Neuropathic Joint Destruction | Diabetic Foot | Eichenholtz Staging | Rocker-Bottom Deformity
- Charcot neuroarthropathy = progressive destructive arthropathy in a neuropathic joint
- Most common cause is diabetes mellitus (type 1 and type 2); other causes include syringomyelia, leprosy, alcohol neuropathy
- Acute presentation mimics infection (warm, red, swollen foot) — delayed diagnosis is common and devastating
- Rocker-bottom deformity results from midfoot collapse during Stage 1, creating plantar prominence and ulceration risk
- Total contact cast (TCC) is gold standard for acute phase — prolonged immobilisation prevents further destruction
- Surgical reconstruction considered when deformity is unstable, non-braceable, or ulceration recurrent
- “Always suspect Charcot in any diabetic patient with a warm, swollen foot — even without a clear history of trauma
- “Skin temperature differential greater than 2 degrees Celsius between feet suggests acute Charcot, not cellulitis
- “Stage 0 has normal X-rays but clinical suspicion — MRI shows bone marrow oedema
- “Rocker-bottom deformity is the hallmark of midfoot Charcot — palpate the plantar prominence
Clinical Photographs
Clinical Appearance


Acute Charcot mimics cellulitis and DVT. A warm (greater than 2 degrees Celsius difference), swollen, erythematous foot in a neuropathic patient with NO systemic symptoms (afebrile, normal WBC) is Charcot until proven otherwise. Starting antibiotics without considering Charcot delays TCC and worsens outcome.
Stage 0 = pre-radiographic. X-rays normal but clinical suspicion high. MRI shows marrow oedema. This is the window for TCC to prevent Stage 1 destruction. By Stage 1, fragmentation has begun. Missed Stage 0 leads to rocker-bottom deformity.
Midfoot collapse creates plantar bony prominence. The navicular-cuneiform or tarso-metatarsal joints collapse, reversing the medial longitudinal arch. The resultant plantar prominence causes focal pressure, callus formation, and eventual ulceration — the gateway to deep infection and amputation.
Immediate offloading in acute Charcot is limb-saving. Every day without TCC during Stage 0-1 permits further bone destruction. TCC duration is typically 3-6 months (until skin temperature normalises and radiographic coalescence occurs). Delayed treatment increases amputation risk from less than 5 percent to over 15 percent.
- Diagnosis
- Stage 0-1 Charcot (MRI if X-ray normal)
- Treatment
- Immediate TCC, strict non-weight-bearing
- Key Pearl
- Do NOT treat as cellulitis without considering Charcot
- Diagnosis
- Stage 2-3 Charcot, rocker-bottom
- Treatment
- Custom CROW boot or total contact orthosis
- Key Pearl
- Monitor for ulceration; consider prophylactic surgery
- Diagnosis
- Stage 3 Charcot with unstable deformity
- Treatment
- Exostectomy or reconstructive arthrodesis
- Key Pearl
- Eradicate infection before reconstruction
- Diagnosis
- MRI + biopsy, staged treatment
- Treatment
- Infection control then reconstruction vs amputation
- Key Pearl
- Infected Charcot carries highest amputation risk
WARMRecognising Acute Charcot
Hook:A WARM neuropathic foot is Charcot until proven otherwise — do not prescribe antibiotics for presumed cellulitis without considering this diagnosis!
STEPEichenholtz Staging
Hook:STEP through the Eichenholtz stages — Suspicion, Tearing, Early healing, Plateau!
FIXEDSurgical Indications in Charcot
Hook:Only proceed to surgery when the problem is FIXED — Failure, Instability, Xostectomy, Eradicate infection, Deformity!
Overview and Epidemiology
Charcot neuroarthropathy is one of the most devastating complications of diabetic neuropathy. It is frequently misdiagnosed as cellulitis, deep vein thrombosis, or gout in its acute phase, leading to delayed offloading and irreversible joint destruction. The resultant rocker-bottom deformity predisposes to recurrent ulceration, deep infection, and ultimately major amputation. Early recognition (Stage 0-1) and immediate total contact casting can prevent this cascade entirely.
- Incidence: 0.3 to 7.5 percent of diabetic patients develop Charcot
- Bilateral: 9 to 75 percent develop contralateral involvement over time
- Most common cause: Diabetes mellitus (accounts for greater than 75 percent of cases in developed countries)
- Other causes: Syringomyelia (upper limb), leprosy, alcohol-related neuropathy, spinal cord injury, congenital insensitivity to pain
- Anatomical distribution: Midfoot (60 percent), rearfoot/ankle (30 percent), forefoot (10 percent)
- Amputation risk: 15-30 percent if untreated or diagnosed late
- Ulceration: Greater than 50 percent develop plantar ulcers from rocker-bottom deformity
- Quality of life: Severe limitation in mobility, employment, and independence
- Healthcare cost: Hospitalisation for Charcot complications is among the highest in diabetic foot disease
- Mortality: 5-year mortality following Charcot-related amputation approaches 50 percent
Pathophysiology
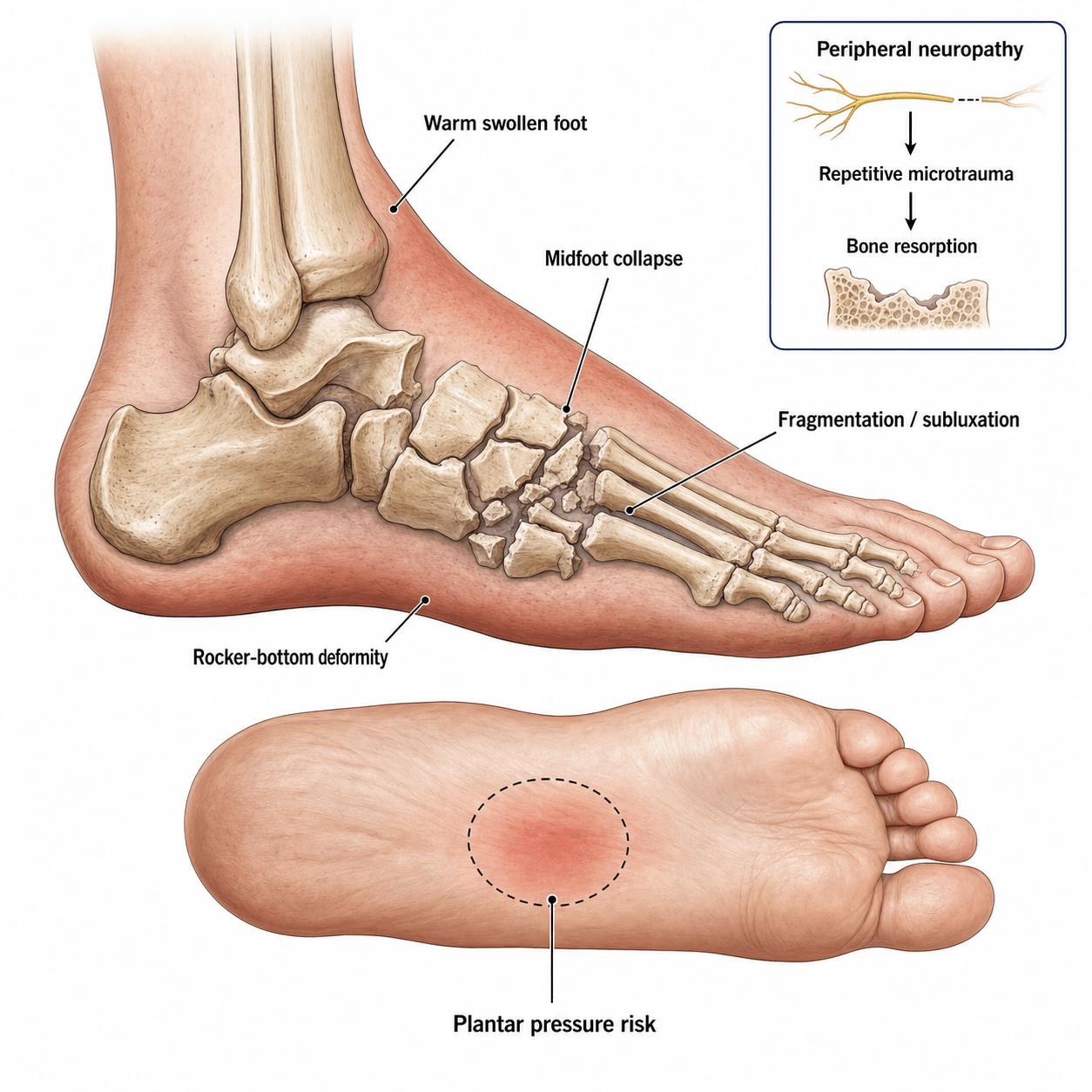
Charcot neuroarthropathy results from the combination of loss of protective sensation and repetitive microtrauma in a vascularly active bone environment. Two complementary mechanisms drive destruction:
Neurotraumatic theory: Loss of proprioception and pain sensation allows repeated micro-injury to the joint beyond physiological tolerance. Minor trauma (twisting, stepping off a curb) goes unrecognised, and weight-bearing continues on an injured joint.
Neurovascular theory: Autonomic neuropathy causes increased blood flow to bone (loss of sympathetic vasoconstriction), leading to osteopenia and increased bone resorption. The hyperaemic, osteopenic bone is structurally weak and fractures easily under normal loads.
Inflammatory cascade: Acute trauma triggers an exaggerated inflammatory response (RANKL upregulation, osteoclast activation) in the neuropathic limb, creating a vicious cycle of bone resorption, fragmentation, and deformity.
- Key Feature
- Loss of sympathetic vasoconstriction
- Result
- Increased bone blood flow, osteopenia
- Clinical Relevance
- Bone structurally weakened before injury
- Key Feature
- Loss of protective sensation
- Result
- Unrecognised microtrauma continues
- Clinical Relevance
- Patient weight-bears on injured joint
- Key Feature
- Intrinsic muscle wasting, imbalance
- Result
- Altered foot mechanics, abnormal loading
- Clinical Relevance
- Contributes to progressive subluxation
- Key Feature
- RANKL upregulation, osteoclast activation
- Result
- Exaggerated bone resorption
- Clinical Relevance
- Explains rapid destruction in Stage 1
Anatomical vulnerability: The tarso-metatarsal (Lisfranc) and naviculocuneiform joints have limited intrinsic stability. When osteopenic bone meets repetitive load, the midfoot collapses dorsally, inverting the longitudinal arch and creating the rocker-bottom deformity.
The plantar tarsometatarsal ligaments attenuate, the cuneiforms displace dorsally, and the cuboid becomes the weight-bearing plantar prominence.
Critical differentiation: Both present with bone destruction in a diabetic foot.
Charcot: Multi-bone, centred on joints, no adjacent ulcer/sinus tract, subluxation pattern, preserved cortical outline in early stages.
Osteomyelitis: Single bone (usually), adjacent to ulcer or sinus tract, cortical destruction, periosteal reaction, soft tissue gas/fluid collection.
MRI distinction: Charcot = diffuse multi-bone marrow oedema; osteomyelitis = focal marrow replacement with adjacent soft tissue defect.
Classification and Types
Eichenholtz Staging (Modified with Stage 0)
- Clinical Features
- Warm, swollen foot, painless or mild ache, temperature differential greater than 2 degrees Celsius
- Radiographic Findings
- Normal X-rays, MRI shows bone marrow oedema
- Treatment
- Immediate TCC, strict non-weight-bearing
- Duration
- Until temperature normalises (typically 4-8 weeks)
- Clinical Features
- Swelling, erythema, bounding pulses, joint laxity
- Radiographic Findings
- Osteopenia, fragmentation, joint subluxation, debris formation, periosteal reaction
- Treatment
- TCC, strict non-weight-bearing, serial X-rays every 4 weeks
- Duration
- Until coalescence begins (typically 3-6 months)
- Clinical Features
- Decreasing swelling and warmth, foot temperature approaches contralateral
- Radiographic Findings
- Absorption of debris, periosteal new bone formation, fusion of fragments
- Treatment
- TCC with gradual progression to weight-bearing, bivalve cast
- Duration
- 2-4 months, until consolidation
- Clinical Features
- Cool, stable foot with fixed deformity (rocker-bottom, varus/valgus)
- Radiographic Findings
- Remodelled, consolidated bone, fixed deformity, mature sclerosis
- Treatment
- Custom orthosis (CROW boot), accommodative footwear
- Duration
- Lifetime bracing and monitoring
Stage 0 was added to the original Eichenholtz classification to capture the pre-radiographic phase where intervention is most effective. Recognising Stage 0 prevents progression to destructive Stage 1.
Clinical Assessment
- Diabetes: Duration, glycaemic control (HbA1c), neuropathy screening history
- Onset: Often cannot recall specific injury — insidious swelling common
- Symptoms: Painless or minimally painful swelling, redness, warmth — patient may notice foot shape change
- Contralateral foot: Prior Charcot episode, current ulceration, or deformity
- Walking status: Has the patient continued to weight-bear on the swollen foot?
- Inspect: Erythema, oedema, foot shape (rocker-bottom, varus/valgus, medial arch collapse), callus patterns, ulceration
- Palpate: Skin temperature (use infrared dermathermometer — greater than 2 degrees Celsius difference is significant), bony prominences, joint stability
- Neurological: Monofilament testing (10g), vibration (128 Hz tuning fork), proprioception, deep tendon reflexes
- Vascular: Pedal pulses, capillary refill, Doppler if pulses not palpable — Charcot requires adequate perfusion to heal
Infrared dermathermometry is the most reliable tool for diagnosing and monitoring acute Charcot activity. A skin temperature difference of greater than 2 degrees Celsius (some authorities use greater than 2.2 degrees Celsius) between the affected and contralateral foot at comparable anatomical sites indicates active inflammation. Temperature normalisation (less than 1 degree Celsius difference) is a key criterion for transitioning from TCC to bracing and for confirming coalescence.
Monitoring schedule: Measure temperature at each visit (every 1-2 weeks during acute phase). Plot trends to track resolution of inflammation. Rising temperature despite TCC suggests ongoing destruction or complication.
- Acute Charcot
- Minimal (neuropathy)
- Cellulitis
- Moderate to severe
- Deep Vein Thrombosis
- Calf pain, foot swelling
- Acute Charcot
- Afebrile, normal WBC, no malaise
- Cellulitis
- Fever, elevated WBC, malaise
- Deep Vein Thrombosis
- Low-grade fever possible
- Acute Charcot
- Greater than 2 degrees Celsius (focal, unilateral)
- Cellulitis
- Warm but often bilateral or less differential
- Deep Vein Thrombosis
- Often less than 2 degrees Celsius differential
- Acute Charcot
- May be normal (Stage 0) or show fragmentation
- Cellulitis
- Soft tissue swelling only
- Deep Vein Thrombosis
- Normal bone, no joint changes
- Acute Charcot
- No improvement (key discriminator)
- Cellulitis
- Improves within 48-72 hours
- Deep Vein Thrombosis
- No improvement
- Acute Charcot
- MRI (bone marrow oedema), temperature monitoring
- Cellulitis
- Blood cultures, clinical response to antibiotics
- Deep Vein Thrombosis
- Venous duplex ultrasound
The most common error is treating acute Charcot as cellulitis. The patient receives antibiotics, the erythema partially resolves (because the inflammatory phase naturally fluctuates), and weight-bearing continues on a collapsing foot. By the time Charcot is diagnosed, the patient has progressed from Stage 0 to Stage 1 with irreversible fragmentation. Always check for neuropathy and measure skin temperature in any diabetic patient with a swollen, red foot.
Investigations
Imaging Protocol
Views: Weight-bearing AP, lateral, oblique of foot and ankle
Look for: Stage-specific findings — osteopenia, fragmentation, subluxation, joint debris, periosteal reaction, rocker-bottom deformity, calcaneal pitch, Meary angle
Serial: Repeat every 4-6 weeks during acute phase to track stage progression
Indication: Clinically suspicious hot swollen foot with normal plain radiographs
Sequences: T1, T2 fat-suppressed, STIR
Findings: Bone marrow oedema (low T1, high STIR), capsular distension, soft tissue oedema, stress fractures occult on X-ray
Charcot vs osteomyelitis: Charcot shows diffuse multi-bone oedema; osteomyelitis shows focal oedema adjacent to ulcer/sinus tract
Indication: Surgical planning for reconstruction — assesses bone stock, fragment position, articular involvement
Findings: Detailed bony architecture, extent of fragmentation, quality of bone for screw/plate fixation
Helpful for: Planning osteotomy, arthrodesis fusion surfaces, hardware placement
Indication: All patients before TCC application and before surgery
Rationale: TCC requires adequate perfusion to heal. Critical ischaemia must be addressed before immobilisation. Surgical reconstruction requires palpable pulses or revascularisation.
Note: ABIs may be falsely elevated in diabetes due to medial arterial calcification (incompressible vessels). Toe pressures are more reliable in diabetics.
The diagnosis of acute Charcot is clinical (warm, neuropathic, swollen foot with temperature differential). X-rays may be normal in Stage 0 — do not wait for radiographic changes to start TCC. MRI confirms Stage 0 but treatment should begin on clinical suspicion alone. The most important investigation is serial temperature monitoring to guide TCC duration.
The topic stresses the Charcot-versus-osteomyelitis dilemma on MRI, but the genuinely hard case is the ulcerated Charcot foot where both show marrow oedema, or where metalwork degrades the MRI. Here nuclear imaging is the high-yield next step.
- Three-phase Tc-99m MDP bone scan: highly sensitive but not specific - it is positive in both Charcot and osteomyelitis, so on its own it cannot distinguish them.
- Labelled-leukocyte (white-cell) scan: uses Tc-99m-HMPAO or indium-111 labelled WBCs, which accumulate in infection. The pitfall is that haemopoietically active or remodelling Charcot marrow can also take up labelled WBCs, causing false positives.
- The decisive combination - labelled-WBC plus Tc-99m sulfur-colloid bone-marrow scan: compare the two. In osteomyelitis there is WBC uptake without matching marrow (sulfur-colloid) uptake - a spatial mismatch/incongruence is positive for infection. In uncomplicated Charcot the WBC and marrow images match (congruent) - no infection. This congruence test is the most reliable nuclear discriminator.
- FDG-PET/CT: increasingly used - osteomyelitis tends to show higher, focal uptake while Charcot shows lower-grade, diffuse uptake; it performs well around metalwork. SPECT/CT adds anatomical localisation to any of the above.
- Supporting signs: the MRI "ghost sign" (a bone poorly defined on T1 that becomes definable after contrast) and secondary signs (sinus tract, adjacent ulcer, soft-tissue collection) favour osteomyelitis.
Exam point: a plain bone scan cannot separate Charcot from osteomyelitis (both positive); when MRI is equivocal or there is metalwork, use a combined labelled-WBC + sulfur-colloid marrow scan - incongruent (WBC without marrow) = osteomyelitis, congruent = uncomplicated Charcot - with FDG-PET/CT or SPECT/CT as alternatives.
Management Algorithm
Acute Charcot: Offloading and Immobilisation
Goal: Halt the destructive cycle by eliminating weight-bearing stress on the osteopenic, fragmenting joint
Treatment Protocol
Total contact cast (TCC): Gold standard offloading device
Technique: Well-padded cast with minimal voids, applied over a tubular stocking, total contact from tibial tubercle to toes
Weight-bearing status: Strict non-weight-bearing (crutches, wheelchair, knee scooter)
Contraindications to TCC: Active ulceration with infection, critical ischaemia, severe oedema (bivalve cast instead)
Cast change: Every 1-2 weeks initially (oedema changing rapidly)
Monitor: Skin temperature, radiographs at 4 weeks, skin integrity
Bisphosphonates: Consider IV pamidronate or oral alendronate (evidence is mixed but may reduce disease activity)
Patient education: Non-weight-bearing compliance is critical — explain this is limb-saving treatment
Criteria for transition: Temperature differential less than 1 degree Celsius, radiographic evidence of coalescence (Stage 2), resolution of erythema
Transition: TCC to bivalve cast, then to Charcot Restraint Orthotic Walker (CROW boot)
Weight-bearing: Gradual progression from non-weight-bearing to partial to full, guided by temperature and symptoms
Goal: Progress to Stage 3 with stable, plantigrade foot
Device: CROW boot or custom total contact orthosis with extra-depth footwear
Monitoring: Temperature check monthly, radiographs at 6 months
If deformity progresses: Extend immobilisation or consider surgical intervention
Total contact cast technique: Apply with the patient prone or supine with leg vertical. Minimal padding over bony prominences (greater risk of pressure ulceration in neuropathic patients). Mold the cast to conform to the leg and foot. Use a walking base if weight-bearing is permitted (usually not in Stage 0-1). Cast changes are needed every 1-2 weeks because oedema fluctuates and a loose cast causes pressure areas. Always check for ulcers at each cast change — neuropathic patients will not feel pressure sores developing.
- Offloading Efficacy
- Gold standard (greatest pressure reduction)
- Patient Compliance
- Moderate (bulky, impractical for some patients)
- Advantages
- Best pressure reduction, enforces compliance
- Disadvantages
- Skin complications, requires skilled application
- Offloading Efficacy
- Good (less than TCC)
- Patient Compliance
- High (removable, adjustable)
- Advantages
- Removable for hygiene, adjustable fit
- Disadvantages
- Patient may remove and weight-bear
- Offloading Efficacy
- Good (similar to TCC)
- Patient Compliance
- High (cannot be removed by patient)
- Advantages
- Combines TCC efficacy with cast walker convenience
- Disadvantages
- Less evidence than traditional TCC
- Offloading Efficacy
- Complete offloading when used correctly
- Patient Compliance
- Variable
- Advantages
- Additional offloading, not device-dependent
- Disadvantages
- Requires upper body strength, fall risk

Reconstruction: Superconstruct Principles, Beaming and External Fixation
When reconstruction is undertaken in the quiescent (Eichenholtz 3) foot, fixation must work in poor-quality, osteopenic neuropathic bone across a deformity-prone foot. The "superconstruct" concept addresses this with four principles, and two fixation strategies - intramedullary beaming and circular external fixation - dominate practice.
- Rationale
- Include adjacent unaffected joints so fixation anchors in sound bone and resists recurrent collapse
- Rationale
- Locked plates, solid bolts or intramedullary beams withstand the long healing times of neuropathic bone
- Rationale
- Intramedullary axial beams and plantar (tension-side) plating maximise mechanical advantage
- Rationale
- A braceable plantigrade foot is the goal; malalignment perpetuates ulceration
- Best Suited To
- Sanders Type 2 (Lisfranc) midfoot collapse with reasonable bone stock and no active infection
- Key Points and Evidence
- Axial screws/bolts driven along the medial and lateral columns restore the arch with minimal soft-tissue stripping; Sammarco reported osseous union in 16 of 22 feet at a mean of 5.8 months, though hardware failure is common and purpose-designed Charcot beams are emerging
- Best Suited To
- Severe osteopenia, bone loss, or active/recent infection where internal hardware is hazardous
- Key Points and Evidence
- A statically applied fine-wire frame corrects severe deformity in hostile bone; Pinzur's 171-foot series showed it achieves correction but with high pin-site infection (around 30-50%), and a new neuropathic ankle can develop after frame removal
The superconstruct answer in the viva is: fuse beyond the zone of injury, use the strongest tolerable device in the most robust position, and restore a plantigrade foot. Beaming (axial intramedullary screws/bolts) suits Lisfranc midfoot Charcot with adequate bone, while circular external fixation is reserved for severe osteopenia, bone loss or infection. Tibiotalocalcaneal arthrodesis with a retrograde nail addresses ankle/hindfoot (Brodsky 3A/Sanders 4) disease. Expect prolonged healing - roughly two to three times longer than non-neuropathic fusion - and a high complication burden.
Complications
- Incidence
- Up to 50-70 percent of midfoot Charcot
- Risk Factors
- Delayed diagnosis, continued weight-bearing in Stage 1
- Management
- TCC for acute phase, CROW boot or surgery for chronic
- Incidence
- Greater than 50 percent with rocker-bottom
- Risk Factors
- Plantar bony prominence, inadequate footwear
- Management
- Exostectomy, custom orthosis, or reconstruction
- Incidence
- 10-20 percent overall, higher with ulceration
- Risk Factors
- Chronic ulceration, poor glycaemic control, peripheral vascular disease
- Management
- Staged treatment: infection control then reconstruction or amputation
- Incidence
- 10-20 percent after midfoot arthrodesis, up to 30 percent after ankle fusion
- Risk Factors
- Poor bone quality, inadequate fixation, tobacco use
- Management
- Revision arthrodesis with bone graft or amputation
- Incidence
- 9-75 percent develop bilateral disease
- Risk Factors
- Similar neuropathic and vascular risk factors
- Management
- Surveillance of contralateral foot, patient education
- Incidence
- 15-30 percent if untreated, less than 5 percent with optimal early management
- Risk Factors
- Uncontrolled infection, unreconstructable deformity, poor vascular status
- Management
- Below-knee amputation with prosthetic rehabilitation
- Incidence
- 10-25 percent during casting
- Risk Factors
- Inadequate padding, infrequent cast changes, severe oedema
- Management
- Cast change every 1-2 weeks, meticulous technique, bivalve if high risk
The Charcot cascade follows a predictable domino pattern: neuropathy leads to unrecognised injury, leading to fragmentation, leading to rocker-bottom deformity, leading to plantar ulceration, leading to deep infection, leading to amputation. Breaking the chain at Stage 0 with immediate TCC prevents the entire cascade. This is the single most important message for exam candidates.
Recurrent plantar ulceration is the gateway complication this topic emphasises, but a viva will expect you to classify that ulcer and to assess it for underlying osteomyelitis - neither classification appears above.
Wagner classification (depth and gangrene):
- Grade 0 - intact skin, at-risk foot (deformity/callus, no ulcer).
- Grade 1 - superficial ulcer (skin only).
- Grade 2 - deeper ulcer to tendon, capsule or bone (no abscess/osteomyelitis).
- Grade 3 - deep ulcer with abscess or osteomyelitis.
- Grade 4 - localised (forefoot/heel) gangrene.
- Grade 5 - extensive gangrene of the whole foot.
University of Texas (UT) system - generally a better outcome predictor because it grades depth (0 to 3) AND stages infection/ischaemia (A to D): A = clean, B = infected, C = ischaemic, D = infected and ischaemic. Higher grade and stage independently predict non-healing and amputation, which Wagner (depth/gangrene only) captures less well.
Probe-to-bone (PtB) test: gently probing the ulcer base with a sterile blunt probe; palpable bone (or a positive probe) substantially raises the likelihood of osteomyelitis - in a high-prevalence ulcerated/Charcot foot a positive PtB has a high positive predictive value, and a negative PtB in a lower-risk setting helps argue against it. It complements the imaging above and bone biopsy (the gold standard for confirming osteomyelitis and guiding antibiotics).
Exam point: classify the Charcot ulcer with Wagner (depth plus gangrene) or, better for predicting outcome, the University of Texas system (depth grade 0-3 plus stage A-D for infection/ischaemia), and use the probe-to-bone test at the bedside as a high-yield pointer to underlying osteomyelitis.
Outcomes and Prognosis
- Treatment
- Immediate TCC, 3-4 months
- Expected Outcome
- No deformity develops, normal or near-normal foot architecture preserved
- Amputation Risk
- Less than 5 percent
- Treatment
- TCC 4-6 months, may avoid surgery
- Expected Outcome
- Moderate deformity possible, manageable with bracing
- Amputation Risk
- 5-10 percent
- Treatment
- TCC to completion, brace thereafter
- Expected Outcome
- Fixed deformity present but may be braceable
- Amputation Risk
- 10-15 percent
- Treatment
- Reconstruction or lifelong bracing
- Expected Outcome
- Variable — depends on deformity severity and surgical success
- Amputation Risk
- 15-30 percent
Best prognosis: Early diagnosis (Stage 0), compliant patient, adequate vascularity, diabetes well-controlled, midfoot location
Poor prognosis: Late diagnosis (Stage 3 with ulceration), ankle/hindfoot involvement, peripheral vascular disease, poor glycaemic control, non-compliant patient, active infection
Key threshold: The temperature differential. Normalisation of skin temperature (less than 1 degree Celsius difference) is the primary clinical marker that the acute phase has resolved and the foot can transition from TCC to bracing.
Guidelines, Registries & Global Practice
- Diabetes prevalence: Rising globally — projected 783 million adults by 2045 (IDF Atlas), driving increased Charcot incidence
- Underdiagnosis: Estimated 25-50 percent of acute Charcot episodes are initially misdiagnosed (as cellulitis, gout, DVT, or sprain)
- Geographic variation: Higher detection rates in centres with dedicated diabetic foot clinics; rural and low-resource settings have worse outcomes due to delayed referral
- Leprosy-related Charcot: Remains a significant cause in endemic regions (India, Brazil, parts of Africa and Southeast Asia)
- High-resource: TCC by trained orthotists, MRI for Stage 0, multidisciplinary foot clinics (diabetology, orthopaedics, vascular, orthotics)
- Middle-resource: Serial casting with plaster of Paris, plain radiograph-based staging, limited MRI access
- Low-resource: Empirical offloading with available materials, reliance on clinical staging, limited surgical reconstruction options
- Universal principle: Early offloading is limb-saving regardless of resource setting — TCC technique is learnable with minimal equipment
- Diagnosis
- Clinical suspicion + temperature monitoring + MRI for Stage 0
- Acute Treatment
- Immediate TCC or irremovable offloading device, non-weight-bearing
- Surgery / Reconstruction
- Consider when deformity is unstable or ulceration recurrent; staged approach
- Diagnosis
- High index of suspicion in neuropathic patients; urgent MRI if X-ray normal
- Acute Treatment
- Immediate offloading with TCC, specialist referral within 24 hours
- Surgery / Reconstruction
- Reconstruction in specialist centres; infection control before surgery
- Diagnosis
- Temperature monitoring, MRI for early detection, differentiate from osteomyelitis
- Acute Treatment
- TCC gold standard; iTCC acceptable alternative for compliance
- Surgery / Reconstruction
- Exostectomy, arthrodesis, or amputation based on deformity and infection
- Diagnosis
- Stage 0 recognition as clinical priority; emphasise dermathermometry
- Acute Treatment
- Offloading is the single most important intervention
- Surgery / Reconstruction
- Reconstruction after infection control; amputation for limb-threatening situations
There is no global Charcot-specific joint registry comparable to arthroplasty registries. The evidence base relies heavily on retrospective case series, expert consensus, and cohort studies from specialist centres. The IDF-IWGDF guidelines represent the broadest international consensus. Key data on amputation rates come from national diabetic foot audit programmes (e.g., the UK National Diabetes Foot Care Audit) which track outcomes including Charcot-related amputations as a subgroup.
Record in every diabetic foot presentation with swelling:
- Skin temperature measurement and comparison to contralateral foot (in degrees Celsius)
- Monofilament testing result (positive or loss of protective sensation)
- Eichenholtz stage with radiographic description
- TCC application date, technique, and planned duration
- Patient counselling on non-weight-bearing compliance and consequences of non-compliance
- Referral to multidisciplinary diabetic foot team
A missed or delayed Charcot diagnosis resulting in amputation is a significant source of medicolegal claims worldwide. The key defence is documented consideration of Charcot in every diabetic patient presenting with foot swelling.
Controversies & Areas of Uncertainty
IV pamidronate and oral alendronate have been trialled to reduce osteoclast activity during the acute Charcot phase. Results are inconsistent — some studies show reduced disease activity markers, others show no clinical benefit. Current guidance does not mandate bisphosphonates but they may be considered as an adjunct to TCC in severe or refractory cases.
Traditional teaching mandates strict non-weight-bearing during Stage 0-1. Some centres now allow partial weight-bearing in a TCC with a walking base, arguing that complete offloading is impractical for many patients and the TCC itself provides significant load redistribution. No high-quality RCTs settle this debate definitively.
The traditional dogma is to avoid surgery during acute Stage 0-1 due to high complication rates. However, some centres advocate early surgical stabilisation (particularly for ankle/hindfoot patterns with severe subluxation) to prevent further deformity. Evidence is limited to case series and no consensus exists.
Denosumab (RANKL inhibitor) and TNF-alpha blockers have theoretical appeal as disease-modifying agents targeting the inflammatory cascade in acute Charcot. Early case reports and small series suggest reduced disease activity, but no RCTs exist. These remain experimental and are not part of standard clinical practice.
MCQ Practice Points
Q: A diabetic patient presents with a warm, swollen foot. X-rays show osteopenia and early joint subluxation but no fragmentation. What Eichenholtz stage is this? A: This represents Stage 0 transitioning to Stage 1. The presence of osteopenia and subluxation suggests the destructive process has begun, but without overt fragmentation this is still an early presentation. Immediate TCC is essential to prevent progression to full Stage 1 with fragmentation. The key exam point is that Stage 0 has normal X-rays — any radiographic change means at least early Stage 1.
Q: How do you clinically differentiate acute Charcot from cellulitis in a diabetic patient? A: Charcot: afebrile, normal WBC, neuropathic, temperature differential greater than 2 degrees Celsius, no response to antibiotics, often bilateral joint involvement. Cellulitis: febrile, elevated WBC, may or may not be neuropathic, responds to antibiotics within 48-72 hours. The temperature differential and absence of systemic inflammatory response are the most reliable discriminators.
Q: What is a rocker-bottom deformity and how does it develop in Charcot? A: Rocker-bottom deformity is collapse of the medial longitudinal arch with plantar displacement of the midfoot bones. It develops when the tarso-metatarsal or naviculocuneiform joints undergo fragmentation and subluxation in Stage 1, allowing the cuneiforms to displace dorsally and the cuboid to become a plantar prominence. The normal concave longitudinal arch inverts to become convex, creating a "rocker" sole shape. The plantar cuboid prominence causes focal pressure, callus formation, and eventual ulceration.
Q: What is the gold standard treatment for acute Charcot and what is the criterion for discontinuing it? A: Total contact cast (TCC) is the gold standard for acute Charcot (Stage 0-1). The criterion for transitioning from TCC to bracing is skin temperature normalisation (less than 1 degree Celsius difference from contralateral foot) sustained over 4 weeks, combined with radiographic evidence of coalescence (Stage 2). Duration is typically 3-6 months, guided by clinical and radiographic resolution rather than a fixed timeframe.
Q: When is surgery indicated in Charcot neuroarthropathy? A: Surgery is indicated for: (1) recurrent ulceration despite optimal conservative management, (2) unstable deformity that cannot be braced, (3) progressive deformity despite TCC, (4) acute irreducible fracture-dislocation (especially ankle), and (5) deep infection requiring staged reconstruction. Surgery should NOT be performed during acute Stage 0-1 (high complication rate) unless there is an irreducible dislocation.
Q: What are the two complementary theories for the pathogenesis of Charcot neuroarthropathy? A: Neurotraumatic theory: Loss of protective sensation allows unrecognised repetitive microtrauma to the joint, with continued weight-bearing on an injured joint causing progressive destruction. Neurovascular theory: Autonomic neuropathy causes loss of sympathetic vasoconstriction, leading to increased bone blood flow, osteopenia, and structural weakness. Both mechanisms act together — the neuropathic bone is weakened by hyperaemia and then destroyed by unperceived mechanical stress.
Clinical Imaging
Imaging in Charcot Neuroarthropathy
Imaging is central to staging, monitoring, and surgical planning. Plain radiographs are first-line; MRI is reserved for Stage 0 (normal X-rays with clinical suspicion) and pre-operative planning. Serial radiographs at 4-6 week intervals track progression through Eichenholtz stages.
- Stage 0: Normal radiographs (MRI required to detect bone marrow oedema)
- Stage 1: Soft tissue swelling, joint subluxation, osteopenia, marginal fractures, bone fragmentation, joint debris
- Stage 2: Absorption of debris, periosteal new bone formation, fusion of large fragments, decreasing sclerosis
- Stage 3: Remodelled joint surfaces, mature bony consolidation, fixed deformity (rocker-bottom, medial arch collapse)
- Calcaneal pitch angle (less than 15 degrees suggests midfoot collapse)
- Meary angle (talar-first metatarsal angle deviation greater than 4 degrees indicates arch collapse)
- Cuboid height (less than 0 mm relative to the medial weight-bearing line indicates significant midfoot breakdown)
- Stage 0: Bone marrow oedema on T2/STIR sequences, capsular distension, soft tissue oedema
- Acute Charcot: Intense marrow oedema involving multiple bones, often centred on the midfoot tarso-metatarsal joints
- Differentiation from osteomyelitis: Charcot shows diffuse multi-bone oedema in a non-contiguous pattern, while osteomyelitis is usually focal with adjacent soft tissue ulcer and sinus tract
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old man with type 2 diabetes of 15 years duration presents with a 5-day history of sudden painless swelling and redness of his right foot. He is afebrile with normal white cell count. He has loss of protective sensation on monofilament testing. Skin temperature is 3.5 degrees Celsius higher than the left foot at the midfoot. Weight-bearing radiographs show subtle osteopenia at the tarso-metatarsal joints but no clear fracture or subluxation. What is your diagnosis and management?”
“A 62-year-old woman with type 2 diabetes and a 2-year history of Charcot midfoot presents with recurrent ulceration over the plantar cuboid. She has a fixed rocker-bottom deformity with Meary angle of 18 degrees. The ulcer is 2cm, probes to bone, with visible bone at the base. Temperature differential is 0.5 degrees Celsius. She has palpable pedal pulses. CRP is mildly elevated. How would you manage this?”
Key Pathophysiology
- Neurotraumatic: loss of protective sensation allows unrecognised microtrauma
- Neurovascular: autonomic neuropathy causes hyperaemia, osteopenia, structural weakness
- RANKL-mediated osteoclast activation drives exaggerated inflammatory bone resorption
- Diabetes is the most common cause (greater than 75 percent); others include syringomyelia, leprosy, alcohol neuropathy
Eichenholtz Staging (Exam Essential)
- Stage 0: Pre-radiographic — normal X-ray, MRI oedema, clinical suspicion — immediate TCC
- Stage 1: Development — fragmentation, bone resorption, subluxation — TCC, strict NWB
- Stage 2: Coalescence — debris absorbed, new bone, fusion — TCC to CROW boot transition
- Stage 3: Consolidation — remodelling complete, fixed deformity — brace or surgery
Diagnosis
- Clinical: warm swollen neuropathic foot with no systemic signs — Charcot until proven otherwise
- Temperature differential greater than 2 degrees Celsius = active Charcot (use dermathermometer)
- X-rays may be normal in Stage 0 — MRI confirms bone marrow oedema
- Differentiate from cellulitis (fever, WBC, antibiotic response) and osteomyelitis (focal, adjacent ulcer)
Management Algorithm
- Acute (Stage 0-1): Total contact cast, strict non-weight-bearing, 3-6 months
- Transition: CROW boot when temperature normalises (less than 1 degree Celsius differential)
- Chronic (Stage 3): Custom orthosis, accommodative footwear, lifelong monitoring
- Surgery: Recurrent ulceration, unstable deformity, progressive collapse — after infection eradicated
Rocker-Bottom Deformity
- Midfoot collapse inverts the longitudinal arch — cuboid becomes plantar prominence
- Meary angle greater than 4 degrees indicates arch collapse; greater than 15 degrees is severe
- Plantar prominence causes pressure, callus, ulceration, and deep infection
- Treatment: exostectomy (isolated) or midfoot arthrodesis (global instability)
Surgical Reconstruction
- Exostectomy: isolated plantar prominence with stable midfoot — ulcer healing 70-90 percent
- Midfoot arthrodesis: unstable deformity — medial and lateral column fusion, plantigrade in 70-85 percent
- Ankle/hindfoot fusion: tibiotalocalcaneal nail for ankle Charcot — high complication rate (30-50 percent)
- Amputation (BKA): unreconstructable deformity, uncontrolled infection, failed reconstruction
Complications & Prognosis
- Amputation risk: less than 5 percent with early Stage 0 treatment, 15-30 percent if late
- Bilateral Charcot develops in 9-75 percent — always monitor contralateral foot
- Nonunion after surgery: 10-20 percent midfoot, up to 30 percent ankle
- Five-year mortality post-Charcot amputation approaches 50 percent
Evidence Base and Key Trials
The Charcot foot in diabetes.
- International consensus on the diagnosis and management of Charcot foot in diabetes
- Temperature differential and MRI for early (Stage 0) detection are emphasised
- TCC remains the cornerstone of treatment
The natural history of acute Charcot's arthropathy in a diabetic foot specialty clinic.
- Prospective documentation of time to resolution with TCC
- Mean duration of acute phase approximately 4 months until temperature normalisation
- Low amputation rate with consistent offloading protocol
Charcot foot syndrome.
- Acute Charcot is a medical emergency requiring immediate offloading
- Skin temperature monitoring is critical for diagnosis and resolution assessment
- Pharmacological adjuncts have inconsistent evidence
Is the Eichenholtz classification still valid for the diabetic Charcot foot?
- Review affirming the continued clinical utility of Eichenholtz staging
- Stage 0 (pre-radiographic) is critical for early intervention
- Modern imaging supports but does not replace the original framework