nerve itself is developed in our Obturator Nerve Anatomy topic.
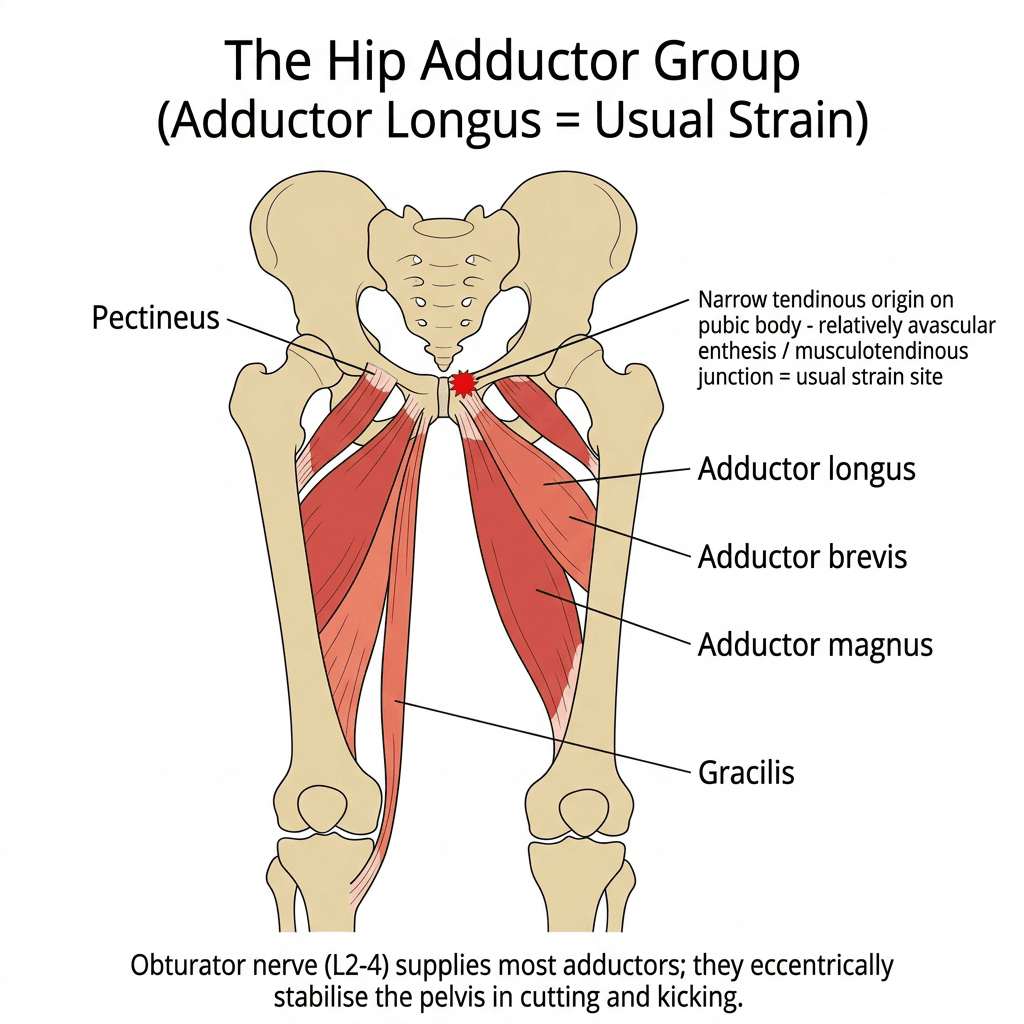
The adductor longus is the usual injury because its proximal origin is a narrow tendon on the pubic body (a relatively avascular enthesis/MTJ) loaded eccentrically in cutting. Group = longus, brevis, magnus, gracilis, pectineus; innervation is mostly obturator (magnus also tibial division; pectineus femoral). Its pelvic-stabilising role is why the adductor-to-abductor balance matters in rehab.
Clinical Presentation and Grading Systems
- History. Sudden medial groin pain during a cut, stretch, lunge or kick, often with a tearing or popping sensation. The athlete can usually localise the pain to the proximal medial thigh. A more insidious onset over weeks points instead to chronic adductor-related groin pain rather than an acute strain.
- Inspection. Swelling and bruising track distally down the medial thigh in higher-grade injuries; ecchymosis appearing a day or two later suggests a more substantial tear.
- Palpation. Tenderness is localised along the adductor longus - at the pubic enthesis, at the musculotendinous junction, or through the muscle belly. The site of maximal tenderness predicts the site of injury on imaging and should be documented.
- Provocation. Pain on resisted adduction and on the squeeze test; passive abduction stretch reproduces pain. Weakness on resisted testing, rather than pain alone, suggests a higher grade.
- Always examine the neighbours. Hip range of motion and impingement testing, the pubic symphysis, the inguinal canal and the abdominal wall - because the Doha entities coexist (the full framework is developed in our Athletic Groin Pain topic).
- How it grades
- I minor (pain, no weakness); II partial tear (pain plus weakness); III complete tear or avulsion
- What it adds
- Simple, bedside, still the commonest exam answer
- How it grades
- MRI grade 0-4, with a suffix for the site: a myofascial, b musculotendinous, c intratendinous
- What it adds
- The suffix matters - intratendinous (c) injuries take longer and reinjure more
- How it grades
- Separates functional (no structural lesion) from structural muscle injury, then subgrades
- What it adds
- Recognises that a painful muscle without a tear is a different problem
- How it grades
- Classifies the clinical entity: adductor-related, iliopsoas-related, inguinal-related, pubic-related, plus hip causes
- What it adds
- Frames the differential; entities frequently coexist
Know two axes: the Doha agreement names the entity (adductor-related groin pain), while BAMIC or Munich grade the severity and site. The examinable nuance in BAMIC is the letter suffix - a c (intratendinous) injury carries a longer return and a higher reinjury risk than the same numerical grade sitting at the musculotendinous junction.
Examination and Objective Strength Testing
- The squeeze test, by position. Resisted isometric adduction against the examiner's fist (or a sphygmomanometer/dynamometer) between the knees, classically tested in three positions - legs straight (0 degrees), hips flexed to about 45 degrees, and the bent-knee (90 degrees) position; pain or weakness reproduces adductor-related groin pain, and the bent-knee position is often the most provocative.
- Other clinical tests. Tenderness over the adductor-longus origin/musculotendinous junction, pain on active/resisted adduction, and bent-knee fall-out for range; localise to confirm the Doha 'adductor-related' entity (the full groin-pain framework sits in our Athletic Groin Pain topic).
- Objective strength. Hand-held dynamometry quantifies adductor and abductor strength; a reduced adductor-to-abductor strength ratio (weak adductors relative to abductors) is associated with increased groin-injury risk and is both a rehabilitation target and a return-to-play criterion (restored strength and a normalised ratio), which is why eccentric strengthening that rebuilds the ratio is central.
Do the squeeze test in three positions (0, 45 and 90 degrees of hip flexion; bent-knee often most provocative) and quantify with hand-held dynamometry. A low adductor-to-abductor strength ratio predicts groin injury and guides both prevention and a criteria-based return - so rehab targets the ratio, not just pain relief.
Investigations and Their Interpretation
- Most acute adductor strains need no imaging. The diagnosis is clinical. Image when the grade will change management, when a complete tear or avulsion is suspected, when the athlete is elite and a timeline is needed, or when the presentation is atypical or failing to progress.
- MRI is the reference standard: it shows the site (enthesis, musculotendinous junction, muscle belly), the extent of the tear, the tendon involvement that drives prognosis, and any retraction. Oedema on fluid-sensitive sequences maps the injury; the key report items are which structure, how much of its cross-section, and whether the tendon itself is involved.
- Ultrasound is quick, cheap and dynamic, and is well suited to confirming a strain, following healing, and guiding injection. It is operator-dependent and less reliable at the pubic enthesis and for intratendinous injury.
- Plain radiographs are for the bony questions: the adolescent apophyseal avulsion that mimics a strain, and the pubic changes of osteitis pubis in the chronic presentation.
- What a normal scan means. A normal MRI in a painful groin does not end the assessment - it pushes you towards the other Doha entities, the hip joint, or a functional (non-structural) injury.
Imaging findings in the groin are common in asymptomatic athletes - pubic marrow oedema and minor adductor signal change are frequently seen in players with no symptoms. Always correlate the scan with the site of maximal tenderness and the provocation tests, or you will treat an incidental finding and miss the real source.
Mechanism, Assessment & Differential
Adductor (groin) strain is the commonest acute groin injury in athletes, usually involving the adductor longus at its musculotendinous junction or proximal enthesis, in cutting/kicking sports. The mechanism is a forceful eccentric contraction during cutting, change of direction, kicking or reaching for a ball - the muscle loaded while lengthening - and large eccentric contractions cause or exacerbate the strain. Clinically there is acute medial groin pain, adductor tenderness, and pain on resisted adduction and the squeeze test, graded I-III. The Doha agreement classifies this as adductor-related groin pain, one of the defined groin-pain entities (with iliopsoas-, inguinal-, pubic-related and hip causes), and more than one may coexist. Ultrasound/MRI confirm and grade; the differential includes osteitis pubis, iliopsoas, sports hernia, hip pathology and - importantly in adolescents - an apophyseal avulsion rather than a strain.
Management & Return to Play
- Acute phase: relative rest, ice, analgesia; protect from re-loading.
- Progressive eccentric strengthening: the core of rehab - restore adductor strength and the adductor-to-abductor ratio (e.g. Copenhagen-adduction-type exercises) and reconditioning for the specific sport demands; validated reconditioning programmes can return professional players in about two weeks for lower-grade injuries.
- Criteria-based return to sport: pain-free, restored strength and sport-specific function - because the REINJURY rate is high if return is premature.
- Prevention: adductor-strengthening programmes (and addressing strength deficits/imbalance) reduce injury risk; directional compression shorts can reduce adductor loading during cutting.
- Surgery is uncommon: reserved for complete tears/avulsions or refractory adductor-related groin pain (e.g. tenotomy or repair).
Two points matter in adductor/groin strain. First, in the SKELETALLY IMMATURE athlete the apophysis is the weak link, so what looks like an adductor 'strain' after a forceful kick or sprint may actually be an APOPHYSEAL AVULSION (e.g. of the pubic or ischial apophysis), which a plain radiograph will show - so do not assume a muscle strain in an adolescent without considering and, if needed, imaging for an avulsion. Second, adductor strains have a HIGH REINJURY rate, and the main determinant of a durable recovery is the quality of rehabilitation and the discipline of a criteria-based return, not just time: a progressive eccentric-strengthening programme that restores adductor strength and balance, with return only when pain-free and strong, is what prevents the frustrating cycle of reinjury.
Complications, the Chronic Case and Outcomes
- Reinjury is the defining complication. It is common, it is usually the consequence of returning before strength and function are restored, and it is the reason a criteria-based return beats a time-based one.
- Progression to chronic adductor-related groin pain. A strain that is inadequately rehabilitated can settle into a persistent enthesopathy at the pubic attachment, with pain on loading that limits the athlete for months. This is the group in whom surgery (adductor tenotomy) is occasionally considered after a genuine, supervised, failed rehabilitation programme.
- Complete tear and proximal avulsion. Uncommon. Many are managed non-operatively with good functional results, even in athletes; repair is considered for the high-demand athlete or where retraction is substantial. Be able to argue both sides - the evidence does not mandate repair.
- Coexisting entities missed. Because the Doha entities overlap, a persisting groin is often a second unrecognised diagnosis (pubic-related, iliopsoas-related, inguinal-related or hip) rather than a failed adductor rehabilitation.
- Prognosis by severity. Low-grade injuries recover in weeks with a structured programme; higher grades, and particularly intratendinous injuries, take substantially longer and carry a higher reinjury risk. The quality of rehabilitation, not the passage of time, is the determinant.
If the groin does not settle, ask two questions before blaming the rehabilitation: is there a second Doha entity (pubic, iliopsoas, inguinal, hip), and is the injury intratendinous on MRI? Both change the timeline and the counselling.
Mnemonics & Memory Aids
ADDUCT
Hook:ADDUCT: Adductor longus, Direction-change mechanism, Doha entity, Use squeeze test, Consider avulsion in teens, Treat eccentrically (high reinjury).
SQUEEZE
Hook:SQUEEZE - the test that names the injury, and the checklist that manages it.
Three positions of the squeeze test
Hook:0 - 45 - 90: test all three, because a negative squeeze in one position does not exclude the diagnosis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A soccer player develops acute medial groin pain after a cutting movement. What is the likely diagnosis and how do you assess it?”
“How would you rehabilitate an adductor strain and reduce reinjury?”
What & mechanism
- Commonest acute groin injury; adductor longus usually (musculotendinous junction/enthesis)
- Eccentric contraction during cutting/kicking/change of direction
- Sports: soccer/football, ice hockey, AFL
Assessment
- Acute medial groin pain; adductor tenderness
- Pain on resisted adduction and the squeeze test; grade I-III
- Doha 'adductor-related groin pain'; ultrasound/MRI confirm and grade
Differential
- Adolescent apophyseal avulsion (image it), osteitis pubis
- Iliopsoas, sports hernia/inguinal disruption
- Hip-joint pathology (FAI/labral tear); entities may coexist
Management
- Acute: relative rest, ice, analgesia
- Progressive eccentric strengthening (Copenhagen adduction); restore adductor:abductor ratio
- Criteria-based return (high reinjury rate); surgery only for complete tear/avulsion or refractory
Evidence & Key Studies
Validated rehab and reconditioning programme after adductor longus injury in professional soccer
- High rates of adductor injuries and reinjuries in soccer indicate that prevention and reconditioning programmes are needed to prepare athletes for the specific demands of the sport.
- An expert-validated rehabilitation and reconditioning programme, based on strengthening the injured muscle and retraining conditional capacities, aimed to reduce reinjury risk.
- When applied to professional players, return to full team training occurred at about 13 days on average.
Hip adductor activation during run-to-cut manoeuvres (mechanism and load reduction)
- Athletes in sports such as hockey and soccer are at high risk of groin/adductor strains, and large eccentric contractions are known to cause or exacerbate strain injuries.
- Run-to-cut manoeuvres load the adductor longus, consistent with the eccentric/cutting mechanism of injury.
- Wearing directional compression shorts reduced stance-limb hip adductor activity, suggesting a way to reduce adductor demand on return to activity.
Doha agreement: the standard terminology and definitions for groin pain in athletes
- Twenty-four international experts from 14 countries reached unanimous agreement on a standard taxonomy after systematic reviews and a Delphi process.
- Groin pain in athletes is classified under three major headings: defined clinical entities (adductor-related, iliopsoas-related, inguinal-related and pubic-related), hip-related groin pain, and other causes.
- The classification is built on history and physical examination rather than imaging, which is what makes it usable at the bedside and in research.
Adductor Strengthening Programme: players adopt it readily but do not maintain it
- Groin injuries represent 4-19% of all time-loss injuries in male football, and the Adductor Strengthening Programme is the first groin-specific prevention programme shown to reduce the risk of groin problems.
- Of 501 players surveyed from the trial cohort, 96% believed preventive measures were needed and 91% believed a strengthening programme would reduce risk; 73% completed it in under five minutes.
- Despite that, only 46% reported performing the programme as recommended and just 31% planned to continue it the following season.
The high adductor injury/reinjury rate in soccer and the value of a validated, strengthening- based rehabilitation/reconditioning programme (with return to training in about two weeks for lower-grade injuries) come from the cited Jimenez-Rubio study; the eccentric/cutting mechanism (large eccentric contractions causing/exacerbating strain, adductor longus loading during run-to-cut, and adductor-load reduction with directional compression) from the cited Chaudhari study. The adductor longus as the usual site, the squeeze test and grading, the Doha adductor-related groin-pain framework, and the differential (including adolescent apophyseal avulsion) are standard, well-established teaching. (See also our Osteitis Pubis and Pelvic Apophyseal Avulsion Fractures topics.)