Cranial Migration of Odontoid | Foramen Magnum Encroachment | Occipitocervical Instability
- Basilar invagination = odontoid tip prolapses superiorly through foramen magnum
- Chamberlain line: odontoid tip greater than 6.6 mm above palato-occipital line is diagnostic
- Rheumatoid arthritis is the most common acquired cause (atlantoaxial and occipitocervical instability)
- Lower cranial nerve palsies (IX-XII) and myelopathy are hallmark presentations
- Treatment requires occipitocervical fusion; decompression alone is contraindicated without stabilisation
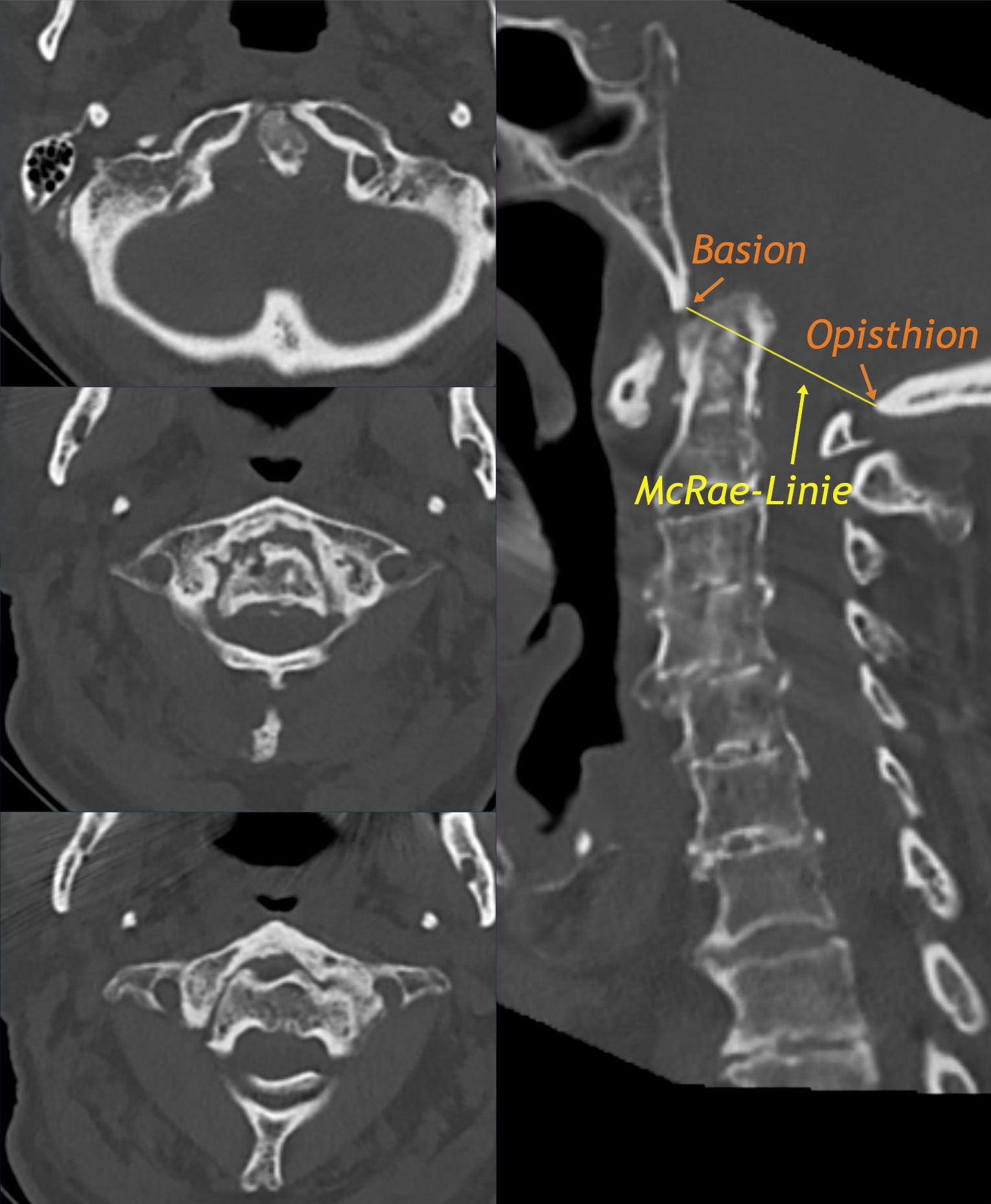
- “Chamberlain line = hard palate to posterior lip of foramen magnum (opisthion)
- “McGregor line = hard palate to lowest point of occipital curve (easier on lateral X-ray)
- “McRae line = anterior to posterior lip of foramen magnum (below this line is normal)
- “Ranawat line measures C2 pedicle to C1 ring on lateral view for RA basilar invagination
- “NEVER decompress without fixation in basilar invagination
Basilar invagination = primary developmental anomaly where the odontoid process prolapses cephalad through the foramen magnum. Basilar impression = secondary/acquired form from bone softening (RA, Paget, OI). Both cause brainstem and upper cervical cord compression.
Chamberlain: hard palate to opisthion. Odontoid tip greater than 6.6 mm above = invagination. McGregor: hard palate to lowest occipital curve. Odontoid tip greater than 4.5 mm above = invagination. McRae: basion to opisthion. Anything below this line is normal.
Myelopathy is the most common presentation. Lower cranial nerve palsies (IX-XII), dysphagia, dysarthria, vertebrobasilar insufficiency, and "cock-robin" head posture. Neck pain and restricted motion are common early symptoms.
Stabilisation is the treatment, NOT decompression alone. Occipitocervical fusion is the gold standard. Transoral odontoidectomy is reserved for irreducible ventral compression. Posterior decompression without fusion worsens instability.
- Diagnosis
- Odontoid above Chamberlain line, Klippel-Feil features
- Treatment
- Occipitocervical fusion if symptomatic or progressive
- Key Pearl
- Screen for Os odontoideum and C1 assimilation
- Diagnosis
- Ranawat index reduced, anterior atlantodental interval widened
- Treatment
- Occipitocervical fusion, consider transoral decompression
- Key Pearl
- Most common acquired cause of basilar invagination
- Diagnosis
- MRI showing cervicomedullary junction compression
- Treatment
- Urgent occipitocervical fixation +/- ventral decompression
- Key Pearl
- Decompression without fixation is contraindicated
CMMRadiographic Lines for Basilar Invagination
Hook:CMM = Chamberlain, McGregor, McRae - measure from hardest landmark first!
Overview and Epidemiology
Basilar invagination is a high-stakes condition where the odontoid process migrates cephalad through the foramen magnum, compressing the cervicomedullary junction. It is a favourite viva topic because it tests knowledge of craniovertebral junction anatomy, radiographic measurement lines, and the critical surgical principle that stabilisation (not decompression alone) is the treatment. Missing the diagnosis can lead to catastrophic brainstem compression.
- Basilar invagination: Primary/congenital upward migration of the odontoid into the foramen magnum
- Basilar impression: Secondary/acquired form due to bone softening at the skull base
- Atlantoaxial instability: May coexist, particularly in RA and congenital forms
- Platybasia: Flattening of the skull base angle (greater than 143 degrees), often coexists but is a distinct measurement
- Congenital: Often associated with Klippel-Feil triad, Chiari I malformation, Os odontoideum
- Acquired: Rheumatoid arthritis is the most common acquired cause (up to 10 percent of severe RA patients)
- Age at presentation: Bimodal - congenital presents in second to third decade; RA-related in fifth to seventh decade
- Sex: No strong sex predilection for congenital forms; RA-related follows RA epidemiology (female predominant)
Pathophysiology
The craniovertebral junction (CVJ) includes the occiput, atlas (C1), and axis (C2). Stability depends on the transverse ligament (primary restraint against anterior C1 translation), the alar ligaments (limit rotation and lateral flexion), and the tectorial membrane (continuation of the posterior longitudinal ligament). The odontoid process normally projects upward from the body of C2 into the ring of C1, articulating with the anterior arch of C1. In basilar invagination, the odontoid tip protrudes above the foramen magnum, compressing the cervicomedullary junction, lower cranial nerves (IX-XII), and the vertebral arteries. The key vulnerability is that the foramen magnum is the narrowest point in the craniospinal axis - even a few millimetres of odontoid migration can produce devastating neurological compromise.
- Attachment
- Behind dens, between C1 lateral masses
- Function
- Primary restraint to anterior C1 translation
- When Disrupted
- C1-2 instability, pannus in RA
- Attachment
- Dens tip to occipital condyles
- Function
- Limit rotation and contralateral flexion
- When Disrupted
- Rotatory instability, occipitocervical subluxation
- Attachment
- Posterior dens to anterior foramen magnum
- Function
- Limits posterior C1 translation and flexion
- When Disrupted
- Vertical instability, basilar invagination
- Attachment
- Dens tip to basion
- Function
- Minor flexion restraint
- When Disrupted
- Clinically insignificant in isolation
Mechanism: Failure of segmentation between C1 and occiput (occipitalisation of C1) forces the odontoid cephalad
Os odontoideum: Separated dens fragment; the body of C2 migrates upward
Chiari I association: Herniation of cerebellar tonsils below foramen magnum, often coexisting, worsening brainstem compression
Klippel-Feil: Congenital fusion of cervical vertebrae concentrates stress at CVJ
Mechanism: RA synovitis attacks the C1-2 articulations (atlantodental, facet joints)
Transverse ligament destruction: Allows anterior atlantoaxial subluxation
Odontoid erosion: Pannus erodes the dens, weakening the fulcrum of CVJ stability
Vertical migration: Progressive erosion allows C2 to migrate cephalad through foramen magnum
Pannus mass: Adds to ventral cord compression beyond bony impingement alone
CRASHCauses of Basilar Invagination
Hook:CRASH into the foramen magnum - Congenital, RA, Acquired, Syndromes, Haltiaarachchi!
Classification and Types
Classification by Cause
- Specific Conditions
- Os odontoideum, C1 assimilation, Klippel-Feil, Down syndrome, Chiari I
- Mechanism
- Failure of segmentation or odontoid development
- Key Features
- Young patient, short neck, low hairline, may have syndromic features
- Specific Conditions
- Longstanding seropositive RA
- Mechanism
- Pannus erosion of transverse ligament, alar ligaments, odontoid
- Key Features
- Cervical spine involvement in 30-80 percent of RA patients
- Specific Conditions
- Paget disease, osteogenesis imperfecta, hyperparathyroidism
- Mechanism
- Bone softening allows skull base settling onto cervical spine
- Key Features
- Basilar impression rather than true invagination
- Specific Conditions
- Remote C1-2 fracture or ligament injury
- Mechanism
- Chronic instability allows gradual vertical migration
- Key Features
- History of significant cervical trauma years prior
- Specific Conditions
- C1-2 tumour (chordoma, metastasis), TB, pyogenic infection
- Mechanism
- Destructive process weakens C1-2 stability
- Key Features
- Pain out of proportion, constitutional symptoms
Distinguishing congenital from acquired basilar invagination is essential because the treatment approach, associated conditions, and prognosis differ significantly.
The mild/moderate/severe scheme above is descriptive; the examinable modern classification is Goel's, which divides basilar invagination by the presence of atlantoaxial instability and fundamentally changes the operation:
- Group A (the "instability" group): there IS atlantoaxial instability - the odontoid tip is above Chamberlain, McRae and Wackenheim's clival lines and indents the brainstem, with an abnormal (reduced) clivus-canal angle. Goel's key insight is that this is essentially a central/vertical atlantoaxial instability problem - it is therefore reducible by posterior atlantoaxial joint distraction and fixation (Goel technique), which restores height and decompresses the cord without a transoral odontoidectomy or a foramen-magnum decompression.
- Group B (the "stable" group): there is no atlantoaxial instability - the odontoid stays below the Chamberlain/McRae/Wackenheim lines and maintains its relationship to the anterior arch of C1 and clivus, but the whole craniovertebral assembly has migrated; this group is strongly associated with Chiari malformation and syringomyelia and was traditionally treated by foramen-magnum decompression.
Exam point: Goel reframed basilar invagination - many cases previously called "irreducible" (needing transoral surgery) are Group A central atlantoaxial instability that reduces with posterior facetal distraction and C1-2/occipitocervical fixation, while Group B (no instability, Chiari-associated) is the one historically managed by decompression. Knowing Group A vs B (and that A is an instability you can fix posteriorly) is the high-yield modern answer.
Clinical Assessment
- Neck pain: Suboccipital, radiating to vertex
- Neurological progression: Numbness, weakness, gait change, clumsiness
- Cranial nerve symptoms: Dysphagia, dysarthria, hoarse voice, tongue weakness
- Vertebrobasilar symptoms: Vertigo, visual disturbance, syncope on rotation
- Inspect: Short neck, low hairline, restricted cervical rotation (Klippel-Feil triad)
- Motor: Spastic quadriparesis (upper motor neuron signs in all four limbs)
- Cranial nerves: Palatal weakness, tongue wasting, gag reflex impairment
- Cerebellar: Ataxia, dysmetria, nystagmus (brainstem/cerebellar compression)
Acute deterioration: Sudden worsening of myelopathy or onset of respiratory distress signals critical brainstem compression. This is a neurosurgical emergency.
Lhermitte sign: Electric shock sensation down the spine on neck flexion indicates cord compression at the CVJ.
Cock-robin posture: Head tilted to one side and rotated to the other suggests atlantoaxial rotatory subluxation, which may coexist with basilar invagination.
Sleep apnoea: Brainstem compression affecting respiratory centres can present as central sleep apnoea.
- Signs and Symptoms
- Spastic quadriparesis, hyperreflexia, Babinski, Lhermitte
- Mechanism
- Direct cord compression by odontoid
- Significance
- Most common presentation, surgical indication
- Signs and Symptoms
- Dysphagia, dysarthria, hoarseness, tongue fasciculations
- Mechanism
- CNs exit skull base near foramen magnum
- Significance
- Highly suggestive of significant invagination
- Signs and Symptoms
- Vertigo, visual changes, brainstem TIA, syncope on rotation
- Mechanism
- Vertebral arteries pass through C1 transverse foramina
- Significance
- Bow-hunter syndrome variant at CVJ
- Signs and Symptoms
- Raised intracranial pressure, hydrocephalus, papilloedema
- Mechanism
- CSF pathway obstruction at foramen magnum
- Significance
- May need CSF diversion before fusion
Distinguish from: (1) Atlantoaxial instability without invagination - odontoid is normal position but C1 translates anteriorly; (2) Chiari I malformation - cerebellar tonsillar herniation without odontoid migration (may coexist); (3) Cervical spondylotic myelopathy - cord compression lower in cervical spine, no cranial nerve involvement; (4) Foramen magnum tumours (meningioma, chordoma) - similar compression but different imaging appearance. MRI is the key discriminator.
BRAINClinical Features of Basilar Invagination
Hook:BRAIN is compressed in basilar invagination!
Investigations
Imaging Protocol
Views: Neutral, flexion, extension lateral
Lines to draw: Chamberlain (hard palate to opisthion), McGregor (hard palate to lowest occipital curve), McRae (basion to opisthion)
RA specific: Ranawat index (C2 pedicle centre to line connecting C1 anterior and posterior arches; normal greater than 13 mm in women, greater than 15 mm in men)
Dynamic views: Assess for reducibility - does the odontoid reduce on extension?
Indication: Mandatory for all suspected basilar invagination
Findings: Cervicomedullary junction compression, cord signal change (T2 hyperintensity = myelomalacia), pannus mass in RA, associated Chiari malformation
CSF flow study: Assess for obstruction at foramen magnum
Measurement: Space available for cord at CVJ (less than 13 mm is critical)
Indication: Pre-operative planning for screw trajectory
Findings: Bony anatomy, C1 lateral mass size, occipital bone thickness, vertebral artery course
3D reconstruction: Essential for understanding complex congenital anatomy
Assess: Reducibility of invagination (can the odontoid be reduced on traction?)
Indication: Pre-operative to map vertebral artery course
Importance: Anomalous vertebral artery at C1-2 occurs in up to 20 percent and affects screw placement
Findings: Persistent first intersegmental artery, arcuate foramen (posterior ponticulate), aberrant course
Planning: Avoid vertebral artery injury during C1 lateral mass or C2 pedicle screw placement
The three key radiographic lines measure the same thing from different landmarks:
Chamberlain line (hard palate to opisthion): odontoid tip greater than 6.6 mm above = invagination. Most specific but opisthion can be hard to see.
McGregor line (hard palate to lowest occipital curve): odontoid tip greater than 4.5 mm above = invagination. Most practical for screening because the lowest occipital curve is always visible.
McRae line (basion to opisthion): odontoid tip below this line = normal. If odontoid tip is above McRae line, invagination is present. This is the most clinically relevant line because it represents the actual foramen magnum boundary.
- Landmarks
- Posterior hard palate to opisthion
- Threshold
- Odontoid greater than 6.6 mm above
- Advantage
- Classic, widely taught
- Limitation
- Opisthion difficult to identify on plain X-ray
- Landmarks
- Posterior hard palate to lowest occipital curve
- Threshold
- Odontoid greater than 4.5 mm above
- Advantage
- Easiest to draw, good screening
- Limitation
- Less specific, lower threshold
- Landmarks
- Basion to opisthion (foramen magnum itself)
- Threshold
- Odontoid above this line = positive
- Advantage
- Clinically most relevant (actual foramen magnum)
- Limitation
- Requires clear visualisation of basion and opisthion
- Landmarks
- C2 pedicle centre to C1 ring line
- Threshold
- Less than 13 mm (women), less than 15 mm (men)
- Advantage
- Specifically validated for RA basilar invagination
- Limitation
- Only applicable in RA population
Chamberlain, McGregor and McRae all measure how far the odontoid has migrated upward; an examiner who pushes further will expect the clival/angular measurements, which detect the associated skull-base abnormality and the actual brainstem indentation:
- Wackenheim's clival line: a line drawn down the posterior surface of the clivus; extended caudally it should be tangential to the posterior aspect of the odontoid tip. If the odontoid crosses (transects) this line, basilar invagination is present - this is the line used in Goel's Group A definition above.
- Clivus-canal angle (clivoaxial angle): the angle between Wackenheim's clival line and the posterior vertebral body line of C2. It is normally roughly 150 degrees in extension to 135 degrees in flexion; an angle below about 135 degrees is abnormal and correlates with ventral brainstem kinking and myelopathy severity - a more functional measure than the height lines alone.
- Platybasia (Welcker basal angle): the angle between the nasion-tuberculum line and the tuberculum-basion line, normally about 125-143 degrees; an angle over roughly 143 degrees is platybasia (flattening of the skull base). The topic already notes platybasia coexists with but is distinct from invagination - the key point is that platybasia alone does not compress the cord, whereas basilar invagination does; they are measured differently and must not be conflated.
Exam point: the Chamberlain/McGregor/McRae lines tell you the odontoid has migrated up; Wackenheim's line and the clivus-canal angle tell you the brainstem is actually being indented/kinked, and the basal angle tells you whether there is coexisting platybasia. The clivus-canal angle is the measurement most tied to myelopathy and to surgical realignment goals.

Management Algorithm
Management Principles
Core principle: Stabilisation is the primary treatment. Decompression without fixation is contraindicated.
Decision Pathway
Confirm diagnosis: Radiographic lines + MRI showing cord compression
Neurological status: Quantify myelopathy (mJOA score, Nurick grade)
Reducibility: Can the odontoid be reduced on extension or traction?
Reducible: Posterior occipitocervical fusion alone (odontoid will reduce and decompress with fixation)
Irreducible: Ventral decompression (transoral odontoidectomy) AND posterior occipitocervical fusion
Asymptomatic/Minimal: Monitor with serial imaging if non-progressive
Approach: Posterior occipitocervical fusion is the gold standard
Levels: Typically occiput to C2 (O-C2) or occiput to C3 depending on instability extent
Fixation: Occipital plate + C1 lateral mass screws + C2 pedicle/pars screws + rod
Bone graft: Autologous iliac crest or local bone + BMP (off-label) for fusion
Immobilisation: Rigid cervical collar or halo vest for 8-12 weeks
Imaging: CT at 3-6 months to confirm fusion
Neurological monitoring: Serial exam for improvement in myelopathy
RA medical management: Optimise disease-modifying therapy perioperatively
If the odontoid can be reduced (on extension or traction), posterior fusion alone is sufficient because fixation in the reduced position decompresses the cord. If the odontoid is fixed in its cephalad position, a ventral decompression (transoral or endoscopic endonasal odontoidectomy) is required before posterior fusion. Attempting posterior decompression alone (laminectomy of C1 or suboccipital craniectomy) without addressing the ventral odontoid or providing fixation will worsen instability and neurological outcome.
Complications
- Incidence
- 5-15 percent
- Risk Factors
- Severe pre-op deficit, intraoperative manipulation
- Management
- High-dose steroids, urgent MRI, check implant position
- Incidence
- 1-2 percent per screw
- Risk Factors
- Aberrant vertebral artery, complex congenital anatomy
- Management
- Tamponade, possible endovascular coiling, avoid contralateral screw
- Incidence
- 5-10 percent
- Risk Factors
- Poor bone quality (RA, osteoporosis), smoking, inadequate fixation
- Management
- Revision fixation with enhanced bone graft
- Incidence
- 3-5 percent
- Risk Factors
- Dural adhesions, ventral decompression
- Management
- Lumbar drain, watertight closure, fibrin glue
- Incidence
- Expected after O-C fusion (approximately 50 percent rotation lost)
- Risk Factors
- Occipitocervical fusion inherently sacrifices C0-1 and C1-2 motion
- Management
- Pre-operative counselling, patient acceptance
- Incidence
- 2-5 percent
- Risk Factors
- RA immunosuppression, long operative time, posterior approach
- Management
- IV antibiotics, wound debridement if hardware exposed
The most feared complication of basilar invagination (and of surgery) is respiratory failure from brainstem compression affecting the respiratory centres. Pre-operative respiratory assessment including forced vital capacity (FVC) and sleep study is mandatory. Post-operatively, monitor respiratory function closely in a high-dependency setting. A decline in FVC below 1 litre or a rise in PaCO2 suggests impending respiratory failure.
Outcomes and Prognosis
- Treatment
- Posterior O-C fusion
- Expected Outcome
- 80-90 percent neurological improvement
- Long-term Function
- Good function, limited cervical rotation
- Treatment
- Ventral decompression + posterior fusion
- Expected Outcome
- 60-75 percent improvement, some residual deficit
- Long-term Function
- Functional improvement, wheelchair to walker often achievable
- Treatment
- O-C fusion, optimise medical therapy
- Expected Outcome
- Pannus regression over 6-12 months, variable neural recovery
- Long-term Function
- Depends on systemic RA control and pre-op deficit
- Treatment
- Natural history
- Expected Outcome
- Progressive myelopathy leading to quadriparesis
- Long-term Function
- High mortality from respiratory failure or sudden death
Best prognosis: Early diagnosis before fixed neurological deficit, reducible invagination, good bone quality for fusion, young patient
Poor prognosis: Severe pre-operative myelopathy (especially Nurick grade 4-5), fixed irreducible deformity, RA with poor disease control, elderly with osteoporotic bone
Key threshold: Duration and severity of myelopathy before surgery is the strongest predictor of neurological recovery. Early intervention before cord signal change on MRI gives the best outcomes.
Guidelines, Registries & Global Practice
- RA prevalence varies from 0.3 to 1.0 percent worldwide; cervical involvement correlates with disease duration and severity
- Congenital basilar invagination has no strong geographic or ethnic predilection but higher detection in regions with advanced imaging access
- Klippel-Feil incidence approximately 1 in 40,000 births worldwide
- Down syndrome carries increased risk of atlantoaxial instability and basilar invagination (15-20 percent have AADI greater than 4.5 mm)
- High-resource: Pre-operative CT angiography, 3D navigation, neuronavigation, intraoperative CT for screw accuracy
- Limited-resource: Plain radiographic lines for screening, CT for surgical planning, fluoroscopy-guided screw placement
- Universal principle: The surgical principle (stabilisation, not decompression alone) applies regardless of resources
- Post-operative: Halo vest in limited-resource settings where modern instrumentation is unavailable; rigid collar in high-resource
- Screening
- Lateral cervical X-ray if RA disease duration greater than 5 years or any neck symptoms
- Surgical Indication
- Basilar invagination (Ranawat reduced) or AADI greater than 10 mm with myelopathy
- Approach
- Occipitocervical fusion; transoral only if irreducible
- Screening
- MRI for any RA patient with neurological signs or planned intubation
- Surgical Indication
- Progressive myelopathy, radiographic instability with cord compression
- Approach
- Posterior O-C fusion standard; ventral decompression for fixed deformity
- Screening
- CT-based classification of CVJ pathology; assess reducibility
- Surgical Indication
- Instability with or without neurological deficit in basilar invagination
- Approach
- Screw-rod construct; emphasizes intraoperative reduction techniques
- Screening
- Dynamic imaging (flexion-extension) essential for surgical planning
- Surgical Indication
- Radiographic basilar invagination + clinical myelopathy or progressive deformity
- Approach
- Tailored to reducibility; modern posterior-only approach increasingly favoured
No dedicated arthroplasty registry covers CVJ fusion specifically. Evidence is drawn from large single-centre neurosurgical and orthopaedic spine series (Menezes, Crockard, Goel). The Swedish and Finnish RA biologics registers capture cervical spine surgery data indirectly. The evidence base relies on level 4 case series rather than randomised trials; management principles are consensus-based and driven by natural history data showing high mortality from untreated basilar invagination.
Every RA patient undergoing general anaesthesia must have pre-operative cervical spine imaging (at minimum lateral flexion-extension radiographs). Unrecognised atlantoaxial instability or basilar invagination can cause cord injury during intubation. Alert the anaesthetist and consider fibreoptic intubation if instability is identified.
Controversies & Areas of Uncertainty
Modern posterior instrumentation (C1-2 or O-C2 screw-rod) can achieve intraoperative reduction in many previously "irreducible" cases, potentially avoiding the morbidity of transoral surgery. However, genuinely fixed ventral compression from chronic pannus or bony mass still requires direct decompression. The threshold for attempting posterior-only reduction is evolving.
Congenital basilar invagination found incidentally poses a management dilemma. Prophylactic fusion is generally recommended if the odontoid projects above the McRae line (even without symptoms), given the risk of catastrophic deterioration with minor trauma. However, the natural history of truly asymptomatic cases is not fully defined.
When basilar invagination coexists with Chiari I malformation, controversy exists over whether to address the ventral invagination first (odontoidectomy + fusion) or perform posterior fossa decompression. Most authorities now recommend treating the basilar invagination (ventral decompression and fusion) first, as the Chiari may improve once CVJ stability and CSF flow are restored.
Modern biological DMARDs (TNF inhibitors, IL-6 blockers, JAK inhibitors) may slow or halt cervical spine destruction in RA. Whether widespread biologics use is reducing the incidence of RA basilar invagination is unclear, but earlier disease control appears to decrease the need for cervical spine surgery in RA cohorts treated with biologics from disease onset.
MCQ Practice Points
Q: Which radiographic line extends from the hard palate to the lowest point of the occipital curve? A: McGregor line. This is the most practical screening line because the lowest point of the occipital curve is always visible on lateral radiographs, unlike the opisthion which can be difficult to identify. Odontoid tip greater than 4.5 mm above the McGregor line indicates basilar invagination.
Q: What is the most common acquired cause of basilar invagination? A: Rheumatoid arthritis. RA causes synovitis and pannus formation at the C1-2 articulations, eroding the transverse ligament, alar ligaments, and odontoid process. This allows progressive vertical migration of the axis through the foramen magnum.
Q: Why is posterior decompression alone contraindicated in basilar invagination? A: Because it increases instability without addressing ventral compression. Removing the posterior arch of C1 or performing suboccipital craniectomy eliminates the posterior tension band while the odontoid continues to compress the cord ventrally. This can precipitate further migration and catastrophic neurological deterioration. The treatment is stabilisation (occipitocervical fusion), not decompression.
Q: When is transoral odontoidectomy required in basilar invagination? A: When the invagination is irreducible. If the odontoid cannot be reduced into a normal position on extension or traction (confirmed on dynamic imaging), ventral decompression via transoral or endoscopic approach is necessary before posterior fusion. If reducible, posterior fusion alone in the reduced position achieves indirect decompression.
Q: What is the Ranawat index and what does it measure? A: The Ranawat index measures vertical migration of C2 in RA. It is the distance from the centre of the C2 pedicle to a line connecting the anterior and posterior arches of C1 on lateral radiograph. Normal values are greater than 13 mm in women and greater than 15 mm in men. Values below these thresholds indicate basilar invagination in RA patients.
Q: What is the primary stabiliser preventing anterior atlantoaxial translation? A: The transverse ligament. It runs behind the odontoid process, attaching to the lateral masses of C1, and is the primary restraint against anterior translation of C1 on C2. In RA, the transverse ligament is destroyed by pannus, leading to atlantoaxial instability and contributing to basilar invagination.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman with longstanding seropositive rheumatoid arthritis presents with progressive difficulty walking, bilateral hand numbness, and occasional dysphagia over the past 6 months. She has been on methotrexate and low-dose prednisone. Examination reveals spastic quadriparesis with MRC grade 4/5 in all four limbs, hyperreflexia, and bilateral Babinski signs. Lateral cervical radiograph shows the odontoid tip projecting 8 mm above the McGregor line. MRI confirms cervicomedullary junction compression with T2 cord signal change. What is your diagnosis and management plan?”
“A 24-year-old man presents with a 2-year history of progressive gait disturbance and occasional electric shock sensations down his arms on neck flexion. He has a short neck, low hairline, and restricted cervical rotation. Neurological examination reveals spastic quadriparesis (grade 4+/5), Hoffman sign positive bilaterally, and sustained ankle clonus. MRI shows the odontoid tip projecting well above the foramen magnum with cervicomedullary junction compression, a Chiari I malformation with 8 mm tonsillar descent, and syringomyelia from C2 to C6. CT confirms assimilation of the atlas to the occiput. What is your diagnosis and surgical plan?”
Key Radiographic Lines
- Chamberlain: hard palate to opisthion; odontoid greater than 6.6 mm above = positive
- McGregor: hard palate to lowest occipital curve; greater than 4.5 mm above = positive (best screening)
- McRae: basion to opisthion; odontoid above this line = invagination present (most clinically relevant)
- Ranawat (RA): C2 pedicle to C1 ring line; less than 13 mm (F) or less than 15 mm (M) = vertical migration
Aetiology
- Congenital: Os odontoideum, C1 assimilation, Klippel-Feil, Down syndrome, Chiari I
- Acquired: Rheumatoid arthritis (most common), Paget disease, osteogenesis imperfecta
- RA mechanism: pannus erodes transverse ligament and alar ligaments, allowing C2 cephalad migration
Clinical Presentation
- Myelopathy: spastic quadriparesis, hyperreflexia, Babinski, Lhermitte phenomenon
- Lower cranial nerve palsies: dysphagia, dysarthria, hoarse voice (CN IX-XII)
- Klippel-Feil triad: short neck, low hairline, restricted cervical rotation
- Vertebrobasilar insufficiency: vertigo, syncope on head rotation
Treatment Algorithm
- Reducible invagination = posterior occipitocervical fusion alone (O-C2)
- Irreducible invagination = ventral decompression (transoral) THEN posterior O-C fusion
- NEVER decompress without fixation - posterior laminectomy alone is contraindicated
- RA pannus regresses after fusion; rarely needs direct pannus excision
Critical Exam Pearls
- Stabilisation (not decompression) is the treatment - this is the most testable point
- Always image RA cervical spine before any general anaesthetic
- Reducibility determines whether ventral surgery is needed
- McRae line = actual foramen magnum boundary; if odontoid above this, cord is compressed
Evidence Base and Key Trials
Craniovertebral junction abnormalities
- Landmark review defining the clinical spectrum of craniovertebral junction abnormalities including basilar invagination in congenital and acquired forms
- Established that reducible lesions require only posterior fusion; irreducible lesions need ventral decompression first
- Chamberlain and McRae lines reliably stratify severity and guide surgical planning
- Posterior decompression without fusion worsened outcomes
Cervical spine fusion in rheumatoid arthritis
- Defined the Ranawat index for measuring vertical migration of the axis in RA patients
- Vertical migration correlates with neurological deterioration and need for surgical intervention
- Combined anterior and posterior atlantodental interval measurements predict myelopathy risk
- Established threshold values guiding surgical referral in RA cervical spine disease
Occipitocervical fusion. Indications, technique, and long-term results in thirteen patients
- Series of occipitocervical fusions demonstrating reliable fusion rates with autologous bone graft
- Neurological improvement in the majority of patients with myelopathy from CVJ pathology
- Established occipitocervical fusion as the gold standard for basilar invagination with instability
- Tri-cortical iliac crest graft with wiring technique (predating modern screw-rod systems)
Posterior Reduction of Fixed Atlantoaxial Dislocation and Basilar Invagination by Atlantoaxial Facet Joint Release and Fixation: A Modified Technique With 174 Cases
- Demonstrated that posterior reduction and C1-2 fixation alone can achieve decompression without ventral surgery in selected cases
- Intraoperative reduction technique using C1 lateral mass and C2 pedicle screws with manipulation
- Avoided transoral approach in over 80 percent of cases by achieving reduction through posterior instrumentation
- Good clinical outcomes with modified JOA score improvement in the majority
Surgery on the rheumatoid cervical spine for the non-ambulant myelopathic patient-too much, too late?
- Large prospective series of RA cervical spine surgery including basilar invagination patients
- Vertical migration (basilar invagination) was the strongest predictor of mortality in RA cervical disease
- Surgical stabilisation improved survival and neurological outcome compared to natural history
- Emphasised the need for early surgical intervention before severe myelopathy develops