Motion-Preserving Surgery | Patient Selection Critical | Outcomes Improving
- TAA preserves motion (average 30° dorsiflexion, 45° plantarflexion) compared to arthrodesis
- Ideal candidate: age 40-60, BMI under 30, intact ligaments, good bone stock, minimal deformity
- Contraindications: active infection, avascular necrosis of talus, severe neuropathy, inadequate bone stock
- Modern 3-component mobile-bearing designs show superior outcomes to fixed-bearing
- AOANJRR shows TAA revision rate 15% at 10 years vs 8% for ankle arthrodesis
- “TAA vs arthrodesis: motion preservation improves gait biomechanics and protects adjacent joints
- “TARVA RCT (Ann Intern Med 2022): no significant difference between TAR and fusion in MOXFQ walking/standing at 1 year - both improve
- “Alignment critical: varus/valgus malalignment over 10° associated with early failure
- “Periprosthetic cysts common (40%) but not always clinically significant - monitor with CT
Clinical Imaging
Imaging Atlas

Wrong patient = early failure. Age 40-60, BMI under 30, non-inflammatory arthritis, intact ligaments, good bone stock, minimal deformity (under 10° coronal, under 15° sagittal). Sedentary to moderate activity level. Realistic expectations about limitations.
Neutral mechanical axis mandatory. Varus/valgus malalignment over 10° leads to edge loading and early failure. May require staged deformity correction (supramalleolar osteotomy, deltoid release, lateral ligament reconstruction) before definitive TAA.
Not either/or - patient-specific. TAA preferred for bilateral disease, ipsilateral hindfoot/midfoot arthritis, contralateral ankle fusion. Arthrodesis for young heavy laborers, severe deformity, poor bone stock, neuropathy. TARVA RCT: comparable 1-year outcomes - choice is patient-specific.
15% revision at 10 years. Wound complications 10%, aseptic loosening 8%, subsidence 5%, periprosthetic fracture 3%, infection 2%. Conversion to arthrodesis possible (80% successful) but bone loss complicates. Adjacent joint degeneration reduced compared to fusion.
| Patient Scenario | Best Option | Rationale | Key Pearl |
|---|---|---|---|
| Age 45-60, unilateral OA, BMI 25, sedentary-moderate activity | Total Ankle Arthroplasty | Ideal candidate - preserves motion, good bone stock, manageable activity | 90% survival at 10 years with modern implants |
| Bilateral ankle arthritis, one side already fused | TAA on contralateral side | Preserve at least one mobile ankle for gait biomechanics | Bilateral fusion severely impacts mobility and quality of life |
| Age 35, heavy laborer, post-traumatic OA, varus malalignment 15° | Arthrodesis (after deformity correction) | Young age, high demand, significant deformity poor for TAA | Can return to heavy labor after fusion - not after TAA |
| Avascular necrosis of talar body, coronal deformity 20° | Arthrodesis or tibiotalocalcaneal fusion | Inadequate bone stock and severe deformity contraindicate TAA | TAA requires intact talus and near-neutral alignment |
STABLETAA Patient Selection Criteria
Hook:A STABLE ankle foundation is required for successful arthroplasty - any instability leads to early failure!
INFECTIONSTAA Absolute Contraindications
Hook:Screen for INFECTIONS and other contraindications - they predict failure, and fusion is the safer option!
TACModern TAA Implant Components
Hook:TAC the ankle - 3-component mobile-bearing design is current gold standard!
Overview and Epidemiology
Total ankle arthroplasty has evolved from a rarely performed procedure with poor outcomes to a viable motion-preserving alternative to ankle arthrodesis. Third-generation mobile-bearing implants demonstrate 90% survival at 10 years, approaching outcomes of total hip and knee arthroplasty. The procedure preserves ankle motion, improves gait biomechanics, and protects adjacent joints from accelerated degeneration seen with fusion. Patient selection and surgical precision are critical for success.
- Primary indication: End-stage ankle osteoarthritis with disability despite conservative management
- Mean age: 60 years (range 40-75 optimal)
- Gender: Equal distribution in post-traumatic OA; females predominate in inflammatory arthritis
- Etiology: 70% post-traumatic, 20% primary OA, 10% inflammatory arthropathy
- Activity level: Sedentary to moderate activity - not high-impact sports or heavy labor
- Registry survival: ~90% at 5 years for modern primary TAR (NJR England & Wales, PMID 37345846)
- Early registry-era benchmark: 89% at 5 years, 76% at 10 years (Norway, PMID 17966015)
- Revision burden: consistently higher than hip/knee arthroplasty across all major registries
- Common implants: STAR (mobile-bearing), Infinity, INBONE, Cadence, Salto Talaris (fixed-bearing)
- Leading failure modes: aseptic loosening, subsidence and instability; conversion to fusion is the commonest salvage
Anatomy and Biomechanics
The ankle (talocrural joint) is a highly congruent, constrained hinge joint that transmits 3-5× body weight during gait. Normal ankle motion is 10° dorsiflexion and 20° plantarflexion (total 30° arc). The talus has no muscular attachments and relies entirely on blood supply from surrounding arteries - making it vulnerable to avascular necrosis. The deltoid ligament complex and lateral collateral ligaments provide coronal plane stability essential for TAA success.
| Structure | Function | TAA Significance |
|---|---|---|
| Tibial plafond | Concave articular surface (wider anteriorly) | Requires flat tibial component with stable fixation |
| Talar dome | Convex articular surface with trochlear contour | Anatomic talar component preserves bone stock |
| Deltoid ligament | Medial stability - resists valgus and external rotation | Incompetence leads to valgus tilt and medial subsidence |
| Lateral collateral complex | ATFL, CFL, PTFL - resists varus and inversion | Laxity causes varus tilt and lateral edge loading |
| Talar blood supply | Artery of tarsal canal, artery of tarsal sinus, deltoid branches | Compromised by extensive dissection - risk of AVN |
Classification Systems
Mobile-Bearing Anatomic Designs (2000s-present)
| Design Features | Biomechanical Advantage | Clinical Benefit |
|---|---|---|
| 3-component mobile-bearing | Polyethylene insert translates and rotates | Reduces constraint and edge loading |
| Anatomic talar component | Preserves talar bone stock and contour | Enables revision or conversion to fusion |
| Flat tibial surface with sulcus | Anterior-posterior stability with mobility | 10° anterior-posterior translation allowed |
| Uncemented porous coating | Biological fixation without cement stress | 90% osseointegration at 2 years |
| Minimally invasive approach | Preserves soft tissue envelope | Reduced wound complications from 20% to 10% |
Current implants: STAR (Stryker), Infinity (Stryker), Cadence (Integra), INBONE (Wright Medical), Salto Talaris (Integra)
Evidence base: TARVA RCT and STAR pivotal trial, plus multiple national registry studies supporting modern mobile- and fixed-bearing designs.
Third generation represents mature technology with reproducible good outcomes in appropriately selected patients.
Clinical Assessment
TAA outcomes are highly dependent on appropriate patient selection. A well-executed TAA in a poor candidate will fail. Key selection criteria: age 40-60, BMI under 30, sedentary to moderate activity, intact or reconstructible ligaments, adequate bone stock, correctable alignment (under 10° coronal, under 15° sagittal), absence of infection or neuropathy, realistic expectations. Wrong patient selection is the most common cause of preventable failure.
Clinical Assessment
- Pain severity: Rest pain vs activity-related, night pain
- Function: Walking distance, stairs, ADLs impact
- Previous treatment: Injections, bracing, physiotherapy, surgery
- Etiology: Trauma, inflammatory, primary OA
- Occupation: Heavy labor contraindication
- Activity goals: High-impact sports unrealistic post-TAA
- Medical comorbidities: Diabetes, peripheral vascular disease, neuropathy
- Smoking status: Must quit minimum 6 weeks preoperatively
- Gait: Antalgic, foot progression angle, hindfoot alignment
- Alignment: Standing hindfoot varus/valgus (clinical and radiographic)
- Range of motion: Active and passive dorsiflexion/plantarflexion
- Ligament stability: Varus/valgus stress, anterior drawer
- Deformity: Fixed vs correctable with manual stress
- Neurovascular: Dorsalis pedis, posterior tibial pulses, sensation
- Skin: Scars, soft tissue coverage, previous surgical approaches
- Adjacent joints: Subtalar, talonavicular, midfoot arthritis
| Test | Assesses | Positive Finding | Significance for TAA |
|---|---|---|---|
| Anterior drawer | ATFL integrity | Anterior subluxation of talus over 10mm | May require lateral ligament reconstruction |
| Varus stress | Lateral collateral complex | Talar tilt over 10° compared to contralateral | Significant instability - may contraindicate TAA |
| Valgus stress | Deltoid ligament | Talar tilt over 10° or medial gapping | Deltoid incompetence leads to valgus subsidence |
| Subtalar motion | Hindfoot mobility | Stiffness or pain with inversion/eversion | Fixed hindfoot deformity complicates TAA |
Assessment findings guide surgical planning and determine if staged procedures needed before TAA.
Differential Diagnosis of the Painful Arthritic Ankle
| Condition | Distinguishing Features | Key Investigation | Implication for TAA |
|---|---|---|---|
| Subtalar / talonavicular arthritis | Hindfoot (not anterior ankle) pain, pain on inversion/eversion rather than dorsi/plantarflexion | Selective diagnostic injection; weight-bearing CT | If the ankle is not the pain source, TAA will not relieve symptoms - may need hindfoot fusion |
| Talar avascular necrosis / osteochondral lesion | Deep aching pain, may follow trauma or steroid/alcohol use | MRI (low T1 signal, collapse); CT for bone stock | Significant talar AVN is a contraindication to TAA - favours TTC fusion |
| Inflammatory arthritis (RA, PsA, gout) | Polyarticular, morning stiffness, systemic features; gout - acute crystal attacks | Inflammatory markers, serology, urate, joint aspirate | Acceptable for TAR if disease controlled; registries show RA survivorship at least as good as OA |
| Septic / infective arthritis | Hot swollen joint, fever, raised CRP/ESR | Aspiration with Gram stain/culture, bloods | Active infection is an absolute contraindication - eradicate before any implant |
| Charcot neuroarthropathy | Gross deformity disproportionate to pain, neuropathy (e.g. diabetes) | Clinical exam, radiographs, sensory testing | Contraindication to TAA - high failure; consider fusion or bracing |
| Chronic ankle instability with secondary OA | Recurrent giving-way, positive anterior drawer / talar tilt | Stress radiographs, MRI of ligaments | Ligament reconstruction may be needed before or with TAA to avoid edge loading |
Investigations
Imaging Protocol
Imaging Sequence
Views: AP ankle, mortise, lateral ankle, hindfoot alignment
Assess:
- Joint space narrowing and subchondral sclerosis
- Coronal plane deformity (tibiotalar angle, talar tilt)
- Sagittal plane deformity (anterior tibial translation, posterior talar subluxation)
- Bone stock (tibia, talus quality and quantity)
- Osteophytes and bone cysts
Measurements:
- Tibiotalar angle (normal 90° ± 3°)
- Talar tilt (normal under 5°)
- Anterior translation (normal under 3mm)
- Hindfoot alignment angle on hindfoot view
3D CT provides:
- Accurate assessment of bone stock and cysts
- Talar body AVN detection
- Precise deformity measurement in all planes
- Templating for component size and positioning
- Assessment of subtalar and talonavicular joints
- Surgical planning for bone cuts
CT particularly useful for revision cases and complex deformity.
Indications:
- Suspected talar AVN
- Soft tissue assessment (ligaments, tendons)
- Osteochondral lesions
- Cyst characterization
Not routinely required for straightforward primary TAA.
Use for:
- Painful TAA - identify component loosening
- Uncertain pain source in polyarticular disease
- Distinguishing subtalar from ankle arthritis
Helpful when conventional imaging inconclusive.
Contraindications on imaging: Talar AVN (low signal on MRI, collapse on CT), severe bone loss (inadequate platform for components), uncorrectable deformity (over 20° coronal or sagittal plane), deltoid insufficiency with valgus tilt, large uncontained bone cysts (over 15mm). These findings should prompt consideration of arthrodesis instead of TAA.
Comprehensive imaging assessment is mandatory for appropriate patient selection and surgical planning.
Management Algorithm
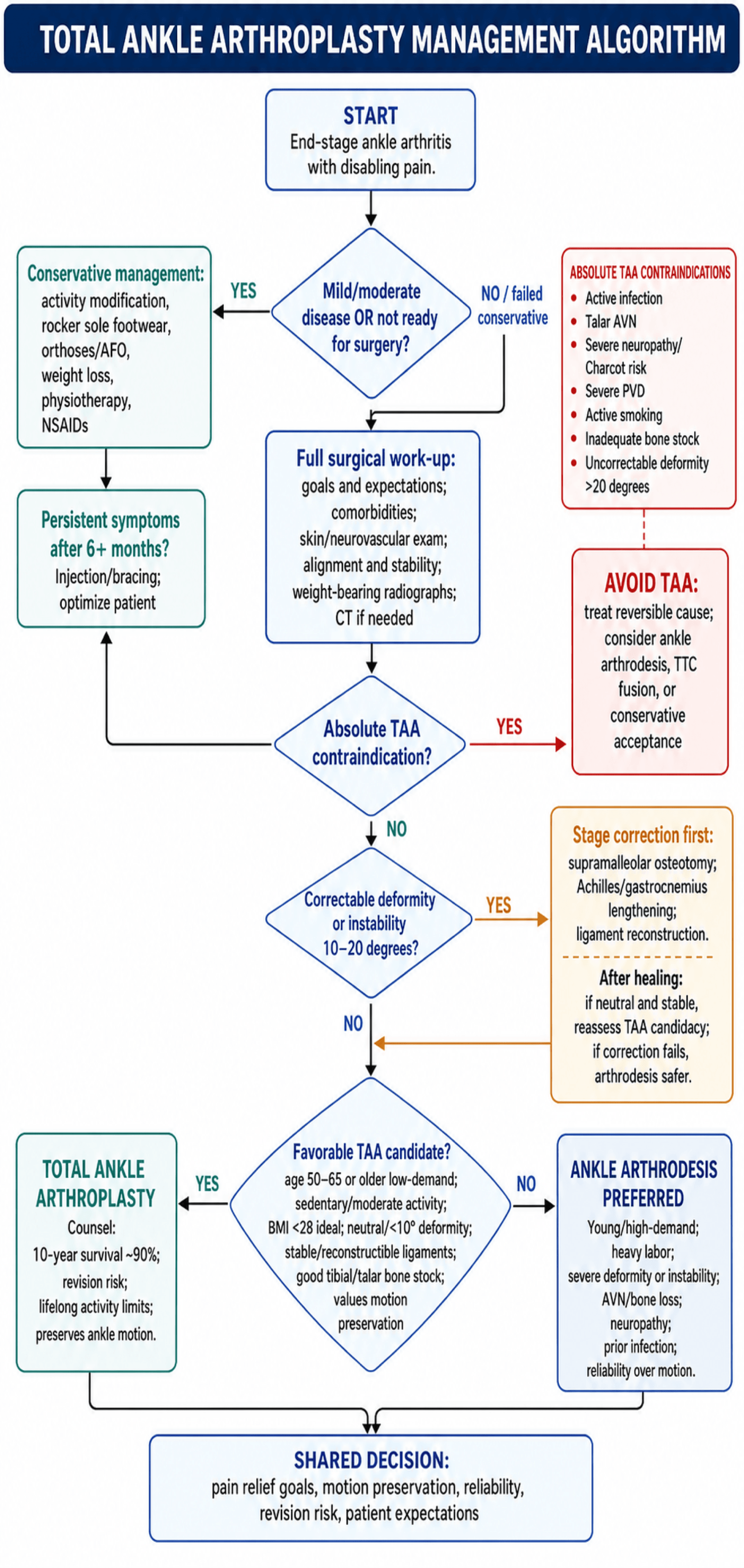
The fundamental management decision in end-stage ankle arthritis is choosing between total ankle arthroplasty (motion-preserving) and ankle arthrodesis (motion-sacrificing). This decision must be individualized based on patient age, activity demands, bone quality, deformity, ligament stability, and expectations. There is no universal "right answer" - both procedures effective for pain relief with different trade-offs.
Non-Operative Treatment Options
Conservative Treatment Escalation
- Activity modification: Avoid high-impact, prolonged standing
- Footwear: Cushioned shoes with rocker-bottom soles
- Orthotics: Custom foot orthoses, ankle-foot orthosis (AFO)
- Weight loss: If BMI elevated (reduces joint load)
- Physiotherapy: Ankle ROM, strengthening, proprioception
- NSAIDs: Oral or topical anti-inflammatories
- Corticosteroid injection: Intra-articular 1-3× per year (max 3 lifetime)
- Hyaluronic acid injection: Limited evidence in ankle (better for knee)
- PRP injection: Emerging - insufficient evidence currently
- Bracing: Arizona brace or similar to limit motion
Indications for surgery:
- Failed 6+ months comprehensive conservative management
- Pain limiting activities of daily living
- Unable to work or perform desired activities
- Patient willing to accept surgical risks and rehabilitation
Conservative management rarely reverses ankle OA - buys time for appropriate surgical candidate.
Conservative management appropriate for: (1) Early OA, (2) Medical contraindications to surgery, (3) Patient preference to delay surgery, (4) Optimization before definitive procedure.
Indications and Contraindications
Primary Indications for TAA
| Indication | Patient Characteristics | Expected Outcome |
|---|---|---|
| Symptomatic post-traumatic OA | Age 40-60, failed conservative management, disability | Pain relief, motion preservation, return to moderate activity |
| Primary ankle OA | Age over 50, low-moderate demand, good bone stock | Excellent pain relief, maintain independent gait |
| Inflammatory arthritis | RA, PsA with controlled disease, bilateral involvement | Pain relief superior to fusion, protect adjacent joints |
| Failed ankle arthrodesis | Nonunion or malunion of previous fusion, adequate bone stock | Restoration of motion, adjacent joint protection |
Best candidate profile: Age 55, BMI 26, unilateral post-traumatic OA, sedentary-moderate activity, neutral alignment, intact ligaments, good bone stock, non-smoker, compliant, realistic expectations.
Primary indication is end-stage ankle arthritis in appropriate candidate who has failed extensive conservative management.
Surgical Technique
Alignment is everything: Neutral mechanical axis (tibiotalar angle 90° ± 3°) is mandatory. Varus/valgus malalignment over 5° doubles failure risk. Use navigation or intraoperative fluoroscopy to confirm neutral axis before final implantation. Ligament balancing essential - if unstable to varus stress, reconstruct lateral ligaments; if valgus unstable, address deltoid competence. Bone preservation critical for potential revision or conversion to fusion.
Surgical Planning Essentials
- Infection: 2% deep infection requiring debridement ± component removal
- Wound complications: 10% superficial, 3% deep requiring flap coverage
- Nerve injury: Superficial peroneal nerve 5%, deep peroneal nerve 2%
- Aseptic loosening: 8% at 10 years, may require revision
- Subsidence: 5%, often asymptomatic but can lead to instability
- Periprosthetic fracture: 3% (tibia, talus, or malleoli)
- Persistent pain: 10-15% not satisfied with pain relief
- Conversion to fusion: 15% at 10 years - bone loss complicates fusion
- Heterotopic ossification: 20% but rarely symptomatic
- DVT/PE: 2-3% despite prophylaxis
- Implant system: STAR, Infinity, Cadence, or INBONE (surgeon preference)
- Sizing: Templated on AP and lateral radiographs
- Cutting guides: System-specific jigs for bone preparation
- Power tools: Oscillating saw, drill for peg holes
- Fluoroscopy: C-arm positioned for AP and lateral ankle views
- Retractors: Self-retaining ankle distractor, Hohmann retractors
- Trial components: Full set for intraoperative sizing
- Backup plan: Ankle arthrodesis implants available if TAA aborted
Preoperative Optimization
- Smoking cessation: Mandatory minimum 6 weeks
- Weight loss: Target BMI under 30 if elevated
- Diabetes control: HbA1c under 7.5%
- Vascular assessment: ABI if PVD suspected
- Dental clearance: Address any oral infection
- Supramalleolar osteotomy: For varus/valgus deformity correction
- Lateral ligament reconstruction: For chronic lateral instability
- Deltoid repair/reconstruction: For valgus instability
- Hindfoot fusion: For subtalar or talonavicular arthritis
Allow full healing and rehabilitation before proceeding with TAA.
- 3D CT analysis: Confirm bone stock, plan bone cuts
- Component sizing: Template tibial and talar components
- Approach planning: Review previous incisions, soft tissue
- Anesthesia: Regional vs general with nerve block
- VTE prophylaxis: Plan for mechanical and pharmacological
Comprehensive preoperative planning is foundation for successful TAA outcome.
Complications
Total ankle arthroplasty complication rates are significantly higher than total hip or knee replacement. Overall complication rate 30-40%, reoperation rate 20-25%, revision rate 15% at 10 years. Wound complications most common (10%), followed by aseptic loosening (8%), subsidence (5%), periprosthetic fracture (3%), and infection (2%). Patient selection and technical precision critical for minimizing complications.
| Complication | Incidence | Risk Factors | Management |
|---|---|---|---|
| Wound dehiscence/infection | 10% superficial, 2% deep | Smoking, diabetes, obesity, prior surgery | Superficial: dressings, antibiotics. Deep: debridement ± flap, component removal if infected |
| Aseptic loosening | 8% at 10 years | Malalignment, obesity, high activity | Revision TAA if adequate bone stock, fusion if severe bone loss |
| Subsidence | 5% (talar more common) | Osteoporosis, overcorrection, undersized component | Often asymptomatic if under 2mm. If over 5mm, revision may be required |
| Periprosthetic fracture | 3% (tibia, talus, malleoli) | Trauma, osteoporosis, oversized component | ORIF if fracture stable, revision if component loose |
| Nerve injury | 5% superficial peroneal, 2% deep peroneal | Excessive retraction, direct injury | Superficial: observation (usually recovers). Deep: may require tendon transfer if foot drop |
| Persistent pain | 10-15% not satisfied | Malalignment, adjacent joint arthritis, component loosening | Investigate source: injections, further imaging, consider revision or fusion |
| Heterotopic ossification | 20% | Extensive soft tissue dissection | Usually asymptomatic; excision if limits ROM significantly |
| Periprosthetic cyst formation | 40% on CT | Polyethylene wear debris, stress shielding | Monitor with serial CT; revise if expanding or symptomatic |
Immediate Postoperative Period
| Complication | Presentation | Prevention | Treatment |
|---|---|---|---|
| Wound dehiscence | Wound breakdown 2-3 weeks | Meticulous closure, elevation, minimize tension | Local wound care, VAC therapy, delayed closure or flap if large |
| Deep infection | Fever, drainage, pain, wound erythema | Prophylactic antibiotics, sterile technique | Debridement, IV antibiotics, component removal if organism virulent |
| DVT/PE | Leg swelling, chest pain, dyspnea | Mechanical and pharmacological prophylaxis | Anticoagulation per protocol, IVC filter if recurrent |
| Compartment syndrome | Severe pain, swelling, neurologic deficit (rare) | Avoid tight dressings, monitor perfusion | Emergency fasciotomy - high suspicion required |
Early complications require prompt recognition and aggressive management to salvage reconstruction.
Postoperative Care and Rehabilitation
Hospital and Early Home Phase
Immediate Postop Protocol
- Pain control: Multimodal analgesia (nerve block, IV/oral opioids, NSAIDs)
- Elevation: Strict elevation above heart level continuously
- Ice: Cryotherapy to reduce swelling
- Splint: Posterior slab in neutral position, well-padded
- Weight-bearing: Non-weight-bearing on affected limb
- DVT prophylaxis: Mechanical (compression stockings) and pharmacological (LMWH)
- Wound check: Inspect for excessive drainage or hematoma
- Mobilization: Wheelchair or crutches, no weight on operative leg
- Elevation: Continue strict elevation - leg up when sitting/lying
- Splint: Maintain posterior slab, do not remove at home
- Weight-bearing: Non-weight-bearing with crutches or walker
- Wound care: Keep splint and dressing dry, no bathing (sponge bath only)
- Pain management: Wean opioids, continue NSAIDs
- Prophylaxis: LMWH for 14 days total
- Watch for: Fever, increasing pain, excessive swelling, drainage
- Wound assessment: Remove splint and dressing, inspect incision
- Suture removal: If non-absorbable sutures used (typically 14 days)
- Radiographs: AP and lateral ankle to assess component position
- Transition to boot: CAM walker boot with ankle in neutral position
- Weight-bearing: Remain non-weight-bearing for another 4 weeks
- Exercises: Begin gentle ankle ROM in boot (dorsi/plantarflexion only)
Early weight-bearing before osseointegration can lead to component subsidence or loosening. Patients must remain completely non-weight-bearing for minimum 6 weeks postoperatively. Use of walker or crutches mandatory - no cheating with "touch weight-bearing" allowed.
Immediate postoperative period is critical for wound healing and early osseointegration - patient compliance essential.
Outcomes and Prognosis
| Outcome Measure | Total Ankle Arthroplasty | Ankle Arthrodesis | Significance |
|---|---|---|---|
| 10-year survival | 90% (modern implants) | 95% (fusion rate) | Fusion slightly more reliable but TAA improving |
| Revision rate | 15% at 10 years | 8% at 10 years | TAA requires more reoperations |
| Pain relief | 85% good-excellent | 90% good-excellent | Both effective for pain - similar outcomes |
| Range of motion | 30° arc preserved | 0° (fused) | TAA clear advantage for motion preservation |
| Gait biomechanics | Near-normal gait pattern | Altered - compensatory midfoot motion | TAA superior for gait |
| Adjacent joint degeneration | Reduced risk vs fusion | Accelerated subtalar/midfoot OA | TAA protective of adjacent joints |
| Return to activity | Low-moderate impact allowed | Can return to heavy labor | Fusion allows higher demands |
| Patient satisfaction | 85% satisfied | 80% satisfied | Similar satisfaction rates |
TARVA (Total Ankle Replacement Versus Arthrodesis) is the landmark multicentre RCT (Goldberg AJ et al, Ann Intern Med 2022): 303 patients (152 TAR, 151 fusion) across 17 UK NHS centres, aged 50-85 with end-stage ankle OA. Primary outcome was change in the Manchester-Oxford Foot Questionnaire (MOXFQ) walking/standing domain at 52 weeks. Both treatments improved significantly; the adjusted difference of -5.6 (95% CI -12.5 to 1.4) favoured TAR but was neither clinically nor statistically significant. Adverse-event totals were similar, but TAR had more wound-healing and nerve complications while fusion had more thromboembolism and nonunion (symptomatic nonunion 7%). A pre-specified post hoc analysis suggested fixed-bearing TAR was superior to fusion (-11.1, 95% CI -19.3 to -2.9). Bottom line: at 1 year both procedures are safe and effective with no clear winner, so the decision is individualised.
Factors Associated with Success
| Factor | Favorable Feature | Why It Predicts Success |
|---|---|---|
| Age | 50-65 years | Lower activity demands, adequate bone quality, reasonable lifespan expectation |
| BMI | Under 28 | Reduced implant stress, lower wound complication risk |
| Etiology | Primary or post-traumatic OA | Predictable bone quality, less systemic involvement |
| Alignment | Neutral or under 5° deformity | Balanced loading, no edge wear |
| Ligament stability | Intact or reconstructible | Prevents instability and component tilt |
| Bone stock | Good quality tibia and talus | Adequate fixation and osseointegration |
| Surgeon experience | Over 20 cases annually | Improved alignment, fewer technical errors |
| Implant design | Third-generation mobile-bearing | Proven longevity and low complication rate |
Ideal candidate: 55-year-old with BMI 26, primary OA, neutral alignment, intact ligaments, good bone stock, operated by experienced surgeon using proven implant.
Evidence Base and Key Studies
TARVA Trial: Total Ankle Replacement vs Arthrodesis (Landmark RCT)
- Multicentre, parallel-group, open-label RCT: 303 patients (152 TAR, 151 fusion) across 17 UK NHS trusts, age 50-85, end-stage ankle OA
- Primary outcome (change in MOXFQ walking/standing at 52 weeks): adjusted difference -5.6 (95% CI -12.5 to 1.4) favouring TAR but not clinically or statistically significant
- Both treatments significantly improved MOXFQ-W/S from baseline; total adverse events similar (109 vs 104)
- TAR: more wound-healing complications and nerve injuries; fusion: more thromboembolism and nonunion (symptomatic nonunion rate 7%)
- Post hoc analysis suggested superiority of fixed-bearing TAR over fusion (-11.1, 95% CI -19.3 to -2.9)
- Companion HTA modelling estimated ~69% probability TAR is cost-effective vs fusion at the NICE 20,000 GBP/QALY threshold
STAR Pivotal Trial: Mobile-Bearing TAR vs Fusion (Non-Inferiority)
- Prospective controlled multicentre non-inferiority study (FDA pivotal): 158 STAR ankle replacements vs 66 ankle fusion controls, plus 448 continued-access STAR cases
- Non-inferiority hypothesis for overall patient success was met for STAR vs fusion at 24 months
- Treatment efficacy higher in the replacement group due to improvement in functional scores; pain relief equivalent between groups
- Major complications and secondary surgical interventions more common in the pivotal arthroplasty group than fusion
- Secondary procedures roughly halved in the continued-access group versus the pivotal arthroplasty group (learning-curve effect)
National Joint Registry: Risk Factors for Failure of Ankle Replacement
- Data-linkage study: National Joint Registry (England & Wales) combined with NHS Digital; failure defined as removal or exchange of any component
- Overall 5-year survival 90.2% (95% CI 89.2-91.1%)
- Younger age (HR 0.96 per year) and higher BMI (HR 1.03 per unit) independently associated with increased risk of failure
- Patients with rheumatoid arthritis had higher survivorship than those with osteoarthritis (etiology HR 0.88)
Norwegian Arthroplasty Register: Long-Term TAR Survival
- Registry study: 257 primary ankle replacements in Norway 1994-2005 (212 cementless STAR, 32 cemented TPR)
- Overall survival 89% at 5 years and 76% at 10 years
- No significant effect of age, sex, prosthesis type, diagnosis or year of operation on revision risk
- Revision rate acceptable versus other ankle series but high compared with knee and hip arthroplasty
- Incidence of ankle replacement for osteoarthritis increased over the study period
National Joint Registries: Real-World TAR Revision (Registry Evidence)
- Major joint registries (AOANJRR Australia, NJR England & Wales, Nordic registries) all report higher cumulative revision for ankle replacement than for hip or knee arthroplasty
- NJR/NHS Digital linkage data: ~90% 5-year survival of primary TAR (Jennison 2023)
- Aseptic loosening, subsidence and instability are consistently the leading revision indications across registries
- Use of ankle replacement is rising internationally, though fusion remains the more frequently performed procedure
- Revision-specific modular implants show better survival than primary implants used at revision (Jennison 2023, BJJ)
Survival of Revision Ankle Arthroplasty (NJR Data-Linkage)
- National Joint Registry and NHS Digital linkage: 228 patients undergoing revision TAA, mean follow-up 2.6 years
- Survival 95.4% at 1 year, 87.7% at 3 years and 77.5% at 5 years
- Failures: of 29 (12.7%) that failed, 19 (8.3%) were converted to fusion, 9 (3.9%) re-revised and 1 amputation
- Revision-specific (modular) implants survived better than primary implants used at revision
- Use of cement was a risk factor for failure (HR 3.02, 95% CI 1.13-8.09)
Long-Term Gait Analysis After TAA (Mean 7.6 Years)
- Prospective 3-dimensional gait analysis in 33 patients (28 STAR, 5 Salto Talaris), preoperative versus minimum 5-year (mean 7.6, range 5-13 years) follow-up
- Sustained, significant improvements in cadence (+9.5 steps/min), step length (+4.4 cm) and walking speed (+0.2 m/s)
- Total sagittal range of motion increased (+2.0 degrees) with increased plantarflexion at initial contact and maximum plantarflexion
- No loss of peak ankle power despite patients ageing - first study to report objective gait outcomes beyond 5 years
- Demonstrates durable functional benefit of motion-preserving TAA on objective gait parameters
Population Comparison of Reoperation: TAA vs Ankle Arthrodesis
- Population-based study of all California inpatient admissions 1995-2004: 4705 ankle fusions vs 480 ankle replacements
- Major revision rate after replacement: 9% at 1 year and 23% at 5 years, versus 5% and 11% after fusion
- Higher risk of major revision with replacement (HR 1.93, 95% CI 1.50-2.49)
- Lower risk of subsequent subtalar fusion after replacement (0.7% vs 2.8% at 5 years; HR 0.28, 95% CI 0.09-0.87)
- Replacement also associated with higher risk of device-related infection
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old office worker presents with severe ankle pain limiting walking to 200 meters. She has end-stage post-traumatic ankle OA following a pilon fracture 10 years ago. BMI 28. Radiographs show maintained coronal alignment, tibiotalar angle 92°, no talar AVN. She wants to preserve motion for walking and light recreational activities. How do you assess and manage?”
“You are performing a primary total ankle arthroplasty using a mobile-bearing 3-component system. Walk me through the key surgical steps from approach to implantation, highlighting critical technical points for achieving optimal alignment and avoiding complications.”
“A 58-year-old patient is 18 months post-TAA and develops progressive medial ankle pain and swelling over 3 months. Radiographs show 3mm of talar component subsidence and a 12mm medial talar cyst. How do you assess and manage this complication?”
MCQ Practice Points
Q: What is the primary blood supply to the talar body that is at risk during TAA? A: The talar body is supplied chiefly by the artery of the tarsal canal (a branch of the posterior tibial artery), supplemented by the artery of the tarsal sinus (from the perforating peroneal and dorsalis pedis arteries) and deltoid branches medially. The talus has no muscular attachments and relies entirely on this peri-talar arterial supply entering at the neck and medially. Extensive anterior dissection during TAA can compromise it and lead to avascular necrosis, so soft-tissue attachments to the talar neck should be preserved. (The medial circumflex femoral artery supplies the femoral head, not the talus - a classic exam trap.)
Q: What is the biomechanical advantage of mobile-bearing (3-component) TAA designs over fixed-bearing (2-component) designs? A: Mobile-bearing designs include a mobile polyethylene insert that can translate anteroposteriorly and rotate slightly, reducing constraint and edge loading on the metal components. This decreases stress at the bone-implant interface, reducing loosening rates. Fixed-bearing designs constrain motion, leading to higher stresses and earlier failure. Registry data shows 92% survival at 10 years for mobile-bearing vs 81% for fixed-bearing designs.
Q: A 38-year-old construction worker with post-traumatic ankle OA and 12° varus deformity requests TAA because he wants to avoid fusion. How do you counsel him? A: This patient has multiple relative contraindications for TAA: (1) Young age (under 40) - higher activity demands and longer lifespan requirement exceed implant durability, (2) Heavy labor occupation - TAA incompatible with construction work (high-impact loading leads to early failure), (3) Varus deformity 12° - may require staged supramalleolar osteotomy and still have edge loading risk. I would counsel that ankle arthrodesis is better option for this patient profile - allows return to heavy labor, more predictable long-term outcome, lower revision rate (8% vs 15% at 10 years). If patient insists on TAA, counsel about very high likelihood of early failure requiring revision or conversion to fusion.
Q: During TAA, you achieve good alignment on fluoroscopy but when you trial the components, the ankle is unstable to valgus stress. What is the likely cause and how do you manage? A: Valgus instability suggests deltoid ligament incompetence. This is a critical finding - proceeding with TAA in presence of medial-sided instability leads to valgus tilt, medial edge loading, and early component loosening or subsidence. Management options: (1) Deltoid ligament repair if tissue quality adequate - advance deltoid to medial malleolus with suture anchors, (2) Deltoid reconstruction using allograft or autograft if native tissue insufficient, or (3) Abort TAA and perform ankle arthrodesis if deltoid is non-reconstructible. Never proceed with unstable TAA - ensure stability with varus and valgus stress testing before final component implantation.
Q: What is the most common cause of TAA failure requiring revision? A: Aseptic loosening (40% of failures in AOANJRR data), followed by subsidence (25%), instability (20%), and infection (10%). Aseptic loosening results from micromotion at the bone-implant interface due to malalignment (varus/valgus tilt causes edge loading), polyethylene wear debris (induces osteolysis), or inadequate osseointegration (poor bone quality, premature loading). Prevention: meticulous attention to neutral alignment (tibiotalar angle 90° ± 3°), appropriate patient selection (good bone stock, BMI under 30), strict 6-week non-weight-bearing protocol, and lifelong activity restrictions.
Q: What were the key findings of the TARVA trial comparing TAR to ankle arthrodesis? A: TARVA (Goldberg AJ et al, Ann Intern Med 2022) was the first adequately powered multicentre RCT (Level 1 evidence): 303 patients aged 50-85 randomised to total ankle replacement or fusion across 17 UK NHS centres. Key findings: (1) Primary outcome (change in MOXFQ walking/standing at 52 weeks) showed no clinically or statistically significant difference (adjusted difference -5.6, 95% CI -12.5 to 1.4), with both arms improving from baseline; (2) Similar total adverse events, but TAR had more wound-healing and nerve complications and fusion had more thromboembolism and nonunion (symptomatic nonunion 7%); (3) a post hoc analysis suggested fixed-bearing TAR was superior to fusion (-11.1, 95% CI -19.3 to -2.9); (4) companion economic modelling estimated TAR is likely cost-effective at the NICE threshold. Conclusion: both treatments are safe and effective at 1 year - the choice is patient-specific. (Note: the initial report was 52-week data; longer-term survival is captured by registries such as the NJR.)
Guidelines, Registries & Global Practice
End-stage ankle OA is predominantly post-traumatic (unlike hip/knee, which are mostly primary OA), affects a younger population, and is treated by either motion-preserving total ankle replacement (TAR) or arthrodesis. The landmark TARVA RCT found no clear superiority of either at 1 year; national registries worldwide show modern TAR has acceptable mid-term survival but is revised more often than hip or knee replacement.
Global Epidemiology
| Parameter | Figure | Source / Note |
|---|---|---|
| Dominant aetiology | Post-traumatic in the majority (vs primary OA in hip/knee) | Reflected in TAA cohorts; younger, often unilateral |
| Typical age at surgery (TARVA cohort) | Mean ~68 years, 71% male | Goldberg AJ et al, Ann Intern Med 2022 (PMID 36375147) |
| TAR 5-year survival (registry) | ~90% (NJR England & Wales) | Jennison T et al, Foot Ankle Int 2023 (PMID 37345846) |
| TAR 10-year survival (early registry era) | 76% (5-yr 89%) | Fevang BT et al, Acta Orthop 2007 (PMID 17966015) |
| Trend | Rising TAR utilisation internationally; fusion still common | Multiple national registries |
Guidelines & Registry Evidence, Side by Side
| Body / Registry (region) | Position on TAR vs fusion | Evidence level / basis |
|---|---|---|
| NICE / NIHR HTA (UK) | Both TAR and fusion are effective; TARVA showed no significant difference at 1 year and TAR likely cost-effective at the 20,000 GBP/QALY threshold | Level 1 RCT (TARVA) + economic modelling |
| BOA / BOFAS (UK) | Supports TAR as an established option in appropriately selected patients; emphasises shared decision-making and surgeon/unit volume | Society consensus + NJR registry |
| US FDA / AOFAS-era evidence | Mobile-bearing STAR approved on non-inferiority to fusion (pivotal trial); TAR endorsed for selected end-stage OA | Level 2 controlled trial (STAR pivotal, PMID 19589303) |
| AOANJRR (Australia) | Reports real-world TAR revision higher than hip/knee; tracks implant-specific survival to guide selection | Registry evidence (annual reports) |
| Nordic registries (Norway/Sweden/Finland) | Long-standing data showing TAR survival below hip/knee but improving with newer designs | Registry evidence (e.g. Fevang 2007) |
Practice Variation
- TAR vs fusion ratio: varies markedly by country and unit; fusion remains commoner overall but TAR use is rising in high-resource settings
- Implant availability: mobile-bearing designs (e.g. STAR) widely used outside the US; fixed-bearing designs (e.g. INBONE, Infinity, Cadence) predominate in the US for historical regulatory reasons
- Centralisation: several systems concentrate TAR in higher-volume foot-and-ankle units, reflecting a registry-supported volume-outcome relationship
- Limited-resource settings: arthrodesis often preferred for reliability, lower implant cost and tolerance of heavier physical demands
- No clear winner at 1 year (TARVA): discuss TAR and fusion as genuine alternatives
- Differing complication profiles: TAR - more wound-healing/nerve issues; fusion - more VTE and nonunion (symptomatic nonunion ~7%)
- TAR is not a lifetime solution: counsel on revision risk and on conversion to fusion as the commonest salvage
- Lifelong activity modification after TAR: no running, jumping, contact sport or heavy labour
- Modifiable risk: smoking cessation and BMI optimisation before surgery (higher BMI predicts failure - PMID 37345846)
- Antibiotic prophylaxis: single dose within 60 minutes of incision (cefazolin, or a glycopeptide such as vancomycin/teicoplanin if beta-lactam allergy or MRSA risk); intra-operative redosing for prolonged surgery; routine prophylaxis limited to 24 hours.
- VTE prophylaxis: combined mechanical and pharmacological prophylaxis individualised to risk, per local/society guidance.
- Tourniquet: minimises blood loss so cell salvage is generally unnecessary.
- Surveillance: serial weight-bearing radiographs to detect subsidence, lucency and periprosthetic cysts; CT for problem-solving.
Patient Selection (STABLE)
- Stock (bone): Adequate tibia/talus quality, no AVN
- Ties (ligaments): Competent or reconstructible medial/lateral ligaments
- Alignment: Coronal under 10°, sagittal under 15° (or correctable)
- BMI under 30: Obesity increases failure risk
- Low-moderate demand: Sedentary to moderate activity only
- Etiology favorable: Primary or post-traumatic OA (not AVN or severe bone loss)
Contraindications (INFECTIONS)
- Infection active, Neuropathy severe, Failure of bone stock
- Extreme deformity (over 20°), Circulation inadequate
- Talus absent/destroyed, Instability uncorrectable
- Ongoing smoking, Non-compliance, Skin coverage poor
Surgical Technique Essentials
- Anterior approach: Between TA and EHL, protect neurovascular bundle laterally
- Neutral alignment: Tibiotalar 90° ± 3° - varus/valgus error leads to edge loading
- Bone preservation: Minimize resection (tibia 5-8mm, talus 3-5mm)
- Trial before implant: Assess ROM, stability, alignment
- Soft tissue balance: Deltoid release for varus, lateral reconstruction for valgus
- Postop: Strict non-weight-bearing 6 weeks, then progressive in boot
Implant Designs
- Third-generation mobile-bearing: Current standard (90% survival at 10 years)
- 3-component: Tibial, talar, mobile polyethylene insert
- Mobile bearing advantage: Reduces constraint and edge loading vs fixed-bearing
- Common implants: STAR, Infinity, Cadence (surgeon familiarity important)
Complications
- Wound complications 10% (superficial) + 2% (deep infection)
- Aseptic loosening 8% at 10 years (most common failure mode)
- Subsidence 5% (talar more common) - revise if over 5mm
- Periprosthetic cysts 40% (often asymptomatic - monitor with CT)
- Nerve injury 5% (superficial peroneal) + 2% (deep peroneal)
- Conversion to fusion 15% at 10 years (80% successful but bone loss complicates)