Systemic Autoinflammatory Disorder
- Adult-onset Still's disease (AOSD) is a systemic AUTOINFLAMMATORY disorder of the innate immune system - the adult counterpart of systemic juvenile idiopathic arthritis - driven by the IL-1 beta/IL-18 and IL-6 cytokine axis; IL-18 (and IL-1) reflect inflammasome activation and disease activity, correlating with the Pouchot score, ferritin and CRP.
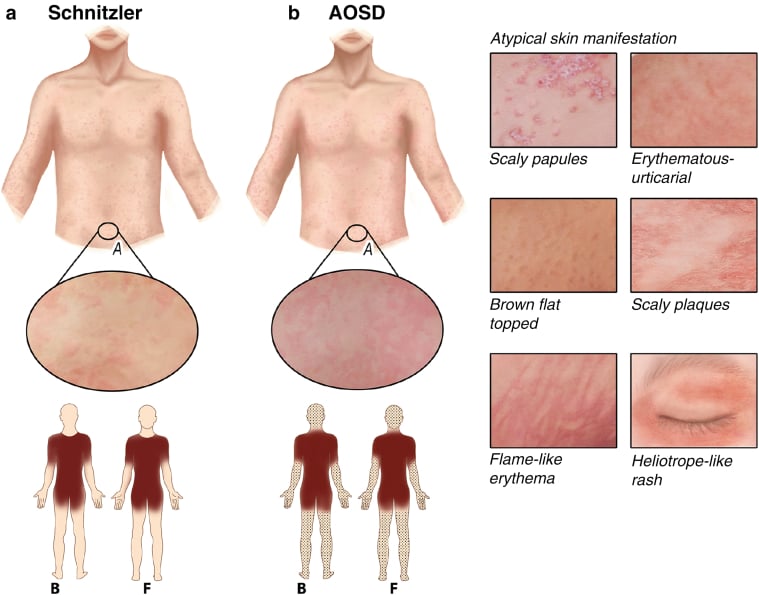
- The CLASSIC TETRAD is a daily (QUOTIDIAN) SPIKING FEVER, an EVANESCENT SALMON-PINK macular RASH (classically appearing with the evening fever spikes and fading between them), ARTHRALGIA/ARTHRITIS, and a markedly HIGH SERUM FERRITIN (with a characteristically LOW glycosylated ferritin fraction); a very high ferritin in a febrile young adult should raise AOSD.
- Supporting features include sore THROAT, LYMPHADENOPATHY, HEPATOSPLENOMEGALY, serositis, and a neutrophilic LEUCOCYTOSIS, with NEGATIVE ANA and RHEUMATOID FACTOR - the seronegativity is a useful clue distinguishing it from rheumatoid arthritis and lupus.
- DIAGNOSIS uses the YAMAGUCHI criteria (major criteria: fever at least one week, arthralgia at least two weeks, typical rash, leucocytosis with predominant neutrophils; minor: sore throat, lymphadenopathy/splenomegaly, abnormal liver function, negative ANA/RF) and is fundamentally a DIAGNOSIS OF EXCLUSION - infection/sepsis, malignancy (especially LYMPHOMA) and other connective-tissue disease must be excluded first.
- The feared complication is MACROPHAGE ACTIVATION SYNDROME (MAS) - a secondary haemophagocytic lymphohistiocytosis with a hyperferritinaemic cytokine storm (cytopenias, very high ferritin, coagulopathy, organ dysfunction) that is life-threatening and requires urgent recognition and treatment; the disease course may be monocyclic, polycyclic (relapsing) or chronic articular.
- The ORTHOPAEDIC relevance is the CHRONIC ARTICULAR form, which can cause a DESTRUCTIVE ARTHRITIS - classically a non-erosive-to-erosive carpal arthritis progressing to CARPAL/WRIST ANKYLOSIS (a recognised Still's pattern), and sometimes hip/knee involvement needing arthroplasty - while MANAGEMENT is medical: NSAIDs for mild disease, CORTICOSTEROIDS for systemic flares, and methotrexate or, increasingly, IL-1 (anakinra/canakinumab) and IL-6 (tocilizumab) BIOLOGICS for refractory or chronic disease and MAS.
- “AOSD tetrad = QUOTIDIAN spiking fever + EVANESCENT SALMON-PINK rash + arthritis + VERY HIGH FERRITIN (low glycosylated fraction). Seronegative (ANA/RF negative). Autoinflammatory (IL-1/IL-18/IL-6).
- “Yamaguchi criteria; DIAGNOSIS OF EXCLUSION - rule out sepsis, malignancy (lymphoma), other connective-tissue disease. Feared complication = macrophage activation syndrome (MAS).
- “Orthopaedic footprint = chronic destructive arthritis incl. carpal/wrist ankylosis. Treatment: NSAIDs -> steroids -> methotrexate / IL-1 (anakinra) / IL-6 (tocilizumab) biologics.
Young adult with daily spiking fever, an evanescent salmon-pink rash (with the spikes), arthritis, sore throat and a strikingly high ferritin - seronegative (ANA/RF negative). Yamaguchi criteria; a diagnosis of exclusion.
Macrophage activation syndrome - cytopenias, soaring ferritin, coagulopathy, organ failure - is the life-threatening complication. Recognise and treat urgently.
Presentation, Diagnosis & Course
AOSD is a systemic autoinflammatory disorder (IL-1/IL-18/IL-6) presenting with the tetrad of quotidian spiking fever, an evanescent salmon-pink rash, arthralgia/arthritis and a very high ferritin (low glycosylated fraction), plus sore throat, lymphadenopathy, hepatosplenomegaly, serositis and neutrophilic leucocytosis, with negative ANA/RF. Diagnosis uses the Yamaguchi criteria and is a diagnosis of exclusion - sepsis, malignancy (especially lymphoma) and other connective-tissue disease must be ruled out. The course is monocyclic, polycyclic (relapsing) or chronic articular, and the feared complication is macrophage activation syndrome (MAS).
The Diagnostic Criteria in Full: Yamaguchi, Fautrel and Pouchot
- The Yamaguchi rule. Diagnosis needs at least 5 criteria, of which at least 2 are major, AND the exclusions are satisfied. The 4 major: fever of at least 39°C for at least 1 week; arthralgia/arthritis for at least 2 weeks; typical rash; leucocytosis of at least 10,000 with at least 80% granulocytes. The 4 minor: sore throat; lymphadenopathy/splenomegaly; abnormal LFTs; negative ANA and RF. The exclusions: infection (especially sepsis/EBV), malignancy (especially lymphoma), and other rheumatic disease (especially vasculitis).
- The Fautrel alternative. An alternative set that adds the glycosylated ferritin fraction of 20% or less as a major criterion (other major items: fever of at least 39°C, arthralgia, transient erythema, pharyngitis, granulocytes at least 80%; minor: maculopapular rash, leucocytosis). It does not require exclusions and is more specific.
- Grading activity. The Pouchot (systemic) score grades disease activity - roughly one point each for a list of systemic manifestations (fever, rash, serositis, organomegaly, leucocytosis, sore throat and so on) - and correlates with ferritin and cytokine levels.
Q: How are the Yamaguchi and Fautrel criteria applied in AOSD?
A: Yamaguchi - need at least 5 criteria with at least 2 major AND exclusions met. Major: fever at least 39°C for at least 1 week, arthralgia at least 2 weeks, typical rash, leucocytosis at least 10,000 with at least 80% granulocytes. Minor: sore throat, lymphadenopathy/splenomegaly, abnormal LFTs, negative ANA/RF. Exclude infection/malignancy/other rheumatic disease. Fautrel adds glycosylated ferritin of 20% or less as a major criterion and needs no exclusions. The Pouchot score grades activity.
Macrophage Activation Syndrome: Recognising and Treating It
- The diagnostic paradoxes. MAS is a secondary haemophagocytic lymphohistiocytosis complicating AOSD. Suspect it when the inflammatory picture changes direction: new cytopenias (falling WBC/platelets/Hb - the opposite of AOSD's leucocytosis), a paradoxically falling ESR with a falling fibrinogen, rising triglycerides, a soaring ferritin (often over 10,000), rising transaminases/LDH, hepatosplenomegaly and coagulopathy/DIC. Haemophagocytosis may be seen on bone marrow, and soluble CD25 (IL-2 receptor) and sCD163 are raised.
- The score. The HScore (reactive-haemophagocytosis score) and the 2016 EULAR/ACR MAS criteria help formalise the diagnosis.
- Treatment. High-dose corticosteroids (pulse methylprednisolone) with anakinra (IL-1 blockade), ciclosporin, and etoposide for refractory/severe disease, plus intensive supportive care. It is a medical emergency.
Q: How do you recognise and treat macrophage activation syndrome in AOSD?
A: MAS is secondary HLH. Suspect it when the picture changes direction: new cytopenias (vs AOSD's leucocytosis), a paradoxically falling ESR + falling fibrinogen, rising triglycerides, a soaring ferritin (often over 10,000), rising LFTs/LDH, hepatosplenomegaly, coagulopathy; haemophagocytosis on marrow; raised sCD25/sCD163. The HScore / 2016 EULAR-ACR criteria formalise it. Treat urgently with high-dose steroids + anakinra ± ciclosporin ± etoposide.
Which Patients Get the Arthritis - the Course in Numbers
Naming three disease courses is only half an answer. For an orthopaedic surgeon the question is which patients end up in the chronic articular group, because those are the only ones who reach an orthopaedic clinic - and it is a minority.
In a retrospective cohort of 82 patients followed over two decades, the polycyclic systemic course was commonest at 45 percent, followed by monocyclic at 34 percent, with only 20 percent progressing to chronic arthropathy. A separate cohort of 57 patients followed for a mean of 8.4 years divided similarly - 17 monocyclic, 25 polycyclic and 15 chronic (roughly 30, 44 and 26 percent). So the destructive arthritis that gives the disease its orthopaedic relevance affects about one patient in four to five, and most patients' disease is systemic and episodic rather than joint-destroying.
The same 57-patient cohort found that a fever above 39.5 degrees predicted a MONOCYCLIC course, whereas arthritis at presentation was associated with the CHRONIC course and thrombocytopenia with complicated disease. The pattern is worth carrying: the loudest systemic presentation tends to burn out, while the patient whose joints are involved early is the one who goes on to chronic articular disease. Corticosteroid dependence occurred in 23 of 57 (45 percent) and was predicted by a low glycosylated ferritin, and the youngest patients had the highest risk of failing first-line treatment. These come from a single retrospective centre and are associations, not a validated prediction rule.
Two numbers put the "diagnosis of exclusion" framing into practical terms. The median time to diagnosis was 4 months in that cohort, which is the price of excluding sepsis and lymphoma first and is why a patient may arrive already months into an undiagnosed febrile illness. And macrophage activation syndrome is not a theoretical footnote: reactive haemophagocytic syndrome occurred in 8 of 57 patients (about 14 percent), with complications overall in 19. Mortality, by contrast, was low - 3 deaths, none attributable to the disease itself. So the honest summary is a condition that is slow to diagnose, complicates often, destroys joints in a minority, and rarely kills.
Quote the split: roughly one third monocyclic, 45 percent polycyclic, and only 20 to 26 percent chronic articular - the last group being the orthopaedic one. High fever points to a monocyclic course; arthritis at presentation points to the chronic one. Ferritin was raised in 91 percent and tracks disease activity, but no validated absolute cut-off defines the diagnosis.
Orthopaedic Relevance & Management
- Orthopaedic footprint: the chronic articular form - reached by only about 20 to 26 percent of patients, and predicted by arthritis being present at presentation rather than by how febrile they were - causes a destructive arthritis, classically a carpal arthritis progressing to carpal/wrist ankylosis (a recognised Still's pattern), and sometimes hip/knee disease needing arthroplasty.
- Medical management (the mainstay): NSAIDs for mild disease; corticosteroids for systemic flares; methotrexate as a steroid-sparing DMARD; IL-1 (anakinra, canakinumab) and IL-6 (tocilizumab) biologics for refractory/chronic disease.
- MAS: urgent recognition and treatment (high-dose steroids, anakinra/ciclosporin) - a medical emergency.
- Perioperative: any joint surgery is undertaken with the rheumatology team, optimising disease control and managing immunosuppression/steroids around surgery.
Adult-onset Still's disease is a diagnosis of exclusion, so the first safety priority is to rule out the serious mimics of a febrile young adult with a high ferritin - sepsis, malignancy (especially lymphoma) and other connective-tissue disease - before settling on AOSD; the seronegativity (negative ANA/RF) and the very high ferritin with a low glycosylated fraction support it, but they do not replace excluding infection and cancer. The second priority is macrophage activation syndrome, a secondary haemophagocytic lymphohistiocytosis that can complicate AOSD: a patient whose ferritin soars further and who develops cytopenias, a falling ESR with rising triglycerides/ferritin, coagulopathy and organ dysfunction may be in a cytokine storm that is rapidly fatal if unrecognised, and needs urgent intensive treatment. For the orthopaedic surgeon, the relevance is mainly the chronic destructive arthritis (notably carpal ankylosis) and the need to coordinate any surgery with the rheumatology team and manage immunosuppression around the procedure.
Mnemonics & Memory Aids
STILL
Hook:STILL: Salmon rash/Sore throat/Seronegative, Temperature (quotidian), IL-cytokines + high ferritin, Lymphadenopathy/Leucocytosis, Look out for MAS (excLusion).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young adult has daily spiking fevers, a salmon-pink rash that comes and goes with the fever, arthritis, and a ferritin of several thousand. What is the diagnosis and how is it managed?”
Classic tetrad
- Quotidian (daily) spiking fever
- Evanescent salmon-pink rash (with fever spikes)
- Arthralgia/arthritis + very high ferritin (low glycosylated fraction)
Diagnosis
- Autoinflammatory (IL-1/IL-18/IL-6); seronegative (ANA/RF negative)
- Yamaguchi criteria; sore throat, lymphadenopathy, hepatosplenomegaly, leucocytosis
- Diagnosis of EXCLUSION (sepsis, malignancy/lymphoma, other CTD)
Course & danger
- Monocyclic ~34% / polycyclic ~45% / chronic articular only 20-26%
- High fever predicts monocyclic; ARTHRITIS at presentation predicts the chronic course
- Macrophage activation syndrome = life-threatening cytokine storm (8 of 57 in one cohort); mortality low
- Orthopaedic: chronic destructive arthritis incl. carpal/wrist ankylosis - the minority course
Management
- NSAIDs (mild) -> corticosteroids (flares) -> methotrexate
- IL-1 (anakinra/canakinumab) and IL-6 (tocilizumab) biologics for refractory/chronic/MAS
- Coordinate joint surgery with rheumatology; manage perioperative immunosuppression
Evidence & Key Studies
Serum active IL-18 reflects inflammasome activation and disease activity in adult-onset Still's disease
- Inflammasome-mediated activation of IL-1 beta and IL-18 plays a key role in the pathogenesis of adult-onset Still's disease, a systemic autoinflammatory disorder.
- Serum active IL-18 was significantly higher in AOSD than in rheumatoid arthritis, familial Mediterranean fever and healthy controls, and correlated with the Pouchot disease-activity score, ferritin and CRP, decreasing after immunosuppressive therapy.
- Elevated active IL-18 was associated with rash and splenomegaly and had high diagnostic accuracy, supporting its role as a biomarker of inflammasome activation and disease activity.
Disease course and complications in 82 patients: only one in five reaches chronic arthropathy
- Retrospective cohort with prospective follow-up of 82 patients diagnosed in Taiwan between 1983 and 2003; 72 percent female and 67 percent aged 16 to 35 at onset.
- Presenting features: fever and articular symptoms in 100 percent, evanescent rash in 87 percent, sore throat in 84 percent, dermatographism in 59 percent.
- Disease course: POLYCYCLIC systemic 45 percent, MONOCYCLIC systemic 34 percent, and only 20 percent progressing to chronic arthropathy.
- Ferritin was elevated in 91 percent and correlated significantly with the disease-activity score and hepatic enzymes, supporting its use for MONITORING activity.
- Single-country retrospective series spanning two decades of changing therapy, and predominantly young women - the course proportions should be read as indicative rather than definitive.
Prognostic factors in 57 patients: arthritis predicts the chronic course, high fever the monocyclic one
- Retrospective review of 57 patients meeting Yamaguchi or Fautrel criteria, followed over a mean 8.4 years; MEDIAN TIME TO DIAGNOSIS was 4 months.
- Course: monocyclic in 17, polycyclic in 25, chronic in 15.
- Fever above 39.5 degrees predicted a MONOCYCLIC course; ARTHRITIS was associated with chronic disease and THROMBOCYTOPENIA with complicated disease; the youngest patients had the highest risk of resistance to first-line treatment.
- Complications were frequent (19 patients), including reactive haemophagocytic syndrome in 8; corticosteroid dependence occurred in 23 (45 percent) and was predicted by a low glycosylated ferritin.
- Mortality was low - 3 deaths, none attributable to the disease.
- Single-centre retrospective cohort of 57 patients: the prognostic associations are hypothesis-generating and have not been validated as a prediction rule.
The autoinflammatory pathogenesis of AOSD (the central role of the IL-1 beta/IL-18 inflammasome axis, with IL-18 correlating with disease activity, ferritin and CRP) comes from the cited Yoshida study. The classic clinical tetrad (quotidian fever, evanescent salmon-pink rash, arthritis, very high ferritin), the Yamaguchi diagnostic criteria, the status as a diagnosis of exclusion, macrophage activation syndrome as the feared complication, the chronic destructive arthritis (carpal ankylosis), and the treatment ladder (NSAIDs/steroids/methotrexate/IL-1 and IL-6 biologics) are standard, well-established teaching. The proportions of the three disease courses, the ferritin elevation rate and the presenting-feature frequencies come from the cited Chen cohort - a single-country retrospective series of 82 predominantly young women spanning two decades of changing therapy; the prognostic associations, the four-month median time to diagnosis, the 45 percent corticosteroid dependence and the 8-in-57 rate of reactive haemophagocytic syndrome from the cited Gerfaud-Valentin cohort, a single retrospective centre of 57 patients whose associations are hypothesis-generating rather than a validated prediction rule. No absolute serum-ferritin threshold with published sensitivity and specificity for diagnosing the condition was retrieved, so none is quoted here - the glycosylated fraction of 20 percent or less in the Fautrel set is the only ferritin-based criterion given a numeric cut-off. Drug doses are not stated: the biologic and immunosuppressive regimens are rheumatology-led and weight- or protocol-based, and no orthopaedic-specific schedule exists - prescribe to local formulary and protocol. Systemic juvenile idiopathic arthritis, of which this is the adult counterpart, is covered within juvenile idiopathic arthritis; for the joint disease that most often enters the differential see rheumatoid arthritis of the hand. No dedicated macrophage activation syndrome topic exists in the library, which is why its recognition and treatment are set out in full here.