Cervical Lateral Mass Fracture-Separation
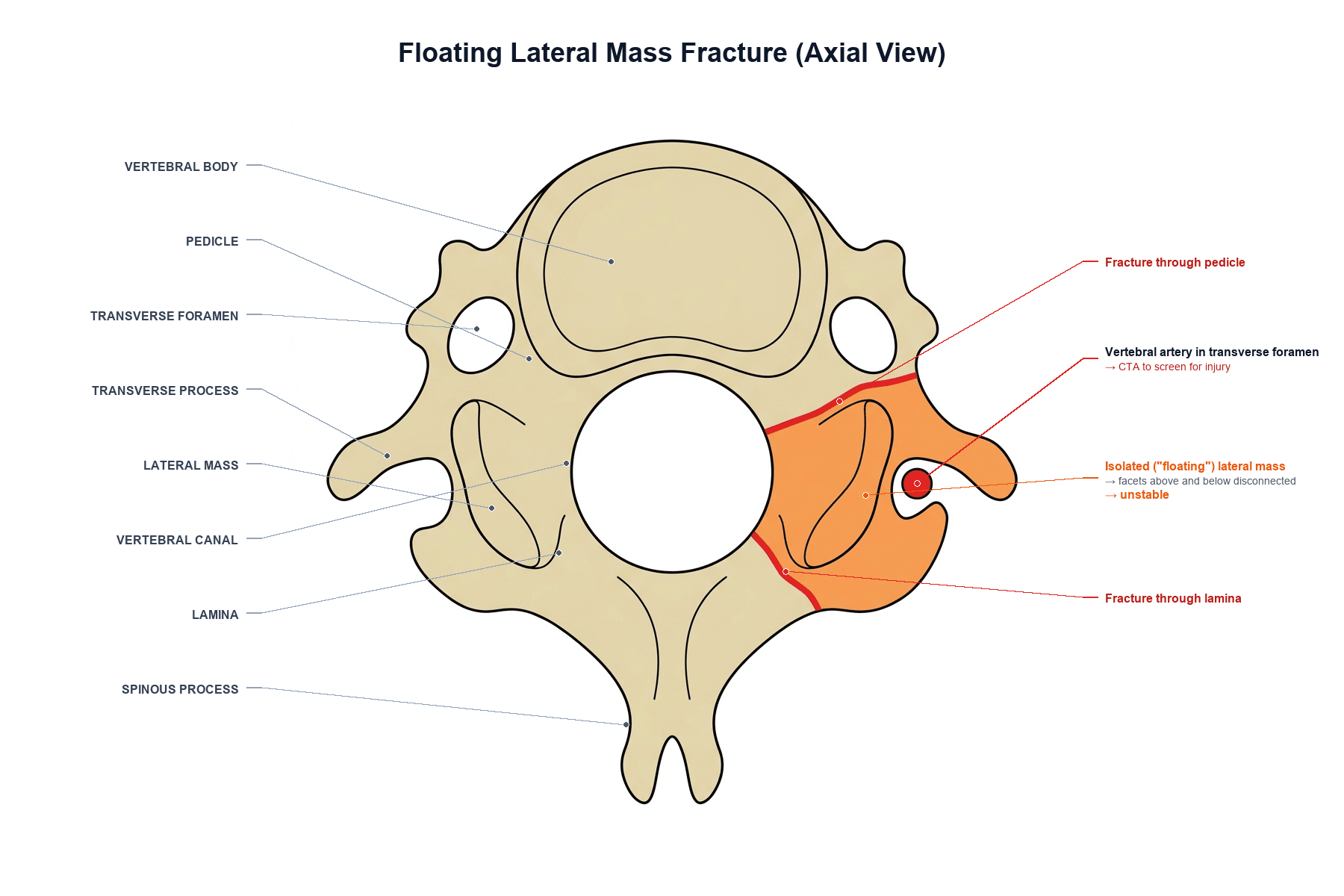
- A floating lateral mass (FLM) fracture-separation of the subaxial cervical spine is defined by a fracture through BOTH the ipsilateral LAMINA and the PEDICLE, which separates the lateral mass from the rest of the vertebra and thereby DISCONNECTS the superior and inferior articular processes (the facet joints above and below that level) - the lateral mass is left 'floating'.
- Because the lateral mass is the structural link between consecutive facet joints, isolating it removes the bony continuity of the posterolateral column and makes the segment HIGHLY UNSTABLE, prone to rotational malalignment, kyphosis and facet subluxation; the injured level often shows the lateral mass rotated into a horizontal ('reverse hamburger') orientation.
- FLM fractures result from HIGH-ENERGY trauma and are frequently associated with NERVE ROOT injury (the exiting root at that level is at risk) and with other cervical fractures or ligamentous injury, so a full assessment of the neurology and the rest of the cervical spine is essential.
- CT is the key investigation to DEFINE the pattern (lamina + pedicle fractures isolating the lateral mass, with assessment of facet alignment); because of the proximity of the lateral mass and pedicle to the TRANSVERSE FORAMEN, and because fracture patterns with DISLOCATION/SUBLUXATION carry the highest risk of BLUNT CEREBROVASCULAR INJURY (BCVI), CT ANGIOGRAPHY should be used to screen for VERTEBRAL ARTERY injury.
- Because the injury is unstable, OPERATIVE stabilisation (fusion) is commonly required and can be performed by an ANTERIOR, POSTERIOR or COMBINED approach; in reported series complications clustered in the posterior (hardware failure) and combined (respiratory) groups, while the anterior approach had fewest - so approach selection should weigh the injury pattern, alignment and associated injuries.
- NON-OPERATIVE management (rigid immobilisation) can be satisfactory for APPROPRIATELY SELECTED FLM fractures - in a reported cohort none of the carefully selected non-operatively treated patients required later surgery for subluxation - so management is individualised to stability, alignment, neurology and the patient, rather than mandating surgery for every FLM.
- “Floating lateral mass = fracture through BOTH lamina AND pedicle -> isolates the lateral mass and DISCONNECTS the facet joints above and below (highly unstable).
- “High-energy; watch for nerve root injury; CT defines it and CTA screens for vertebral artery (BCVI) injury - dislocation/subluxation patterns carry the highest BCVI risk.
- “Often operative (anterior/posterior/combined); selected cases manage non-operatively with rigid immobilisation.
Fracture through both the lamina and the pedicle isolates the lateral mass, so the facet joints above and below are disconnected - the mass 'floats'. Highly unstable.
Nerve root injury at that level, and vertebral artery injury - CTA screen (dislocation/ subluxation patterns carry the highest BCVI risk).
Definition, Instability & Workup
A floating lateral mass fracture is defined by a fracture through both the lamina and the pedicle on one side, which separates the lateral mass from the vertebra and disconnects the superior and inferior articular processes - the facet joints above and below. Because the lateral mass is the bony link between consecutive facets, isolating it removes the posterolateral column's continuity and leaves the segment highly unstable, prone to rotation, kyphosis and facet subluxation (the lateral mass may rotate into a horizontal orientation). These are high-energy injuries, often with nerve root involvement and associated cervical injuries. CT defines the pattern, and because the lateral mass/pedicle lie next to the transverse foramen - and fracture-dislocation/subluxation patterns carry the highest risk - CTA should screen for vertebral artery (BCVI) injury.
Where It Sits in the Classifications (FLM = AO Spine F3)
Calling the injury unstable is not enough in a viva - the examinable step is to place it in the formal systems (the general subaxial frameworks are developed in our Subaxial Cervical Fractures topic):
- AO Spine subaxial classification. Alongside the morphology types (A compression, B tension-band, C translation), facet injuries are graded F1-F4 - and the floating lateral mass is the F3 subtype. Knowing the ladder shows why: F1 a nondisplaced facet fracture, F2 a facet fracture with potential instability, F3 the floating lateral mass (separation by fractures through the pedicle AND lamina), and F4 a pathologic subluxation/perched or dislocated facet.
- SLIC (Subaxial Injury Classification). Scores morphology + the discoligamentous complex + neurology; the facet disruption and any subluxation/malalignment of an FLM push the score toward the operative range, which is consistent with how unstable the injury is.
- Definition
- Nondisplaced facet fracture (smaller fragment - less than about 1 cm and under ~40% of the lateral mass)
- Definition
- Facet fracture with potential instability (larger/comminuted - more than about 1 cm or over ~40% of the lateral mass)
- Definition
- Lateral mass separated by fractures through BOTH the pedicle and the lamina (THIS injury) - disconnects the facets above and below
- Definition
- Pathologic subluxation or a perched/dislocated facet
One line for the viva: a floating lateral mass is the AO Spine F3 facet injury - the lateral mass isolated by pedicle + lamina fractures. Distinguish it from F2 (a big facet fragment still attached) and F4 (a subluxated/dislocated facet). On SLIC, the disrupted facet and any malalignment typically score into the operative range.
If the CTA Is Positive: Grading and Managing the Vertebral Artery Injury
- Grade it (Biffl / Denver scale). Grade I - luminal irregularity or dissection with less than about a quarter narrowing; Grade II - dissection/intramural haematoma with more than about a quarter narrowing, an intraluminal thrombus or a raised intimal flap; Grade III - pseudoaneurysm; Grade IV - complete occlusion; Grade V - transection with active extravasation.
- Treat to prevent stroke. Antithrombotic therapy (antiplatelet, e.g. aspirin, or systemic anticoagulation/heparin) is the mainstay for grades I-IV and reduces the posterior-circulation stroke risk - balanced against bleeding risk in a polytrauma patient and the timing of spinal surgery.
- Endovascular/serial imaging. Many low-grade injuries stabilise or resolve, so they are followed with repeat imaging; an enlarging Grade III pseudoaneurysm or a Grade V transection may need endovascular treatment (stent/coil/embolisation), while a Grade IV occlusion is usually managed antithrombotically.
- Coordinate with the spine plan. The antithrombotic decision is made jointly with the trauma/neuro teams around the timing of fixation.
A positive CTA is not the end: grade the BCVI (Biffl I-V), start antithrombotic therapy (antiplatelet or anticoagulation) for grades I-IV to cut stroke risk, follow low grades with repeat imaging, and reserve endovascular treatment for an enlarging pseudoaneurysm (III) or transection (V) - all balanced against bleeding and the timing of spinal stabilisation.
Mechanism, Presentation and the Non-operative Route
- Mechanism. A high-energy extension–compression or extension–rotation load drives the inferior articular process of the level above into the lateral mass, splitting it; the same force may be applied in lateral bending with axial load. Because it takes that much energy, an isolated finding should prompt a search for associated cervical and non-cervical injuries rather than reassurance.
- Presentation. Axial neck pain with restricted, painful rotation (the fractured facet complex is the restraint), often torticollis-like posturing to the injured side. Radicular symptoms in the exiting root are common because the root sits immediately anterior to the fractured mass — document power in the myotome for that level before any intervention. A Horner syndrome, hemiparesis, ataxia or posterior circulation symptoms point at the vertebral artery, not the root.
- Non-operative selection. Where the injury is a genuinely isolated lateral mass fracture with no translation or kyphosis, an intact discoligamentous complex on MRI and normal neurology, a rigid collar for a period of weeks with upright radiographs at intervals is reasonable — the critical part is the interval imaging, because late subluxation is the failure mode that converts a conservative plan into a delayed fusion.
- What pushes toward surgery: translation or facet subluxation, progressive kyphosis, a positive discoligamentous injury on MRI, radiculopathy that does not settle, or the same injury in a multi-level or polytrauma context where a collar cannot be relied on.
Fixation Technique and Its Two Hazards
If posterior fixation is chosen, the segment is usually held with lateral mass screws, and the examinable content is the trajectory — because the two structures at risk sit either side of the screw.
- Roy-Camille. Start at the midpoint of the lateral mass, aim straight lateral by about 10 degrees and perpendicular to the posterior cortex (no cephalad angulation).
- Magerl. Start 1–2 mm medial and caudal to the midpoint, aim about 25 degrees lateral and parallel to the facet joint surface (roughly 30 degrees cephalad). More lateral and cephalad angulation.
- An. Start at the midpoint, aim about 15 degrees lateral and 30 degrees cephalad.
- The principle behind all three: aim LATERAL and CEPHALAD. Medial angulation threatens the vertebral artery in the transverse foramen; insufficient cephalad angulation threatens the exiting nerve root below. Getting that single sentence out is worth more than reciting exact degrees.
- Where lateral mass screws stop. They are used C3–C6 reliably. C7 has a thin, small lateral mass, so pedicle screw fixation is usually preferred there, and C2 takes a pars, pedicle or translaminar screw instead.
- A fractured lateral mass cannot hold a screw at the injured level, so the construct must span it — instrumenting the intact levels above and below rather than the fracture itself.
Management
- Assess fully. Document neurology (the exiting nerve root is at risk), assess alignment and the rest of the cervical spine, and CTA to screen for vertebral artery injury.
- Operative stabilisation is commonly required for this unstable injury - anterior, posterior or combined fusion. In reported series complications clustered in the posterior (hardware failure) and combined (respiratory) groups, with fewest in the anterior approach - so weigh injury pattern, alignment and associated injuries when choosing.
- Non-operative management (rigid immobilisation) is satisfactory for appropriately selected FLM fractures - in a reported cohort no carefully selected non-operative patient needed later surgery for subluxation.
- Individualise. Base the decision on stability, alignment, neurology and the whole injury picture rather than treating every FLM the same way.
Two associated injuries must not be overlooked in a floating lateral mass fracture. First, the VERTEBRAL ARTERY: the lateral mass and pedicle lie immediately adjacent to the transverse foramen, and fracture patterns with dislocation or subluxation carry the highest risk of blunt cerebrovascular injury, so CT angiography should be used to screen - a missed vertebral artery injury risks a posterior circulation stroke. Second, the NERVE ROOT: the exiting root at the injured level is frequently involved, so the neurological examination must be carefully documented. Recognise the injury as highly unstable because both the facet joints above and below have been disconnected, but individualise the operative-versus-non-operative decision, since carefully selected FLM fractures can be managed non-operatively.
Mnemonics & Memory Aids
FLOAT
Hook:FLOAT: Fracture lamina+pedicle, Lateral mass floats, Off-line facets (unstable), Artery (CTA)/root, Treat by stabilising or selected non-op.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is a floating lateral mass fracture, and why is it unstable?”
“How would you manage a floating lateral mass fracture?”
Definition
- Fracture through BOTH lamina and pedicle isolating the lateral mass
- Disconnects superior and inferior articular processes (facets above and below)
- The lateral mass 'floats' - may rotate horizontal
Why it matters
- Highly unstable (loss of posterolateral column continuity)
- High-energy; nerve root injury common at that level
- Associated cervical fractures/ligamentous injury
Workup
- CT defines the pattern and facet alignment
- CTA to screen for vertebral artery / BCVI
- Dislocation/subluxation and upper-cervical/multilevel patterns = highest BCVI risk
Management
- Often operative stabilisation (anterior/posterior/combined)
- Anterior had fewest complications in series; posterior (hardware), combined (respiratory)
- Selected cases non-operative (rigid immobilisation) - individualise
Evidence & Key Studies
Assessing treatment of floating lateral mass (FLM) fractures of the subaxial cervical spine
- An FLM fracture involves separation of the lateral mass from the vertebra via disruption of BOTH the lamina and the pedicle, disconnecting the superior and inferior articular processes - a highly unstable injury.
- In a 10-year cohort of 45 patients (25 non-operative, 20 operative: 6 anterior, 12 posterior, 2 combined), no non-operative patient crossed over to surgery for subluxation.
- Complications occurred in the posterior (hardware failure) and combined (respiratory) groups, with none in the anterior group - suggesting carefully selected non-operative treatment can be satisfactory.
Cervical fracture patterns associated with blunt cerebrovascular injury on CT angiography
- The only fracture pattern associated with increased risk of blunt cerebrovascular injury (BCVI) was a fracture associated with dislocation/subluxation (odds ratio 3.8).
- Combined upper-cervical (occiput-C3) fractures and multilevel fractures were also associated with increased BCVI risk; among screened patients, BCVI was found in 30% and all strokes occurred in BCVI patients.
- The authors recommend CT-angiography screening for any upper-cervical, multilevel, or fracture-with-dislocation/subluxation pattern.
The definition of the floating lateral mass (lamina + pedicle disruption disconnecting the articular processes), its instability, and the operative-versus-non-operative outcomes (including satisfactory selected non-operative treatment and the approach-specific complications) come from the cited Prezelski cohort; the association of dislocation/subluxation and upper-cervical/multilevel patterns with blunt cerebrovascular (vertebral artery) injury and the recommendation to screen with CT angiography from the cited Du study. The high-energy mechanism, the nerve-root risk and the general principles of subaxial cervical stabilisation are standard, well-established teaching. (See also our Subaxial Cervical Spine Injuries and Facet Dislocation topics.)