Cock-Robin Torticollis | Fixed C1-C2 Rotation | Grisel Syndrome | Dynamic CT | Reduce Early to Avoid Chronic Fixation
- Cock-robin posture: head tilted to one side, chin rotated to the OPPOSITE side, with painful resistance to correction
- The deformity is FIXED - unlike muscular torticollis, the patient cannot rotate past midline toward the chin side
- Dynamic (3-position) CT confirms a fixed C1-C2 relationship that does not correct on attempted counter-rotation
- Grisel syndrome = non-traumatic AARS after head/neck infection or ENT surgery - the worst prognosis
- Chronicity drives outcome - early closed reduction; chronic or recurrent cases need C1-C2 fusion
- “AARS is the dangerous mimic of common childhood torticollis - do not just prescribe stretches
- “On open-mouth (odontoid) view the lateral mass rotated forward looks wider and closer to the dens (wink sign)
- “The key distinction from muscular torticollis: SCM on the side TOWARD which the chin points may be contracted (paradoxical), and rotation is fixed
- “Pang dynamic CT motion analysis grades pathological stickiness (Type I worst, Type III best)
The defining feature is a fixed rotation at C1-C2. The child holds a cock-robin posture and resists correction with pain. Plain muscular torticollis can usually be coaxed past midline; AARS cannot. Treating it as simple torticollis delays diagnosis and risks chronic fixation.
Classic deformity: head tilted toward one side, chin rotated to the OPPOSITE side, slight flexion. The contracted-looking sternocleidomastoid is often on the side the chin points TO - a paradox that catches candidates out, because the muscle is splinting rather than causing the deformity.
A static CT shows the rotation; a dynamic (3-position) CT - neutral, then maximal active rotation each way - proves the relationship is FIXED and does not correct. This both confirms the diagnosis and grades severity (Pang). Plain films and open-mouth views are screening only.
Non-traumatic AARS following pharyngitis, otitis, retropharyngeal abscess, or ENT/adenoidectomy surgery is Grisel syndrome. Inflammatory ligament laxity plus delayed recognition make it the subgroup most likely to need prolonged treatment or fusion.
- Findings
- Fielding type I-II, no anterior shift or minimal
- Management
- Analgesia, soft collar, early reduction - many resolve quickly
- Findings
- Type I-III, fixed on dynamic CT
- Management
- Halter (or caliper) traction, muscle relaxants, monitor neurology
- Findings
- Pathological stickiness, occiput-C1 compensation
- Management
- More aggressive traction; higher chance of irreducibility and fusion
- Findings
- Loss of normal C1-C2 dynamics, ligament failure
- Management
- Posterior C1-C2 fusion in best achievable alignment
- Findings
- Large anterior or posterior shift, narrowed SAC
- Management
- Urgent MRI, protect the cord, surgical stabilization
Overview and Epidemiology
Atlantoaxial rotatory subluxation (AARS) - when fixed and persistent, often called atlantoaxial rotatory fixation (AARF) - is an abnormal, locked rotation of the atlas (C1) on the axis (C2). The patient presents with a painful, fixed torticollis (the cock-robin posture) that, unlike ordinary muscular torticollis, cannot be voluntarily corrected.
it is the classic "dangerous torticollis" that must not be missed. Recognise it, image it correctly (dynamic CT), and treat it early before the rotation becomes permanently fixed.
- Children are the predominant group. The atlantoaxial joint is shallow and ligamentously dependent, and children have more horizontal facets and greater ligamentous laxity, so relatively minor force or inflammation can lock C1 on C2.
- According to PubMed, a 15-year paediatric series of 55 children with AARS/F had a mean age of about 8.5 years with a roughly even sex distribution [Spinnato 2020].
- Adults can develop AARF, almost always after trauma. A systematic review of published adult cases found a mean age of about 36 years, with motor-vehicle accidents and falls the leading mechanisms, and Fielding-Hawkins type I the most common pattern [Zafarshamspour 2024].
- Typical setting
- Children, often trivial event
- Key point
- Most common; frequently resolves with early treatment
- Typical setting
- After pharyngitis, otitis, retropharyngeal abscess, or ENT surgery
- Key point
- Worst prognostic group; treat infection AND the neck
- Typical setting
- Adults and adolescents
- Key point
- Higher-energy; look for associated fractures and ligament injury
The most useful bedside question is: can the patient rotate the head past the midline toward the side the chin points to? In AARS this movement is blocked and painful because the joint is mechanically fixed. In muscular torticollis it is usually possible, if uncomfortable.
Pathophysiology and Anatomy
- The C1-C2 complex provides roughly 50% of all cervical rotation (about 45 degrees to each side), pivoting around the dens.
- There is no intervertebral disc; stability depends entirely on bone shape and ligaments.
- The transverse ligament is the primary restraint holding the dens against the anterior arch of C1 and preventing anterior translation. The alar ligaments check rotation and the capsular ligaments of the facet joints stabilise the lateral masses.
According to PubMed, normative CT motion studies in children showed a highly reproducible pattern: as the head turns, C1 first moves alone (single-motion phase), then C1 and C2 move together but C1 faster (double-motion phase), and beyond about 65 degrees they move in unison with a fixed maximal separation [Pang 2010]. AARF is a loss of this normal, predictable C1-on-C2 rhythm - the two vertebrae stay locked together regardless of how the head is turned.
The atlas rotates on the axis and then fails to return to neutral. Proposed mechanisms include the lateral mass capsule and synovium becoming caught or swollen, the facet articulation effectively "over-riding" or jamming, and muscle splinting that maintains the abnormal position. Once locked, the joint behaves like a fixed deformity rather than a transient spasm.
According to PubMed, children with chronic AARF develop increasing occiput-C1 laxity and separation as a compensation to keep the eyes level - the mean occiput-C1 angle was markedly higher in chronic than acute cases [Pang and Li 2005]. This shows why a long-standing deformity becomes structural and harder to reverse: the whole craniocervical junction adapts to the malalignment.
Certain underlying disorders weaken the C1-C2 complex and lower the threshold for rotatory subluxation or frank atlantoaxial instability - their presence should heighten suspicion and caution (including before intubation or general anaesthesia). Remember them as ligamentous laxity, bony anomaly and inflammatory destruction: (1) Down syndrome (generalised ligamentous laxity, transverse-ligament incompetence and occasional os odontoideum - a recognised cause of atlantoaxial instability); (2) mucopolysaccharidoses, especially Morquio syndrome (odontoid hypoplasia/dysplasia with instability); (3) os odontoideum (a separate ossicle in place of the dens, allowing C1-C2 translation); (4) juvenile idiopathic arthritis and rheumatoid arthritis (erosive/inflammatory C1-C2 instability); (5) connective-tissue disorders (Ehlers-Danlos, Marfan); and (6) congenital craniocervical anomalies (e.g. Klippel-Feil). A torticollis in such a child deserves a particularly low threshold for imaging and specialist involvement.
Classification Systems
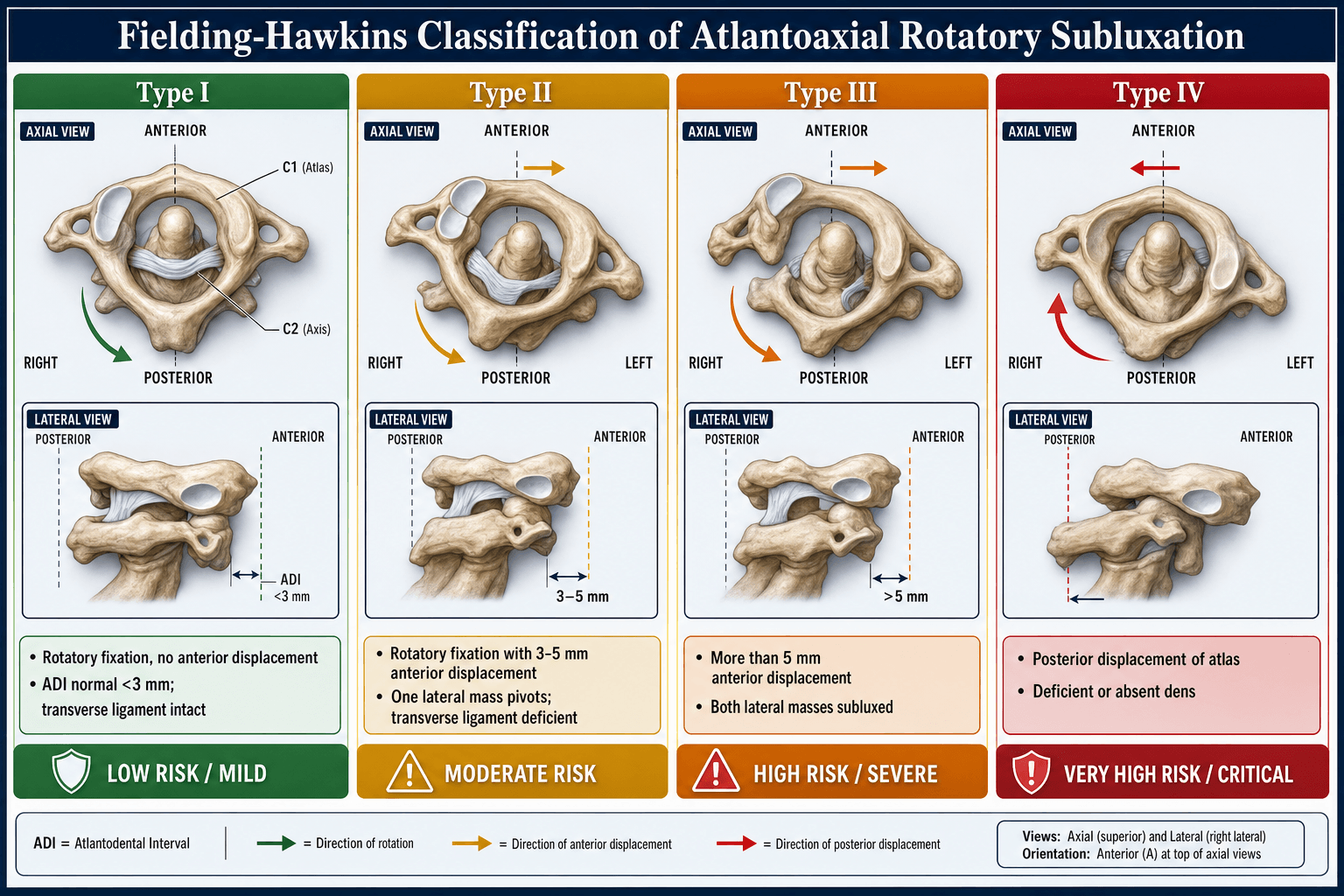
Fielding-Hawkins classification - the traditional, anatomy/displacement-based system, graded on the degree of anterior atlantodental shift:
- Description
- Rotatory fixation without anterior displacement
- Anterior shift
- None
- Ligament status
- Transverse ligament intact
- Treatment emphasis
- Collar, gentle reduction
- Description
- Rotatory fixation with anterior displacement; one lateral mass acts as pivot
- Anterior shift
- 3-5mm
- Ligament status
- Transverse ligament deficient
- Treatment emphasis
- Halter traction
- Description
- Rotatory fixation with anterior displacement of both lateral masses
- Anterior shift
- Greater than 5mm
- Ligament status
- Transverse and secondary ligaments incompetent
- Treatment emphasis
- Traction, likely fusion
- Description
- Rotatory fixation with posterior displacement
- Anterior shift
- Posterior
- Ligament status
- Usually deficient/absent dens
- Treatment emphasis
- Rare, careful reduction, fusion
Type I (no anterior shift) is by far the most common, especially in children and in adult traumatic series. Higher types (II-IV) imply progressive transverse ligament incompetence and are more likely to need surgical stabilization.
Clinical Presentation
- Acute onset of a painful, twisted neck, often in a child.
- A trigger may be identified: minor trauma, or a recent upper respiratory / ENT infection or ENT surgery (Grisel).
- The head is held in a characteristic position and the patient resists attempts to straighten it.
- Head tilted toward one side, chin rotated to the OPPOSITE side, with slight flexion.
- The posture resembles a robin "cocking" its head to listen.
- The sternocleidomastoid that looks contracted is typically on the side the chin points to - it is splinting, not the primary cause (a key difference from congenital muscular torticollis, where the tight SCM is on the side opposite the chin).
- AARS (rotatory fixation)
- Acute, often after trauma/infection
- Congenital muscular torticollis
- Present at or shortly after birth
- AARS (rotatory fixation)
- FIXED; cannot rotate past midline toward chin side
- Congenital muscular torticollis
- Usually can be coaxed past midline
- AARS (rotatory fixation)
- Often painful
- Congenital muscular torticollis
- Usually painless
- AARS (rotatory fixation)
- None
- Congenital muscular torticollis
- Palpable pseudotumour may be present
- AARS (rotatory fixation)
- On the side chin points TO (splinting)
- Congenital muscular torticollis
- Opposite the chin (primary contracture)
A torticollis that is new, painful, follows trauma or infection, has no palpable SCM mass, or fails to correct is not muscular torticollis until proven otherwise. The two dangerous misses are atlantoaxial rotatory fixation and a posterior fossa / spinal tumour.
Most AARS, especially type I, has no neurological deficit. However, large anterior or posterior displacement can narrow the space available for the cord. Always perform and document a full neurological examination; any deficit, or a high-grade displacement, mandates urgent MRI and cord protection.
Differential Diagnosis of Paediatric Torticollis
AARS is only one cause of a child holding the head twisted. The examinable skill is a structured differential that separates the benign, the time-critical and the dangerous.
- Distinguishing features
- Acute, painful, FIXED cock-robin posture; cannot rotate past midline toward chin side
- Action
- Dynamic CT; reduce early
- Distinguishing features
- Infant; palpable SCM pseudotumour; painless; correctable past midline; tight SCM opposite the chin
- Action
- Stretching/physiotherapy; surgery if persistent
- Distinguishing features
- Compensatory head tilt for strabismus/superior oblique palsy; DISAPPEARS when the eye is covered or during sleep; no neck pathology
- Action
- Ophthalmology referral
- Distinguishing features
- Progressive, morning/night symptoms, headache, ataxia, cranial-nerve or long-tract signs
- Action
- URGENT MRI brain and whole spine
- Distinguishing features
- Fever, raised inflammatory markers, dysphagia/drooling; can itself trigger Grisel AARS
- Action
- MRI, antibiotics, drainage as needed
- Distinguishing features
- After metoclopramide/antipsychotics; acute, fluctuating, often with oculogyric crisis
- Action
- Stop the drug; anticholinergic (e.g. procyclidine)
- Distinguishing features
- Painless, long-standing, low hairline/short neck; restricted motion; structural on radiograph
- Action
- Imaging; screen for associated anomalies
- Distinguishing features
- Recurrent self-limiting episodes in infants, often with pallor/vomiting; normal between attacks (migraine variant)
- Action
- Reassurance; exclude posterior fossa lesion
Investigations
- Open-mouth (odontoid) view: the lateral mass that has rotated forward looks wider and closer to the dens, while the contralateral mass looks narrower and further - the asymmetric "wink" appearance. Asymmetry of the dens-lateral mass spaces raises suspicion.
- Lateral view: may show the assimilated posterior arch of C1 and an increased atlantodental interval if there is anterior shift.
- Plain films are suggestive, not confirmatory - positioning the twisted neck reproducibly is difficult and a normal film does not exclude AARS.
- The diagnostic test of choice. A static CT demonstrates the rotational malalignment of C1 on C2.
- A dynamic CT (neutral, then maximal active rotation to each side) shows the relationship is FIXED and does not correct - this both confirms AARF and grades it (Pang).
- Indicated if there are neurological signs, to assess the cord and space available for cord, and to evaluate soft-tissue/inflammatory change in Grisel syndrome. MRI also helps exclude a posterior fossa or cord tumour in atypical torticollis.

Management
Guiding principle: reduce early, before the joint becomes permanently fixed. Most acute cases respond to conservative measures; chronicity and recurrence drive the need for surgery.
Analgesia, muscle relaxant, soft collar and rest. Many early, low-grade (type I) cases reduce spontaneously or with gentle measures within days.
Halter (or caliper/Gardner-Wells) traction to achieve gradual reduction, with regular neurological checks. Reduction is then held in a collar, SOMI brace or halo depending on type and chronicity.
Posterior C1-C2 fusion in the best achievable alignment for joints that cannot be reduced or that repeatedly re-slip.
As above PLUS treat the underlying infection (appropriate antibiotics) and address any persisting ENT source. Prompt diagnosis can avert surgery.
Non-operative care (the default for most cases):
- Analgesia and muscle relaxants to break the splinting cycle.
- Soft collar and activity rest for very acute, low-grade cases.
- Traction (halter for lower-grade; skeletal calipers for higher-grade or chronic) to reduce the locked joint gradually; monitor neurology throughout.
- Immobilisation after reduction (collar, SOMI brace, or halo) to maintain alignment while the soft tissues settle.
- In Grisel syndrome, add antibiotics for the underlying infection.
According to PubMed, in adult traumatic AARF, conservative management succeeded in the majority of acute cases but in only a minority of chronic cases [Zafarshamspour 2024]; in children, conservative treatment is effective in most, with delayed recovery concentrated in Grisel cases and higher-grade/larger-rotation deformities [Spinnato 2020; Pang and Li 2005].
RICELadder of Treatment - 'RICE-F'
Hook:Climb the RICE-F ladder rung by rung - escalate only as far as the joint forces you to
Complications
The principal complication of late diagnosis. A long-standing locked joint develops compensatory occipitocervical changes, becomes irreducible, and leaves a permanent cosmetic and functional torticollis - the main reason early reduction is stressed.
Re-slippage after reduction is common in higher-grade and chronic cases and predicts a worse outcome. Recurrent AARF is a leading trigger for moving to fusion.
Even after successful treatment, some patients permanently lose normal atlantoaxial rotation. Fusion deliberately sacrifices C1-C2 rotation (about 50% of cervical rotation) for stability.
Uncommon but serious with large displacement or during manipulation/surgery. Vertebral artery injury and cord compromise are the feared operative complications.
According to PubMed, recurrent AARF patients did markedly worse on every measure, and recurrence was driven by both higher type and greater chronicity [Pang and Li 2005]. This links the whole topic together: delay leads to fixation, fixation leads to recurrence, and recurrence leads to fusion.
Clinical Relevance and Exam Approach
How to structure a viva answer on a child with acute torticollis:
- Recognise the red flags - acute, painful, post-trauma or post-infection, fixed deformity, no SCM mass.
- Differentiate AARS from muscular torticollis, ocular torticollis, posterior fossa tumour, and infection (osteomyelitis/discitis).
- Image correctly - plain films to screen, dynamic CT to confirm and grade, MRI if neurology or tumour suspected.
- Classify - Fielding-Hawkins (displacement) and Pang (dynamic, with chronicity).
- Treat by a ladder - analgesia/collar then traction then bracing then fusion, reducing early.
- Address the cause in Grisel syndrome - antibiotics plus neck treatment.
Fixed abnormal rotation of C1 on C2 producing a painful cock-robin torticollis.
Dynamic 3-position CT showing the C1-C2 relationship does not correct.
Fielding-Hawkins (I-IV by displacement); Pang (I-III by dynamic stickiness, I worst).
Reduce early (traction); fuse C1-C2 if recurrent, irreducible or chronic.
Guidelines, Registries & Global Practice
AARS/AARF is a rare condition managed largely on the basis of case series and expert consensus rather than randomised trials or implant registries, so practice is guided by the principles below rather than by a single national guideline.
Points of broad international agreement:
- Consensus position
- Dynamic (3-position) CT is the reference standard for confirming and grading fixation; plain films screen only
- Consensus position
- Early reduction is universally emphasised; chronicity predicts irreducibility and fusion across paediatric and adult series
- Consensus position
- Conservative care (analgesia, muscle relaxant, traction, immobilisation) for most acute cases
- Consensus position
- Reserved for irreducible, recurrent, chronic, neurologically compromised or unstable cases - posterior C1-C2 fusion
- Consensus position
- Treat the underlying infection alongside the neck; maintain a low threshold for imaging after ENT procedures
- Classification preference - the displacement-based Fielding-Hawkins system remains the most widely quoted internationally, while the dynamic-CT-based Pang system is favoured where the 3-position protocol is available and where grading guides treatment intensity.
- Traction method and setting - halter traction at home or on the ward versus inpatient skeletal (caliper) traction varies with resources and chronicity.
- Brace choice after reduction - soft collar, SOMI brace and halo are all used, selected by type, chronicity and local practice.
unlike hip and knee arthroplasty, there is no dedicated international registry for C1-C2 fusion in AARF; when fusion is performed, technique (screw-rod versus historical wiring) follows the wider upper-cervical fixation literature.
Present AARS as a time-critical diagnosis: anywhere in the world the message is the same - recognise the fixed cock-robin deformity, confirm with dynamic CT, reduce early, treat any inflammatory source, and reserve C1-C2 fusion for the chronic, recurrent or unstable joint.
Memory Aids
COCKCOCK-ROBIN - The Clinical Picture
Hook:A COCK-ROBIN bird cocks its head - the same fixed, tilted-and-rotated posture you see in AARS
GRISELGRISEL - Non-Traumatic AARS
Hook:GRISEL = inflammation around the throat travels to the C1-C2 joint via the pharyngovertebral veins
IIIIIIIVFielding-Hawkins 0-3-5
Hook:Climb the numbers 0 then 3-5 then over 5 then backwards - rising displacement equals rising instability
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old is brought in with a sudden painful twisted neck that started 3 days after a sore throat. The head is tilted to the right and the chin points to the left, and the child cries when you try to straighten it. How do you assess and manage this child?”
“A 10-year-old presents with a 4-month history of a fixed twisted neck that was initially treated as torticollis. Dynamic CT shows a Pang type I rotatory fixation that does not correct on counter-rotation, and previous traction reduced it but it re-slipped. How do you manage this now?”
“A 30-year-old presents to the emergency department after a motor vehicle accident with neck pain and a rotated head posture. CT shows a Fielding-Hawkins type I atlantoaxial rotatory fixation with no other injury and a normal neurological examination. How do you proceed?”
Definition and Buzzwords
- Fixed abnormal rotation of C1 on C2 - painful torticollis
- Cock-robin posture: head tilted one way, chin rotated the opposite way
- AARS (subluxation) becomes AARF (fixation) when persistent
- Grisel syndrome = non-traumatic AARS after head/neck infection or ENT surgery
Who Gets It
- Children predominate (mean age around 8 years; shallow, ligament-dependent joint)
- Adults: almost always traumatic (mean age around 36, MVA and falls)
- Three buckets: idiopathic/minor trauma, Grisel (inflammatory), major trauma
- Grisel cases have the worst prognosis
Diagnosis
- Key test: dynamic 3-position CT - relationship is FIXED and does not correct
- Open-mouth view: forward-rotated lateral mass looks wider and nearer the dens
- MRI if neurological signs or to assess cord / exclude tumour
- Differentiate from muscular torticollis (fixed deformity, no SCM mass)
Classification
- Fielding-Hawkins I-IV by displacement (I none, II 3-5mm, III greater than 5mm, IV posterior)
- Type I most common; higher types = transverse ligament incompetence
- Pang I-III by dynamic stickiness - Type I is WORST, Type III best
- Chronicity (acute less than 1mo / subacute 1-3mo / chronic greater than 3mo) is independent prognostic axis
Management Ladder
- Acute low-grade: analgesia, muscle relaxant, soft collar
- Persistent/higher grade: halter then caliper traction to reduce, then brace/halo
- Recurrent or irreducible or chronic: posterior C1-C2 fusion (Goel-Harms)
- Grisel: add antibiotics and treat the ENT source
- Reduce EARLY - chronicity is the modifiable enemy
Complications and Viva Essentials
- Chronic fixation, recurrence, permanent loss of C1-C2 rotation
- Vertebral artery injury is the feared operative complication - CT angiography to plan
- Recurrence is driven by higher type and greater chronicity
- Fusion sacrifices about 50% of cervical rotation for stability
- Always document neurology; escalate urgently if any deficit
Evidence Base
- In 50 children with painful torticollis studied with the 3-position dynamic CT protocol, 29 had true AARF (8 Type I, 11 Type II, 10 Type III). Treatment difficulty, irreducibility, need for halo and fusion, and loss of normal C1-C2 rotation were significantly worse with Type I than Type III, and far worse in chronic than acute cases. The worst subgroup was chronic Type I and the best was acute Type III; recurrence worsened all outcomes. Chronic cases developed marked compensatory occiput-C1 separation (mean 31.2 degrees vs 5 degrees acute).
- CT motion analysis in children aged 0-18 defined a highly concordant normal C1-C2 rotation curve (single-motion, double-motion and unison-motion phases). Against this template, three AARF types were defined by descending pathological stickiness (Type I locked regardless of counter-rotation; Type III crosses only with extreme counter-rotation), plus a diagnostic gray zone. A 3-position CT protocol allows both diagnosis and severity grading, with closed traction reduction recommended immediately and C1-C2 fusion for recurrent or irreducible cases.
- Across 55 children (mean age 8.5 years) treated conservatively over 15 years, 16.4% had late recovery (persistence or relapse at 3 months). A concomitant head/neck infection or inflammation (Grisel's syndrome) was the strongest predictor of late recovery (p less than 0.001). Fielding-Hawkins type (p = 0.019) and the measured C1-C2 rotation degree (p = 0.027) also correlated significantly with recovery time.
- Across 61 articles of adult AARF, mean age was about 36 years (54% male). Motor-vehicle accidents (38%) and falls (22%) were the leading mechanisms, and Fielding-Hawkins type I predominated (63%). Conservative management was used in 65% of acute and only 29% of chronic cases; acutely diagnosed patients were more often successfully treated conservatively, while chronically diagnosed patients more often required surgery. Neurological deficits were uncommon.