Emergency Diagnosis | CES-I vs CES-R | Urgent Decompression
- CES-I (Incomplete) = altered bladder sensation but control preserved - URGENT surgery to prevent progression
- CES-R (Retention) = painless urinary retention with overflow - poorer prognosis regardless of timing
- MRI is mandatory emergency - do not wait until morning if red flags present
- Post-void residual greater than 500ml is significantly predictive of CES
- Bilateral sciatica + saddle anaesthesia + bladder dysfunction = assume CES until proven otherwise
- “Know Gleave & Macfarlane classification: CES-I vs CES-R distinction is prognostically critical
- “Timing debate: state of patient (CES-I vs R) matters more than exact surgical timing
- “Medico-legal hot topic: 'Better to scan 100 negatives than miss 1 positive'
- “Digital rectal exam is mandatory: assess anal tone AND sensation
Cauda Equina Syndrome
CES-I (Incomplete): Altered sensation but voluntary control preserved. URGENT surgery often prevents progression. CES-R (Retention): Painless retention with overflow. Poorer prognosis regardless of timing.
"Better to scan 100 negatives than miss 1 positive." Low threshold for MRI. This is the most litigated condition in spinal surgery.
Decompression in CES-I is time-critical. Once CES-R occurs, recovery is unpredictable. Do not wait for morning if red flags are present.
Always define the difference between I and R. Examiners look for this distinction immediately.
Anatomy of the Cauda Equina
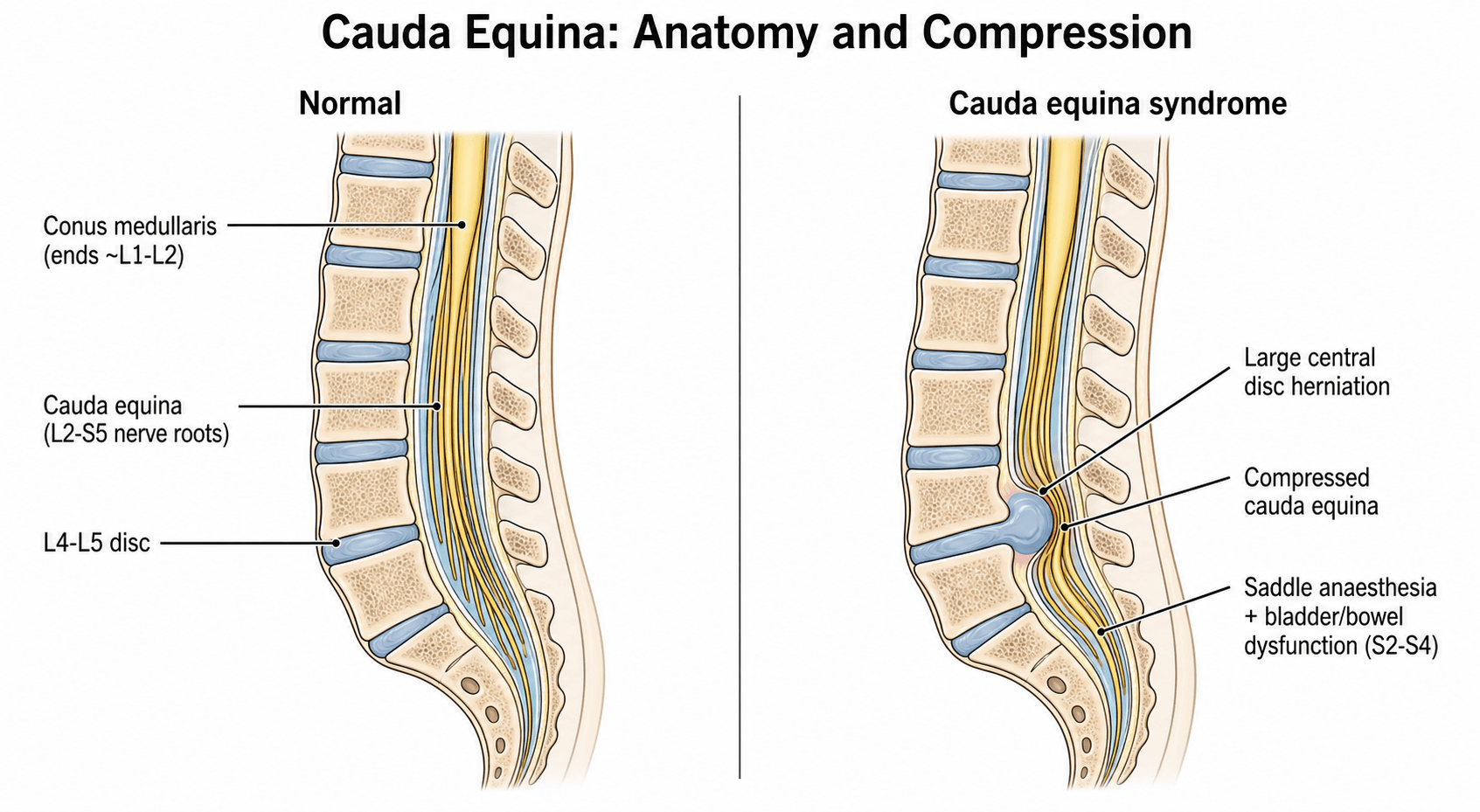
- Collection of nerve roots distal to conus medullaris (which ends at L1/L2 in adults)
- Contains nerve roots L2 to S5
- Provides motor and sensory innervation to legs, perineum, and sphincters
- Contains parasympathetic bladder supply (S2-S4 - "S2, 3, 4 keeps the wee off the floor")
- Nerve roots are tethered within the spinal canal and have less protective connective tissue than peripheral nerves
- Compression compromises intraneural blood flow (venous congestion leading to arterial ischaemia)
- Autonomic fibres to bladder (S2-S4) are most vulnerable due to small diameter and peripheral location
- Sensory fibres affected before motor fibres in early stages
The Micturition Reflex and Neural Control of the Bladder
A viva follow-up in this topic asks you to "describe the micturition reflex and which spinal levels control it", and the bladder picture of CES only makes sense from this circuit. Continence and voiding depend on three nerve supplies coordinated by the brainstem.
Neural Control of the Bladder
CES damages the S2-4 roots - the parasympathetic detrusor supply, the somatic external-sphincter supply and the afferents - producing a LOWER-motor-neuron, areflexic/acontractile (flaccid) bladder: painless retention with overflow and loss of filling sensation, plus reduced anal tone and saddle sensory loss. Contrast this with a SUPRASACRAL cord lesion, which spares the sacral reflex arc and produces an UPPER-motor-neuron, overactive (spastic) bladder, often with detrusor-sphincter dyssynergia. The reflex itself is switched on and off by the pontine micturition centre under cortical control.
Causes of CES and Cause-Specific Management
The demographics, guideline and imaging sections list several causes and state that you must "treat the cause", and the MRI atlas shows a post-operative haematoma and arachnoiditis - but the causes and their differing management are never set out. The first operative question is always "what is compressing the cauda equina?", because the answer changes the operation and the wider work-up.
Causes of Cauda Equina Syndrome
The commonest cause is a disc, but always ask what is doing the compressing, because it redirects the whole pathway: an abscess needs blood cultures and antibiotics, a haematoma needs anticoagulation reversal and rapid evacuation, a metastatic deposit needs dexamethasone, whole-spine imaging and oncology, and arachnoiditis is not a decompression at all. Raised inflammatory markers or a known cancer should immediately broaden the work-up beyond a simple discectomy.
CES Staging - Critical for Prognosis
CES-I vs CES-R Classification
CES-I patients have altered bladder sensation but can still voluntarily void. They often describe needing to strain to urinate, incomplete emptying, or loss of normal desire to void. However, they retain control.
CES-R patients have a paralysed bladder. They develop painless urinary retention (bladder fills without sensation) and overflow incontinence (dribbling when bladder is overfull). This represents established neurological damage.
The transition from CES-I to CES-R is often irreversible - hence the urgency to operate while still CES-I.
Clinical Significance
Cauda equina syndrome (CES) is compression of the cauda equina nerve roots (L2-S5) below the conus medullaris, causing a constellation of lower back pain, unilateral or bilateral sciatica, saddle anaesthesia, and motor/sphincter dysfunction. It represents a surgical emergency requiring urgent decompression.
- Incidence: 0.04% of all lower back pain presentations
- Rarity: 1-2 per 100,000 population annually
- Age: Any age, peak 40-60 years
- Gender: Equal distribution
- Most common cause: Large central lumbar disc herniation (L4/5 or L5/S1)
- Other causes: Tumour, infection (epidural abscess), haematoma, trauma
Despite rarity, high index of suspicion is essential due to catastrophic consequences of missed diagnosis.
- Permanent bladder dysfunction: Up to 50% in CES-R
- Permanent bowel dysfunction: 30-40%
- Sexual dysfunction: Up to 50%
- Chronic pain: Very common
- Litigation: Extremely common for delayed diagnosis
- Quality of life: Severely impacted
Economic and personal burden is substantial. Delayed diagnosis is the leading cause of spine-related litigation.
History
- Onset: Acute vs gradual deterioration
- Back pain: Severity, radiation pattern
- Leg symptoms: Unilateral vs bilateral, dermatomal distribution
- "Can you feel when your bladder is full?"
- "Can you start and stop urinating normally?"
- "Have you had any wetting accidents?"
- "Have you noticed you're not passing urine as often?"
- "Can you feel the paper when wiping?" (S2-S4 sensation)
- "Any change in bowel control?"
- "Can you feel when you need to pass a motion?"
- Sensation changes
- Erectile dysfunction (males)
- Loss of genital sensation (both sexes)
Examination
- Full lower limb motor exam (L2-S1 myotomes)
- Full lower limb sensory exam (L2-S1 dermatomes)
- Reflexes: knee (L3/4), ankle (S1), Babinski
- Light touch sensation in saddle area (S2-S5)
- Pin-prick sensation perineum
- Compare both sides for asymmetry
- Resting anal tone: Assess baseline sphincter tone
- Voluntary squeeze: Ask patient to squeeze examiner's finger
- Perianal sensation: Light touch around anus
- Document findings: Essential for medico-legal purposes
- Palpate suprapubically for distended bladder
- Bladder scan: PVR greater than 200ml suspicious, greater than 500ml highly predictive
Loss of bladder sensation (desire to void) is often the earliest sign of autonomic dysfunction in CES-I, occurring before painless retention. Ask specifically about alteration in sensation, not just ability to urinate.
Clinical Pearl: Subjective change in urinary function is a RED FLAG - do not dismiss.
Emergency Imaging
- Gold Standard investigation for suspected CES
- Must be performed urgently (day or night) if red flags present
- Whole lumbar spine with sagittal and axial T2-weighted sequences
- Look for: Canal occlusion (usually greater than 50-75%), disc herniation level, nerve root compression, other pathology (tumour, abscess)
- If MRI contraindicated (pacemaker, severe claustrophobia)
- Requires lumbar puncture and intrathecal contrast
- Second-line but still diagnostic
- Post-void residual (PVR) measurement
- PVR greater than 200ml: suspicious
- PVR greater than 500ml: highly predictive of CES
- Quick, non-invasive, can be performed at bedside
MRI Imaging Atlas



Differential Diagnosis
Many conditions mimic CES (so-called "scan-negative" or pseudo-CES, where up to 60-70% of emergency MRIs for suspected CES show no compressive lesion). Distinguishing true compressive CES from mimics avoids both missed diagnoses and unnecessary night-time operating.
CES and its Mimics
The conus medullaris (T12-L2 vertebral level) produces an early, symmetrical, mixed UMN/LMN picture with prominent early bladder involvement and sometimes preserved reflexes. The cauda equina produces an asymmetrical, purely LMN, areflexic picture with radicular leg pain. Both are emergencies, but examiners frequently test the anatomical distinction.
Management Algorithm
- Full history and examination (including DRE)
- Bladder scan for PVR
- Catheterise if retention confirmed (document volume - medico-legal)
- Keep nil by mouth in anticipation of surgery
- Analgesia (avoid masking neurological progression)
- Request EMERGENCY MRI - do not wait until morning
- Contact on-call spine surgeon immediately
- Book emergency theatre
- Consent for surgery (high risk of permanent dysfunction despite surgery)
- Thromboprophylaxis
Long-term Outcomes and Complications
Long-term Outcomes by CES Type
Surgical Complications:
- Wound infection (1-2%)
- CSF leak/dural tear (2-5%)
- Haematoma requiring return to theatre (rare)
- Recurrent disc herniation (5-10%)
- Wrong level surgery (rare but documented)
Guidelines, Registries & Global Practice
Global epidemiology
- Incidence approximately 1-3 per 100,000 population per year; roughly 0.04% of low back pain presentations and around 2-6% of lumbar disc operations.
- Most common cause is a large central lumbar disc herniation (L4/5 then L5/S1); other causes include tumour (primary or metastatic), epidural abscess, spontaneous or post-operative epidural haematoma, spinal stenosis decompensation and trauma.
- True compressive CES is confirmed on only about 30-40% of emergency MRIs performed for suspected CES, so a high false-positive clinical rate is expected and acceptable.
Society Guidance Compared
Registry and audit notes
- CES is not an arthroplasty/implant condition, so there is no implant registry; instead, national audit data (e.g. the UK UCES prospective cohort) provide the best contemporary outcome benchmarks.
- Across these datasets, median time from symptom onset to surgery is measured in days rather than hours, and only about a third of patients reach theatre within 48 hours - a reminder that real-world pathways lag behind the textbook ideal.
High- vs limited-resource practice variation
- High-resource settings: 24/7 MRI access, dedicated spinal on-call rotas and rapid inter-hospital transfer allow same-day decompression.
- Limited-resource settings: MRI may be unavailable out of hours, so CT myelogram or even clinical judgement with urgent referral becomes necessary; transfer distances and theatre availability commonly delay surgery, increasing the proportion presenting as CES-R. Early urinary catheterisation and intermittent self-catheterisation teaching remain universally available and important interim measures.
Controversies and Areas of Uncertainty
Retrospective meta-analyses (Ahn 2000, DeLong 2008) suggest benefit from decompression within 48h and a graded relationship with timing. The largest modern prospective cohort (Woodfield/UCES 2022) found no association between time to surgery and 1-year disability or urinary outcome. The likely truth: timing matters most for patients still CES-I, whilst once CES-R is established the damage is largely fixed.
A majority of emergency MRIs for suspected CES show no compressive lesion. Operating on imaging without correlation, or conversely dismissing genuine early CES, are both errors. Imaging must match the clinical picture.
Todd (2017) argues many classic red flags (painless retention, established saddle anaesthesia) are signs of late, irreversible CES. Triaging on these alone guarantees late presentation; earlier, subtler symptoms should trigger MRI.
Decompression at night by a fatigued team without the full set of staff and equipment may add morbidity (a point Gleave and Macfarlane raised). "As soon as safely possible" balances urgency against operating under suboptimal conditions; many networks transfer to a 24/7 spinal centre rather than operate locally at 3am.
Key Mnemonics
BB-SADDLERed Flags for CES
Hook:Sitting on a numbness SADDLE - think CES when patients describe perineal symptoms!
WIPECES Clinical Questions
Hook:WIPE - the key questions to ask every patient with red flag back pain!
S2-3-4Bladder Innervation
Hook:S2, 3, 4 keeps the wee off the floor - and the poo out of the shoe!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man presents to ED at 2am with severe back pain and bilateral sciatica. He mentions he hasn't passed urine since the morning (16 hours ago) but 'doesn't feel the need to go'. DRE reveals reduced anal tone. What do you do?”
“A 38-year-old woman presents with 3 days of worsening back pain radiating to both legs. She mentions her bladder 'feels strange' - she has to strain to start urinating and doesn't feel like she empties fully. On examination, she has reduced perineal sensation but intact anal tone. What are your concerns?”
“A 29-year-old woman presents with 2 days of bilateral leg pain, a feeling of numbness 'down below' and urinary urgency. DRE shows normal anal tone and normal perianal sensation to pinprick. Emergency MRI of the whole lumbar spine shows a small L5/S1 disc bulge but no significant canal compromise and free-floating nerve roots. How do you proceed?”
Red Flags (BB-SADDLE)
- Bilateral sciatica (though can be unilateral)
- Bladder dysfunction - THE critical symptom
- Saddle anaesthesia (perineal numbness)
- Anal tone loss on DRE
- Deficit in legs (motor/sensory)
- Disturbance of bowels
- Lower back pain (severe)
- Erectile/Sexual dysfunction
Classification (Gleave & Macfarlane)
- CES-I (Incomplete): Altered bladder sensation, volitional control PRESERVED - URGENT
- CES-R (Retention): Painless retention, overflow incontinence - POORER PROGNOSIS
Investigation
- Gold Standard: Emergency MRI Lumbar Spine
- Bladder scan: PVR greater than 500ml highly predictive
- CT Myelogram if MRI contraindicated
Management
- Emergency surgical decompression
- Laminectomy +/- discectomy
- Timing: As soon as safely possible (within 24-48h)
- Goal: Operate while CES-I to prevent CES-R
Evidence Base
Decompression within 48 hours - Ahn meta-analysis
- Meta-analysis of 322 patients with CES secondary to lumbar disc herniation (42 studies)
- No significant difference between surgery under 24h versus 24-48h
- Significant advantage for decompression within 48h versus after 48h for sensory, motor, bladder and bowel recovery
- Pre-operative chronic back pain and rectal dysfunction predicted worse urinary outcome
CES-R vs CES-I should not be analysed together - DeLong meta-analysis
- Meta-analysis of 16-27 observational cohorts of CES with retention (CES-R)
- Later surgery predicted a worse (Fair/Poor) urinary outcome (relative risk 1.77 to 2.19 across breakpoints)
- CES-R carried a worse outcome than incomplete CES (relative risk 2.58)
- Concluded CES-R and CES-I must be reported separately, not pooled
CES classification and the timing controversy
- Articulated the incomplete (CES-I) versus retention/overflow (CES-R) distinction now in routine use
- CES-I: subjective bladder symptoms with volitional control preserved
- CES-R: painless retention with overflow incontinence and a paralysed bladder
- Authors argued that once retention with overflow is established, urgent decompression confers no additional benefit
UCES - UK prospective cohort (Woodfield)
- Prospective multicentre cohort of 621 surgically treated CES patients with 1-year follow-up
- Median time to surgery 3 days; only 32% operated within 48h
- No association between time to surgery (or radiological compression) and Oswestry Disability Index or urinary outcome at 1 year
- Functional improvement occurred even in those presenting in retention; 65% needed extra healthcare services during follow-up
Long-term micturition, defecation and sexual outcome (Korse)
- Cohort of 75 surgically decompressed CES patients; L5-S1 most common level
- At presentation: micturition dysfunction 92%, saddle sensory change 93%, defecation dysfunction 74%
- At follow-up: micturition dysfunction 48%, defecation dysfunction 42%, sexual dysfunction 53%
- Recovery is slow and incomplete in the majority despite decompression
Red flags versus 'white flags' - rethinking triage (Todd)
- Systematic review of 7 guideline sources, 37 recommendations
- Up to two-thirds of so-called 'red flags' actually describe late, often irreversible CES ('white flags' of defeat)
- Only ~32% of features were true early warning signs that allow avoidable damage to be prevented
- Calls for low-threshold MRI as part of triage at the district general hospital
BASS / SBNS national standards for suspected CES
- Emergency MRI mandatory for suspected CES, day or night, where the patient presents
- Confirmed CES should be transferred and decompressed on an emergency basis
- No arbitrary hour limit - operate as soon as safely feasible
- Meticulous documentation of bladder, bowel, perineal and DRE findings is mandatory
References
- Gleave JRW, Macfarlane R. Cauda equina syndrome: what is the relationship between timing of surgery and outcome? Br J Neurosurg. 2002;16(4):325-328. PMID 12389883. doi:10.1080/0268869021000032887
- Ahn UM, Ahn NU, Buchowski JM, et al. Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976). 2000;25(12):1515-1522. PMID 10851100. doi:10.1097/00007632-200006150-00010
- DeLong WB, Polissar N, Neradilek B. Timing of surgery in cauda equina syndrome with urinary retention: meta-analysis of observational studies. J Neurosurg Spine. 2008;8(4):305-320. PMID 18377315. doi:10.3171/SPI/2008/8/4/305
- Korse NS, Pijpers JA, van Zwet E, et al. Cauda equina syndrome: presentation, outcome, and predictors with focus on micturition, defecation, and sexual dysfunction. Eur Spine J. 2017;26(3):894-904. PMID 28102451. doi:10.1007/s00586-017-4943-8
- Woodfield J, Hoeritzauer I, Jamjoom AAB, et al. Presentation, management, and outcomes of cauda equina syndrome up to one year after surgery: a multi-centre prospective cohort study. Lancet Reg Health Eur. 2022;24:100545. PMID 36426378. doi:10.1016/j.lanepe.2022.100545
- Todd NV. Guidelines for cauda equina syndrome. Red flags and white flags. Systematic review and implications for triage. Br J Neurosurg. 2017;31(3):336-339. PMID 28637110. doi:10.1080/02688697.2017.1297364
- Korse NS, Veldman AB, Peul WC, Vleggeert-Lankamp CLA. The long term outcome of micturition, defecation and sexual function after spinal surgery for cauda equina syndrome. PLoS One. 2017;12(4):e0175987. PMID 28423044. doi:10.1371/journal.pone.0175987
- British Association of Spine Surgeons and Society of British Neurological Surgeons. Standards of care for established and suspected cauda equina syndrome. 2018.