Balance Thrombosis Risk | Balance Bleeding Risk | Evidence-Based Protocols
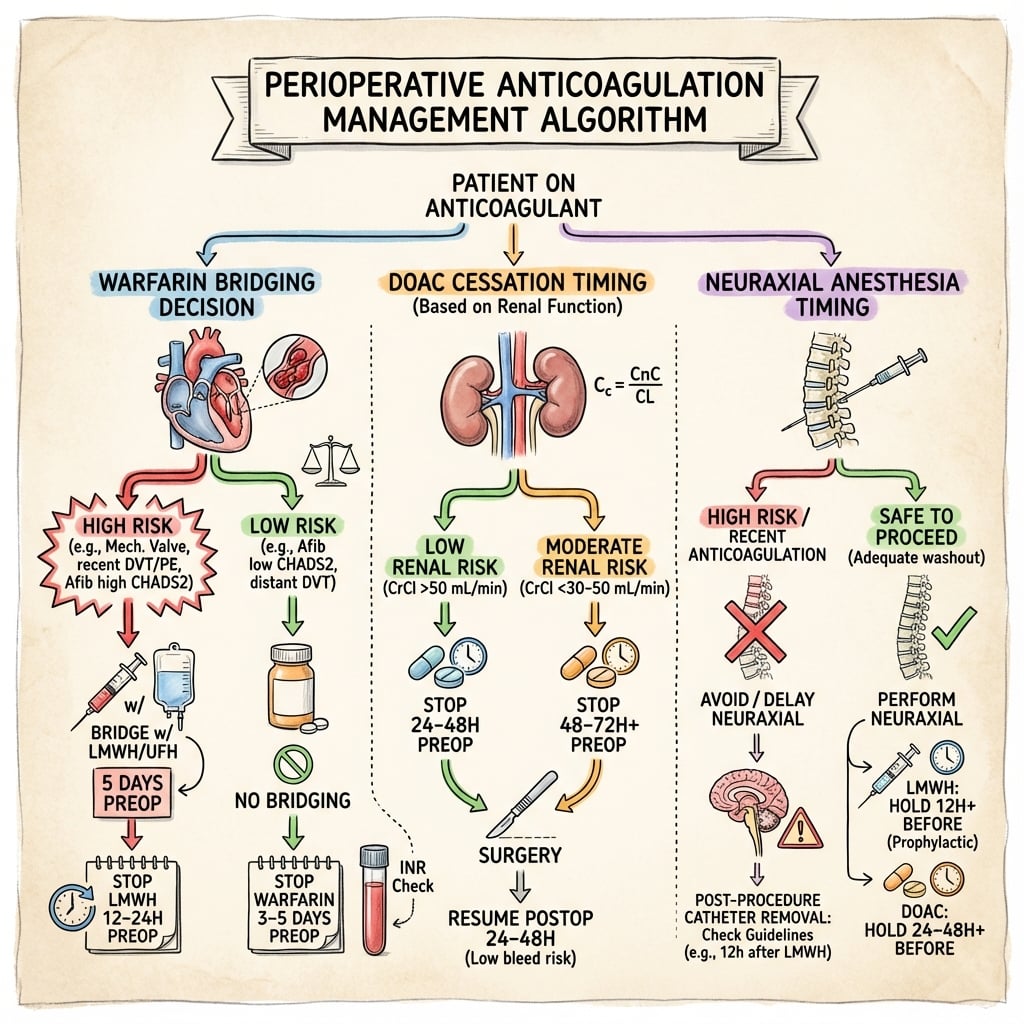
- Warfarin: stop 5 days preop, bridge if high thrombosis risk (mechanical valve, recent VTE)
- DOACs: stop 24h if CrCl greater than 50, 48h if CrCl less than 50
- Neuraxial anesthesia: 12h after LMWH prophylactic, 24h after therapeutic
- Restart anticoagulation 24-72h postop depending on bleeding risk
- Use current guideline tables for evidence-based cessation/restart protocols
- “Bridging with LMWH/UFH only for HIGH thrombosis risk patients (mechanical valve, recent VTE less than 3mo)
- “Most patients do NOT need bridging - BRIDGE trial showed bridging increases bleeding without preventing thrombosis
- “DOACs easier than warfarin - predictable offset, no bridging needed
- “Neuraxial timing critical - spinal hematoma is catastrophic complication
Only bridge HIGH thrombosis risk: mechanical mitral valve, recent VTE (less than 3 months), AF with CHA2DS2-VASc greater than or equal to 5. Bridging increases bleeding risk.
Apixaban, Rivaroxaban: 24-48h. Dabigatran: 24-96h (renal dependent). Check CrCl and use current perioperative tables.
Spinal hematoma is catastrophic. Wait 12h after prophylactic LMWH, 24h after therapeutic LMWH before neuraxial.
Low risk: 6-12h. Moderate: 24-48h. High risk (spine, revision): 48-72h. Balance VTE vs bleeding.
| Anticoagulant | Stop Before Surgery | Restart After Surgery | Bridge? |
|---|---|---|---|
| Warfarin (low thrombo risk) | 5 days preop | 24-72h postop | NO - do not bridge |
| Warfarin (high thrombo risk) | 5 days preop + LMWH bridge | LMWH 24h postop, warfarin overlap | YES - mechanical valve, recent VTE |
| DOACs (CrCl greater than 50) | 24-48h preop | 24-72h postop | NO - never bridge DOACs |
| DOACs (CrCl less than 50) | 48-96h preop (longer) | 24-72h postop | NO - never bridge DOACs |
| LMWH prophylactic | 12h before neuraxial | Restart 6-12h postop | N/A - this IS prophylaxis |
BRAVEHigh Thrombosis Risk Requiring Bridging
Hook:Be BRAVE and bridge only the highest thrombosis risk patients - most do NOT need bridging!
RENALDOAC Cessation Timing Factors
Hook:Check RENAL function before deciding DOAC cessation timing - it is the key variable!
CLOTNeuraxial Timing Safety
Hook:Prevent CLOT complications with proper neuraxial timing - spinal hematoma is catastrophic!
Overview and Clinical Significance
The BRIDGE trial (2015) changed practice. It showed that bridging with LMWH for AF patients increased bleeding (3.2% vs 1.3%) WITHOUT reducing thrombosis. Most patients do NOT need bridging. Only bridge if HIGH thrombosis risk (mechanical mitral valve, recent VTE less than 3mo).
- Atrial fibrillation (most common in ortho)
- Mechanical heart valves
- VTE treatment or prophylaxis
- Coronary stents (antiplatelet)
- Stroke prevention
- Bleeding risk with ongoing anticoagulation
- Thrombosis risk if stopped too long
- Neuraxial anesthesia contraindicated if coagulopathic
- Major surgery requires INR normalization
- Balance is patient-specific
Pathophysiology and Risk Stratification
Assess THROMBOSIS risk first. Only HIGH-risk patients need bridging. Most orthopaedic patients are LOW-MODERATE thrombosis risk and do NOT need bridging.
| Risk Category | Clinical Features | Annual Risk | Periop Management |
|---|---|---|---|
| HIGH | Mechanical MITRAL valve, VTE less than 3mo, stroke less than 3mo | Greater than 10% | BRIDGE with LMWH or UFH |
| MODERATE | Mechanical AORTIC valve, VTE 3-12mo ago, AF CHA2DS2-VASc 3-4 | 5-10% | Consider bridging, individualize |
| LOW | AF CHA2DS2-VASc 0-2, VTE greater than 12mo, bioprosthetic valve | Less than 5% | NO bridging - stop AC, restart postop |
AF Thrombosis Risk (CHA2DS2-VASc Score)
CHA2DS2-VASc Scoring:
- CHF (1 point)
- Hypertension (1)
- Age greater than or equal to 75 (2)
- Diabetes (1)
- Stroke/TIA/thromboembolism (2)
- Vascular disease (1)
- Age 65-74 (1)
- Sex female (1)
| Score | Risk | Bridging Decision |
|---|---|---|
| 0-2 | Low | NO bridging |
| 3-4 | Moderate | Consider bridging if additional risks |
| 5 or more | High | Bridge with LMWH |
Mechanical mitral valves have 2-4x higher thrombosis risk than aortic valves due to larger surface area, lower flow velocities, and left atrial stasis. Always bridge mechanical mitral valves.
Classification
Classification of Anticoagulant Agents
- Examples
- Warfarin
- Mechanism
- Inhibits factors II, VII, IX, X
- Half-life
- 36-42 hours
- Examples
- Dabigatran
- Mechanism
- Direct factor IIa inhibition
- Half-life
- 12-17 hours
- Examples
- Rivaroxaban, Apixaban
- Mechanism
- Direct factor Xa inhibition
- Half-life
- 8-15 hours
- Examples
- Enoxaparin, UFH
- Mechanism
- AT-III mediated
- Half-life
- 4-7 hours (LMWH)
- Examples
- Aspirin, Clopidogrel
- Mechanism
- Platelet inhibition
- Half-life
- Variable
DOAC Considerations:
- Renal clearance varies (dabigatran 80%, apixaban 25%)
- No reliable reversal agents for all DOACs
- Shorter half-life allows faster cessation
Clinical Assessment and Bleeding Risk
| Risk Category | Orthopaedic Procedures | Management |
|---|---|---|
| LOW | Arthroscopy, carpal tunnel, trigger finger, K-wire removal | Minimal interruption, restart 6-12h |
| MODERATE | THA, TKA, ORIF, shoulder arthroplasty, fracture fixation | Stop AC preop, restart 24-48h postop |
| HIGH | Spine surgery, revision THA/TKA, pelvic ORIF, tumor resection | Extended cessation, restart 48-72h postop |
Spinal or epidural anesthesia is considered HIGH bleeding risk due to catastrophic consequences of spinal hematoma (paralysis). This determines timing of anticoagulation cessation and restart.
Investigations and Monitoring
- INR testing if on warfarin - check day before and day of surgery
- Creatinine/eGFR for DOAC patients - determines cessation timing
- Platelet count if on heparin - HIT screening if indicated
- Coagulation studies (PT, APTT) if bleeding concern
- Blood group and crossmatch for major procedures
- Evidence-based cessation/restart protocols
- DOAC timing tables based on renal function
- Bridging decision algorithms
- Neuraxial anesthesia safety guidelines
- Updated regularly with new evidence
Use current institutional protocols alongside ASRA, ACCP/CHEST, ESC/EHRA, NICE and other national guidance for cessation, restart and neuraxial-timing decisions. In smaller or remote centres, specific DOAC reversal agents (idarucizumab, andexanet alfa) and prothrombin complex concentrate may not be held on site - factor this into emergency planning.
Differential of Unexpected Perioperative Bleeding / Coagulopathy
When a patient bleeds more than expected or has an abnormal coagulation screen, distinguish residual anticoagulant from other causes before attributing it to the agent alone.
| Cause | Discriminating Feature | Typical Screen | Action |
|---|---|---|---|
| Residual warfarin effect | Recent VKA, INR raised | INR/PT prolonged, APTT normal-to-raised | Vitamin K +/- PCC; recheck INR |
| Residual DOAC | Recent dose, reduced CrCl, dabigatran | Variable; raised APTT (dabigatran) or anti-Xa | Time/renal clearance; specific reversal if life-threatening |
| Residual heparin/LMWH | Recent dose, raised anti-Xa | APTT prolonged (UFH); anti-Xa raised | Protamine (full for UFH, partial for LMWH) |
| Liver disease | Stigmata of chronic liver disease, low albumin | INR raised, low platelets | Vitamin K, FFP/PCC, treat cause |
| DIC / dilutional coagulopathy | Massive transfusion, sepsis, trauma | Low fibrinogen, low platelets, raised D-dimer | Treat cause; targeted blood products, fibrinogen |
| Inherited bleeding disorder (e.g. von Willebrand, haemophilia) | Lifelong/familial bleeding history | Prolonged APTT, abnormal factor/vWF assays | Haematology; factor concentrate/desmopressin |
Management Algorithm
Warfarin Perioperative Management
Warfarin Perioperative Protocol
Stop warfarin 5 days before surgery. INR will normalize to less than 1.5 by day of surgery in most patients. Check INR on day before surgery to confirm.
If HIGH thrombosis risk, start LMWH (enoxaparin 1mg/kg BD) or UFH infusion when INR less than 2. Give last LMWH dose 24h before surgery.
Confirm INR less than 1.5 (ideally less than 1.2 for neuraxial). If INR greater than 1.5, delay or give vitamin K 1-2mg PO.
Restart warfarin when hemostasis secure (24h for low bleeding risk, 48-72h for high). If bridging, give LMWH until INR greater than 2 for 2 consecutive days.
This protocol follows contemporary guideline recommendations and BRIDGE trial evidence.
Direct Oral Anticoagulant (DOAC) Management
Advantages of DOACs: Predictable pharmacokinetics, no INR monitoring needed, no bridging required, rapid offset. Key variable: RENAL FUNCTION determines cessation timing.
| DOAC | CrCl greater than 50 | CrCl 30-50 | CrCl less than 30 |
|---|---|---|---|
| Apixaban | 24-48h preop | 48h preop | 48-72h preop |
| Rivaroxaban | 24-48h preop | 48h preop | 48-72h preop |
| Dabigatran | 24-48h preop | 72h preop | 96h preop (4 days) |
| Edoxaban | 24-48h preop | 48h preop | 48-72h preop |
- Calculate CrCl (Cockcroft-Gault)
- Stop 24h if CrCl greater than 50 and LOW bleeding risk surgery
- Stop 48h if CrCl greater than 50 and HIGH bleeding risk surgery
- Stop 48-96h if CrCl less than 50 (dabigatran longest)
- NO bridging - DOACs have rapid offset
- Low bleeding risk: Restart 6-12h postop (full dose)
- Moderate risk: Restart 24-48h postop
- High risk: Restart 48-72h postop
- Start at full therapeutic dose (no loading)
- Ensure hemostasis before restarting
Dabigatran is 80% renally excreted. If CrCl less than 50, stop 72-96h preop (3-4 days). Check renal function in all patients on dabigatran. Apixaban and rivaroxaban are less renal-dependent.
Antiplatelet Agents and Coronary Stents
Antiplatelet management is a distinct, high-yield problem from anticoagulant management — and getting the coronary-stent patient wrong can be fatal.
Perioperative Antiplatelet Cessation
| Agent | Stop before surgery | Before neuraxial (ASRA) | Note |
|---|---|---|---|
| Aspirin (low-dose, secondary prevention) | Usually CONTINUE | Not a contraindication alone | Modest bleeding increase; stop only for very-high-risk (intracranial/some spine) or per cardiology |
| Clopidogrel | 5-7 days | 5-7 days | Irreversible P2Y12 inhibitor |
| Ticagrelor | 3-5 days | 5-7 days | Reversible but potent |
| Prasugrel | 7 days | 7-10 days | Most potent; longest interval |
Coronary Stents and Dual Antiplatelet Therapy (DAPT)
A patient with a recent coronary stent on DAPT (aspirin + a P2Y12 inhibitor) is at risk of catastrophic, often fatal stent thrombosis if antiplatelets are stopped too early. Elective surgery should be DEFERRED through the mandatory DAPT period:
- Bare-metal stent (BMS): at least 6 weeks (ideally longer).
- Drug-eluting stent (DES): ideally 6 months; newer-generation DES a minimum of ~3 months (absolute minimum ~1 month) only for time-sensitive surgery, after cardiology discussion.
If surgery cannot wait, continue aspirin throughout wherever possible and stop only the P2Y12 inhibitor, with a clear cardiology-agreed plan to restart it as soon as haemostasis allows. Never interrupt both agents in the high-risk window without multidisciplinary (cardiology) input.
Heparin-Induced Thrombocytopenia (HIT)
HIT is a critical complication of the very heparins used to bridge and prophylax in this topic — and it is prothrombotic, not a bleeding problem.
- Mechanism: immune (IgG) antibodies against the platelet factor 4 (PF4)–heparin complex activate platelets, causing thrombosis and a falling platelet count.
- Timing: platelet fall (typically >50% from baseline) at days 5-10 after heparin exposure (or within hours if recent prior exposure). More common with UFH than LMWH.
- The paradox: despite thrombocytopenia the danger is arterial and venous thrombosis (not bleeding) — limb ischaemia, DVT/PE, stroke.
- Probability: use the 4Ts score (Thrombocytopenia magnitude, Timing, Thrombosis, oTher causes excluded); confirm with PF4 ELISA and a functional assay (serotonin-release assay).
- Management: STOP all heparin (including LMWH, line flushes and heparin-bonded catheters); start a non-heparin anticoagulant (argatroban, danaparoid, fondaparinux, or a DOAC); do NOT transfuse platelets and do NOT start warfarin until the platelet count recovers (warfarin in acute HIT risks venous limb gangrene).
Neuraxial Anesthesia and Anticoagulation
Spinal epidural hematoma causes irreversible paralysis if not decompressed within 8 hours. Prevention requires strict adherence to anticoagulation timing guidelines.
| Anticoagulant | BEFORE Neuraxial (Wait Time) | AFTER Neuraxial / Catheter (Restart) |
|---|---|---|
| LMWH prophylactic | 12 hours | 4h after needle/catheter (catheter OK) |
| LMWH therapeutic | 24 hours | 24h after block; no indwelling catheter |
| Unfractionated heparin SC (prophylactic) | 4-6 hours (or normal APTT) | 1 hour |
| Warfarin | INR less than or equal to 1.4 | Restart once catheter removed |
| Apixaban / Rivaroxaban | 72 hours | 6 hours after catheter removal |
| Dabigatran | 72-120 hours (renal dependent) | 6 hours after catheter removal |
The DOAC interval that makes surgery safe (PAUSE: 1-2 days) is shorter than the interval ASRA requires for a neuraxial block (72h for factor Xa inhibitors). When a spinal/epidural is planned, the ASRA neuraxial interval governs - this is a classic exam discriminator.
If epidural catheter in situ, anticoagulation must be held until AFTER catheter removal. Wait 12h after LMWH prophylactic dose, 24h after therapeutic dose, before removing catheter. Then wait 4h after removal before next LMWH dose.
Surgical Technique
Pre-operative Assessment
- Document last dose date/time
- Check INR (warfarin) or drug levels if available (DOACs)
- Review renal function for DOAC clearance
- Confirm bridging plan if applicable
- Anticoagulation held per protocol
- Bridging LMWH stopped appropriately (24h for prophylactic, 24-48h therapeutic)
- Platelet function normal if on aspirin/clopidogrel
- Group and screen current
- Discuss plan with anaesthesia for neuraxial
- Confirm patient fasted and anticoagulation held
- Recheck INR for warfarin patients (target less than 1.5)
- Document consent includes bleeding risks
Complications and Special Situations
Emergency Surgery on Anticoagulation
Patient needs urgent surgery but is anticoagulated:
Emergency Reversal Protocol
Give Vitamin K 5-10mg IV (onset 6-12h) PLUS Prothrombin Complex Concentrate (PCC) 25-50 units/kg (immediate reversal). Check INR 30 min after PCC.
Consider Idarucizumab (dabigatran reversal) or Andexanet alfa (Xa inhibitor reversal). Expensive and limited availability. May delay surgery 12-24h if possible.
Protamine sulfate reverses heparin (1mg per 100 units UFH). Partial reversal of LMWH. Wait 4-6h if possible.
Balance: Bleeding risk of surgery vs thrombosis risk of reversal. Discuss with hematology.
Postoperative Care
Anticoagulation Restart Timing
- DOAC Restart
- 24-48 hours
- Warfarin Restart
- Day 1 (takes days to effect)
- DOAC Restart
- 48-72 hours
- Warfarin Restart
- Day 1-2
- DOAC Restart
- 72-96 hours
- Warfarin Restart
- Day 2-3, check hemostasis
- DOAC Restart
- 5-7 days
- Warfarin Restart
- Delayed, individualized
- Hemostasis adequacy (drain output, wound)
- Thrombotic risk vs bleeding risk
- Neuraxial anaesthesia removal timing
- Hematology input for complex cases
- For high-risk patients who were bridged, continue LMWH until INR therapeutic (warfarin) or 24-48 hours (DOACs)
Outcomes
Bleeding Outcomes
- Major Bleeding Risk
- 3-5%
- Major Bleeding Risk
- 1-2%
- Major Bleeding Risk
- 1-2%
- Major Bleeding Risk
- 5-10%
- Hb drop ≥20 g/L
- Transfusion ≥2 units
- Bleeding at critical site
- Reoperation for bleeding
- Fatal bleeding
- Inadequate drug cessation
- Renal impairment (DOAC accumulation)
- Concurrent antiplatelet therapy
- Complex/revision surgery
Evidence Base and Key Trials
BRIDGE Trial - Bridging Anticoagulation in AF
- Double-blind RCT of 1884 AF patients on warfarin interrupted for elective procedure; randomised to dalteparin bridging or placebo
- Arterial thromboembolism 0.4% (no-bridge) vs 0.3% (bridge) - no-bridging non-inferior (P=0.01 for non-inferiority)
- Major bleeding 1.3% (no-bridge) vs 3.2% (bridge); RR 0.41 (95% CI 0.20-0.78), P=0.005 for superiority
- Most procedures were low bleeding risk; minor bleeding also reduced by forgoing bridging
PAUSE Cohort - Standardised DOAC Interruption
- Prospective cohort of 3007 AF patients on apixaban, dabigatran or rivaroxaban undergoing elective surgery/procedure
- Standardised, pharmacokinetics-based interruption: omit 1 day pre-op (low bleeding risk) or 2 days (high bleeding risk); no heparin bridging or coagulation testing
- 30-day major bleeding 0.9-1.85% across DOAC cohorts; ~3% for high-bleeding-risk procedures
- 30-day arterial thromboembolism 0.16-0.6%; most patients had minimal residual DOAC level (less than 50 ng/mL) at surgery
ARISTOTLE - Apixaban vs Warfarin in AF
- Double-blind RCT of 18,201 AF patients with at least one stroke risk factor; apixaban 5mg BD vs dose-adjusted warfarin
- Stroke or systemic embolism 1.27% vs 1.60% per year (HR 0.79, 95% CI 0.66-0.95; superior)
- Major bleeding 2.13% vs 3.09% per year (HR 0.69, 95% CI 0.60-0.80)
- All-cause mortality 3.52% vs 3.94% per year (HR 0.89, 95% CI 0.80-0.99)
RE-LY - Dabigatran vs Warfarin in AF
- RCT of 18,113 AF patients; dabigatran 110mg and 150mg BD vs adjusted-dose warfarin
- Dabigatran 150mg reduced stroke/systemic embolism (1.11% vs 1.69% per year; RR 0.66)
- Dabigatran 110mg non-inferior for stroke with lower major bleeding (2.71% vs 3.36% per year)
- Both doses reduced haemorrhagic stroke; GI bleeding higher with 150mg
PERIOP-2 - Postoperative LMWH Bridging RCT
- Double-blind RCT of 1471 patients with AF or mechanical heart valves whose warfarin was interrupted for a procedure
- Randomised after the procedure to postoperative dalteparin bridging vs placebo
- Major thromboembolism 1.0% (dalteparin) vs 1.2% (placebo) - no significant difference (risk difference -0.3%)
- Major bleeding 1.3% (dalteparin) vs 2.0% (placebo) - no significant difference; results consistent for AF and mechanical-valve subgroups
ASRA Evidence-Based Guidelines (4th Edition) - Neuraxial Anaesthesia and Antithrombotics
- Defines safe intervals between antithrombotic dosing and neuraxial puncture/catheter removal to prevent spinal-epidural haematoma
- Prophylactic LMWH: 12h before neuraxial; therapeutic LMWH: 24h before; resume 4h after needle/catheter (prophylactic) or 24h (therapeutic)
- Apixaban/rivaroxaban: hold 72h before neuraxial; dabigatran: 72-120h depending on CrCl
- Warfarin should be stopped and INR normalised (=1.4-1.5) before neuraxial block
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman is scheduled for elective total hip arthroplasty in 10 days. She takes warfarin for atrial fibrillation (CHA2DS2-VASc score 3). Her INR today is 2.5. How would you manage her anticoagulation perioperatively?”
“A 68-year-old man on apixaban 5mg BD for AF is scheduled for TKA with spinal anesthesia. His CrCl is 55 ml/min. When would you stop the apixaban, when is it safe to perform the spinal, and when would you restart?”
MCQ Practice Points
Q: How many days before elective surgery should warfarin be stopped? A: 5 days. Warfarin half-life is 36-42 hours. Stopping 5 days preop allows INR to normalize to less than 1.5 in most patients.
Q: Which patients require bridging anticoagulation with LMWH when stopping warfarin? A: HIGH thrombosis risk only: Mechanical MITRAL valve, recent VTE (less than 3 months), or AF with CHA2DS2-VASc greater than or equal to 5. BRIDGE trial showed bridging increases bleeding without preventing thrombosis in most patients.
Q: What is the main advantage of DOACs over warfarin for perioperative management? A: Predictable offset and NO bridging needed. DOACs can be stopped 24-48h preop and restarted postop without bridging, unlike warfarin which may need LMWH bridging in high-risk patients.
Q: How long after prophylactic LMWH is it safe to perform spinal anesthesia? A: 12 hours. Therapeutic LMWH requires 24 hours. This prevents spinal epidural hematoma, which causes irreversible paralysis.
Q: Why does dabigatran require longer preoperative cessation than other DOACs? A: 80% renal excretion. If CrCl less than 50, dabigatran must be stopped 72-96h preop (3-4 days) vs 48h for apixaban/rivaroxaban.
Guidelines, Registries & Global Practice
Atrial fibrillation affects an estimated 50+ million people worldwide and prevalence rises sharply with age; roughly 1 in 6 patients presenting for elective surgery is on long-term anticoagulant or antiplatelet therapy. With ageing arthroplasty and fragility-fracture populations, the orthopaedic surgeon manages perioperative anticoagulation almost daily, and DOACs have now overtaken warfarin as the most prescribed oral anticoagulant in most high-income health systems.
| Body / Document | Region | Key Position | Evidence Level |
|---|---|---|---|
| ACCP / CHEST (Douketis 2022) | North America / Global | No bridging for most AF; selective bridging only for highest thrombotic risk; standardised DOAC interruption | Guideline (GRADE) |
| ASRA 4th ed (2018) | North America / Global | Defines neuraxial intervals: 72h for factor Xa inhibitors, 12h/24h for prophylactic/therapeutic LMWH | Guideline |
| ESC AF Guidelines (2020/2024) + EHRA DOAC guide | Europe | DOAC interruption by bleeding risk and renal function; bridging discouraged in AF | Guideline |
| NICE NG197 / NG89 | UK | DOAC-led stroke prevention in AF; perioperative VTE prophylaxis for major orthopaedic surgery | Guideline |
| Therapeutic Guidelines (eTG) + ANZCA | Australia / NZ | PK-based DOAC interruption tables; ANZCA neuraxial timing aligned with ASRA | Guideline |
| Source | Type | Practice Point |
|---|---|---|
| BRIDGE (NEJM 2015) | RCT, n=1884 | Forgoing bridging non-inferior for ATE, halves major bleeding in AF |
| PAUSE (JAMA IM 2019) | Prospective cohort, n=3007 | Standardised 1-2 day DOAC interruption without bridging is safe |
| PERIOP-2 (BMJ 2021) | RCT, n=1471 | No benefit of postoperative LMWH bridging, including mechanical valves |
| AOANJRR / national joint registries | Registry | Track VTE, reoperation for haematoma and bleeding-related revision after TJA |
Despite concordant guidelines, real-world bridging rates vary widely between centres and countries (historically 10-40% of warfarin patients), reflecting clinician risk perception rather than evidence. The consistent message across AAOS-aligned practice, NICE, ESC/EHRA, ACCP and eTG is: bridge rarely, interrupt DOACs by a simple PK rule, and let renal function and the neuraxial plan drive timing.
Warfarin Protocol
- Stop 5 days preop, check INR day before surgery (target less than 1.5)
- Bridge only if HIGH risk: mechanical mitral, VTE less than 3mo, AF CHA2DS2-VASc greater than or equal to 5
- Last LMWH bridge dose 24h before surgery
- Restart 24-72h postop (bleeding risk dependent)
DOAC Protocol
- Calculate CrCl first - determines cessation timing
- Stop 24-48h if CrCl greater than 50, 48-96h if CrCl less than 50
- Dabigatran longest (96h if CrCl less than 50)
- NO bridging ever - DOACs have rapid offset
Neuraxial Timing (ASRA 2018 - Spinal Haematoma Prevention)
- LMWH prophylactic: Wait 12h before neuraxial, restart 4h after
- LMWH therapeutic: Wait 24h before neuraxial; avoid indwelling catheter
- Factor Xa inhibitors (apixaban/rivaroxaban): Wait 72h before neuraxial
- Dabigatran: 72-120h before neuraxial (renal dependent); restart 6h after catheter out
Bridging Indications (HIGH Risk Only)
- Mechanical MITRAL valve (always bridge)
- Recent VTE less than 3 months
- AF with CHA2DS2-VASc greater than or equal to 5
- Prior stroke/VTE while on therapeutic anticoagulation
Bleeding Risk Stratification
- LOW: Minor procedures - restart 6-12h postop
- MODERATE: THA/TKA/fracture ORIF - restart 24-48h
- HIGH: Spine, revision THA/TKA - restart 48-72h
- Neuraxial anesthesia = HIGH bleeding risk