Congenital Short Metatarsal
- Brachymetatarsia is a congenitally SHORT METATARSAL, most often caused by PREMATURE CLOSURE of the metatarsal physis (growth plate); the FOURTH metatarsal is the most commonly affected, the condition is more common in FEMALES, is frequently BILATERAL, and has recognised syndromic associations (e.g. pseudohypoparathyroidism/pseudo-pseudohypoparathyroidism, Down syndrome, Turner syndrome, Apert syndrome).
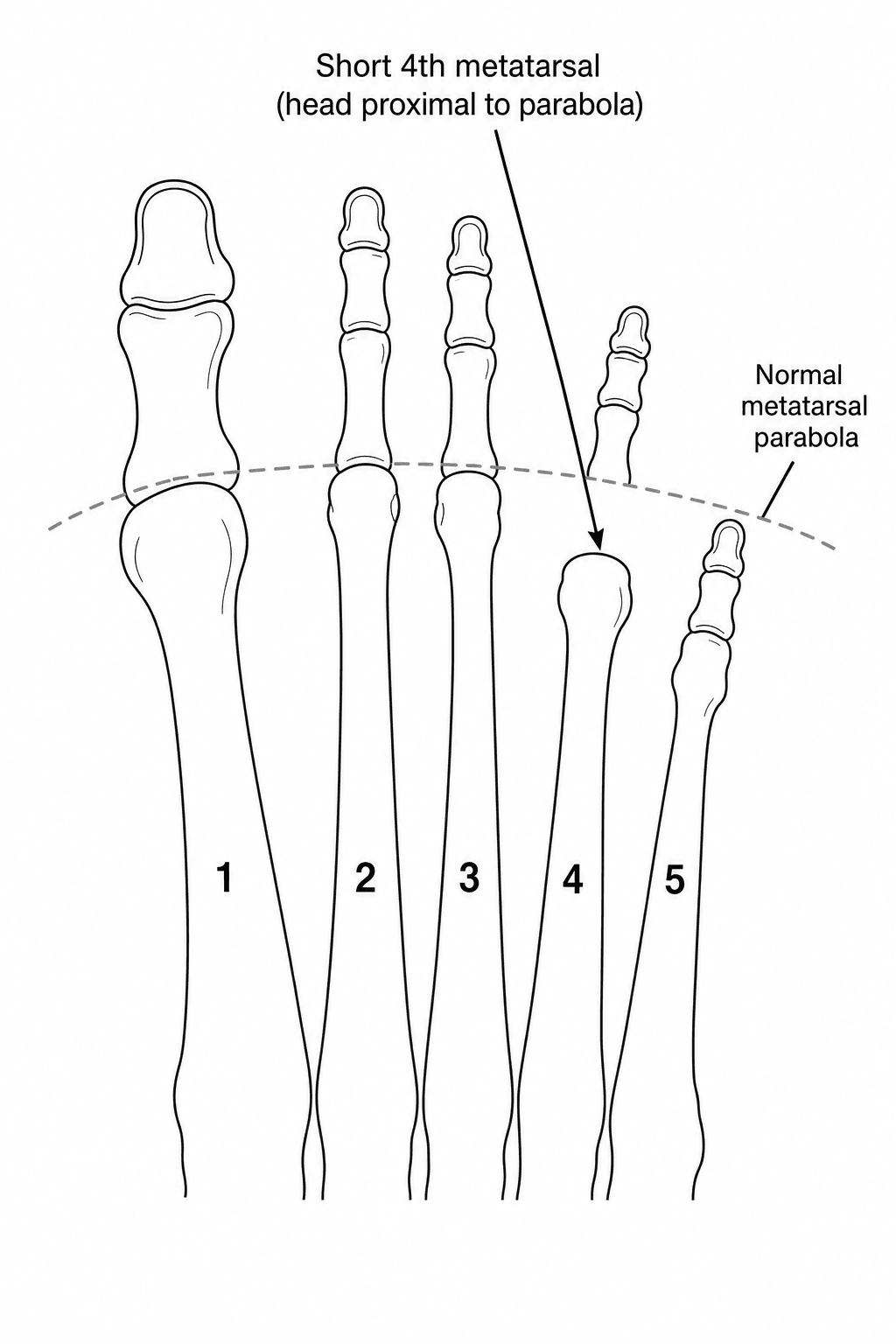
- The short metatarsal disrupts the normal METATARSAL PARABOLA (the smooth cascade of metatarsal head lengths), so the affected metatarsal head sits PROXIMAL to the parabola and the corresponding TOE is SHORTENED and typically rides DORSALLY (it sits up out of the line of the other toes).
- Most patients present with COSMETIC concern and difficulty with footwear; some develop TRANSFER METATARSALGIA, with pain under the adjacent metatarsal heads because the short ray does not share the weight-bearing load, and the dorsally-displaced toe can rub in shoes.
- DIAGNOSIS is clinical plus a weight-bearing AP foot RADIOGRAPH, which shows the short metatarsal with its head proximal to the metatarsal parabola and the disrupted cascade; the contralateral foot is compared, and the degree of shortening (and the planned lengthening) is measured.
- MANAGEMENT of the ASYMPTOMATIC patient is reassurance and shoe modification; for SYMPTOMATIC or cosmetically-distressing cases, surgical LENGTHENING is offered, by one of two strategies - a ONE-STAGE lengthening with an interpositional bone graft, or GRADUAL lengthening by distraction osteogenesis (CALLOTASIS) using a mini-external fixator after a metatarsal osteotomy.
- The TRADE-OFFS between techniques are key: ONE-STAGE bone grafting gives a LIMITED length gain and the SHORTEST fixation time but carries the risk of acute neurovascular/soft-tissue stretch (limiting how much length is safe) and somewhat lower satisfaction; GRADUAL distraction (callotasis) achieves GREATER length gain WITH concomitant soft-tissue lengthening and a lower neurovascular risk, but requires a prolonged period in an external fixator - with the most reliable results reported for gradual distraction after an osteotome (rather than saw) osteotomy; complications include stiffness/MTP subluxation, nonunion/failure of bone formation, malunion and pin-site problems.
- “Brachymetatarsia = congenitally short metatarsal (premature physeal closure); FOURTH metatarsal most common; female predominance, often bilateral; syndromic associations (pseudohypoparathyroidism, Down, Turner, Apert).
- “Disrupts the metatarsal PARABOLA -> short, dorsally-riding toe; cosmetic/footwear concern + transfer metatarsalgia. Weight-bearing AP radiograph shows the short metatarsal proximal to the cascade.
- “Symptomatic -> LENGTHENING: ONE-STAGE interpositional bone graft (limited gain, faster) vs GRADUAL distraction/callotasis (greater length + soft-tissue lengthening, lower neurovascular risk, longer in fixator). Watch stiffness/MTP subluxation, nonunion, malunion.
A congenitally short metatarsal (usually the 4th, from premature physeal closure) disrupting the metatarsal parabola - the toe is short and rides dorsally. Often female/bilateral.
Asymptomatic -> shoe modification. Symptomatic/cosmetic -> lengthening: one-stage graft (limited) vs gradual distraction/callotasis (greater length, lower neurovascular risk).
Cause, Presentation & Diagnosis
Brachymetatarsia is a congenitally short metatarsal, usually from premature physeal closure; the fourth metatarsal is most commonly affected, it is more common in females, often bilateral, and has syndromic associations (pseudohypoparathyroidism, Down, Turner, Apert). The short metatarsal disrupts the metatarsal parabola, so its head sits proximal and the toe is short and rides dorsally. Most present with cosmetic and footwear concerns, some with transfer metatarsalgia under the adjacent heads. Diagnosis is clinical plus a weight-bearing AP radiograph showing the short metatarsal proximal to the cascade. Asymptomatic patients need only reassurance/shoe modification; symptomatic or cosmetically-distressing cases are offered surgical lengthening - a one-stage interpositional bone graft or gradual distraction (callotasis) with a mini-external fixator.
- Length gain / soft tissue
- Limited gain; acute (no gradual soft-tissue lengthening)
- Trade-offs
- Shortest fixation time; risk of neurovascular/soft-tissue stretch; somewhat lower satisfaction
- Length gain / soft tissue
- Greater gain WITH concomitant soft-tissue lengthening
- Trade-offs
- Lower neurovascular risk; prolonged time in fixator; pin-site issues
- Length gain / soft tissue
- Osteotome (vs saw) osteotomy
- Trade-offs
- Osteotome-based distraction reported most reliable (fewer non-formations)
Lengthening: One-Stage vs Gradual
- Asymptomatic: reassurance and shoe modification - surgery is for symptoms or significant cosmetic distress, not for the radiograph alone.
- One-stage interpositional bone graft: a single procedure with an interpositional graft - limited length gain and the shortest fixation time, but acute lengthening risks neurovascular/soft-tissue stretch, so the amount of lengthening is limited.
- Gradual distraction osteogenesis (callotasis): a metatarsal osteotomy and mini-external fixator with gradual distraction - achieves greater length gain WITH concomitant soft-tissue lengthening and a lower neurovascular risk, at the cost of a prolonged period in the fixator; distraction after an osteotome (rather than saw) osteotomy gives the most reliable bone formation.
- Anticipate complications: stiffness and MTP joint subluxation, nonunion/failure of bone formation, malunion, and pin-site problems; protect the MTP joint and lengthen within safe limits.
The key surgical principle in brachymetatarsia lengthening is that the SOFT TISSUES and the neurovascular bundle limit how much length can be gained acutely: a one-stage interpositional bone graft is quicker and needs the shortest fixation, but the acute stretch restricts the safe length gain and risks neurovascular/soft-tissue compromise and MTP stiffness, so it suits cases needing only limited lengthening. When greater length is required, gradual distraction osteogenesis (callotasis) is preferred, because lengthening the bone slowly allows the soft tissues to lengthen with it, achieving a greater gain with a lower neurovascular risk - the trade-off being a prolonged time in an external fixator. Across techniques, watch for MTP subluxation/stiffness, nonunion or failure of bone formation, and malunion, and remember that surgery is reserved for symptomatic or significantly cosmetically-distressing patients - the asymptomatic short metatarsal is managed conservatively.
Planning the Lengthening: How Much, How Fast
- Quantify the deficit: on the weight-bearing AP, the target is to restore the affected metatarsal head to the normal metatarsal parabola (the smooth cascade), judged against the adjacent metatarsals and the contralateral normal foot; this defines the required lengthening, which in brachymetatarsia is often substantial (commonly more than a centimetre).
- The acute-lengthening limit: one-stage interpositional grafting is limited because the constraint is acute stretch of the digital nerves and vessels - acute gains beyond roughly 15% of the metatarsal length (a small absolute amount) risk neurovascular compromise and stiffness, so one-stage suits small deficits only.
- Callotasis parameters (the brachymetatarsia application of distraction osteogenesis): after a low-energy osteotome osteotomy (more reliable than a saw), a latency of about a week, then distraction at roughly 0.5 to 1 mm per day in divided increments, followed by a consolidation phase in the fixator until the regenerate corticates. The healing index (time in fixator per centimetre gained) is higher (slower) for first than fourth brachymetatarsia, because of the larger osteotomy surface and weight-bearing.
(The general principles of distraction osteogenesis and limb lengthening are covered in our Distraction Osteogenesis and Limb Lengthening topics, and the parabola in our Metatarsalgia topic; the point here is the brachymetatarsia-specific planning and limits.)
Plan against the metatarsal parabola (and the contralateral foot). One-stage grafting is limited to small deficits (acute gains beyond roughly 15% risk the neurovascular bundle); callotasis - osteotome osteotomy, about a week's latency, 0.5 to 1 mm per day, then consolidation - achieves more, and the healing index is slower for first than fourth brachymetatarsia.
Protecting the MTP Joint & the Toe
- During lengthening the MTP joint is dragged distally and the already dorsally-riding toe is at real risk of dorsal subluxation/dislocation and stiffness - so the joint is protected, commonly with a temporary axial Kirschner wire across the MTP joint (and sometimes down the toe) during distraction and consolidation to hold the reduction and resist subluxation, removed afterwards.
- Soft-tissue adjuncts: a dorsal capsulotomy and extensor (sometimes flexor) lengthening or release may be needed as the ray lengthens, and any associated syndactyly/webbing or toe deformity addressed - although gradual distraction itself reduces the need by lengthening the soft tissues with the bone.
- Post-operatively: a supervised distraction schedule, pin-site care, and early MTP range-of-motion physiotherapy to combat stiffness, with weight-bearing modified during consolidation.
(Associated toe deformities are covered in our Lesser Toe Deformities topic; the point here is protecting the MTP joint during lengthening.)
Protect the MTP joint during lengthening with a temporary axial K-wire (it is dragged distally and the dorsal toe subluxes), add a dorsal capsulotomy/extensor lengthening if the ray will not come out, address any syndactyly, and drive early MTP range-of-motion with pin-site care to limit stiffness.
Selecting the Patient, and the Complications to Consent For
The operation is elective, technically demanding and carries a real complication burden, so who is offered it matters as much as how it is done.
- The indication is usually a combination, not pure appearance: difficulty with footwear, a transfer lesion or metatarsalgia under the adjacent heads, a dorsally riding or non-functional toe, and distress about the appearance of the foot. Purely cosmetic requests deserve a frank discussion of the complication rate, the months in a fixator and the realistic aesthetic result.
- Non-operative management is legitimate and often chosen: accommodative footwear with a wide toe box, metatarsal padding or a bar to offload the transfer lesion, and a toe prop or sleeve for a floating toe. Many patients, once the alternative is explained, prefer this.
- Timing. Lengthening is generally deferred until skeletal maturity, since the causative physis has usually closed prematurely and operating earlier risks further growth of the adjacent rays altering the parabola again.
- Floating toe is the characteristic functional disappointment: the lengthened toe sits clear of the ground and takes no load, because tendon length and MTP mechanics have not kept pace with the bone. It is more likely after large gains and is a specific thing to warn about, because the foot may look better while the toe still does nothing.
- The complications worth consenting for, in the order they actually occur: MTP stiffness (the commonest), dorsal MTP subluxation, pin-site infection, premature consolidation or a poor/insufficient regenerate requiring re-osteotomy or grafting, malunion or axial deviation of the lengthening ray, nonunion, neurovascular compromise if distraction is too rapid, floating toe, and an aesthetic result the patient does not consider worth it.
Mnemonics & Memory Aids
SHORT
Hook:SHORT: Short 4th metatarsal, Heritable/syndromic, Out of parabola (dorsal toe), Radiograph, Treat by lengthening (one-stage vs callotasis).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is brachymetatarsia and how does it present?”
“What are the surgical options to lengthen a short metatarsal, and how do you choose?”
What & cause
- Congenitally short metatarsal (premature physeal closure)
- Fourth metatarsal most common; female predominance; often bilateral
- Syndromic associations: pseudohypoparathyroidism, Down, Turner, Apert
Presentation
- Disrupted metatarsal parabola; short toe rides dorsally
- Cosmetic and footwear concern; transfer metatarsalgia in some
- Weight-bearing AP radiograph (short metatarsal proximal to the cascade)
Management
- Asymptomatic -> reassurance / shoe modification
- Symptomatic/cosmetic -> surgical lengthening
- One-stage interpositional graft (limited) vs gradual distraction/callotasis (greater length)
Technique & complications
- Gradual distraction: greater length + soft-tissue lengthening, lower neurovascular risk (longer in fixator)
- Distraction after osteotome (vs saw) osteotomy most reliable
- Complications: MTP stiffness/subluxation, nonunion/failure of bone formation, malunion, pin-site issues
Evidence & Key Studies
Lengthening of fourth brachymetatarsia by three different surgical techniques
- In 153 feet, the fourth metatarsal was lengthened by one-stage intercalary bone grafting, or by gradual distraction with a mini-external fixator after either a saw or an osteotome osteotomy.
- Gradual distraction achieved greater length than one-stage grafting; the one-stage bone-graft group had the shortest fixation time but more dissatisfaction, while the saw group had failures of bone formation.
- Gradual lengthening by distraction osteogenesis after an osteotome osteotomy gave the most reliable results.
Metatarsal lengthening by callotasis in first brachymetatarsia
- One-stage lengthening with an autologous bone graft is preferred for metatarsals requiring limited lengthening, whereas gradual lengthening by callus distraction (callotasis) achieves a greater length gain with concomitant soft-tissue lengthening.
- In adults with first brachymetatarsia treated by callotasis, the average length gain was about 16 mm (around 44%).
- Bony consolidation took longer in first than in fourth brachymetatarsia (a higher healing index), attributed to the larger osteotomy surface and weight-bearing function.
The comparison of lengthening techniques for fourth brachymetatarsia (gradual distraction achieving greater length than one-stage grafting, the one-stage graft having the shortest fixation but more dissatisfaction, and distraction after an osteotome osteotomy being most reliable) comes from the cited Lee study; the principle that one-stage grafting suits limited lengthening while callotasis achieves greater gain with soft-tissue lengthening, and the slower consolidation of first brachymetatarsia, from the cited Hwang study. The fourth-metatarsal predominance, the premature-physeal-closure cause, the female/bilateral/syndromic associations, the disrupted metatarsal parabola, and the conservative-for-asymptomatic approach are standard, well-established teaching. (See also our Metatarsalgia and Distraction Osteogenesis topics.)