Blood-Filled Cavities | Fluid-Fluid Levels | USP6 Gene | Curettage + Adjuvant
ABC CLASSIFICATION
Critical Must-Knows
- Fluid-fluid levels on MRI are the diagnostic hallmark (but not pathognomonic)
- USP6 gene rearrangement in 70% of primary ABC confirms diagnosis
- Eccentric expansile lytic lesion with soap-bubble appearance on X-ray
- 30% are secondary - always exclude underlying primary tumour (GCT, chondroblastoma)
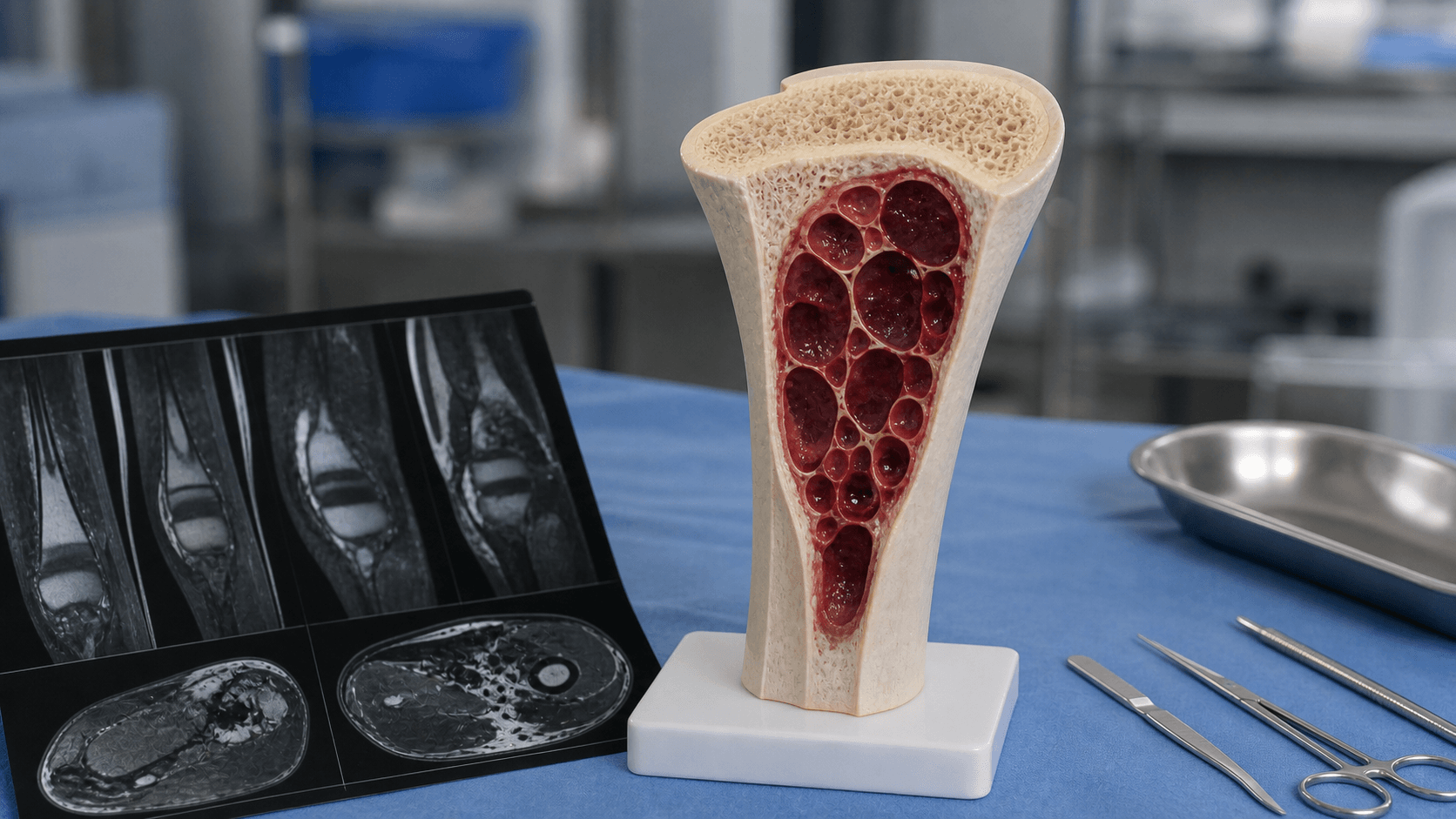
- Not a true cyst - blood-filled spaces separated by fibrous septa
Clinical Pearls
- "Fluid-fluid levels also seen in GCT, telangiectatic osteosarcoma - not specific
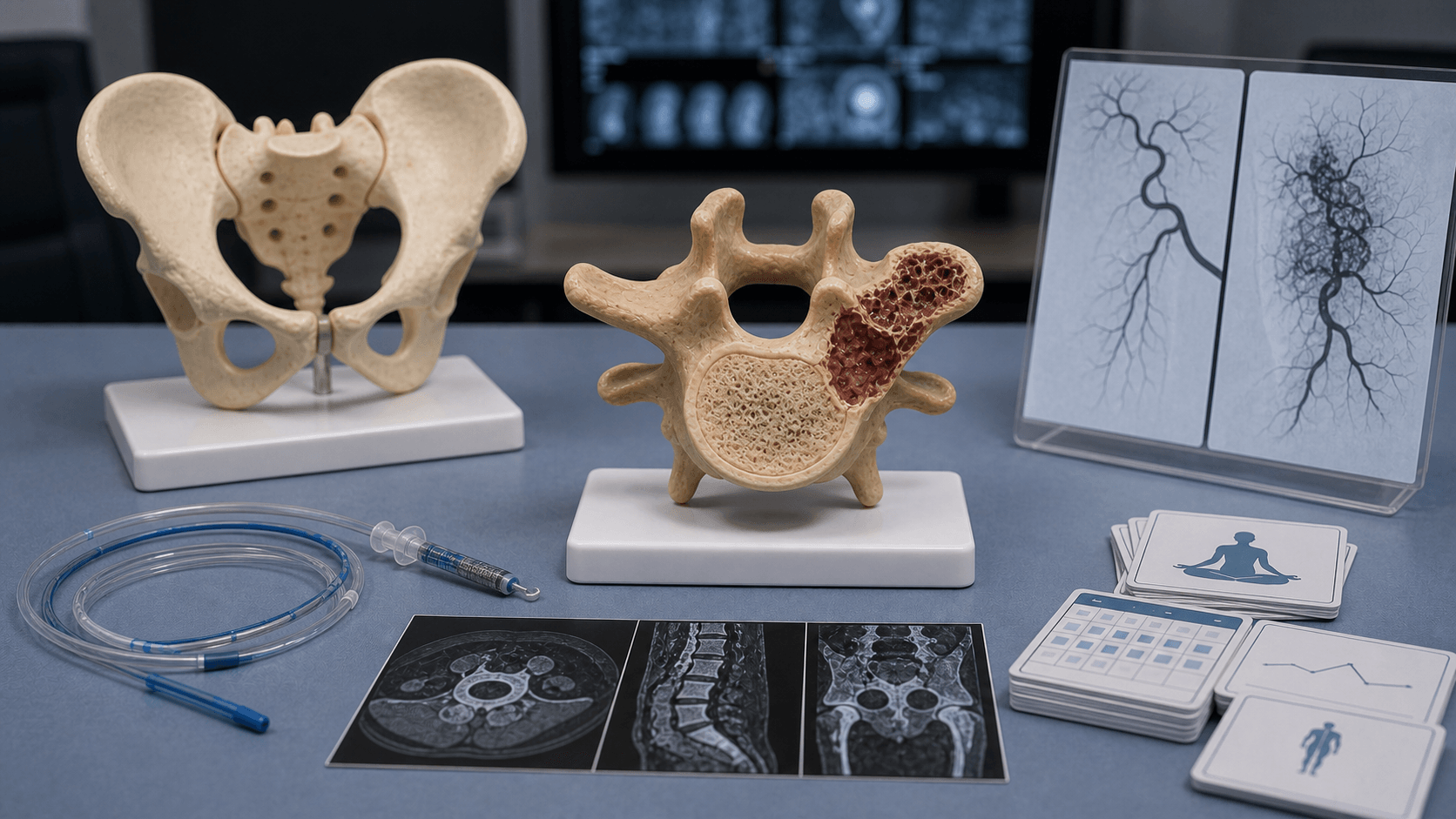
- "Spine ABC can present with neurological deficit requiring urgent decompression
- "Denosumab emerging as effective non-surgical treatment option
- "Recurrence usually within first 2 years after surgery
Clinical Imaging
Imaging Gallery


Critical ABC Exam Points
Fluid-Fluid Levels
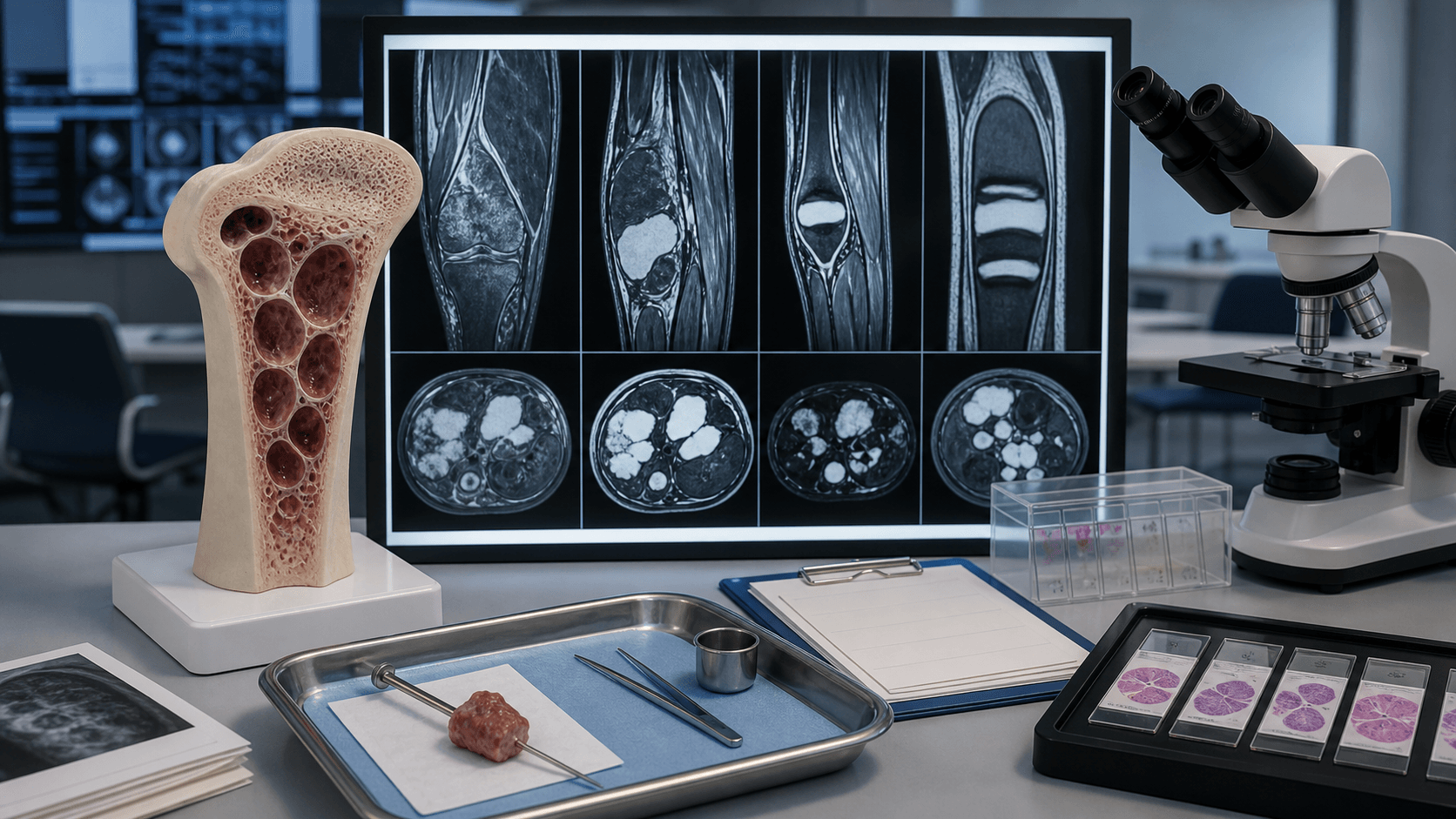
MRI fluid-fluid levels are characteristic but not pathognomonic. They represent blood products of different ages layering in cystic spaces. Also seen in GCT (14%), telangiectatic osteosarcoma, and other cystic lesions. Always consider malignancy.
Secondary ABC
30% of ABC are secondary to underlying lesions. Common precursors include giant cell tumour, chondroblastoma, osteoblastoma, and rarely telangiectatic osteosarcoma. Always biopsy solid areas to exclude malignancy.
USP6 Gene
USP6 gene rearrangement (FISH or RT-PCR) confirms primary ABC in 70% of cases. This genetic marker is not present in secondary ABC or in other tumours with fluid-fluid levels. Useful for diagnostic confirmation.
Management Options
Treatment options include curettage with adjuvant (bone grafting, PMMA, phenol), selective arterial embolisation, and emerging denosumab therapy. Recurrence rates 20-30% after curettage. Surgical inaccessibility may favour embolisation or denosumab.
Quick Decision Guide - Differential of Expansile Lytic Lesions with Fluid-Fluid Levels
| Diagnosis | Age | Key Features | Management |
|---|---|---|---|
| Primary ABC | Under 20 years | Eccentric, expansile, USP6 positive | Curettage + adjuvant |
| Secondary ABC | Any age | Within other lesion (GCT, chondroblastoma) | Treat underlying lesion |
| Giant Cell Tumour | 20-40 years | Epiphyseal, subarticular, RANK-L+ | Curettage + cement or denosumab |
| Telangiectatic osteosarcoma | 10-25 years | Aggressive, cortical destruction, atypical cells | Neoadjuvant chemo + resection |
| Simple bone cyst (UBC) | Under 20 years | Central, metaphyseal, fallen leaf sign | Steroid injection, curettage |
ABC - KABC - Key Features of Aneurysmal Bone Cyst
| A | Age under 20 75% occur in first two decades of life |
| B | Blood-filled cavities Separated by fibrous septa with giant cells |
| C | Cystic with fluid levels MRI fluid-fluid levels from layered blood products |
| A | Age under 20 75% occur in first two decades of life |
| B | Blood-filled cavities Separated by fibrous septa with giant cells |
| C | Cystic with fluid levels MRI fluid-fluid levels from layered blood products |
Hook:ABC is as easy as ABC - Age under 20, Blood-filled, Cystic with fluid levels
ABCSOAP - X-ray Features of ABC
| S | Soap-bubble appearance Multiloculated lytic lesion with thin septa |
| O | Off-centre (eccentric) Typically arises from metaphysis eccentrically |
| A | Aggressive expansion Expansile remodelling with cortical thinning |
| P | Pencil-thin cortex Blown-out appearance with eggshell cortex |
| S | Soap-bubble appearance Multiloculated lytic lesion with thin septa | A | Aggressive expansion Expansile remodelling with cortical thinning |
| O | Off-centre (eccentric) Typically arises from metaphysis eccentrically | P | Pencil-thin cortex Blown-out appearance with eggshell cortex |
Hook:SOAP bubble appearance with pencil-thin cortex
CURE - TCURE - Treatment Principles
| C | Curettage (extended) High-speed burr to extend margins |
| U | Use adjuvants Phenol, liquid nitrogen, or argon beam |
| R | Reconstruct defect Bone graft, PMMA cement, or combination |
| E | Embolisation or denosumab For surgically challenging locations |
| C | Curettage (extended) High-speed burr to extend margins | R | Reconstruct defect Bone graft, PMMA cement, or combination |
| U | Use adjuvants Phenol, liquid nitrogen, or argon beam | E | Embolisation or denosumab For surgically challenging locations |
Hook:CURE the ABC with extended curettage and adjuvant therapy
Overview and Epidemiology
Definition
Aneurysmal bone cyst (ABC) is a benign, locally aggressive bone lesion characterised by blood-filled cavities separated by fibrous septa containing fibroblasts and osteoclast-like giant cells. Despite the name, it is not a true cyst as it lacks an epithelial lining.
Key Epidemiology
Age Distribution:
- 75% occur in patients under 20 years old
- Peak incidence 10-20 years
- Rare in children under 5 years and adults over 50 years
Location:
- Long bone metaphysis (50%) - most commonly femur, tibia, humerus
- Spine (20%) - typically posterior elements
- Pelvis (10%)
- Flat bones and small bones (20%)
Types:
- Primary ABC (70%): De novo lesion with USP6 rearrangement
- Secondary ABC (30%): Arises within pre-existing bone lesion
Pathophysiology and Genetics
Genetic Basis
The understanding of ABC has been transformed by discovery of the USP6 gene rearrangement.
Primary ABC:
- 70% harbour USP6 (Tre2) gene rearrangement on chromosome 17p13
- Most common fusion partner is CDH11 (cadherin-11)
- USP6 overexpression leads to increased MMP production and osteoclast activation
- This confirms ABC is a true neoplasm, not a reactive process
Secondary ABC:
- Arises within pre-existing bone lesion
- No USP6 rearrangement
- Common precursor lesions:
- Giant cell tumour (most common)
- Chondroblastoma
- Osteoblastoma
- Fibrous dysplasia
- Telangiectatic osteosarcoma (must exclude)
Histological Features
Characteristic Findings:
- Blood-filled cavities (not lined by endothelium)
- Fibrous septa containing:
- Spindle-shaped fibroblasts
- Osteoclast-type giant cells
- Reactive woven bone
- Hemosiderin deposits
- Blue reticulated chondroid material - characteristic basophilic calcified matrix
- No cytologic atypia (important to exclude malignancy)
Classification
ABC Classification Systems
Classification by Origin:
| Type | Frequency | Characteristics | USP6 Status |
|---|---|---|---|
| Primary ABC | 70% | De novo lesion, no underlying pathology | Positive (70%) |
| Secondary ABC | 30% | Within pre-existing bone lesion | Negative |
Common Precursor Lesions for Secondary ABC:
- Giant cell tumour (most common)
- Chondroblastoma
- Osteoblastoma
- Fibrous dysplasia
- Telangiectatic osteosarcoma (must exclude)
- Osteosarcoma

Clinical Presentation
Presenting Symptoms
Local Pain:
- Most common presentation (80%)
- Gradual onset, progressive
- May worsen with activity
- Night pain uncommon (unlike malignancy)
Swelling:
- Visible or palpable mass
- May be warm due to vascularity
- Rapid enlargement can occur
Pathological Fracture:
- Occurs in 10-15%
- Due to cortical thinning and expansion
- May be the presenting complaint
Neurological Symptoms (Spine ABC):
- Present in 60-70% of spinal ABC
- Radiculopathy, myelopathy
- May require urgent decompression
- Posterior elements most commonly affected

Physical Examination
Findings:
- Local tenderness over lesion
- Swelling or mass effect
- Decreased range of motion if near joint
- Neurological deficit (spinal lesions)
Red Flags for Malignancy:
- Systemic symptoms (fever, weight loss)
- Rapid progression
- Severe night pain
- Very young or very old patient
Investigations
Imaging
Plain Radiographs
Classic Features:
- Eccentric expansile lytic lesion
- Soap-bubble or honeycomb appearance
- Pencil-thin periosteal shell (eggshell cortex)
- Internal septations creating multiloculated appearance
- Usually metaphyseal in long bones
Zone of Transition:
- Geographic pattern with narrow zone of transition
- No periosteal reaction (unless fractured)
- Trabeculated internal architecture
Aggressive Features (require careful evaluation):
- Cortical breach
- Soft tissue extension
- May indicate secondary ABC in malignant lesion
Plain radiographs are the first-line imaging but cannot reliably distinguish ABC from other lesions.

Biopsy
When Required:
- Diagnostic confirmation
- Rule out malignancy (especially secondary ABC)
- Before definitive treatment
Technique:
- CT-guided core needle biopsy preferred
- Sample solid areas - avoid purely cystic regions
- Send for histology AND cytogenetics (USP6 FISH)
Interpretation:
- Confirm ABC histology
- Exclude telangiectatic osteosarcoma (cellular atypia)
- USP6 rearrangement confirms primary ABC
Genetic Testing
USP6 Rearrangement:
- Present in 70% of primary ABC
- Detectable by FISH or RT-PCR
- Useful for diagnostic confirmation
- Absent in secondary ABC and other tumours
Management
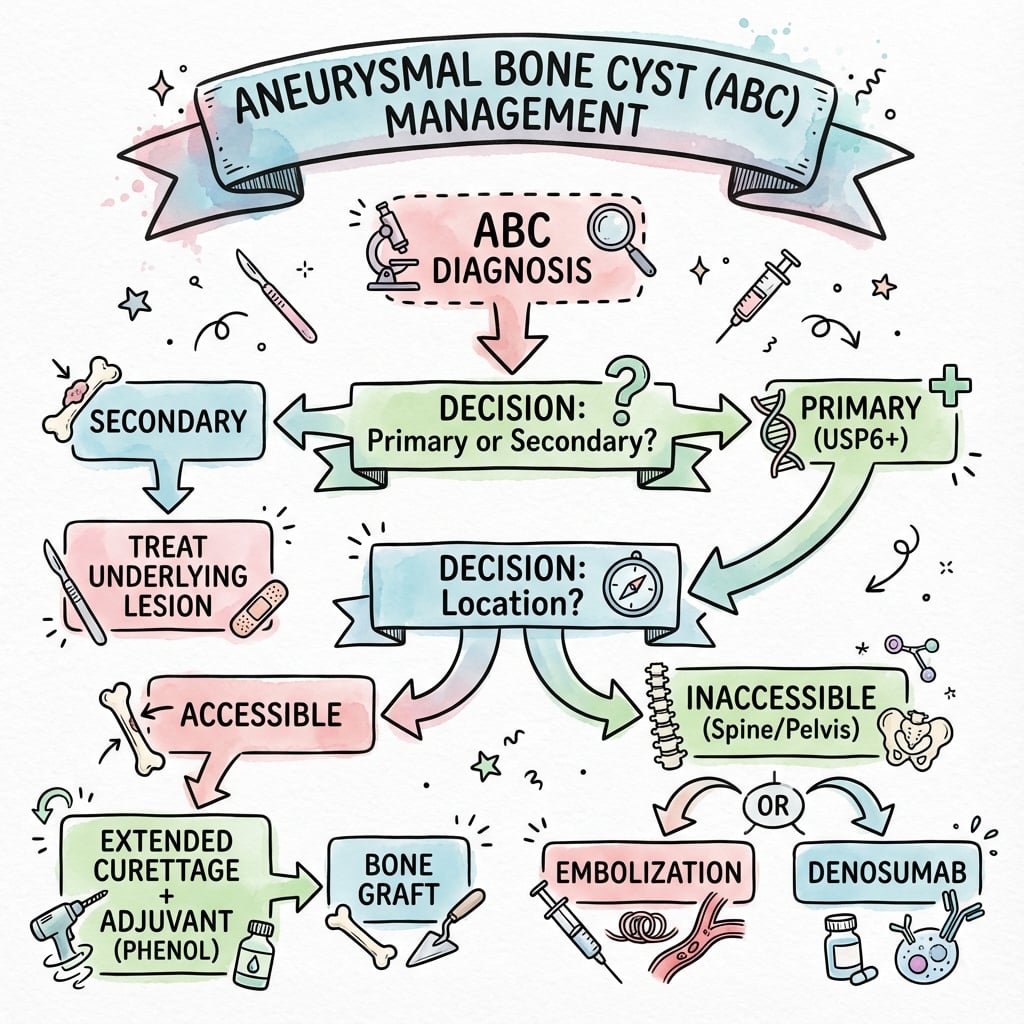
Treatment Algorithm
Factors Influencing Treatment:
- Location and accessibility
- Patient age and activity level
- Presence of pathological fracture
- Secondary vs primary ABC
- Risk of functional impairment
Surgical Management
Extended Curettage with Adjuvant
Gold Standard Treatment for accessible ABC:
Technique:
- Adequate surgical exposure
- Create cortical window
- Thorough curettage of all cyst contents
- High-speed burr to extend margins (2-3mm)
- Adjuvant therapy:
- Phenol (3 minutes)
- Liquid nitrogen cryotherapy
- Argon beam coagulation
- High-speed burr alone
- Reconstruct defect

Reconstruction Options:
- Autograft (iliac crest)
- Allograft (chips or structural)
- PMMA cement (provides immediate stability)
- Combination graft and cement
Outcomes:
- Local recurrence 10-30%
- Most recurrences within 2 years
- Better outcomes with adjuvant use
Extended curettage preserves bone stock and function while achieving local control.
Special Situations
Spinal ABC:
- May present with neurological deficit
- Posterior elements most commonly affected
- Treatment options include:
- Embolisation + surgery
- Curettage with stabilisation
- Radiation (controversial, reserved for inaccessible)
- Denosumab showing promise
Pathological Fracture:
- Initial immobilisation/splinting
- Allow fracture to heal before definitive treatment if possible
- May proceed with curettage and internal fixation
- Higher recurrence rate
Surgical Technique
Extended Curettage Technique
Pre-operative Planning:
- Review imaging for extent and cortical integrity
- Consider pre-operative embolisation for large/vascular lesions
- Plan reconstruction (bone graft vs cement)
- Blood products available for large lesions
Surgical Steps:
-
Positioning and Exposure:
- Position for adequate access to lesion
- Standard surgical approach to affected bone
- Identify and protect neurovascular structures
-
Create Cortical Window:
- Large enough for adequate visualization
- Usually through area of maximal cortical thinning
- Preserve cortical rim where possible
-
Curettage:
- Systematic removal of all cyst contents
- Remove septa and lining completely
- Curette all corners and recesses
Intraoperative Considerations
- Be prepared for significant bleeding (have blood products available)
- Complete curettage is essential - inspect all recesses
- Sample any suspicious solid tissue for pathology
- Preserve cortical rim where possible for stability
Complications and Prognosis
Complications
Local Recurrence:
- Most important complication
- Rate: 20-30% after curettage
- Usually within first 2 years
- Risk factors:
- Open physes (growth-related)
- Inadequate surgical margins
- No adjuvant use
- Pathological fracture at presentation
Treatment-Related:
- Pathological fracture (intra- or post-operative)
- Infection
- Joint stiffness (periarticular lesions)
- Growth disturbance (paediatric patients)
- Neurological injury (spinal ABC)
Malignant Transformation:
- Extremely rare
- Usually to secondary osteosarcoma
- Often after radiation therapy
Prognosis
Excellent Overall Prognosis:
- Benign lesion with zero metastatic potential
- Local control achievable in most cases
- 10-year disease-free survival over 90%
Recurrence Management:
- Re-curettage usually effective
- May consider resection after multiple recurrences
- Embolisation or denosumab for difficult locations
Long-term Follow-up:
- Clinical and radiographic at 3-6 monthly intervals for 2 years
- Then annually for 5 years
- Longer follow-up for spinal or pelvic lesions
Postoperative Care
Post-operative Protocol
Immediate Post-operative Care (0-2 weeks):
Wound Management:
- Standard surgical wound care
- Monitor for infection, haematoma
- Drains removed when output minimal
Pain Management:
- Multimodal analgesia
- Ice, elevation for swelling
Mobility:
- Weight-bearing status depends on:
- Lesion location and size
- Reconstruction type (cement vs graft)
- Internal fixation used
- Upper limb: Sling for comfort
- Lower limb: Protected weight-bearing with crutches
VTE Prophylaxis:
- Mechanical prophylaxis
- Chemical prophylaxis based on risk assessment
Outcomes
ABC Treatment Outcomes
Extended Curettage Outcomes:
| Outcome Measure | Rate | Notes |
|---|---|---|
| Local control | 70-90% | With adjuvant therapy |
| Recurrence | 10-30% | Usually within 2 years |
| Functional outcome | Excellent | MSTS scores 85-95% |
| Limb salvage | greater than 99% | Near universal |
Factors Affecting Recurrence:
- Open physes: 37% vs 21% in mature skeleton
- No adjuvant use: Higher recurrence
- Incomplete curettage: Major risk factor
- Solid ABC variant: Higher recurrence
Controversies and Areas of Uncertainty
- Optimal first-line modality: extended curettage remains standard, but the only randomised trial (Varshney 2010) showed sclerotherapy with comparable healing, fewer complications and lower hospital burden. Practice varies by region and lesion site rather than by high-level consensus.
- Denosumab role and risks: effective for inaccessible/recurrent ABC but evidence is case-series level. Concerns include rebound lytic activity and hypercalcaemia after cessation (especially in children), uncertain treatment duration, and effect on the open physis. It is not first-line for accessible lesions.
- Adjuvant choice: phenol, cryotherapy, argon beam and high-speed burring all reduce recurrence, but no adjuvant has been shown superior in randomised comparison.
- Solid ABC variant: must be distinguished from giant cell reparative granuloma and low-grade malignancy; its true recurrence risk is debated.
- Radiotherapy: historically used for inoperable lesions but largely abandoned because of the small but real risk of post-radiation sarcoma.
- Spinal ABC stabilisation: timing and extent of instrumentation versus embolisation-led management remain individualised, with no trial-level guidance.
Evidence Base
USP6/CDH11 Rearrangement Defines Primary ABC
- USP6 and/or CDH11 rearrangement in 36 of 52 primary ABC (69%)
- Rearrangement restricted to spindle (stromal) cells, absent in giant cells
- Absent in all 17 secondary ABC (GCT, chondroblastoma, osteoblastoma, fibrous dysplasia)
- Confirms primary ABC is a true clonal neoplasm, not a reactive process
CDH11-USP6 Fusion Oncogene Mechanism
- t(16;17)(q22;p13) juxtaposes the CDH11 promoter to the USP6 coding sequence
- The highly active bone-restricted CDH11 promoter drives USP6 over-expression
- Other ABC carry CDH11 or USP6 rearrangements via alternate mechanisms
- Established the oncogenic basis of ABC as a USP6-driven neoplasm
ABC Natural History and Curettage Outcomes (n=150)
- 150 ABC treated over 20 years; tibia, femur, pelvis, humerus, spine predominate
- Primary curettage with allograft/PMMA or autograft was standard
- Local recurrence rate 20%, consistent with other major series
- Lesions remain difficult to distinguish radiologically from other entities
Radiographic Classification and Surgical Treatment
- Proposed a radiographic staging system for ABC from a series of 198 cases
- Treatment of choice is surgical (curettage +/- phenol/cryosurgery, or resection)
- Surgical type selected by radiographic stage and growth rate of the cyst
- Radiotherapy reserved only for inoperable lesions
Sclerotherapy vs Curettage (Randomised Trial, n=94)
- 94 patients randomised to polidocanol sclerotherapy vs extended curettage + graft
- Healing 93.3% (sclerotherapy) versus 84.8% (curettage) at mean 4.4 years
- Fewer major complications and better function with sclerotherapy
- Similar recurrence rates between groups in this preliminary study
Selective Arterial Embolisation with NBCA (n=102)
- 102 patients embolised with N-2-butyl-cyanoacrylate; mean follow-up 7 years
- Complete healing in 81.8% (single or repeat embolisations)
- Recurrences more common under 15 years and in cysts over 6 cm
- Low complication rate (4.5%); not feasible in 13.6% (e.g. Adamkiewicz at risk)
Denosumab (RANKL Inhibition) in ABC
- Stromal cells express RANKL; giant/precursor cells express RANK in ABC
- RANKL expression comparable to giant cell tumour of bone
- Aggressive sacral ABC: tumour shrinkage and fracture healing after 3 months denosumab
- Function restored at 6 months; treatment well tolerated
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 14-year-old presents with a 3-month history of proximal tibial pain. X-ray shows an eccentric expansile lytic lesion with soap-bubble appearance. MRI demonstrates fluid-fluid levels. What is your diagnosis and how would you manage this patient?"
"Tell me about the pathological features of aneurysmal bone cyst and how you distinguish it from other lesions."
"A 25-year-old presents with back pain and leg weakness. MRI shows an expansile lesion of L3 posterior elements with fluid-fluid levels causing neural compression. How would you manage this?"
"What is the role of denosumab in managing aneurysmal bone cyst?"
Suggested Reading
Key References
-
Oliveira AM, Hsi BL, Weremowicz S, et al. USP6 (Tre2) fusion oncogenes in aneurysmal bone cyst. Cancer Res. 2004;64(6):1920-1923.
-
Oliveira AM, Perez-Atayde AR, Inwards CY, et al. USP6 and CDH11 oncogenes identify the neoplastic cell in primary aneurysmal bone cysts and are absent in so-called secondary aneurysmal bone cysts. Am J Pathol. 2004;165(5):1773-1780.
-
Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res. 1986;(204):25-36.
-
Mankin HJ, Hornicek FJ, Ortiz-Cruz E, et al. Aneurysmal bone cyst: a review of 150 patients. J Clin Oncol. 2005;23(27):6756-6762.
-
Varshney MK, Rastogi S, Khan SA, et al. Is sclerotherapy better than intralesional excision for treating aneurysmal bone cysts? Clin Orthop Relat Res. 2010;468(6):1649-1659.
-
Rossi G, Mavrogenis AF, Facchini G, et al. How effective is embolization with N-2-butyl-cyanoacrylate for aneurysmal bone cysts? Int Orthop. 2017;41(8):1685-1692.
-
Pelle DW, Ringler JW, Peacock JD, et al. Targeting receptor-activator of nuclear kappaB ligand in aneurysmal bone cysts: verification of target and therapeutic response. Transl Res. 2014;164(2):139-148.
-
De Cristofaro R, Biagini R, Boriani S, et al. Selective arterial embolization in the treatment of aneurysmal bone cyst and angioma of bone. Skeletal Radiol. 1992;21(8):523-527.
Suggested Reading
- WHO Classification of Tumours: Soft Tissue and Bone Tumours (5th Edition)
- Greenspan's Orthopedic Imaging
- Dahlin's Bone Tumors (6th Edition)
MCQ Practice Points
Diagnostic Imaging
Q: What is the characteristic MRI finding in aneurysmal bone cyst? A: Fluid-fluid levels - representing layered blood products of different ages within cystic spaces. Present in 70-90% of ABCs. However, this finding is NOT pathognomonic - also seen in GCT (14%), telangiectatic osteosarcoma, and chondroblastoma.
Genetics
Q: What genetic marker confirms the diagnosis of primary ABC? A: USP6 gene rearrangement - present in 70% of primary ABC. CDH11-USP6 is the most common fusion. This confirms ABC is a true neoplasm. Importantly, USP6 is ABSENT in secondary ABC and other lesions with fluid-fluid levels.
Epidemiology
Q: What is the typical age distribution of ABC? A: 75% occur in patients under 20 years with peak incidence at 10-20 years. Long bone metaphysis is the most common location (50%), followed by spine (20%) and pelvis (10%).
Secondary ABC
Q: What percentage of ABC are secondary and what lesions are they associated with? A: 30% are secondary - arising within pre-existing lesions. Common precursors include: giant cell tumour (most common), chondroblastoma, osteoblastoma, fibrous dysplasia, and rarely telangiectatic osteosarcoma. Always biopsy solid areas to exclude malignancy.
Treatment
Q: What is the gold standard treatment for accessible ABC and expected recurrence rate? A: Extended curettage with adjuvant therapy (phenol, cryotherapy, or argon beam) is the gold standard. Reconstruct with bone graft, PMMA, or combination. Local recurrence rate is 20-30%, usually within first 2 years. Risk factors for recurrence include open physes and inadequate margins.
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence: Approximately 0.14 per 100,000 population per year (roughly 1.4 per million); ABC accounts for around 1-6% of primary bone tumours
- Age: Peak 10-20 years; about 75-80% occur before age 20, consistent across populations
- Sex: Slight female predominance in most series
- Site distribution: Long-bone metaphysis (most common), spine and pelvis next; this pattern is stable worldwide
Side-by-Side Guidance and Consensus
| Body | Position relevant to ABC |
|---|---|
| WHO Classification (5th ed, 2020) | Defines ABC as a benign USP6-rearranged neoplasm; recognises primary vs secondary and solid variant |
| AAOS / MSTS (US) | Tissue diagnosis before definitive treatment; intralesional surgery (extended curettage + adjuvant) for accessible lesions |
| BOA / BSCOS (UK) | Suspected primary bone tumours referred to a specialist sarcoma/bone-tumour centre before biopsy |
| EFORT / European consensus | Endorses minimally invasive options (sclerotherapy, embolisation, denosumab) alongside curettage, especially in spine/pelvis |
| EMSOS (European Musculoskeletal Oncology) | Multidisciplinary planning and centralised biopsy for axial and pelvic lesions |
Where guidelines genuinely differ, the divergence is mainly in first-line modality for accessible lesions (curettage in most US/UK practice versus greater early use of sclerotherapy/embolisation in several European and high-volume Asian centres) rather than in oncological principles.
Registry and Trial Evidence
- No implant joint-registry (NJR/AJRR/AOANJRR) directly tracks ABC because reconstruction is usually graft or cement, not arthroplasty
- Evidence is driven by bone-tumour centre series and the single randomised trial comparing sclerotherapy with curettage (Varshney 2010)
- Multi-institutional sarcoma networks (e.g. EMSOS, regional bone-tumour registries) provide the pooled outcome data underpinning recurrence estimates
High- vs Limited-Resource Practice
| Setting | Typical pathway |
|---|---|
| High-resource | MRI + image-guided biopsy, USP6 FISH, MDT planning, choice of curettage, embolisation, sclerotherapy or denosumab |
| Limited-resource | Reliance on plain films and clinical diagnosis; percutaneous sclerotherapy attractive as low-cost, repeatable and theatre-light; molecular testing and denosumab often unavailable |
Centralised Referral
Suspected primary bone tumours, and all spinal/pelvic or recurrent ABC, should be referred to a specialist bone-tumour/sarcoma centre before biopsy to avoid compromising later surgery.
Multidisciplinary Care
Radiology, pathology, interventional radiology and orthopaedic oncology should jointly plan management, particularly for axial lesions and minimally invasive options.
Aneurysmal Bone Cyst - Exam Summary
Clinical summary
Definition & Epidemiology
- •Benign expansile lesion with blood-filled cavities
- •Peak age 10-20 years, 75% under 20
- •Primary (70%, USP6+) vs Secondary (30%, in other lesion)
- •Long bone metaphysis, then spine, then pelvis
Imaging Features
- •X-ray: Eccentric, expansile, soap-bubble, pencil-thin cortex
- •MRI: Fluid-fluid levels (70-90%), peripheral low signal rim
- •CT: Cortical detail, septations, surgical planning
- •Fluid-fluid levels NOT pathognomonic - also GCT, telangiectatic OS
Pathology
- •Blood-filled cavities (not true cysts - no epithelial lining)
- •Fibrous septa with giant cells, fibroblasts, reactive bone
- •Blue reticulated chondroid material characteristic
- •USP6 gene rearrangement in 70% of primary ABC
Management
- •Extended curettage + adjuvant (phenol, cryo, burr)
- •Reconstruct with bone graft, cement, or combination
- •Embolisation for spine/pelvis or pre-operatively
- •Denosumab emerging for difficult cases
Prognosis & Recurrence
- •Local recurrence 20-30% (usually within 2 years)
- •Higher recurrence with open physes
- •Zero metastatic potential
- •Re-curettage effective for recurrence
Exam Pearls
- •Always exclude secondary ABC (biopsy solid areas)
- •USP6 testing differentiates from other lesions
- •Spinal ABC may need urgent decompression
- •Denosumab - know mechanism and indications