ABCDE Systematic Assessment | Damage-Control Resuscitation | Orthopaedic Role in Polytrauma
- cABCDE prioritises catastrophic haemorrhage BEFORE airway in combat and prehospital settings
- Tension pneumothorax is a clinical diagnosis — treat immediately with needle decompression, do NOT wait for imaging
- Permissive hypotension targets SBP 80-90 mmHg until surgical haemorrhage control (NOT in TBI)
- Damage-control resuscitation: minimise crystalloid, give blood products early in 1:1:1 ratio
- TXA must be given within 3 hours of injury — greatest benefit within 1 hour
- “ABCDE is sequential — do not move to B until A is secured
- “Lethal triad of trauma: hypothermia, acidosis, coagulopathy — each worsens the others
- “Pelvic binder reduces volume in open-book pelvic fractures and tamponades bleeding
- “Damage-control orthopaedics (DCO): external fixation in unstable polytrauma, definitive fixation later
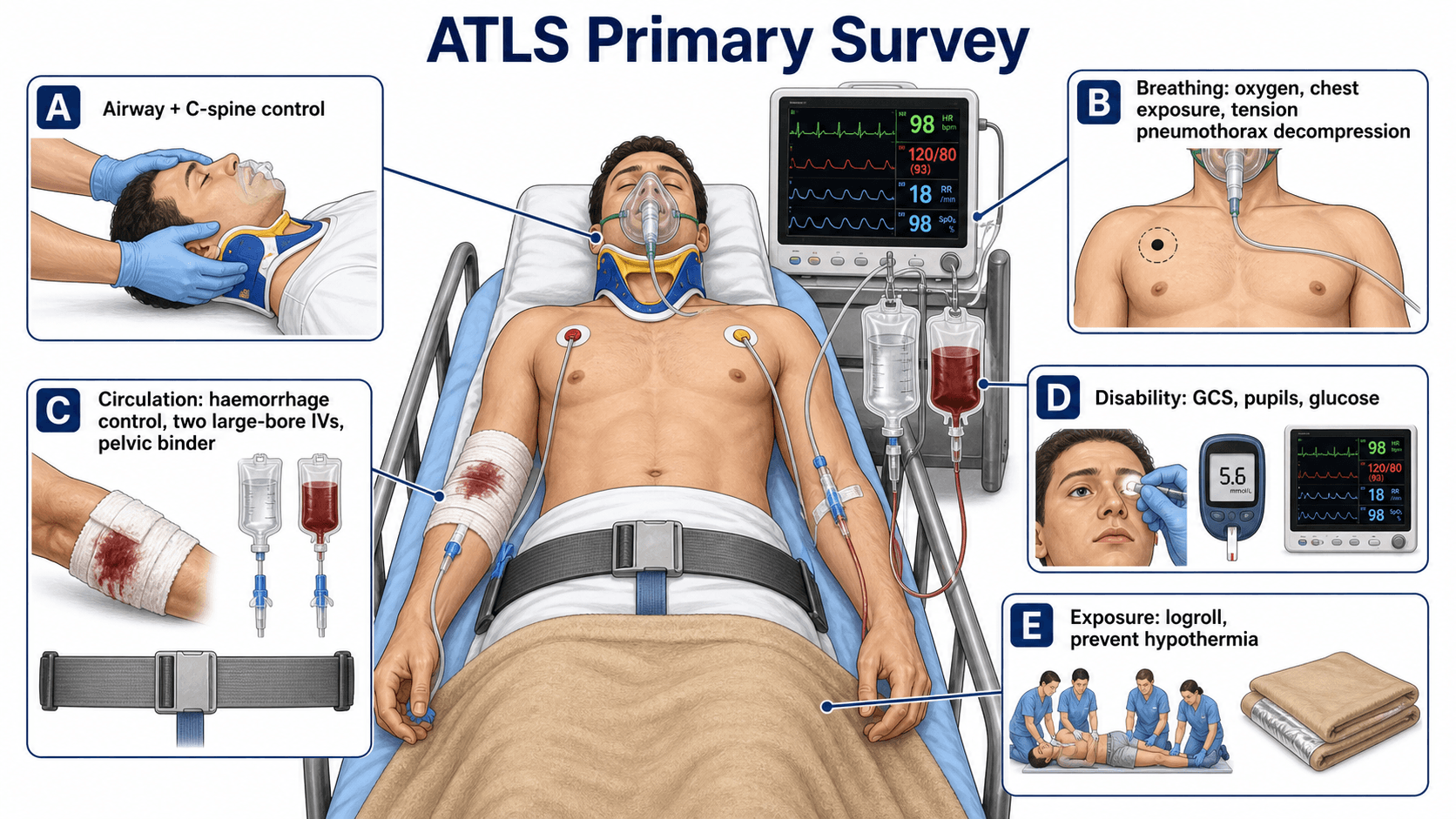
Primary Survey Framework
Airway always comes first. A patient who cannot breathe because of a blocked airway will die before any other injury matters. Secure the airway while maintaining cervical spine immobilisation. Manual inline stabilisation (MILS) is required during intubation — do NOT remove the collar to intubate.
Clinical diagnosis — treat before imaging. Hypotension, absent breath sounds, tracheal deviation (late), distended neck veins, and hyper-resonance. Needle decompression: 2nd intercostal space mid-clavicular line OR 5th intercostal space mid-axillary line. Follow with chest drain.
Target SBP 80-90 mmHg until haemorrhage control. Aggressive crystalloid raises BP, disrupts fresh clot ("pops the clot"), dilutes clotting factors, and worsens coagulopathy. EXCEPTION: traumatic brain injury requires SBP greater than 90 mmHg (ideally greater than 100) to maintain cerebral perfusion pressure greater than 60 mmHg.
Hypothermia, acidosis, coagulopathy. Each factor potentiates the others in a vicious cycle. The trauma coagulopathy seen on arrival (not just from dilution) is an independent predictor of mortality. Prevention is paramount: warm the patient, give blood products not crystalloid, correct acidosis.
- Distinguishing Features
- Tachycardia, hypotension, cool peripheries, pallor
- Key Investigation
- FAST, CT, dropping Hb
- First-Line Treatment
- MTP + surgical haemorrhage control
- Distinguishing Features
- Absent breath sounds, tracheal deviation, distended neck veins
- Key Investigation
- Clinical diagnosis — do NOT wait for imaging
- First-Line Treatment
- Needle decompression then chest drain
- Distinguishing Features
- Beck triad (hypotension, JVD, muffled heart sounds) — present in minority
- Key Investigation
- FAST subxiphoid view, bedside echo
- First-Line Treatment
- Pericardiocentesis or thoracotomy
- Distinguishing Features
- Warm, dry skin, hypotension with bradycardia (loss of sympathetic tone)
- Key Investigation
- Clinical: spinal cord level injury above T6
- First-Line Treatment
- Fluids, vasopressors (norepinephrine or phenylephrine)
ABCDEATLS Primary Survey Sequence
Hook:ABCDE is the lifeline — never skip ahead until the current step is complete!
AMPLETrauma History: AMPLE
Hook:AMPLE history guides anaesthesia safety and identifies bleeding risk!
MARCHTactical Combat Casualty Care: MARCH
Hook:MARCH puts catastrophic haemorrhage before airway — the combat lesson that saves lives!
Overview and Epidemiology
Trauma is the leading cause of death in people aged 1 to 44 years worldwide. The "trimodal distribution" of trauma deaths describes three peaks: immediate (minutes — lethal injuries, haemorrhage), early (minutes to hours — the "golden hour" where ATLS interventions save lives), and late (days to weeks — multisystem organ failure, sepsis). The primary survey targets the second peak where timely, systematic intervention is most impactful. Haemorrhage is the leading preventable cause of death in the early period.
- 5.8 million deaths/year worldwide from injury (WHO data)
- Road traffic crashes: leading mechanism in young adults globally
- Falls: leading mechanism in elderly trauma patients
- Penetrating trauma: increasing proportion in urban centres worldwide
- Blast and combat: military conflict zones, terrorism
- First 60 minutes from injury: highest impact for intervention
- Platinum 10 minutes: the critical window for primary survey completion
- Preventable deaths: up to 30 percent of trauma deaths may be preventable with timely care
- Trauma systems: organised trauma networks reduce mortality by 15-25 percent
- Team approach: simultaneous assessment by trained trauma team is standard
Pathophysiology
The lethal triad of hypothermia, acidosis, and coagulopathy is the primary driver of mortality in severe haemorrhage. Each component potentiates the others in a vicious cycle:
- Hypothermia (core temperature less than 35 degrees Celsius): impairs coagulation enzyme function (platelets become dysfunctional below 33 degrees), shifts oxyhaemoglobin curve leftward, reduces citrate metabolism
- Acidosis (pH less than 7.2): impairs coagulation factor function by approximately 10 percent per 0.1 pH unit drop, reduces myocardial contractility, impishes drug metabolism
- Coagulopathy: up to 25 percent of severely injured patients arrive coagulopathic on admission — this is NOT solely from dilution; trauma-induced coagulopathy (TIC) is an endogenous process driven by tissue injury, shock, and inflammation
Damage-control resuscitation targets all three simultaneously: warm the patient, give blood products (not crystalloid), and achieve haemorrhage control.
- Class I (up to 15%)
- Up to 750 mL
- Class II (15-30%)
- 750-1500 mL
- Class III (30-40%)
- 1500-2000 mL
- Class IV (over 40%)
- Greater than 2000 mL
- Class I (up to 15%)
- Normal
- Class II (15-30%)
- Tachycardic (100-120)
- Class III (30-40%)
- Tachycardic (over 120)
- Class IV (over 40%)
- Tachycardic (variable, may be bradycardic in extremis)
- Class I (up to 15%)
- Normal
- Class II (15-30%)
- Normal (compensated)
- Class III (30-40%)
- Decreased
- Class IV (over 40%)
- Profoundly decreased
- Class I (up to 15%)
- Normal
- Class II (15-30%)
- Slowly (greater than 2 seconds)
- Class III (30-40%)
- Delayed (greater than 3 seconds)
- Class IV (over 40%)
- Absent
- Class I (up to 15%)
- Slightly anxious
- Class II (15-30%)
- Anxious, restless
- Class III (30-40%)
- Confused, anxious
- Class IV (over 40%)
- Lethargic, obtunded
- Class I (up to 15%)
- Crystalloid may suffice
- Class II (15-30%)
- Crystalloid, prepare blood
- Class III (30-40%)
- Blood products required
- Class IV (over 40%)
- Massive transfusion protocol
On arrival: up to one-quarter of severely injured patients are already coagulopathic before any fluid administration. This is driven by:
- Tissue injury releasing tissue factor and thromboplastin
- Shock causing endothelial activation and glycocalyx disruption
- Hyperfibrinolysis (pathological clot breakdown)
- Protein C activation (anticoagulant pathway)
Implication: coagulopathy must be anticipated and treated proactively with haemostatic resuscitation from the outset.
Relevance: long bone and pelvic fractures release fat globules into the circulation. Features (typically 24-72 hours post-injury):
- Respiratory distress (most common)
- Cerebral dysfunction (confusion, altered consciousness)
- Petechial rash (upper body, axilla, conjunctiva — pathognomonic but present in only 20-50 percent)
Orthopaedic implication: early fracture stabilisation reduces fat embolism incidence. This is a key rationale for damage-control orthopaedics in polytrauma.
Classification and Types
ATLS Civilian vs Tactical Approach
- Origin
- ATLS civilian standard (ACS)
- First Step
- Airway with C-spine protection
- When to Use
- Standard hospital trauma reception
- Key Difference
- Airway assessed before haemorrhage
- Origin
- TCCC / military / prehospital
- First Step
- Catastrophic haemorrhage control
- When to Use
- Combat zones, prehospital, mass casualty
- Key Difference
- Haemorrhage controlled BEFORE airway
The ATLS 10th edition (2018) acknowledges the cABCDE approach. In modern civilian practice, catastrophic external haemorrhage (exsanguinating limb, massive scalp bleed) should be controlled simultaneously with or even before airway assessment. The key exam point: explain why the order matters — a patient can survive several minutes without a protected airway but will die within 1-2 minutes from exsanguinating haemorrhage.
The same ABCDE applies to everyone, but two populations have physiology that will catch you out and are high-yield exam material - this topic otherwise covers only the adult.
- Children compensate, then crash: they maintain a normal blood pressure until roughly 30 to 45 percent blood loss, so hypotension is a late, pre-terminal sign - tachycardia is the earliest indicator of shock.
- Weight-based resuscitation: estimate weight (age formula or a length-based tape), give crystalloid 20 mL/kg boluses then 10 mL/kg of blood; use intraosseous access early if IV fails.
- Anatomy: relatively large head and small airway, and a high surface-area-to-mass ratio make hypothermia a major risk; compliant ribs allow significant pulmonary contusion without rib fracture, and the immature spine gives SCIWORA (cord injury without radiographic abnormality). Always consider non-accidental injury.
- Aortocaval compression: the gravid uterus compresses the IVC and aorta when supine, causing supine hypotension - manage with 15 to 30 degrees left lateral tilt or manual uterine displacement.
- "Resuscitate the mother to save the fetus": maternal blood volume is expanded by ~40 to 50 percent, so she can lose large volumes before showing signs while the fetus is already hypoperfused - optimise maternal resuscitation first.
- Specific steps: assess fetal heart rate/CTG, send a Kleihauer-Betke test for fetomaternal haemorrhage, give anti-D (Rh immunoglobulin) to Rh-negative mothers, and do not withhold essential imaging. Consider a perimortem caesarean section within about 4 to 5 minutes of maternal cardiac arrest if the gestation is around 23 weeks or more (improves maternal and fetal survival).
Exam point: in children, hypotension is a late sign (treat tachycardia, resuscitate by weight, IO access, watch for SCIWORA/contusion without fracture); in late pregnancy, tilt left to relieve aortocaval compression, resuscitate the mother first, and remember Kleihauer-Betke, anti-D, fetal monitoring and early perimortem caesarean in arrest.
Clinical Assessment
- Speaking? A talking patient has a patent airway
- Inspect: secretions, blood, vomit, foreign bodies, swelling
- Listen: stridor, hoarseness, gurgling, snoring
- C-spine: manual inline stabilisation (MILS) throughout; semi-rigid collar applied
- Interventions: jaw thrust (NOT head tilt-chin lift), suction, oropharyngeal airway, nasopharyngeal airway (contraindicated in suspected base of skull fracture), endotracheal intubation, surgical cricothyroidotomy as last resort
- Look: chest expansion (symmetrical?), respiratory rate, accessory muscle use, flail segments, open wounds
- Listen: breath sounds bilaterally, added sounds, absent sounds (pneumothorax/haemothorax)
- Feel: tracheal position (central vs deviated), subcutaneous emphysema, chest wall crepitus, percussion (dull = haemothorax, hyper-resonant = pneumothorax)
- Oxygen: high-flow 15L via non-rebreather mask; titrate SpO2 to 94-98 percent
- Pulse: rate, rhythm, quality (thready = shock), compare radial vs femoral
- Blood pressure: may be normal in compensated shock — tachycardia is the earliest sign
- Capillary refill: normal less than 2 seconds; central (sternum) more reliable in hypothermia
- Skin: cool, pale, clammy = vasoconstriction from shock
- IV access: two large-bore cannulae (14G or 16G) in antecubital fossae; IO access if unable
- Blood samples: cross-match, FBC, coagulation, metabolic panel, lactate, blood group
- GCS: Eye (1-4), Verbal (1-5), Motor (1-6) — maximum 15
- GCS less than 8: indicates need for definitive airway protection (intubation)
- Pupils: size, equality, reactivity — unilateral fixed dilated suggests uncal herniation
- Lateralising signs: asymmetric motor responses, babinski reflex
- Spinal cord level: sensory level, motor function in all four limbs
- Blood glucose: bedside — hypoglycaemia masquerades as decreased GCS
Complete exposure is required for thorough assessment (log-roll for posterior examination), but hypothermia must be prevented aggressively:
- Remove wet clothing
- Warm blankets and forced-air warming devices
- Warm IV fluids (to 39 degrees Celsius via fluid warmer)
- Increase ambient temperature
- Cover the patient as soon as examination is complete
Core temperature less than 35 degrees Celsius is an independent predictor of mortality in trauma.
- Key Findings
- Absent breath sounds unilaterally, tracheal deviation (late), hypotension, distended neck veins, hyper-resonance
- Immediate Treatment
- Needle decompression (2nd ICS MCL or 5th ICS MAL) followed by chest drain
- Key Findings
- Sucking chest wound, air entry through wound (if wound diameter greater than two-thirds tracheal diameter)
- Immediate Treatment
- Three-sided occlusive dressing (chest seal), then formal chest drain at a separate site
- Key Findings
- Dullness to percussion, absent breath sounds, hypovolaemia, greater than 1500 mL blood in pleural space
- Immediate Treatment
- Large-bore chest drain (36-40Fr), autotransfusion if available, thoracotomy if ongoing output greater than 200 mL/hour
- Key Findings
- Paradoxical chest wall movement, crepitus, at least 3 ribs fractured in 2 or more places
- Immediate Treatment
- Analgesia, positive pressure ventilation if hypoxic, consider intubation
- Key Findings
- Beck triad (hypotension, JVD, muffled heart sounds) — often incomplete; tachycardia, pulsus paradoxus
- Immediate Treatment
- FAST subxiphoid view, pericardiocentesis (temporising), emergency thoracotomy
Investigations
Adjuncts to the Primary Survey
- ECG monitoring: continuous cardiac monitoring
- SpO2 pulse oximetry: continuous oxygen saturation
- End-tidal CO2 (capnography): if intubated — confirms ETT position, guides ventilation
- Bedside glucose: excludes hypoglycaemia as cause of altered consciousness
- Arterial blood gas: lactate (greater than 4 mmol/L = severe shock), base deficit, pH
The traditional trauma "triad" of X-rays: chest X-ray, pelvic X-ray, lateral cervical spine X-ray
- Chest X-ray: pneumothorax, haemothorax, mediastinal widening (aortic injury), rib fractures
- Pelvic X-ray: pelvic ring disruption — if unstable, apply pelvic binder immediately
- Lateral C-spine: in ATLS, C-spine is cleared clinically (Canadian C-Spine Rule or NEXUS criteria) or by CT — plain X-ray alone is insufficient
Modern practice: many centres proceed directly to whole-body CT (pan-scan) in haemodynamically stable patients, replacing the traditional plain film series.
Four standard views (bedside, rapid, repeatable):
- RUQ (Morison pouch): free fluid between liver and kidney — most sensitive view
- LUQ (splenorenal): free fluid around spleen
- Suprapubic (pelvic): free fluid in pelvis (retrovesical in males, pouch of Douglas in females)
- Subxiphoid (pericardial): pericardial effusion or tamponade
Extended FAST (eFAST) adds: bilateral lung views for pneumothorax
Limitations: detects free fluid (not solid organ injury directly), operator-dependent, lower sensitivity in retroperitoneal injuries, poor in obese patients. A negative FAST does NOT exclude significant injury in an unstable patient — proceed to operative intervention or CT if stable.
- Cross-match (type and screen): prepare blood products
- Full blood count: baseline Hb (may be normal initially in acute haemorrhage — equilibration takes hours)
- Coagulation: PT/INR, aPTT, fibrinogen (less than 1.5 g/L triggers cryoprecipitate)
- Metabolic panel: electrolytes, urea, creatinine
- Lactate and base deficit: markers of tissue hypoperfusion and resuscitation adequacy
- Blood alcohol and drug screen: altered consciousness assessment
- Beta-hCG: all women of childbearing age
- Urinary catheter: measure output (target greater than 0.5 mL/kg/hour), detect haematuria
- Contraindications: blood at urethral meatus, high-riding prostate, perineal ecchymosis (suspect urethral injury — perform retrograde urethrogram first)
- Nasogastric tube: decompress stomach, reduce aspiration risk. OROGASTRIC preferred if suspected base of skull fracture
The initial Hb may be normal in acute haemorrhage because whole blood is lost — the remaining blood is not diluted until interstitial fluid shifts into the vascular space over hours. Do NOT rely on a normal Hb to exclude significant haemorrhage. Lactate and base deficit are far more reliable markers of shock severity and resuscitation adequacy.
Management Algorithm
DCR: The Three Pillars
Damage-Control Resuscitation Protocol
Target: SBP 80-90 mmHg (MAP approximately 60 mmHg) until surgical haemorrhage control is achieved.
Rationale: aggressive fluid raises BP, disrupts fresh clot, dilutes clotting factors, accelerates bleeding from uncontrolled sources.
Method: limited crystalloid (up to 1L warmed crystalloid bolus initially, then blood products). Titrate to mentation (conscious and talking = adequate cerebral perfusion).
EXCEPTIONS:
- Traumatic brain injury: maintain SBP greater than 90 mmHg (ideally greater than 100) to preserve CPP
- Spinal cord injury: maintain MAP greater than 85 mmHg for 7 days
- Elderly patients with limited cardiac reserve: may tolerate hypotension poorly
Minimise crystalloid, give blood products early. Crystalloid dilutes clotting factors, causes haemodilution, and worsens coagulopathy.
Ratio target: RBC to FFP to Platelets 1:1:1 (PROPPR trial)
Tranexamic acid (TXA): 1g IV bolus over 10 minutes, then 1g infusion over 8 hours. MUST be given within 3 hours of injury (CRASH-2 trial). Greatest benefit within 1 hour.
Cryoprecipitate: if fibrinogen less than 1.5 g/L (some centres use threshold of less than 2.0 g/L)
Calcium: 10 mL of 10% calcium chloride for every 4 units of blood products (citrate in stored blood chelates calcium — hypocalcaemia impairs coagulation and myocardial contractility)
Activation criteria (any one):
- Anticipated need for greater than 10 units RBC in 24 hours
- Greater than 4 units RBC in 1 hour
- Active massive haemorrhage with haemodynamic instability
MTP pack contents (varies by institution):
- 4-6 units RBC
- 4-6 units FFP
- 1 apheresis platelet (or 6 random donor platelets)
- Cryoprecipitate (10 units or 2 pools)
Monitoring during MTP: ionised calcium (target greater than 1.0 mmol/L), temperature (target greater than 36 degrees Celsius), ABG (pH, lactate, base deficit), coagulation (TEG or ROTEM if available), fibrinogen, platelet count
The three pillars of DCR work synergistically. Permissive hypotension buys time by reducing bleeding rate. Haemostatic resuscitation restores what is lost (clotting factors, platelets, oxygen-carrying capacity) without dilution. MTP ensures products arrive in the right ratios. All three must operate simultaneously for optimal outcome.
For the trauma patient who is peri-arrest or arrested from non-compressible torso/pelvic haemorrhage, two salvage adjuncts go beyond the standard primary survey and are increasingly examined.
- A salvage procedure via a left anterolateral thoracotomy for the patient who arrests or loses vital signs from trauma.
- Best outcomes in penetrating chest trauma (especially stab wounds) with signs of life recently present; outcomes are dismal in blunt trauma with prolonged CPR or no signs of life (a key selection point).
- Aims: relieve cardiac tamponade (pericardiotomy), control intrathoracic haemorrhage, internal cardiac massage, and cross-clamp the descending thoracic aorta to redistribute the remaining blood to the brain and heart and limit sub-diaphragmatic bleeding.
- A less-invasive temporising adjunct for non-compressible torso or pelvic haemorrhage in profound shock - a balloon catheter is passed via the femoral artery and inflated in the aorta.
- Zone I (descending thoracic aorta, above the diaphragm) for abdominal haemorrhage; Zone III (infrarenal, above the bifurcation) for pelvic/junctional haemorrhage (Zone II is a no-occlusion zone).
- It raises proximal (cerebral and coronary) perfusion and reduces distal bleeding, buying time to definitive control (laparotomy, angioembolisation) - but it is limited by distal ischaemia time and is a bridge, not definitive treatment.
Exam point: the arrested/peri-arrest trauma patient with non-compressible bleeding may need resuscitative thoracotomy (best for penetrating chest with recent signs of life - tamponade release and aortic cross-clamp) or REBOA (femoral balloon, Zone I for abdominal, Zone III for pelvic haemorrhage) as a temporising bridge to definitive haemorrhage control.
Complications
- Incidence / Risk
- Present in up to 25 percent of major trauma admissions on arrival
- Risk Factors
- Severe haemorrhage, prolonged extrication, massive crystalloid
- Prevention and Management
- DCR principles: warm patient, blood products early, haemorrhage control
- Incidence / Risk
- TRALI 1 in 5000; hyperkalaemia from stored blood
- Risk Factors
- Massive transfusion, large volume of older stored RBC units
- Prevention and Management
- Use freshest blood available, monitor K+ and Ca2+, irradiated products if indicated
- Incidence / Risk
- 5-15 percent after massive fluid resuscitation
- Risk Factors
- Greater than 5L crystalloid or blood products, pelvic packing
- Prevention and Management
- Monitor bladder pressure (greater than 20 mmHg), decompressive laparotomy
- Incidence / Risk
- Up to 10 percent of trauma patients have missed injuries initially
- Risk Factors
- Haemodynamic instability preventing full assessment, intoxication, intubation
- Prevention and Management
- Complete secondary survey when stabilised; tertiary survey within 24 hours
- Incidence / Risk
- Common after massive transfusion, lung contusion, femoral nailing
- Risk Factors
- Pulmonary contusion, fat embolism, massive transfusion, aspiration
- Prevention and Management
- Lung-protective ventilation (tidal volume 6 mL/kg), avoid fluid overload
- Incidence / Risk
- Leading cause of late trauma deaths (days to weeks)
- Risk Factors
- Persistent shock, massive transfusion, severe ISS, infection
- Prevention and Management
- Early haemorrhage control, DCR, DCO to limit inflammatory burden
Up to 10 percent of injuries are missed during the initial assessment, particularly in intubated, haemodynamically unstable, or intoxicated patients. A tertiary survey (complete head-to-toe re-examination, review of all imaging, and reassessment of laboratory results) must be performed within 24 hours of admission or when the patient's condition allows. Missed injuries are a significant source of morbidity, medicolegal claims, and preventable mortality.
Outcomes and Prognosis
- Population
- Severe haemorrhage requiring MTP
- Key Outcome
- Reduced coagulopathy, less crystalloid, earlier haemostasis
- Mortality Impact
- Mortality reduced by 25-50 percent compared to crystalloid-heavy approaches
- Population
- Penetrating torso trauma (Bickell study)
- Key Outcome
- Less blood loss before surgical control, fewer coagulopathy complications
- Mortality Impact
- Survival improved from 70 percent to 62 percent in immediate resuscitation group (Bickell, NEJM 1994)
- Population
- Severe trauma requiring massive transfusion
- Key Outcome
- No significant difference in 24h or 30-day mortality between ratios
- Mortality Impact
- Trend toward earlier haemostasis and lower death from exsanguination in 1:1:1
- Population
- Polytrauma with ISS greater than 40 or borderline physiology
- Key Outcome
- Reduced 'second hit' inflammatory response, fewer pulmonary complications
- Mortality Impact
- Reduced ARDS incidence compared to early total care in borderline patients
Best outcomes: organised trauma system, rapid transport (under 60 minutes), damage-control resuscitation initiated prehospital or on arrival, massive transfusion protocol activation, early haemorrhage control (within 60-90 minutes)
Poor prognosis: delayed presentation, persistent coagulopathy despite MTP, lactate greater than 4 mmol/L that fails to clear within 24 hours, ISS greater than 40, base deficit greater than 6, core temperature less than 35 degrees Celsius on arrival
Key threshold: the "lethal triad" on arrival (any two of hypothermia, acidosis, coagulopathy) carries mortality of 50-90 percent if not aggressively reversed.
Guidelines, Registries & Global Practice
- Trauma: leading cause of death worldwide in people aged 1-44 years
- Road traffic injuries: 1.35 million deaths/year globally (WHO); rising in low- and middle-income countries
- Falls: leading cause of trauma death in adults over 65 in high-income countries
- Penetrating trauma: increasing globally, dominates urban trauma centres in the Americas and parts of Africa
- Conflict and humanitarian settings: blast, gunshot, and shrapnel injuries follow military/TCCC protocols (MARCH)
- High-resource settings: organised trauma systems, MTP, TEG/ROTEM, whole-body CT, helicopter retrieval
- Middle-resource: CT may be available; blood banking varies; TXA widely adopted due to low cost
- Low-resource: limited imaging (X-ray, ultrasound), crystalloid-heavy resuscitation, delayed surgical access
- Universal principle: the ABCDE framework and DCR principles are applicable in ALL settings — the resources differ, not the approach
- TXA: particularly important in low-resource settings where blood products are scarce
- Primary Survey
- ABCDE framework; cABCDE acknowledged for catastrophic haemorrhage
- Resuscitation Strategy
- Minimise crystalloid, early blood products, permissive hypotension, TXA within 3 hours
- Orthopaedic Guidance
- Fracture stabilisation reduces morbidity; DCO in unstable patients
- Primary Survey
- ABCDE as per ATLS; emphasise team-based approach and trauma network activation
- Resuscitation Strategy
- Major haemorrhage protocol: 1:1:1 ratio, TXA 1g bolus, FFP and cryoprecipitate early
- Orthopaedic Guidance
- BOAST guidelines for open fractures (debridement within 6h), pelvic fractures, DCO principles
- Primary Survey
- ABCDE with emphasis on simultaneous assessment by trauma team
- Resuscitation Strategy
- MAP 50-60 target in bleeding without TBI; viscoelastic-guided (TEG/ROTEM) transfusion; TXA; calcium; fibrinogen
- Orthopaedic Guidance
- Early fracture stabilisation; DCO in borderline patients
- Primary Survey
- MARCH sequence — catastrophic haemorrhage FIRST
- Resuscitation Strategy
- Whole blood preferred if available; TXA mandatory in combat casualties; tourniquets and haemostatic dressings
- Orthopaedic Guidance
- Tourniquet conversion, damage-control external fixation, far-forward surgery
- Primary Survey
- Standard ABCDE; emphasis on fracture assessment during C and E steps
- Resuscitation Strategy
- Blood product resuscitation per institutional MTP
- Orthopaedic Guidance
- DCO with external fixation principles; timing of definitive fixation based on physiology; specific fixation techniques per fracture pattern
Trauma registries (including TARN, NTDB, and Australian and European trauma registries) provide benchmarking data for mortality, morbidity, and process measures. These registries have consistently demonstrated that organised trauma systems, standardised MTP activation, and adherence to ATLS/DCR principles reduce mortality. The evidence base for trauma resuscitation has shifted dramatically in the past 15 years from crystalloid-heavy to haemostatic resuscitation — exam answers should reflect current DCR practice, not older crystalloid-first approaches.
Record in every trauma primary survey:
- Time of arrival, mechanism of injury, prehospital interventions
- ABCDE findings at each step with interventions performed and response
- GCS (with components E/V/M), pupils, spinal assessment
- Blood products given with times and volumes
- TXA time of administration relative to injury time
- FAST findings
- All imaging performed and results
- Secondary survey findings (when completed)
- Tertiary survey planned within 24 hours
Thorough documentation is essential for handover, quality assurance, and medicolegal protection. Trauma is among the most common sources of medicolegal claims worldwide.
Controversies and Areas of Uncertainty
The debate has largely been settled: balanced crystalloid (e.g., Hartmann's/Ringer's lactate) in limited volume (up to 1L) followed by blood products. Colloids (albumin, starches) have NOT shown survival benefit over crystalloid and may cause harm (renal injury with starches). Normal saline in large volumes causes hyperchloraemic metabolic acidosis — balanced solutions are preferred.
Low-titre whole blood (LTWB) is used by some military and civilian helicopter services. Advantages: single product provides RBC, plasma, and platelets in physiologic ratios; less storage lesion; warm. However, logistical challenges (short shelf life, need for low-titre O donors, leukoreduction) limit widespread adoption. Component therapy (1:1:1) remains the civilian standard.
ATLS suggests SBP 80-90 mmHg. The European guideline suggests MAP 50-60 mmHg. The Bickell study was in penetrating trauma only — evidence for blunt trauma is less robust. There is ongoing debate about whether the target should differ by injury pattern, age, and comorbidity. The consensus is to titrate to consciousness (if the patient can talk, cerebral perfusion is adequate) until haemorrhage control is achieved.
The optimal timing for conversion from external fixation to definitive fixation remains debated. Early total care within 24-48 hours is increasingly supported for patients who stabilise rapidly, while DCO is reserved for those with persistent physiological derangement. The "borderline" patient (ISS 25-40, borderline lactate, borderline coagulopathy) remains a clinical judgement call. Biomarkers (IL-6, CRP) have been proposed but are not yet validated for clinical decision-making.
MCQ Practice Points
Q: What is the correct sequence of the ATLS primary survey? A: ABCDE — Airway (with C-spine protection), Breathing, Circulation (with haemorrhage control), Disability, Exposure/Environment. Each step must be completed before proceeding to the next. In the cABCDE approach used in tactical and prehospital settings, catastrophic haemorrhage is addressed before airway.
Q: What is permissive hypotension and when is it contraindicated? A: Permissive hypotension targets SBP 80-90 mmHg until surgical haemorrhage control is achieved. It avoids the "popping the clot" phenomenon where aggressive fluid resuscitation raises BP and disrupts fresh clot. It is CONTRAINDICATED in traumatic brain injury (SBP must be maintained greater than 90 mmHg for CPP) and spinal cord injury (MAP greater than 85 mmHg for 7 days).
Q: What is the time window for TXA administration in trauma and why does timing matter? A: TXA must be given within 3 hours of injury — ideally within 1 hour for maximum benefit. The CRASH-2 trial showed greatest survival benefit when given within 1 hour (RR 0.68 for death from bleeding). Importantly, TXA given AFTER 3 hours was associated with increased mortality. Dose: 1g IV over 10 minutes, then 1g over 8 hours.
Q: What are the activation criteria for massive transfusion protocol? A: Anticipated need for greater than 10 units RBC in 24 hours, OR greater than 4 units RBC in 1 hour, OR active massive haemorrhage with haemodynamic instability. The target ratio is 1:1:1 (RBC to FFP to Platelets). Key adjuncts include TXA, cryoprecipitate (fibrinogen less than 1.5 g/L), and calcium supplementation.
Q: How do you diagnose and treat tension pneumothorax in the primary survey? A: Clinical diagnosis: absent breath sounds unilaterally, hypotension, distended neck veins, and tracheal deviation (a late sign). Treat immediately with needle decompression (2nd ICS mid-clavicular line OR 5th ICS mid-axillary line) followed by formal chest drain. Do NOT wait for imaging — this is a treatable cause of death in the B step.
Q: What is damage-control orthopaedics and when is it indicated? A: DCO uses temporary external fixation to stabilise fractures in physiologically unstable polytrauma patients, deferring definitive fixation until the patient is stabilised. Indicated in patients with ISS greater than 40, chest AIS greater than 3, persistent coagulopathy, hypothermia, or acidosis. It avoids the "second hit" inflammatory surge of definitive surgery. Conversion to definitive fixation occurs at days 2-8 when physiology normalises.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old man is brought to the emergency department by ambulance after a high-speed motor vehicle collision. He was the unrestrained driver. On arrival, he is agitated, tachypnoeic (RR 32), SpO2 82 percent on 15L oxygen, HR 128, BP 78/50. His trachea is deviated to the left, the right hemithorax is silent with hyper-resonance to percussion, and neck veins are distended. What is your immediate management?”
“A 78-year-old woman on warfarin for atrial fibrillation (INR 3.2 on arrival) falls down a flight of stairs. She is confused (GCS E3V4M5 = 12), HR 110, BP 72/44, and complains of severe pelvic pain. Pelvic X-ray shows an open-book pelvic fracture (APC type III). FAST shows free fluid in the pelvis. How do you manage this patient?”
Primary Survey ABCDE
- A: Airway with C-spine protection (MILS during intubation, jaw thrust, ETT, cricothyroidotomy)
- B: Breathing (RR, SpO2, breath sounds — treat tension pneumothorax before imaging)
- C: Circulation with haemorrhage control (2 large-bore IV, MTP, pelvic binder, tourniquet)
- D: Disability (GCS, pupils, glucose — GCS less than 8 = intubate)
- E: Exposure with temperature control (full exam, log-roll, warm patient)
Damage-Control Resuscitation (3 Pillars)
- Permissive hypotension: SBP 80-90 mmHg until haemorrhage control (NOT in TBI)
- Haemostatic resuscitation: blood products early, 1:1:1 ratio, minimize crystalloid
- MTP activation: greater than 10 units RBC/24h or greater than 4 units/1h or massive haemorrhage
- TXA: 1g bolus then 1g over 8 hours — MUST be within 3 hours (ideally within 1 hour)
- Calcium: 10 mL 10% CaCl for every 4 units blood products (citrate chelation)
Lethal Triad and Targets
- Hypothermia: keep core temperature greater than 36 degrees Celsius
- Acidosis: target pH greater than 7.2; lactate clearance monitors resuscitation adequacy
- Coagulopathy: INR less than 1.5, platelets greater than 50, fibrinogen greater than 1.5 g/L
- Initial Hb may be normal in acute haemorrhage — do not rely on it to exclude shock
- Lactate and base deficit are the most reliable markers of tissue hypoperfusion
Life-Threatening Injuries (Treat in Primary Survey)
- Tension pneumothorax: clinical diagnosis — needle decompression immediately, then chest drain
- Massive haemothorax: greater than 1500 mL in pleural space — large-bore chest drain
- Cardiac tamponade: FAST subxiphoid view — pericardiocentesis or thoracotomy
- Open pneumothorax: three-sided dressing (chest seal), then chest drain at separate site
- Flail chest with pulmonary contusion: analgesia, positive pressure ventilation if hypoxic
Orthopaedic Role in Polytrauma
- Pelvic binder: immediate C-step intervention for open-book pelvic fractures
- DCO: external fixation in unstable patients (ISS greater than 40, coagulopathy, acidosis)
- ETC: definitive fixation within 24-48h in stable patients (normal lactate, normothermic)
- Open fractures: debridement within 6 hours (BOAST); antibiotics and tetanus prophylaxis
- DCO-to-definitive conversion: days 2-8 when physiology normalises
Key Exceptions and Pitfalls
- Permissive hypotension is CONTRAINDICATED in TBI (maintain SBP greater than 90-100 mmHg)
- Nasogastric tube contraindicated in suspected base of skull fracture (use orogastric)
- Urinary catheter contraindicated if suspected urethral injury (meatal blood, high prostate)
- TXA after 3 hours may be HARMFUL — note the time of injury
- Normal initial Hb does NOT exclude significant haemorrhage
Evidence Base and Key Trials
Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2)
- Randomised placebo-controlled trial of over 20,000 adult trauma patients with significant haemorrhage across 274 centres in 40 countries
- TXA (1g loading dose over 10 minutes then 1g over 8 hours) reduced all-cause mortality from 16.0 percent to 14.5 percent (RR 0.91)
- Benefit greatest when given within 1 hour of injury (RR 0.68 for death from bleeding); treatment within 3 hours was effective
- TXA given AFTER 3 hours from injury was associated with INCREASED mortality (harm signal)
- No significant increase in vascular occlusive events
Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial
- Multicentre RCT comparing 1:1:1 vs 1:1:2 (RBC to FFP to Platelets) in 680 severely injured trauma patients
- No significant difference in 24-hour mortality (12.7 percent vs 17.0 percent) or 30-day mortality (22.4 percent vs 26.1 percent)
- More patients in the 1:1:1 group achieved haemostasis (86 percent vs 78 percent) and fewer died of exsanguination by 24 hours (9.2 percent vs 14.6 percent)
- No difference in complications (ARDS, multi-organ failure, infection, venous thromboembolism)
Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries
- RCT of 598 patients with penetrating torso injuries and prehospital SBP less than 90 mmHg
- Delayed resuscitation group (fluid withheld until OR) had higher survival (70 percent vs 62 percent)
- Delayed group had shorter hospital stay and fewer complications
- Suggested that raising BP before surgical haemorrhage control disrupts clot and accelerates bleeding
The European guideline on management of major bleeding and coagulopathy following trauma (sixth edition)
- Multidisciplinary consensus guideline synthesising evidence on trauma haemorrhage management
- Recommends damage-control resuscitation with permissive hypotension (target MAP 50-60 mmHg) until haemorrhage control in patients without TBI
- Recommends 1:1:1 or 1:1:2 blood product ratios with goal-directed therapy guided by viscoelastic testing (TEG/ROTEM)
- Strongly recommends TXA within 3 hours (ideally within 1 hour) at 1g bolus then 1g over 8 hours
- Recommends fibrinogen supplementation if levels less than 1.5 g/L (or TEG/ROTEM-guided), calcium supplementation, and temperature target greater than 36 degrees Celsius
Military application of tranexamic acid in trauma emergency resuscitation (MATTERs study)
- Retrospective cohort study of 896 combat casualties requiring massive transfusion at a military treatment facility
- TXA administration was independently associated with reduced mortality (17.4 percent vs 23.9 percent without TXA)
- Benefit was greatest in patients receiving massive transfusion (greater than 10 units RBC) — unadjusted survival difference of 13.7 percent
- No increase in thromboembolic complications