Anterolateral Complex of the Knee
- The ANTEROLATERAL LIGAMENT (ALL) and the wider anterolateral complex - which includes the iliotibial band and its deep Kaplan fibre attachments to the distal femur - act as SECONDARY restraints to INTERNAL ROTATION of the tibia, controlling the anterolateral rotatory instability that is clinically detected as the PIVOT SHIFT; they work alongside the ACL, which is the primary restraint to anterior translation.
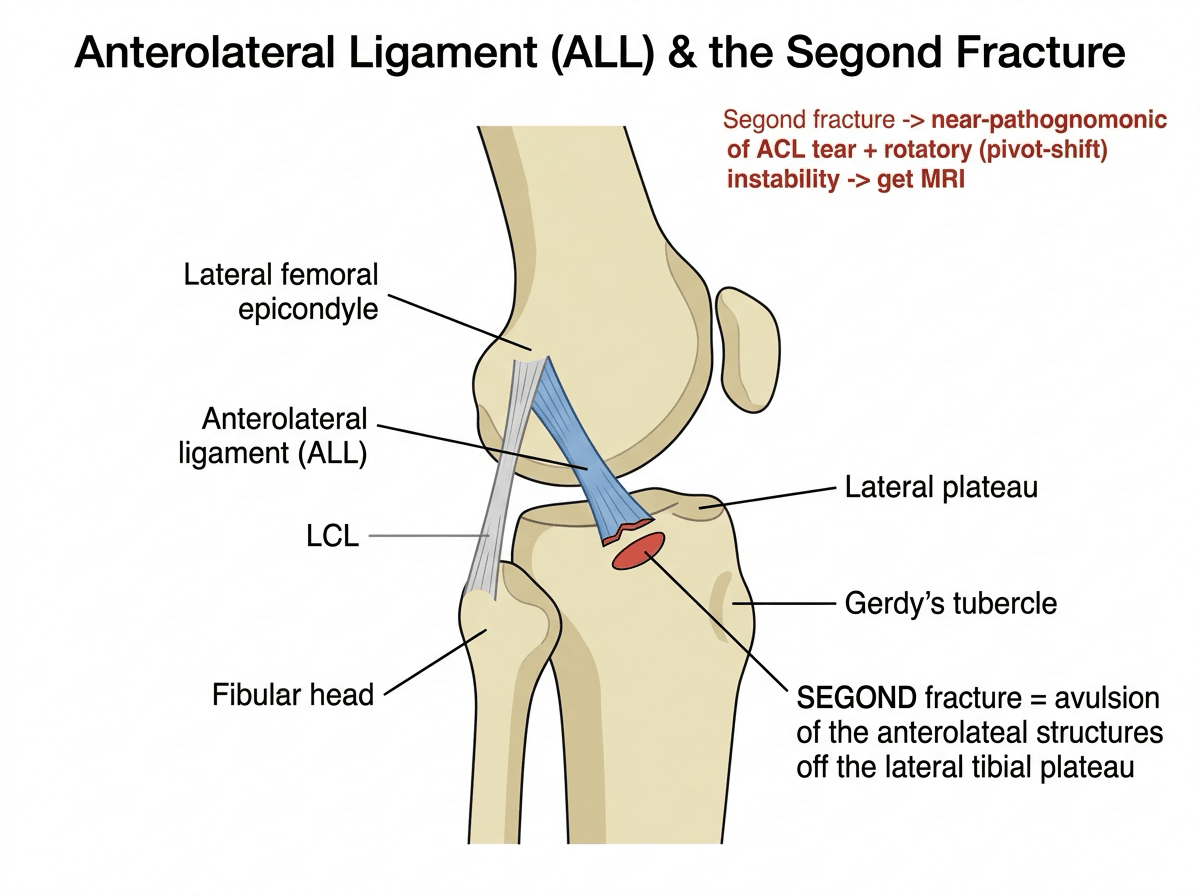
- The SEGOND FRACTURE is the radiographic signature of anterolateral injury: a small elliptical bony AVULSION off the LATERAL margin of the proximal tibial plateau (a lateral capsular/anterolateral structure avulsion), and it is near-pathognomonic of an ACL tear - so a Segond fracture on a knee radiograph should prompt MRI and careful assessment of rotatory stability.
- After ACL reconstruction, residual ANTEROLATERAL ROTATORY INSTABILITY (a persistent pivot shift) and graft failure are problems particularly in HIGH-RISK patients, which is the rationale for adding an EXTRA-ARTICULAR procedure - either a LATERAL EXTRA-ARTICULAR TENODESIS (LET) or an ANTEROLATERAL LIGAMENT RECONSTRUCTION - to the intra-articular ACL graft to better control the pivot shift.
- The INDICATIONS for adding LET/ALL reconstruction to ACLR are high-risk features: young age (under about 25), generalised LIGAMENTOUS LAXITY/hyperlaxity, a high-grade (grade 2 or greater) PIVOT SHIFT, REVISION ACL reconstruction or previous graft failure, elite athletes in CUTTING/PIVOTING sports, and an increased posterior TIBIAL SLOPE.
- The EVIDENCE is strong: in the STABILITY randomised controlled trial, adding LET to a hamstring-autograft ACL reconstruction reduced clinical failure from about 40% to 25% and graft rupture from about 11% to 4% at 2 years, with similar return-to-sport rates; meta-analyses confirm reduced graft failure and reduced postoperative anterolateral rotatory instability with the addition of an extra-articular procedure.
- TECHNIQUE (LET, modified Lemaire): a strip of the iliotibial band is harvested (left attached distally at Gerdy's tubercle), passed DEEP to the lateral collateral ligament, and fixed to the distal femur approximately proximal-and-posterior to the lateral epicondyle with the knee around 60 degrees of flexion in neutral rotation; the iliotibial band is then repaired - the downsides are reported to be minimal, though long-term osteoarthritis is being monitored.
- “Anterolateral complex (ALL + IT band/Kaplan fibres) = secondary restraint to internal rotation -> controls the PIVOT SHIFT (works with the ACL).
- “SEGOND fracture = lateral tibial plateau avulsion = near-pathognomonic of ACL/anterolateral injury -> MRI + assess rotatory stability.
- “Add LET (modified Lemaire) or ALL reconstruction to ACLR in HIGH-RISK patients (young, hyperlax, high-grade pivot, revision, pivoting athletes, steep slope). STABILITY trial: clinical failure 40%->25%, graft rupture 11%->4%.
The anterolateral complex (ALL + IT band/Kaplan fibres) restrains internal rotation - the pivot shift. A Segond fracture is its avulsion signature (and a marker of ACL injury).
Add LET (modified Lemaire) or ALL reconstruction to ACLR in high-risk patients - the STABILITY trial showed less graft failure and clinical failure.
Overview and Epidemiology
- The problem it answers. Isolated intra-articular ACL reconstruction leaves a subset of knees with a residual pivot shift and a graft-rupture rate that is unacceptable in young pivoting athletes. The anterolateral complex is the structure that explains why, and augmenting it is the response.
- Who fails. Failure concentrates in the young (particularly under 25), those with generalised ligamentous laxity or hyperextension, revision reconstructions, soft-tissue (hamstring) grafts, high posterior tibial slope, and athletes returning to cutting and pivoting sport.
- Not a new idea. Extra-articular tenodesis was widely performed in the 1970s-80s, largely abandoned when arthroscopic intra-articular reconstruction matured, and has returned as a selective adjunct on the back of Level I evidence - a useful historical arc for a viva.
- The Segond fracture is the visible epidemiological marker: uncommon, but when present it is near-pathognomonic of ACL rupture and signals anterolateral injury.
Anatomy, the Segond Fracture & the Pivot Shift
The anterolateral ligament and the anterolateral complex (the iliotibial band with its deep Kaplan fibres) are secondary restraints to internal rotation of the tibia, controlling the anterolateral rotatory instability detected as the pivot shift - they work with the ACL (the primary restraint to anterior translation). The radiographic signature of anterolateral injury is the Segond fracture: a small elliptical avulsion off the lateral tibial plateau margin, near-pathognomonic of an ACL tear, which should prompt MRI and assessment of rotatory stability. Because residual pivot shift and graft failure remain problems after ACL reconstruction - especially in high-risk patients - an extra-articular procedure (LET or ALL reconstruction) is added to better control the pivot shift.
Augmentation: LET & ALL Reconstruction
- Indications (high-risk): young age (under ~25), generalised ligamentous laxity, high-grade (grade 2+) pivot shift, revision ACLR or previous graft failure, elite cutting/pivoting athletes, and increased posterior tibial slope.
- LET (modified Lemaire): harvest a strip of iliotibial band (left attached distally at Gerdy's tubercle), pass it deep to the LCL, and fix it to the distal femur ~proximal-and-posterior to the lateral epicondyle with the knee at ~60 degrees flexion in neutral rotation; repair the IT band.
- ALL reconstruction: an anatomic graft reconstruction of the anterolateral ligament is an alternative extra-articular augment.
- Evidence: the STABILITY RCT showed LET reduced clinical failure (about 40% to 25%) and graft rupture (about 11% to 4%) at 2 years; avoid isolated soft-tissue grafts in high-risk patients - add an extra-articular procedure.
The key modern lesson in ACL surgery is that, in high-risk knees, controlling the anterolateral rotatory instability - the pivot shift - is as important as restoring anterior translation, because a residual pivot shift and graft failure are concentrated in young, hyperlax patients, those with a high-grade pivot, revisions and pivoting athletes. In these patients an isolated intra-articular ACL graft, especially a soft-tissue graft, is more likely to fail, and adding an extra-articular procedure - LET or ALL reconstruction - significantly reduces graft failure and clinical failure (STABILITY trial). A Segond fracture is a useful flag that the anterolateral complex is involved. The downsides of LET appear minimal, but long-term osteoarthritis should be monitored, so reserve the augment for the genuinely high-risk patient rather than applying it indiscriminately.
The Pivot-Shift Test: Performing and Grading It
The pivot shift is the clinical metric that selects a knee for an extra-articular augment, so it has to be elicited and graded properly:
- How to perform it: with the knee in extension, apply a valgus force and internal rotation with a gentle axial load, then slowly flex the knee. In a positive test the anterolaterally subluxed lateral tibial plateau (held subluxed in extension by the deficient ACL) reduces with a palpable/visible clunk at around 20 to 30 degrees of flexion, as the iliotibial band converts from an extensor to a flexor and pulls the plateau back. (The Jerk test is the same phenomenon elicited from flexion into extension.)
- How to grade it (IKDC): grade 0 = none (symmetrical with the other side); grade 1 = a smooth glide; grade 2 = a clunk; grade 3 = gross subluxation with transient locking/impingement.
- Examine under anaesthesia where possible - guarding abolishes a subtle shift in the awake patient. The pivot shift is the clinical correlate of anterolateral rotatory instability, and a high-grade (grade 2 or greater) shift is exactly the feature that selects a knee for an added extra-articular procedure. (The wider knee-ligament examination is covered in our ACL Injuries topic.)
Pivot shift: extension → valgus + internal rotation + axial load → flex; the subluxed lateral plateau reduces with a clunk at 20 to 30 degrees (IT band flips extensor-to-flexor). Grade 0 none, 1 glide, 2 clunk, 3 gross/transient lock - grade 2 or greater (best confirmed under anaesthesia) is the high-risk feature that selects for LET.
The ALL Itself: Anatomy and the 'Is It a Ligament?' Debate
- Described course of the ALL: it arises from the lateral femoral epicondyle region (just proximal-and-posterior to the LCL origin, near the IT-band/Kaplan-fibre attachment), runs anterodistally (with an attachment to the periphery of the lateral meniscus in many descriptions), and inserts on the anterolateral proximal tibia roughly midway between Gerdy's tubercle and the fibular head, about 5 to 10 mm below the joint line - which is precisely the Segond avulsion site, so the Segond fragment is the bony avulsion of this insertion (the fracture itself is covered in our Segond Fractures topic).
- The Kaplan fibres: the deep IT-band attachments to the distal lateral (supracondylar) femur - a key anterolateral rotatory restraint that complements the ALL, and the anatomical reason an IT-band-based LET (modified Lemaire) works.
- The controversy: whether the ALL is a discrete, consistent ligament or merely a thickening of the anterolateral capsule is still debated (it is variably identified in cadaver and imaging studies) - which is why the term "anterolateral complex" is often preferred, and why surgeons may choose an IT-band tenodesis over an "anatomic ALL reconstruction."
The ALL runs from the lateral epicondyle (proximal-posterior to the LCL) to the anterolateral tibia midway between Gerdy's tubercle and the fibular head - the Segond site (the Segond fragment = its bony avulsion). The Kaplan fibres are the deep IT-band femoral attachments. Whether the ALL is a true discrete ligament is debated, so "anterolateral complex" is the safer term.
Pathophysiology
- The mechanism is the same event as the ACL tear - a valgus, internally rotated, decelerating pivot. The anterolateral structures are loaded in internal rotation, so they fail alongside the ACL rather than in isolation. A genuinely isolated ALL injury is rare.
- What is lost. The ACL is the primary restraint to anterior translation; the anterolateral complex is a secondary restraint to internal rotation. Sectioning studies show the ALL and Kaplan fibres contribute little to translation but meaningfully to internal rotation control, especially at higher flexion angles.
- Why that produces a pivot shift. With the ACL gone, the lateral plateau subluxes anteriorly in extension. If the anterolateral restraints are also incompetent, nothing limits that rotation, so the reduction as the knee flexes becomes the palpable clunk rather than a smooth glide.
- Why an intra-articular graft may not fix it. A central graft resists translation well but has a short lever arm for rotation. An extra-articular tenodesis sits far lateral, giving a long lever arm, which is the biomechanical reason it controls rotation so effectively - and also why over-tensioning it over-constrains.
The anterolateral complex is a secondary restraint to internal rotation, not to translation. An extra-articular tenodesis works because it has a long lever arm far from the joint centre - the same reason it will over-constrain the lateral compartment if fixed too tight or in the wrong rotation.
Clinical Presentation
- History. The ACL history - a pivoting or decelerating injury, a pop, immediate haemarthrosis, giving way. What points specifically to anterolateral involvement is rotational giving way: instability on turning, cutting or pivoting rather than on straight-line activity, and often a poor response to rehabilitation alone.
- Examination. Lachman and anterior drawer confirm ACL deficiency; the pivot shift grades the rotatory component and is the number that drives the decision. Compare with the contralateral knee and grade both.
- Look for the risk phenotype, because it changes the operation: generalised laxity (Beighton score), knee hyperextension/recurvatum, and a history of contralateral ACL injury.
- In the chronic ACL-deficient knee, symptomatic rotatory instability despite rehabilitation is itself an indication to consider an anterolateral procedure at reconstruction.
Investigations
- Plain radiographs. Look specifically for the Segond fracture on the AP view - a small elliptical avulsion off the lateral tibial plateau margin. Its presence means ACL rupture until proven otherwise. Also measure the posterior tibial slope on a true lateral, because a slope above roughly 12 degrees is one of the recognised risk factors for graft failure.
- MRI. Confirms the ACL tear and associated injury (bone bruise pattern, meniscal tears, ramp lesion, posterolateral corner). The ALL itself is inconsistently visualised - a normal-looking ALL on MRI does not exclude anterolateral injury, and this uncertainty is precisely why the anatomical debate persists. Report the anterolateral complex rather than claiming a discrete ALL tear.
- Examination under anaesthesia remains the most reliable assessment of the pivot shift, because guarding abolishes a subtle shift in the clinic.
- Quantified pivot shift (accelerometer or image-analysis methods) exists largely as a research tool; it is worth naming as an attempt to make a subjective grade objective, but it is not routine practice.
Do not let imaging overrule the examination. The ALL is variably identified even in cadaveric dissection, so MRI cannot reliably confirm or exclude an "ALL tear". The decision to add an extra-articular procedure is driven by the pivot-shift grade and the patient's risk profile, not by an MRI report.
Management
Anterolateral augmentation has moved from a routine add-on, to abandoned, to a selective adjunct. An international consensus published in 2025 reached strong agreement (at or above 90%) that a lateral extra-articular procedure should be added at primary ACL reconstruction for:
- a grade 3 pivot shift
- knee hyperextension
- revision ACL reconstruction
- return to pivoting sport
- active patients 25 or under receiving a non-hamstring graft
- a grade 3 Lachman
- multiple relative risk factors coexisting
with consensus (75-89.9%) for skeletally immature patients, chronic symptomatic ACL deficiency, posterior tibial slope above 12 degrees, and a history of contralateral ACL injury.
- Non-operative management is for the ACL injury as a whole, not for the anterolateral complex in isolation: a genuinely isolated anterolateral injury is rare and does not require reconstruction on its own.
- The choice of augment. An iliotibial-band-based LET (modified Lemaire) and an anatomic ALL reconstruction are both used; comparative evidence has not established clear superiority, and the pragmatic argument for LET is that it uses local tissue and does not depend on the ALL being a discrete structure.
- Do not apply it indiscriminately. The consensus is framed around risk factors precisely because the benefit is concentrated in high-risk knees.
If asked "who gets a LET?", answer with the risk profile, not a single number: grade 3 pivot shift, hyperextension or generalised laxity, revision, pivoting sport, young patient with a soft-tissue graft, slope above 12 degrees, contralateral ACL injury - and say explicitly that coexisting risk factors strengthen the indication.
Complications
- Over-constraint of the lateral compartment. The theoretical concern: fixing the tenodesis too tight, or in internal rotation, restricts rotation and could raise lateral compartment contact pressure. Fix with the knee at around 60 degrees in neutral rotation and avoid over-tensioning.
- Lateral compartment osteoarthritis. The long-term worry that follows from over-constraint. It is the main reason the augment is reserved for high-risk knees; longer follow-up is still needed.
- Adverse events in trial data were not increased. The STABILITY randomised trial reported no increase in adverse events with LET augmentation - a reassuring and frequently examined finding.
- Local problems - lateral knee pain and irritation over the fixation, IT-band donor-site morbidity or Gerdy's tubercle discomfort, haematoma, and hardware prominence requiring removal.
- Neurovascular risk. The dissection passes near the lateral inferior geniculate vessels and, distally, the common peroneal nerve must be respected; passing the graft deep to the LCL is a technical step with its own risk.
- Stiffness and loss of terminal extension if the construct is over-tensioned or rehabilitation is delayed.
Mnemonics & Memory Aids
PIVOT
Hook:PIVOT: Pivot shift target, Internal rotation restraint, Very high-risk indications, Outcomes improved (STABILITY), Tenodesis/ALLR (Segond flag).
Pivot shift grades: 0-1-2-3
Hook:Glide, Clunk, Gross - and it is the CLUNK (grade 2) where the operation changes.
RISKY knee - who gets a LET
Hook:RISKY: the coexistence of these factors strengthens the indication more than any single one.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the anterolateral complex of the knee, and what is a Segond fracture?”
“When would you add a lateral extra-articular tenodesis to an ACL reconstruction, and what does the evidence show?”
Anatomy & function
- Anterolateral complex = ALL + IT band/Kaplan fibres
- Secondary restraint to internal rotation -> controls the pivot shift
- Works with the ACL (primary restraint to anterior translation)
Segond fracture
- Small avulsion off the lateral tibial plateau margin
- Near-pathognomonic of an ACL tear / anterolateral injury
- Prompt MRI and assessment of rotatory stability
Indications to augment ACLR
- Young (under ~25), generalised ligamentous laxity
- High-grade (grade 2+) pivot shift; revision/graft failure
- Elite cutting/pivoting athletes; increased posterior tibial slope
LET & evidence
- Modified Lemaire: IT-band strip deep to LCL, fixed proximal-posterior to lateral epicondyle (~60 deg, neutral rotation)
- ALL reconstruction is an alternative extra-articular augment
- STABILITY RCT: clinical failure 40%->25%, graft rupture 11%->4%; monitor long-term OA
Evidence & Key Studies
Lateral extra-articular tenodesis as an adjunct to ACL reconstruction (indications, technique, STABILITY data)
- LET supplements internal rotational stability and reduces the pivot shift; indications include age under 25, increased posterior tibial slope, ligamentous laxity, elite cutting/pivoting athletes, grade 2 or greater pivot shift, and prior ACL graft failure.
- In the STABILITY randomised controlled trial, adding LET to hamstring-autograft ACLR reduced 2-year clinical failure from 40% to 25% and graft rupture from 11% to 4%, with a similar return-to-sport rate.
- A meta-analysis of ACLR versus ACLR plus LET reported reduced graft failure and reduced postoperative anterolateral rotatory instability.
Extra-articular procedures (ALL reconstruction/LET) improve ACLR outcomes in high-risk patients
- Outcomes of ACL reconstruction were historically disappointing in high-risk populations (generalised ligament laxity, pivoting athletes) with low return-to-sport rates, incomplete restoration of rotatory stability and relatively high osteoarthritis rates.
- A renewed focus on extra-articular procedures (anterolateral ligament reconstruction and lateral extra-articular tenodesis) and avoiding isolated soft-tissue grafts in high-risk patients has significantly improved outcomes.
- Indications for extra-articular procedures have expanded with apparently minimal downsides, though long-term osteoarthritis should be monitored.
The role of LET (supplementing internal rotational stability/reducing pivot shift), its indications, the STABILITY-trial outcomes (clinical failure 40% to 25%, graft rupture 11% to 4%) and the supporting meta-analysis come from the cited McGovern article; the improvement in high-risk ACLR outcomes with extra-articular procedures (ALL reconstruction/LET), the avoidance of isolated soft-tissue grafts in high-risk patients and the need to monitor long-term osteoarthritis from the cited van der List commentary. The anterolateral complex anatomy, the Segond fracture and the pivot-shift mechanism are standard, well-established teaching. (See also our ACL Reconstruction and Pivot Shift / Knee Examination topics.)