Obstetric Plexopathy | Erb's and Klumpke's | Early Referral
Narakas Classification
Critical Must-Knows
- Definition: Stretch injury to the brachial plexus during delivery. Usually traction on the head-neck angle.
- Erb-Duchenne (C5-C6): 'Waiter's Tip' - Shoulder adducted, Elbow extended, Forearm pronated, Wrist flexed.
- Klumpke (C8-T1): 'Claw Hand' - Intrinsic weakness. Often associated with Horner's syndrome (T1 avulsion).
- Observation Window: Most recover spontaneously by 3-6 months. Surgery considered if no biceps function by 3-6 months.
- Shoulder Sequelae: Posterior dislocation (internal rotation contracture) is the major late complication.
Clinical Pearls
- "Biceps recovery by 3 months predicts good overall recovery (Gilbert criteria).
- "Horner's syndrome (ptosis, miosis, anhidrosis) indicates T1 root avulsion - poor prognosis.
- "Late sequelae are primarily at the SHOULDER (Medial rotation contracture, posterior dislocation).
- "MRI of plexus is useful to identify root avulsions (pseudomeningoceles).
Clinical Imaging
Imaging Gallery

BPBP Pitfalls
Missed Fracture
Rule out Clavicle/Humerus fracture. Pseudoparalysis from pain mimics BPBP. X-ray essential.
Internal Rotation Contracture
The Silent Dislocator. Progressive internal rotation contracture leads to posterior shoulder subluxation. Monitor and stretch.
Delayed Referral
Window for Nerve Surgery is 3-6 Months. Delayed referral misses the optimal timing for nerve graft/transfer.
The 'Recovered' Child
Hidden Deficits. Even with good recovery, subtle weakness and Glenohumeral Dysplasia can progress. Long-term follow-up.
At a Glance: Erb's vs Klumpke's
| Feature | Erb-Duchenne (C5-C6) | Klumpke (C8-T1) |
|---|---|---|
| Frequency | 80-90% | Less than 5% |
| Posture | Waiter's Tip (Adducted, Pronated) | Claw Hand (Intrinsic minus) |
| Key Losses | Deltoid, Biceps, Supinator | Intrinsics, Finger Flexors |
| Horner's | No | Yes (if T1 avulsed) |
| Prognosis | Good (Majority recover) | Poor (Often permanent) |
AIPEFWaiter's Tip Posture
| A | Adducted Shoulder Adducted (Weak Deltoid) |
| I | Internally Rotated Shoulder Internally Rotated (Weak Infraspinatus) |
| P | Pronated Forearm Pronated (Weak Supinator/Biceps) |
| E | Extended Elbow Extended (Weak Biceps) |
| F | Flexed Wrist Wrist Flexed (Weak Wrist Extensors if C7) |
| A | Adducted Shoulder Adducted (Weak Deltoid) | E | Extended Elbow Extended (Weak Biceps) |
| I | Internally Rotated Shoulder Internally Rotated (Weak Infraspinatus) | F | Flexed Wrist Wrist Flexed (Weak Wrist Extensors if C7) |
| P | Pronated Forearm Pronated (Weak Supinator/Biceps) |
Hook:Erb's Palsy Posture.
Robert Taylor Drinks Cold BeerBrachial Plexus Roots
| R | Roots C5, C6, C7, C8, T1 |
| T | Trunks Upper, Middle, Lower |
| D | Divisions Anterior, Posterior (each trunk) |
| C | Cords Lateral, Posterior, Medial |
| B | Branches Terminal Nerves |
| R | Roots C5, C6, C7, C8, T1 | C | Cords Lateral, Posterior, Medial |
| T | Trunks Upper, Middle, Lower | B | Branches Terminal Nerves |
| D | Divisions Anterior, Posterior (each trunk) |
Hook:Anatomy of the Plexus.
1, 2, 3, Horner'sNarakas Types
| I | C5-C6 Erb's (Shoulder/Elbow) |
| II | C5-C7 Extended Erb's (+Wrist/Fingers) |
| III | C5-T1 Total (Flail Arm) |
| IV | +Horner's Total + Root Avulsion (Worst) |
| I | C5-C6 Erb's (Shoulder/Elbow) | III | C5-T1 Total (Flail Arm) |
| II | C5-C7 Extended Erb's (+Wrist/Fingers) | IV | +Horner's Total + Root Avulsion (Worst) |
Hook:Narakas Classification.
Overview and Epidemiology
Definition: Brachial Plexus Birth Palsy (BPBP), also known as Obstetric Brachial Plexus Injury (OBPI), is a stretch injury to the brachial plexus occurring during delivery. It results from lateral flexion of the head away from the shoulder, causing traction on the plexus.
Epidemiology:
- Incidence: 1-2 per 1000 live births.
- Risk Factors: Shoulder dystocia, Macrosomia, Forceps/Vacuum delivery, Breech presentation.
- Recovery: Approximately 80-90% recover spontaneously, often fully or with minimal residual deficit.
Neuroanatomical Pattern:
- Upper Plexus (Erb's - C5, C6 +/- C7): Most common (80-90%). Best prognosis.
- Lower Plexus (Klumpke's - C8, T1): Rare in isolation (less than 5%). Associated with Horner's.
- Total Plexus (C5-T1): Flail arm. Worst prognosis.
Pathophysiology and Mechanisms
Plexus Anatomy: The brachial plexus is formed by the ventral rami of C5-T1. It has 5 components (Roots, Trunks, Divisions, Cords, Branches).
- Upper Trunk: C5, C6.
- Middle Trunk: C7.
- Lower Trunk: C8, T1.
- Key Nerve Outputs: Musculocutaneous (Biceps), Axillary (Deltoid), Radial (Triceps/Wrist Extensors), Median (Forearm Flexors/Thenar), Ulnar (Intrinsics/Hypothenar).
Injury Mechanisms:
- Stretch/Neurapraxia: Temporary conduction block. Full recovery expected.
- Rupture: Nerve disrupted distal to DRG. Scar formation. May need grafting.
- Avulsion: Root torn from spinal cord. No spontaneous recovery. Requires nerve transfer.
Pathophysiology of Late Shoulder Deformity: Muscle imbalance (Strong internal rotators vs Weak external rotators) leads to:
- Internal rotation contracture.
- Posterior subluxation of glenohumeral joint.
- Glenoid retroversion, posterior humeral head flattening.
- Ultimately, Glenohumeral Dysplasia (GHD).
Classification
Narakas Classification
Based on clinical pattern and root involvement.
| Type | Roots | Presentation | Prognosis |
|---|---|---|---|
| I | C5-C6 | Erb's. Shoulder/Elbow weak. | Good (greater than 90% recover) |
| II | C5-C7 | Extended Erb's. +Wrist/Finger Ext weak | Good (70-80% recover) |
| III | C5-T1 | Total. Flail arm. | Guarded (20-30% recover) |
| IV | C5-T1 + Horner's | Total + Root Avulsion | Poor (No spontaneous recovery if avulsion) |
Horner's Syndrome (Ptosis, Miosis, Anhidrosis) indicates T1 root avulsion.
Clinical Assessment
Initial Exam (Newborn):
- Posture: Waiter's Tip? Flail? Claw?
- Passive ROM: Full in newborn (to exclude contracture or fracture).
- Reflexes: Moro (abducted arm doesn't follow), Grasp (if lower plexus involved).
- Horner's Syndrome: Ptosis, Miosis, Anhidrosis.
- Rule Out Fracture: Clavicle, Humerus (Pseudoparalysis). Order X-ray.
Serial Assessment:
- Active Movement: Use Active Movement Scale (AMS). 0-7 per muscle.
- Key Milestone: Biceps recovery. If antigravity biceps by 3-6 months, expect good recovery (Gilbert).
- Shoulder ROM: Monitor for internal rotation contracture (External Rotation deficit).
- Later: Mallet Classification for shoulder function.
Mallet Classification (Shoulder Function): Grades shoulder function (Abduction, External Rotation, Hand to Mouth, etc.).
- Grade I: Flail shoulder.
- Grade V: Normal.
- Grade II-IV: Intermediate.
Investigations
Imaging:
- X-ray (Clavicle, Humerus): Initial. Rule out fracture.
- MRI Brachial Plexus: If no recovery by 3 months. Look for pseudomeningoceles (root avulsion), neuroma.
- Ultrasound Shoulder: Assess glenohumeral joint if internal rotation contracture. Look for posterior subluxation, glenoid retroversion.
- CT Shoulder (3D): For surgical planning in older children with GHD.
Electrodiagnostics:
- EMG/NCS: Can differentiate neurapraxia from axonotmesis/avulsion. Often used to supplement clinical exam.
- Timing: 3-4 weeks after injury (for fibrillation potentials).
Differential Diagnosis
The flaccid or under-moving newborn arm has several mimics. The single most important step is to exclude a painful pseudoparalysis (fracture, infection) before attributing weakness to plexopathy.
Differential Diagnosis of the Newborn 'Weak Arm'
| Condition | Distinguishing Features | Key Test |
|---|---|---|
| Brachial plexus birth palsy | Posture-specific weakness (waiter's tip / claw), normal passive ROM, +/- Horner's | Serial Active Movement Scale |
| Clavicle fracture | Crepitus, palpable callus, pain on movement, full recovery in 1-2 weeks | Clavicle radiograph |
| Proximal humeral physeal separation | Pseudoparalysis, swelling, pain; epiphysis unossified so radiograph subtle | Ultrasound / radiograph |
| Septic arthritis / osteomyelitis (shoulder) | Pseudoparalysis with systemic signs, fever, raised inflammatory markers | Ultrasound, aspiration, bloods |
| Cervical spinal cord injury | Bilateral involvement, lower-limb signs, sphincter/respiratory compromise | MRI cervical cord |
| Hemiplegic cerebral palsy | Emerges later, hypertonia and hyperreflexia, hand fisting, no birth event | Neurological follow-up |
| Arthrogryposis / congenital deficiency | Bilateral, fixed contractures from birth, normal sensation | Clinical, passive ROM |
Management Algorithm
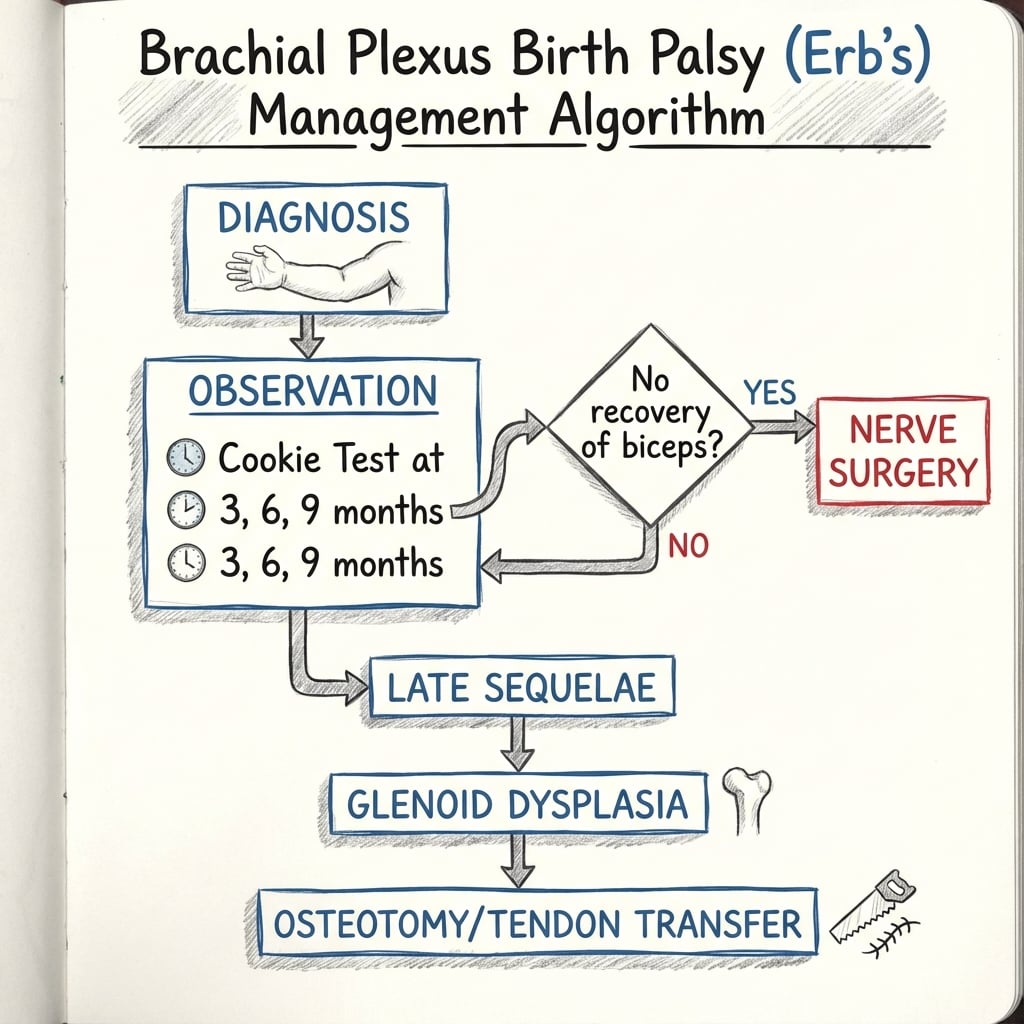
Early Management (0-3 Months)
- Parental Reassurance: Majority recover spontaneously.
- Gentle ROM Exercises: Prevent contracture. Physio referral.
- Positioning: Avoid adduction contracture. Full ROM.
- Serial Exam: AMS at each visit. Document biceps recovery.
- Referral: If no biceps recovery by 3 months, refer to a BPBP specialist center.
Splinting is generally NOT indicated in BPBP.

Surgical Technique
Release and Transfer (Shoulder)
For Internal Rotation Contracture.
Anterior Subscapularis Release (Modified Carlioz):
- Indication: Internal Rotation Contracture greater than 20 degrees, Mallet III or less.
- Approach: Anterior axillary incision.
- Procedure: Release Subscapularis from humerus (lengthen or slide).
- Post-op: Immobilize in External Rotation (Spica or Shoulder Immobilizer) for 6 weeks.
L'Episcopo / Mod Sever-L'Episcopo:
- Indication: Weak External Rotation (Mallet II-III).
- Procedure: Transfer Latissimus Dorsi and Teres Major to the posterior humerus (act as External Rotators).
- Post-op: Similar. External Rotation immobilization.
Often combined: Release + Transfer.
Complications
Key Complications
| Complication | Cause | Management |
|---|---|---|
| Glenohumeral Dysplasia | Muscle imbalance, Internal Rotation Contracture | Early release, Osteotomy |
| Posterior Dislocation | Progressive dysplasia | Reduction + Bony Reconstruction |
| Internal Rotation Contracture | Weak ER, Strong IR | Stretching, Subscap Release |
| Elbow Flexion Weakness | Poor biceps recovery | Nerve transfer / Steindler |
| Co-Contraction | Abnormal re-innervation | Botox, Selective Transfer |
Glenohumeral Dysplasia (GHD): The major late complication. Characterized by:
- Glenoid retroversion.
- Posterior subluxation of humeral head.
- Flattening of humeral head.
- Eventual osteoarthritis.
Postoperative Care
- Nerve Surgery: Sling/Shoulder Immobilizer. Gentle ROM at 4-6 weeks. Expect recovery over 12-18 months.
- Tendon Transfer/Release: External Rotation Immobilization (Spica or Brace) for 6 weeks. Intensive physio after.
- Osteotomy: Sling. ROM as tolerated. Bone healing in 6-8 weeks.
Outcomes

- Erb's (Type I): Greater than 90% recover good function (Mallet IV-V).
- Total Palsy (Type III/IV): Poor prognosis. Permanent deficits common.
- Nerve Surgery: Improves function significantly but rarely restores normal.
- Long-term: Shoulder problems (GHD, OA) are the main late issues.
Controversies & Areas of Uncertainty
True Recovery Rate
The classic "90% recover" figure is challenged. Methodologically rigorous natural-history data (Pondaag systematic review) suggest full recovery may be closer to two-thirds, with a meaningful minority left with deficits. Over-reassurance risks late referral.
Timing of Nerve Surgery
No biceps by 3 months (Gilbert/Paris) versus a multi-movement composite at 3 months (Toronto/Clarke) versus waiting to 6 months for partial recovery. No randomised trial has resolved the optimal threshold; practice varies by centre.
Role of Microsurgery vs Watchful Waiting
The absence of randomised data comparing primary nerve reconstruction with continued observation in incomplete upper-trunk lesions remains the field's biggest evidence gap. Decisions rest on cohort data and serial examination.
Glenohumeral Dysplasia: Early Intervention
How early to intervene for posterior subluxation - botulinum toxin, closed reduction and casting, arthroscopic versus open release, and the place of glenoid osteotomy - is debated. Earlier joint reduction may remodel the glenoid, but thresholds are not standardised.
Evidence Base
Toronto Test Score & Natural History
- 66 infants reviewed; 61 (92%) recovered spontaneously, 5 (8%) required primary plexus exploration.
- Elbow flexion at 3 months alone mispredicted final recovery in 12.8% of cases.
- A combined test score (elbow flexion + elbow/wrist/thumb/finger extension) reduced misprediction to 5.2%.
Natural History Systematic Review
- Systematic review of natural-history studies of obstetric brachial plexus palsy.
- Methodologically robust studies suggest full spontaneous recovery is closer to 66%, lower than the often-quoted 90%.
- Heterogeneous outcome definitions inflate reported recovery rates.
Oberlin Transfer (Original Description)
- Four patients with C5-C6 root avulsion treated by transfer of ~10% of the ulnar nerve to the biceps motor branch.
- Restored elbow flexion with no significant impairment of hand function.
- Established intraplexal fascicular transfer as an alternative to long nerve grafts.
Double Fascicular Transfer for Elbow Flexion
- 15 patients had ulnar-to-biceps plus median-to-brachialis double transfer; 10 had at least 6 months follow-up.
- Grade 4 (MRC) elbow flexion restored in all 10 followed patients, lifting 1-5 kg.
- No secondary deficit in grip strength or sensation.
Glenohumeral Deformity: Natural History
- Prospective study; mean glenoid retroversion (glenoscapular angle) -25.7 degrees on the affected side versus -5.5 degrees on the unaffected side.
- 26 of 42 shoulders (62%) showed posterior subluxation of the humeral head on CT/MRI.
- Deformity progressed significantly with increasing age (p less than 0.001).
Shoulder Reconstruction Outcomes
- Case-control comparison of tendon transfer versus rotational humeral osteotomy, selected by age and degree of deformity.
- Global Mallet scores improved from 9.5 to 15.6 after tendon transfer and from 9.5 to 15.1 after osteotomy.
- Both procedures predictably improve shoulder function when matched to the deformity.
Epidemiology & Declining Incidence
- Swedish population registry (1997-2019): OBPP in cephalic vaginal births fell from 3.1 to 1.0 per 1000 (OR 0.31).
- Shoulder dystocia incidence rose over the same period (2.0 to 3.3 per 1000), yet OBPP still declined.
- Falling macrosomia and operative vaginal delivery explained only a small fraction of the decline.
Narakas Classification
- Defined the four-group clinical classification (Groups I-IV) by root involvement.
- Correlated extent of injury with prognosis; Group IV (total palsy with Horner's) carries the worst outlook.
- Remains the standard prognostic grouping at presentation.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Newborn with Arm Weakness
"What is your assessment and initial management?"
The Stiff Shoulder
"What is your assessment and management plan?"
The Infant with No Recovery
"Discuss prognosis and management."
MCQ Practice Points
Erb's Posture
Q: What is the classic posture in Erb-Duchenne palsy? A: Waiter's Tip - Shoulder Adducted and Internally Rotated, Elbow Extended, Forearm Pronated, Wrist Flexed.
Key Recovery Predictor
Q: What is the most important clinical predictor of good outcome in BPBP? A: Biceps recovery (antigravity elbow flexion) by 3-6 months.
Horner's Syndrome
Q: What does the presence of Horner's Syndrome indicate in BPBP? A: T1 root avulsion. Indicates poor prognosis (no spontaneous recovery of avulsed root). Nerve transfer required.
Major Late Complication
Q: What is the major late orthopedic complication of BPBP? A: Glenohumeral Dysplasia (GHD) - posterior subluxation and glenoid retroversion due to internal rotation contracture.
Oberlin Transfer
Q: What is the Oberlin procedure? A: A nerve transfer where a fascicle of the Ulnar nerve is transferred to the Musculocutaneous nerve (Biceps branch) to restore elbow flexion.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Incidence approximately 1-2 per 1000 live births, falling in high-resource settings. A Swedish national registry recorded a decline from 3.1 to 1.0 per 1000 cephalic vaginal births between 1997 and 2019 despite rising recognition of shoulder dystocia (PMID 36345990).
- Risk factors: shoulder dystocia, fetal macrosomia, maternal gestational diabetes, instrumental (forceps/vacuum) delivery, prolonged second stage, and breech delivery. Notably, a proportion of cases occur without documented dystocia (including caesarean births), implicating in-utero maladaptation.
- Upper-trunk (Erb's) pattern accounts for roughly 80-90% of cases and carries the best prognosis.
Side-by-Side Guidance:
Practice Frameworks Across Societies
| Body / Framework | Position on Referral & Surgery | Emphasis |
|---|---|---|
| ACOG (US, obstetric) | Shoulder dystocia drills; document delivery; no routine caesarean for suspected macrosomia alone | Prevention and obstetric documentation |
| RCOG / BOA (UK) | Early referral to a specialist plexus service; structured therapy pathway | Multidisciplinary specialist referral |
| Narakas-Gilbert (Paris school) | Explore if no biceps by 3 months | Earliest microsurgical threshold |
| Clarke/Toronto school | Composite Active Movement Scale; operate if score below threshold at 3 months | Quantified serial assessment |
| AAOS / POSNA (US, paediatric ortho) | Surveillance for glenohumeral dysplasia; timely shoulder reconstruction | Long-term shoulder outcomes |
Service Organisation & Resource Variation:
- High-resource settings: dedicated multidisciplinary plexus clinics (paediatric hand/peripheral-nerve surgery, physiotherapy, occupational therapy), early MRI and microsurgical capability, and structured glenohumeral surveillance.
- Limited-resource settings: emphasis on prevention (dystocia training, gestational diabetes screening), parent-delivered range-of-motion therapy, and clear referral pathways; advanced microsurgery and secondary reconstruction may be regionally centralised or unavailable, making timely triage critical.
- Universal principles: exclude a fracture, protect passive range of motion, document serial active movement, refer early if recovery stalls, and monitor lifelong for shoulder dysplasia regardless of setting.
Clinical summary
Patterns
- •Erb's: C5-C6 (Waiter's Tip)
- •Extended Erb's: C5-C7
- •Klumpke: C8-T1 (Claw Hand)
- •Total: C5-T1 (Flail)
- •Horner's: T1 Avulsion
Key Milestones
- •Biceps by 3 months: Good
- •No Biceps by 6mo: Surgery
- •90% Erb's Recover
- •Horner's = Poor Prognosis
Surgery
- •Nerve Graft (Rupture)
- •Nerve Transfer (Avulsion)
- •Subscap Release (Contracture)
- •L'Episcopo (Weak ER)
- •Osteotomy (Fixed Posture)
Red Flags
- •Rule out Clavicle Fracture
- •Horner's = T1 Avulsion
- •Refer early (by 3mo)
- •Monitor for GHD