TGF-beta Superfamily | Osteoinduction | Smad Signaling | Clinical Applications
- BMPs are secreted growth factors in the TGF-beta superfamily
- BMP-2 and BMP-7 are osteoinductive - induce bone formation in non-skeletal sites
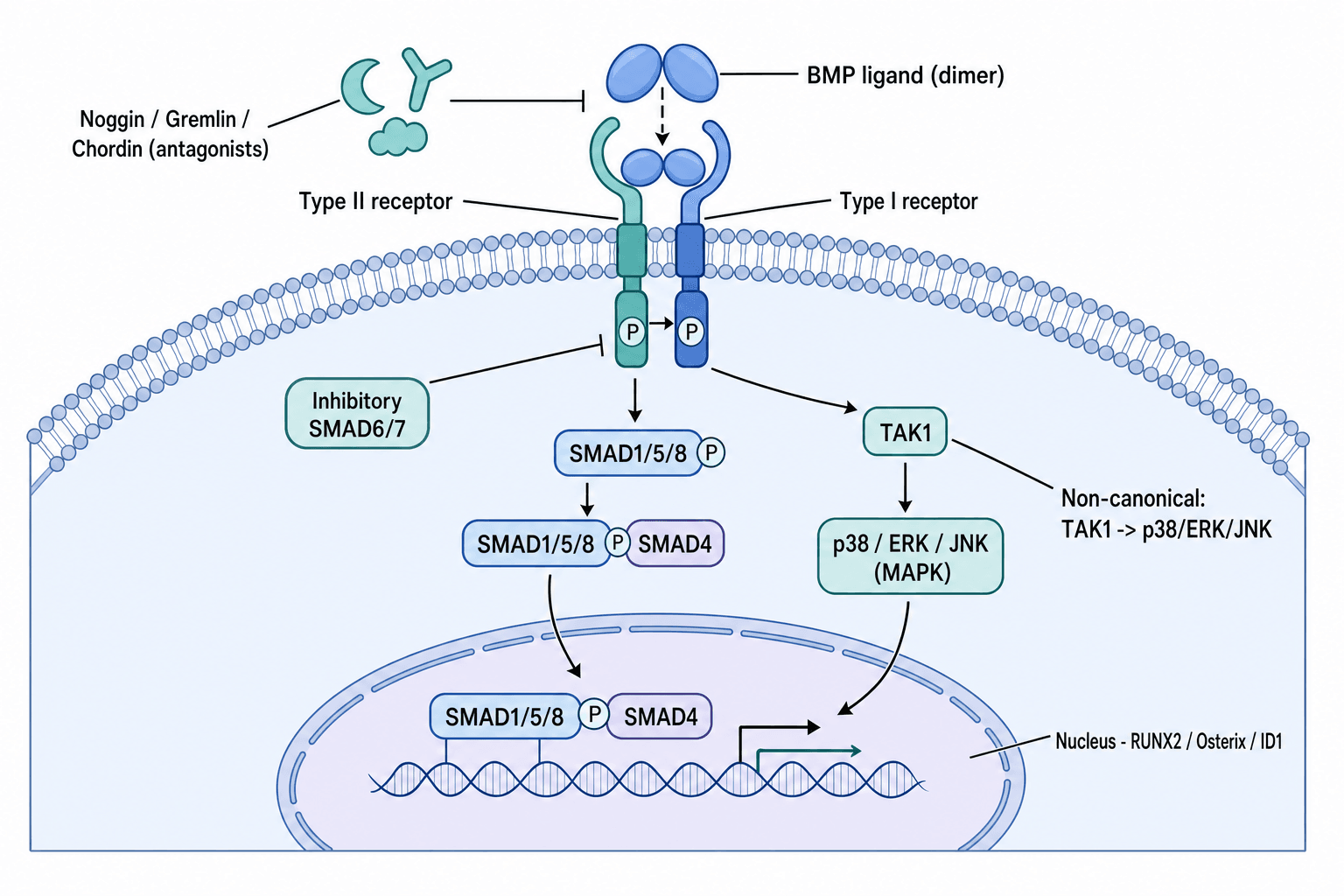
- Signaling via Smad pathway: BMP binds type I/II receptors, activates Smad1/5/8, induces Runx2
- Clinical use: spinal fusion, long bone nonunion, critical-size defects
- Complications: ectopic bone, inflammatory swelling, osteolysis, cost
- “Urist 1965 discovered BMPs by implanting demineralized bone matrix subcutaneously
- “BMP-2 is more osteogenic than BMP-7 but has higher complication risk
- “Supraphysiologic doses used clinically (mg amounts vs ng in normal healing)
- “Carrier scaffold critical - absorbable collagen sponge standard
BMPs induce bone formation in non-skeletal sites (ectopic ossification). This distinguishes osteoinduction from osteoconduction (scaffold for bone growth) and osteogenesis (direct bone formation by osteoblasts).
Canonical BMP signaling: BMP binds type I and II serine/threonine kinase receptors, phosphorylates receptor-Smads (Smad1/5/8), complex with Smad4, translocates to nucleus, activates Runx2 and osterix transcription.
FDA-approved uses: BMP-2 for anterior lumbar interbody fusion (ALIF) and tibial nonunion. BMP-7 (OP-1) humanitarian device exemption for recalcitrant long bone nonunion. Off-label use common but controversial.
Dose-dependent adverse effects: Ectopic bone formation, inflammatory swelling (especially cervical spine), osteolysis, heterotopic ossification. Supraphysiologic dosing (1000x normal levels) contributes to complications.
Overview
Bone morphogenetic proteins (BMPs) are secreted signaling molecules in the transforming growth factor-beta (TGF-beta) superfamily that induce bone and cartilage formation. Marshall Urist discovered BMPs in 1965 by demonstrating that demineralized bone matrix implanted subcutaneously in rabbits induced ectopic bone formation.
Why BMPs matter clinically:
BMPs provide osteoinductive capacity to bone grafts and synthetic scaffolds. Unlike autograft (osteoconductive and osteogenic) or allograft (osteoconductive only), BMPs actively recruit mesenchymal stem cells and induce osteoblast differentiation.
FDA-approved BMP-2 (InFuse, Medtronic) for anterior lumbar interbody fusion and tibial nonunion. BMP-7/OP-1 (Stryker) has humanitarian device exemption for recalcitrant long bone nonunions. Off-label use in posterior spinal fusion, fracture nonunion, and revision arthroplasty is common but controversial.
Osteoinduction is the process by which primitive mesenchymal cells are recruited and induced to differentiate into bone-forming osteoblasts. BMPs are osteoinductive. Osteoconduction is passive scaffold support for bone growth from existing bone. Allograft and synthetic scaffolds are osteoconductive but not osteoinductive unless combined with BMPs.
Where BMP Sits Among Bone-Graft Options (Differential)
A common viva trap is to position BMP correctly against the alternative graft materials. The key discriminators are the three biological properties - osteogenesis (living cells that directly form bone), osteoconduction (a scaffold), and osteoinduction (signals that recruit and differentiate host stem cells).
- Osteogenic
- Yes
- Osteoconductive
- Yes
- Osteoinductive
- Yes
- Key Distinguishing Feature
- Reference standard - all three properties; donor-site morbidity (10-20%)
- Osteogenic
- No
- Osteoconductive
- Yes
- Osteoinductive
- Weak/none
- Key Distinguishing Feature
- Scaffold only; no live cells; disease-transmission and immunogenicity concern
- Osteogenic
- No
- Osteoconductive
- Yes
- Osteoinductive
- Variable
- Key Distinguishing Feature
- Retains some BMP - osteoinductivity is donor- and processing-dependent
- Osteogenic
- No
- Osteoconductive
- Yes
- Osteoinductive
- No
- Key Distinguishing Feature
- Pure synthetic scaffold; needs combining with cells or BMP
- Osteogenic
- No
- Osteoconductive
- No (needs carrier)
- Osteoinductive
- Yes (potent)
- Key Distinguishing Feature
- Pure osteoinductive signal delivered on a collagen-sponge carrier
- Osteogenic
- Yes (MSCs)
- Osteoconductive
- No
- Osteoinductive
- Limited
- Key Distinguishing Feature
- Supplies osteoprogenitor cells; often combined with a scaffold
Understanding BMP biology is essential for basic science vivas and explaining clinical decision-making regarding biologics use.
Concepts: Core BMP Principles
Five concepts unlock every BMP viva:
BMPs are TGF-beta superfamily ligands. Urist (1965) showed demineralised bone matrix induces ectopic bone (osteoinduction); Wozney (1988) cloned the responsible proteins, making recombinant BMP-2/7 possible.
BMPs recruit host mesenchymal stem cells and drive osteoblast differentiation - distinct from osteoconduction (scaffold) and osteogenesis (live cells).
BMP dimer binds type II then type I serine-threonine kinase receptors, phosphorylating Smad1/5/8, which partner Smad4 and activate Runx2 - the master osteoblast transcription factor.
rhBMP-2 (ALIF, open tibia) and rhBMP-7 (HDE nonunion) on collagen-sponge carriers at supraphysiologic doses (100-1000x normal).
5. The evidence pendulum - early industry RCTs (Burkus, Govender) were favourable, but independent re-analyses (Carragee 2011; Fu 2013) found markedly higher harms and no proven advantage over autograft. This tension is the heart of any BMP discussion.
Anatomy
BMP Molecular Structure
Molecular architecture:
- Secreted polypeptide growth factors
- Active form is homodimer (two identical chains)
- Cysteine-rich domain for dimerization
- BMP-2: 114 amino acids per chain, 26 kDa dimer
- BMP-7: 139 amino acids per chain, 35 kDa dimer
Family relationships:
- BMPs belong to TGF-beta superfamily
- Share cysteine knot motif structure
- Conserved receptor binding domains
- Over 20 BMP subtypes identified
- BMP-2, 4, 5, 6, 7 most osteogenic
BMPs must form dimers to be biologically active. The active BMP ligand consists of two polypeptide chains joined by disulfide bonds. This dimeric structure is essential for binding to type I and type II receptors on cell surfaces. Monomeric BMP has no biological activity.
BMP Biology and Classification
BMP Superfamily
The BMP family contains over 20 members, divided into subgroups based on structure and function.
- Key Members
- BMP-2, BMP-4, BMP-6, BMP-7
- Primary Function
- Bone and cartilage induction
- Clinical Relevance
- BMP-2 and BMP-7 FDA-approved for clinical use
- Key Members
- BMP-3 (Osteogenin)
- Primary Function
- Negative regulator of bone formation
- Clinical Relevance
- Inhibits osteogenesis (opposite effect)
- Key Members
- GDF-5, GDF-6, GDF-7
- Primary Function
- Joint and tendon development
- Clinical Relevance
- Experimental tendon/ligament healing
- Key Members
- BMP-5, BMP-8
- Primary Function
- Embryonic development
- Clinical Relevance
- Limited orthopaedic application
BMP-2 and BMP-7 are the most osteogenic and have been developed for clinical use. BMP-2 shows greater osteoinductive potency but higher complication rates compared to BMP-7.
BMP-2 (Recombinant Human BMP-2, rhBMP-2)
Commercial name: InFuse Bone Graft (Medtronic)
Structure:
- Homodimer of two identical 114 amino acid chains
- Molecular weight: 26 kDa
- Requires dimerization for receptor binding
FDA-approved indications:
- Anterior lumbar interbody fusion (ALIF) single-level L4-S1
- Open tibial shaft fractures (acute fracture, not nonunion initially)
- Oral maxillofacial reconstruction (sinus augmentation, ridge preservation)
Off-label uses (controversial):
- Posterior lumbar fusion
- Cervical fusion (BLACK BOX WARNING - airway swelling risk)
- Long bone nonunion
- Revision arthroplasty with bone loss
Clinical dosing:
- ALIF: 12 mg total (1.5 mg/mL on absorbable collagen sponge)
- Posterolateral fusion: 12-24 mg per level (off-label)
- Nonunion: 6-12 mg depending on defect size
Doses are 100-1000 times higher than physiologic levels during normal fracture healing, contributing to adverse effects.
BMP Signaling Pathways
BMPs exert their effects through cell surface receptor binding and intracellular signal transduction.
Canonical BMP-Smad Signaling
The primary BMP signaling mechanism involves Smad proteins (mothers against decapentaplegic homologs).
BMP-Smad Signaling Cascade
BMP ligand (homodimer) binds to type II serine/threonine kinase receptor (BMPR-II, ActR-II) on cell surface. Type II receptor is constitutively active.
Type II receptor recruits and phosphorylates type I receptor (ALK-2, ALK-3, ALK-6). Type I receptor becomes activated kinase.
Activated type I receptor phosphorylates receptor-regulated Smads (R-Smads): Smad1, Smad5, Smad8 at C-terminal serine residues.
Phosphorylated Smad1/5/8 dissociates from receptor, binds to common mediator Smad4 (Co-Smad), forming heteromeric complex.
Smad1/5/8-Smad4 complex translocates to nucleus via importin proteins.
Smad complex binds DNA at Smad-binding elements (SBEs), recruits co-activators (p300, CBP), activates target gene transcription: Runx2, Osterix, Osteocalcin, Alkaline phosphatase.
Runx2 (Cbfa1) is the master transcription factor for osteoblast differentiation. BMP-Smad signaling directly activates Runx2 gene expression. Runx2 then induces downstream osteoblast genes (Osterix, Osteocalcin, Bone sialoprotein, Collagen type I). Runx2 mutations cause cleidocranial dysplasia (absent clavicles, delayed skull ossification).
The Smad pathway is the canonical and most important BMP signaling route for osteogenesis.
Classification
BMP Classification by Function
- BMP Members
- BMP-2, BMP-4, BMP-6, BMP-7, BMP-9
- Primary Function
- Bone and cartilage induction
- Clinical Status
- BMP-2: FDA approved; BMP-7: HDE
- BMP Members
- BMP-3 (Osteogenin)
- Primary Function
- Negative regulator of bone formation
- Clinical Status
- Not for clinical osteoinduction
- BMP Members
- GDF-5 (BMP-14), GDF-6, GDF-7
- Primary Function
- Tendon, ligament, joint development
- Clinical Status
- Experimental tendon repair
- BMP Members
- BMP-5, BMP-8, BMP-10
- Primary Function
- Embryonic patterning, heart
- Clinical Status
- Limited orthopaedic use
- BMP-2 (InFuse): Most widely used
- BMP-7 (OP-1): Limited availability
- ALIF L4-S1 (BMP-2)
- Open tibial fractures (BMP-2)
- Recalcitrant nonunion (BMP-7 HDE)
Under investigation:
- BMP-9: Most potent in vitro
- BMP-6: Strong osteogenic capacity
- GDF-5: Tendon/ligament applications
No clinical approval for these BMPs yet due to manufacturing, cost, and regulatory hurdles.
Investigations
Assessing BMP Response and Bone Healing
- Serial X-rays at 6, 12, 24 weeks post-BMP
- Look for bridging bone formation
- Assess fusion mass in spinal surgery
- Monitor for ectopic bone formation
- Gold standard for assessing fusion
- 3D reconstruction for complex anatomy
- Detect trabecular bridging across fusion
- Pain reduction at fracture/fusion site
- Stability on clinical examination
- Return of weight-bearing capacity
- Soft tissue swelling assessment
- Neurological examination (ectopic bone)
- Dysphagia screening (cervical - contraindicated)
CT scan is superior to plain radiographs for assessing spinal fusion. CT can detect fine trabecular bridging and cortical continuity that plain films miss. Fusion assessment by CT shows 20-30% lower fusion rates compared to X-ray alone, suggesting plain films overestimate fusion success.

Management
Clinical Decision Making for BMP Use
- ALIF L4-S1 (FDA-approved)
- Severe open tibial fractures (Gustilo IIIA/B)
- Recalcitrant nonunion (after failed autograft)
- High-risk fusion patients (smokers, revision surgery)
- Inadequate autograft quantity
- Donor site morbidity concerns
- Metabolic bone disease
- Anterior cervical spine (BLACK BOX)
- Active malignancy
- Pregnancy or breastfeeding
- Known hypersensitivity to BMP or bovine collagen
- Active infection
- Recent cancer history
- Immunocompromised patients
BMP-2 is absolutely contraindicated in anterior cervical spine surgery. The confined prevertebral space amplifies inflammatory swelling, causing life-threatening airway obstruction. Case reports include prolonged intubation, emergency tracheostomy, and death. This is an FDA BLACK BOX warning.
Surgical Technique
BMP Application Techniques
BMP Preparation and Application
- Open BMP kit sterilely
- Add sterile water to lyophilized BMP vial
- Allow to dissolve completely (do not shake)
- Final concentration: 1.5 mg/mL for BMP-2
- Remove absorbable collagen sponge from kit
- Pour BMP solution evenly over sponge
- Allow to absorb for minimum 15 minutes
- Do not wring, squeeze, or manipulate excessively
- Prepare fusion bed or fracture site
- Decorticate surfaces if applicable
- Ensure hemostasis before placement
- Clear soft tissue from target area
- Place BMP-soaked sponge at target site
- Position within cage for ALIF
- Pack into nonunion site for fractures
- Avoid contact with dura, neural elements, vessels
- Meticulous hemostasis
- Layer closure without excess tension
- Drain placement controversial (may remove BMP)
- Monitor for swelling postoperatively
Technique for anterior lumbar fusion:
- Place BMP-soaked sponge inside interbody cage
- Or place sponge anterior/lateral to cage
- Total dose: 12 mg (small kit) or 4.2 mg (XS)
- Sponge dimensions matched to cage size
Technique for posterior fusion (off-label):
- Place BMP sponge over transverse processes
- May combine with local bone or allograft
- Higher doses: 12-24 mg per level
- Contained within paraspinal gutters
Complications and Controversies
Supraphysiologic BMP dosing and off-label use have led to recognized complications and ongoing controversies.
- Incidence
- 10-30% posterior fusion
- Mechanism
- BMP diffusion into surrounding soft tissues
- Management
- Observation if asymptomatic, excision if nerve compression
- Incidence
- 10-50% anterior cervical (CONTRAINDICATED)
- Mechanism
- Cytokine release, edema in confined space
- Management
- Airway monitoring, intubation if severe
- Incidence
- 3-8% ALIF
- Mechanism
- Inflammation, ectopic bone near nerve roots
- Management
- NSAIDs, neuropathic agents, decompression if severe
- Incidence
- 5-15% spinal fusion
- Mechanism
- Inflammatory osteoclast activation
- Management
- Observation, revision if structural concern
- Incidence
- Variable
- Mechanism
- Ectopic induction in muscle/soft tissue
- Management
- Prophylaxis with NSAIDs (if used), excision if symptomatic
- Incidence
- 5-10%
- Mechanism
- Fluid accumulation at BMP site
- Management
- Aspiration if large, observation
Clinical BMP doses are 100-1000 times physiologic levels. Normal fracture healing involves nanogram amounts; clinical use involves milligrams (12 mg = 12,000,000 nanograms). This massive excess causes off-target effects: inflammation, ectopic bone, osteolysis. Dose-reduction strategies under investigation but not yet validated.
Retrograde Ejaculation and Urogenital Complications (Anterior Approach)
A BMP-specific complication that the technique viva and the FDA MAUDE signal both raise - but the complications table omits - is retrograde ejaculation after anterior lumbar interbody fusion (ALIF) using rhBMP-2.
- What it is. Loss of antegrade ejaculation (semen passes retrograde into the bladder) from dysfunction of the superior hypogastric plexus, the sympathetic network draped over the L5-S1 disc and sacral promontory - exactly where the anterior approach dissects and where the BMP sponge sits.
- The association. Both independent re-analyses in this topic's evidence base report higher retrograde ejaculation and urogenital problems with rhBMP-2 in ALIF than with autograft (Carragee 2011; Fu 2013, where the increase was present but not statistically significant). The proposed mechanism is a BMP-driven local inflammatory reaction injuring the adjacent autonomic plexus, additive to the dissection itself.
- Practical points. It affects men, is often permanent, and matters for fertility, so it is a specific, documented consent item for any man undergoing ALIF with rhBMP-2. Risk reduction includes blunt (not monopolar) dissection over the promontory, a left-sided retroperitoneal approach, and containing the BMP sponge within the cage away from the plexus - or choosing a posterior approach / autograft in young men wishing to father children.
Retrograde ejaculation is the classic exam complication of rhBMP-2 in anterior lumbar fusion - injury to the superior hypogastric (sympathetic) plexus over L5-S1. It is more frequent with rhBMP-2 than autograft, can be permanent, and must be specifically consented in men of reproductive age; consider a posterior approach or autograft if fertility is a priority.
Controversies:
Studies suggest over 50% of BMP use is off-label (posterior fusion, cervical spine, nonunion). Lack of FDA approval for these indications creates medico-legal exposure. Evidence quality variable. Industry-sponsored trials dominate literature.
BMP costs thousands of dollars per dose. Cost-effectiveness compared to autograft is debatable. Savings from avoiding donor site morbidity offset by BMP cost. Higher complication management costs. QALY analyses show marginal benefit at best.
Early retrospective studies suggested increased cancer risk with BMP. Subsequent analyses showed no causal link. Theoretical concern: BMPs stimulate cell proliferation. Current consensus: no proven cancer risk, but avoid in active malignancy or recent cancer history.
Most BMP research funded by manufacturers. Concerns about publication bias, ghostwriting, selective outcome reporting. Independent studies show less favorable results. Regulatory scrutiny of manufacturer marketing practices.
Understanding complications and controversies is essential for informed clinical decision-making and exam discussions.
Reconciling the Malignancy Signal
This topic states both that there is "no proven cancer risk" and, via the YODA re-analysis, that rhBMP-2 carried an increased 24-month cancer risk (RR 3.45). Both statements are true, and the reconciliation is the examinable point.
- The signal. The independent YODA / Annals individual-patient-data meta-analysis (Fu 2013) found a statistically significant increase in new cancers at 24 months (RR 3.45, 95% CI 1.98-6.00), and the concern was dose-dependent - most prominent in the high-dose rhBMP-2 ("Amplify", around 40 mg) posterolateral-fusion programme, which the FDA did not approve.
- Why it is not accepted as a proven causal risk. The event numbers were small and the tumour types heterogeneous (no single cancer dominated), follow-up was short, and harm ascertainment in the source (industry) trials was poor. Larger, longer administrative-database and registry studies at standard clinical doses have not confirmed a consistent causal increase.
- The practical position. There is no proven causal cancer risk at standard doses, but a biologically plausible concern (BMPs are mitogenic) plus the dose-dependent signal means rhBMP-2 is avoided in active malignancy and recent cancer, and high off-label doses are discouraged. This nuanced synthesis - not a flat "safe" or "carcinogenic" - is the exam-ready answer.
Postoperative Care
Post-BMP Monitoring Protocol
Postoperative Care Timeline
- Monitor for soft tissue swelling
- Neurological assessment if spinal procedure
- Wound inspection for hematoma
- Pain management per protocol
- Wound check at 2 weeks
- Assess for radiculitis symptoms
- Monitor inflammatory markers if concerns
- Mobilization per surgical protocol
- First radiographs to assess fusion/healing
- Continue activity restrictions
- Physical therapy as appropriate
- Assess for ectopic bone symptoms
- CT scan to confirm fusion (spinal cases)
- Progressive return to activities
- Final radiographs at 12 months
- Discharge if healed
- X-rays at 6, 12, 24 weeks
- CT scan for definitive fusion assessment
- Look for bridging bone, no lucency
- Pain improvement
- Mechanical stability
- Return to function
- Radiculitis (leg pain, numbness)
- Wound swelling or seroma
- New neurological symptoms
- Persistent inflammatory pain
- Early imaging if symptoms
- Neurological examination
- Consider decompression if nerve compression
Outcomes
BMP Clinical Outcomes Summary
- Fusion rate: 94-100%
- Superior to autograft (85-90%)
- Eliminates donor site morbidity
- Fusion rate: 85-95% (variable)
- Mixed evidence vs autograft
- Higher complication rates
- 44% reduction in secondary intervention risk
- Fewer infections in Gustilo type-III injuries
- Faster union and wound healing
- 75-85% union rate
- Comparable to autograft
- Avoids donor site morbidity
Landmark BMP trials:
- Burkus 2002: ALIF RCT - rhBMP-2 94.5% fusion vs autograft 88.7% at 24 months
- Govender 2002 (BESTT): Open tibial fractures - 44% reduction in secondary intervention with 1.5 mg/mL rhBMP-2
- Carragee 2011 / Fu 2013: Independent re-analyses found markedly higher adverse-event rates and no proven advantage over autograft
BMP-2 is most effective for ALIF (FDA-approved) and open tibial fractures. Off-label use has less robust evidence and independent data temper the early industry-sponsored conclusions.
Clinical Applications
BMP-2 is the most widely used osteobiologic in orthopaedic surgery, despite controversies regarding safety and off-label use.
BMP in Spinal Fusion
FDA-approved indication: Anterior lumbar interbody fusion (ALIF), single-level L4-S1
Evidence for ALIF:
- Fusion rates: BMP-2 (95%) vs autograft iliac crest (85%) at 2 years
- Eliminates donor site morbidity (10-20% chronic pain with iliac crest harvest)
- Shorter operative time
- Equivalent clinical outcomes (ODI, VAS)
Off-label use in posterolateral fusion (controversial):
- Not FDA-approved for posterior approach
- Higher doses used (12-24 mg per level)
- Complications: ectopic bone (nerve root compression), osteolysis (screw loosening), radiculitis
- Mixed evidence on fusion rates vs autograft
Cervical spine (BLACK BOX WARNING):
- NOT approved for anterior cervical fusion
- Life-threatening complications: airway edema, hematoma, dysphagia, dysphonia
- Enclosed anterior cervical space amplifies inflammatory swelling
- Case reports of intubation, tracheostomy, death
FDA black box warning: Do NOT use BMP-2 in anterior cervical spine fusion. Soft tissue swelling in the confined prevertebral space can cause life-threatening airway obstruction. Multiple case reports of respiratory compromise requiring prolonged intubation or emergency tracheostomy.
BMP-2 in ALIF is well-established, but off-label use requires careful risk-benefit consideration.
Guidelines, Registries & Global Practice
Global Epidemiology and Regulatory Landscape
rhBMP-2 use peaked in the United States in the late 2000s (used in roughly a quarter to a half of lumbar fusions at its height) and has since declined substantially following the 2011 Spine Journal critique (Carragee) and the 2013 independent YODA/Annals re-analysis (Fu). Uptake has always been far lower in Europe, the UK, Australia and Asia, driven by cost and a more conservative stance toward off-label use. The vast majority of BMP exposure worldwide is now in anterior or posterolateral lumbar fusion and selected long-bone trauma/nonunion.
- Regulator
- FDA (PMA)
- Approved Indications
- rhBMP-2: single-level ALIF (LT-CAGE), acute open tibial fracture with IM nail, sinus/alveolar ridge augmentation; rhBMP-7: HDE only
- Practice Note
- Black-box-equivalent safety communication for anterior cervical use
- Regulator
- CE mark (medicinal product, dibotermin alfa)
- Approved Indications
- rhBMP-2: single-level lumbar interbody fusion, acute tibial fracture; rhBMP-7 (eptotermin alfa) historically for tibial nonunion
- Practice Note
- OP-1 / InductOs availability has contracted; cervical use contraindicated
- Regulator
- MHRA + NICE
- Approved Indications
- InductOs (rhBMP-2) for acute tibial fracture and lumbar fusion within licence
- Practice Note
- NICE has not endorsed routine biologic use over autograft; cost-effectiveness scrutiny
- Regulator
- TGA (ARTG)
- Approved Indications
- rhBMP-2 registered for spinal fusion and tibial fracture indications mirroring FDA labelling
- Practice Note
- Use reserved for high-risk cases; cost borne by hospital or insurer
Key drivers of variation:
- Cost - thousands of dollars/pounds/euros per kit; the dominant barrier outside the US private system
- Evidence shift - independent re-analyses (Carragee 2011; Fu 2013) showed no proven advantage over autograft and higher harms, reducing enthusiasm
- Off-label exposure - historically more than half of US use was off-label; far more restrained internationally
- Reserved indications - revision fusion, recalcitrant nonunion, smokers, metabolic bone disease, inadequate autograft
Across all systems autograft (iliac crest or local bone) remains the reference standard for primary fusion.
MCQ Practice Points
Q: What is the mechanism of action of BMP-2 and BMP-7 in bone healing?
A: Osteoinduction - BMPs induce differentiation of mesenchymal stem cells (MSCs) into osteoblasts. They signal through SMAD pathway (receptor binding → SMAD phosphorylation → gene transcription). BMP-2 and BMP-7 are the only clinically approved BMPs. Distinct from osteoconduction (scaffold providing surface for bone growth) and osteogenesis (cells directly forming bone).
Q: What are the approved clinical indications for recombinant BMP-2 (rhBMP-2, Infuse)?
A: (1) Anterior lumbar interbody fusion (ALIF) in titanium cage - FDA approved. (2) Open tibial fractures with IM nail - FDA approved. Off-label use in many other applications (posterolateral fusion, nonunion, spinal deformity). Note: NOT approved for posterior cervical spine due to swelling risk (dysphagia, airway compromise). Dose: 1.5mg/mL on absorbable collagen sponge.
Q: What are the potential complications of BMP-2 use in spinal surgery?
A: (1) Heterotopic ossification (can cause neural compression), (2) Radiculitis/nerve inflammation, (3) Osteolysis adjacent to cage, (4) Increased cancer risk (controversial - early studies suggested, later refuted), (5) Swelling - especially concerning in anterior cervical spine (dysphagia, airway compromise). Use in posterior cervical spine discouraged. Cost: approximately $5000-$10000 per application.
Q: How does BMP-7 (OP-1) differ from BMP-2 in clinical applications?
A: BMP-7 (OP-1, Stryker) was approved for tibial nonunion and posterolateral spinal fusion under Humanitarian Device Exemption (HDE). Lower osteoinductive potency than BMP-2 but possibly fewer inflammatory complications. BMP-7 is no longer commercially available (discontinued 2014). BMP-2 remains the only clinically available recombinant BMP. Research continues on other BMPs and delivery systems.
Q: What is the role of the carrier/scaffold in BMP delivery and what carriers are used?
A: The carrier provides: (1) Sustained release of BMP, (2) Localization at target site, (3) Structural support. Absorbable collagen sponge (ACS) is the FDA-approved carrier for BMP-2. Other carriers: DBM, calcium phosphate ceramics, synthetic polymers. The carrier affects release kinetics - initial burst release followed by sustained release. BMP alone without carrier has poor retention at site.
At a Glance
Bone morphogenetic proteins (BMPs) are secreted growth factors in the TGF-β superfamily that are osteoinductive—capable of inducing bone formation in non-skeletal sites, as demonstrated by Urist in 1965. BMP signaling occurs via the Smad pathway: BMP binds type I/II serine-threonine kinase receptors, phosphorylates Smad1/5/8, which translocates to the nucleus and activates Runx2 transcription for osteoblast differentiation. FDA-approved applications include rhBMP-2 for ALIF and tibial nonunion, and BMP-7 (OP-1) for recalcitrant nonunion. Clinical use requires supraphysiologic doses (1000× normal levels) delivered on absorbable collagen sponge carriers. Complications include ectopic bone formation, inflammatory swelling (life-threatening in cervical spine), osteolysis, and significant cost.
BMPBMP - Key Functions
Hook:BMP induces Bone formation via Mesenchymal stem cells through Smad Pathway
SMADSMAD - BMP Signaling Cascade
Hook:SMAD pathway: Serine kinase receptors, MAD proteins, Activate Runx2, Differentiation
ECHOESBMP Clinical Complications
Hook:BMP complications ECHO through treatment: Ectopic bone, Cost, Hematoma, Osteolysis, Edema, Subsidence
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“How are BMPs classified and which are used clinically?”
“When would you consider using BMP in a patient undergoing spinal fusion?”
“Describe how you would use BMP-2 in an anterior lumbar interbody fusion.”
“What is the evidence for BMP-2 use in spinal fusion, and what are the controversies?”
“A patient in your public hospital requires spinal fusion. How do you decide whether to use BMP?”
BMP Biology Fundamentals
- BMPs: TGF-beta superfamily, secreted growth factors
- Over 20 BMP subtypes, BMP-2 and BMP-7 most osteogenic
- Osteoinductive: induce bone in non-skeletal sites (Urist 1965)
- BMP-2 more potent than BMP-7 but higher complications
Smad Signaling Pathway
- Type II receptor (BMPR-II) binds BMP, recruits type I (ALK-2/3/6)
- Type I phosphorylates Smad1/5/8 (R-Smads) at C-terminus
- Smad1/5/8 + Smad4 (Co-Smad) complex translocates to nucleus
- Activates Runx2 (master osteoblast TF) → Osterix, Osteocalcin, BSP, Collagen I
Clinical BMPs
- BMP-2 (InFuse): FDA-approved ALIF L4-S1, open tibial fractures
- BMP-7 (OP-1): HDE for recalcitrant long bone nonunion (limited availability)
- Dosing: 12 mg ALIF, 12-24 mg posterolateral (off-label)
- Supraphysiologic: 100-1000x normal healing levels
FDA-Approved Indications
- BMP-2: ALIF single-level L4-S1 (fusion rate 94-100%)
- BMP-2: Open tibial shaft fractures (44% fewer secondary interventions, BESTT)
- BMP-2: Oral maxillofacial (sinus augmentation, ridge preservation)
- BMP-7: HDE only - recalcitrant nonunion after failed autograft
Complications
- Ectopic bone: 10-30% posterolateral (nerve compression risk)
- Osteolysis/cysts: 5-15% (screw loosening concern)
- Radiculitis: 3-8% ALIF (inflammation near nerve roots)
- Cervical CONTRAINDICATED: airway edema, life-threatening (BLACK BOX)
Key Exam Points
- Urist 1965: demineralized bone matrix subcutaneous → ectopic bone
- Osteoinduction (active MSC recruitment) vs osteoconduction (passive scaffold)
- Runx2 knockout: cleidocranial dysplasia (absent clavicles)
- Off-label use over 50%: posterolateral fusion, nonunion, revision surgery
Evidence Base
Bone Formation by Autoinduction - The Founding Observation
- Demineralised (decalcified) bone matrix implanted into non-skeletal sites induced new bone via autoinduction
- Host mesenchymal cells of the recipient bed were recruited and differentiated into bone-forming cells
- Established the concept of an osteoinductive substance latent within bone matrix
- Coined the framework that later led to identification of bone morphogenetic protein
Molecular Cloning of BMPs - Defining the Family
- Isolated human cDNA clones for three BMPs (BMP-1, BMP-2A, BMP-3) from purified bovine bone extract
- Each recombinant protein independently induced cartilage formation in vivo
- BMP-2A and BMP-3 identified as new members of the TGF-beta supergene family
- Enabled recombinant production of BMPs and the subsequent clinical biologics
rhBMP-2 vs Autograft in ALIF - Pivotal RCT
- 279 patients randomised: rhBMP-2/absorbable collagen sponge (143) vs iliac crest autograft (136), tapered threaded cages
- Fusion rate at 24 months: rhBMP-2 94.5% vs autograft 88.7%
- Shorter operative time and lower blood loss with rhBMP-2 (no harvest)
- 32% of autograft patients reported persistent iliac crest donor-site discomfort at 24 months
rhBMP-2 in Open Tibial Fractures - BESTT Trial
- 450 open tibial shaft fractures randomised to standard IM nail care vs rhBMP-2 (0.75 or 1.5 mg/mL) on collagen sponge
- 1.5 mg/mL group: 44% reduction in risk of secondary intervention (RR 0.56, 95% CI 0.40-0.78, p=0.0005)
- Significantly faster fracture and wound healing; fewer infections in Gustilo type-III injuries (p=0.0219)
- Dose-dependent effect (1.5 mg/mL superior to 0.75 mg/mL)
Emerging Safety Concerns - Critical Review of Industry Trials
- Systematic review comparing 13 industry-sponsored rhBMP-2 publications (780 patients) with FDA data and follow-up studies
- Original trials reported 0% rhBMP-2-associated adverse events; true rate estimated at 10-50% depending on approach
- Anterior cervical fusion: ~40% increased early adverse-event risk including life-threatening airway events
- Higher rhBMP-2 doses associated with greater apparent risk of new malignancy; methodological bias against autograft controls
Independent IPD Meta-Analysis (YODA Project)
- Individual-patient-data analysis of 17 industry studies (13 RCTs, 31 cohorts) via the Yale Open Data Access project
- For lumbar fusion, rhBMP-2 and iliac crest autograft were similar in fusion and overall success (77-93% at 24 months)
- Anterior cervical fusion: increased wound complications and dysphagia with rhBMP-2
- Increased 24-month cancer risk with rhBMP-2 (RR 3.45, 95% CI 1.98-6.00), though event rates were low and heterogeneous