Avulsion or Shear Fracture | High Association with Carpal Ligament Injury | ORIF Standard
- Chauffeur's fracture = radial styloid avulsion/shear fracture
- Historical name from hand-crank car starters causing direct blow injuries
- High association with scapholunate ligament injury - must assess on all cases
- Fragment size determines treatment - small fragments may be excised, larger need ORIF
- Greater arc injury pattern must be excluded - perilunate spectrum
- “Always assess for associated scapholunate ligament injury (30-50% incidence)
- “Fragment size greater than 5mm and articular step-off over 2mm = surgical indication
- “Headless compression screws preferred - avoids hardware prominence
- “Part of greater arc injury pattern - exclude perilunate dislocation
CRITICAL: 30-50% of Chauffeur's fractures have associated scapholunate ligament injury. This is the RSL ligament insertion site. Always obtain stress views or MRI/arthroscopy if clinical suspicion exists. Missing this leads to carpal instability.
Chauffeur's fracture may be part of a greater arc injury pattern (perilunate spectrum). The radial styloid fracture occurs instead of SL ligament rupture. Assess for lunate alignment, VISI/DISI, and perilunate dislocation.
Named after early automobile chauffeurs who sustained this injury from backfiring hand-crank starters. The crank would spin backwards, striking the radial styloid directly. Modern mechanism is usually ulnar deviation stress or direct trauma.
Headless compression screws (Herbert, Acutrak) are preferred for cosmesis and to avoid extensor tendon irritation. Plate fixation for comminuted or large fragments. Fragment excision only for small non-articular pieces with intact SL ligament.
- Fragment Size
- Under 5mm
- SL Ligament
- Intact
- Management
- Cast immobilization 4-6 weeks
- Fragment Size
- Under 5mm
- SL Ligament
- Intact
- Management
- Fragment excision if symptomatic
- Fragment Size
- 5-15mm
- SL Ligament
- Intact
- Management
- ORIF with headless screws
- Fragment Size
- Over 15mm
- SL Ligament
- Intact
- Management
- ORIF with plate or multiple screws
- Fragment Size
- Any
- SL Ligament
- Torn/lax
- Management
- ORIF + SL repair or reconstruction
- Fragment Size
- Variable
- SL Ligament
- Disrupted
- Management
- Address perilunate + ORIF styloid
CHAUFFEURCHAUFFEUR - Key Features
Hook:CHAUFFEUR reminds you to always assess for scapholunate ligament injury
Overview and Epidemiology
Definition
Chauffeur's fracture is an avulsion or shear fracture of the radial styloid process of the distal radius. This intra-articular fracture involves the lateral aspect of the radiocarpal joint and is critically associated with scapholunate ligament injury in 30-50% of cases.
- Accounts for approximately 5% of distal radius fractures
- Bimodal age distribution: young adults (sports/MVA) and elderly (falls)
- Male predominance in younger patients
- Equal sex distribution in osteoporotic fractures
- Often occurs in isolation or as part of greater arc injury
- High-energy trauma in young patients
- Contact sports (snowboarding, football, rugby)
- Motor vehicle accidents
- Falls on outstretched hand with ulnar deviation
- Osteoporosis in elderly patients
- Previous wrist injuries
Historical Context
The term "Chauffeur's fracture" originated in the early 20th century when automobile chauffeurs would manually start cars using hand-cranks. When the engine backfired, the crank would spin rapidly backwards, delivering a direct blow to the radial aspect of the wrist. This mechanism is now historical, but the eponym persists due to its descriptive anatomical accuracy.
Chauffeur's fracture is also known as "Hutchinson's fracture" (after Jonathan Hutchinson who described it) or simply "radial styloid fracture." In the exam, any of these terms may be used interchangeably.
Anatomy and Biomechanics
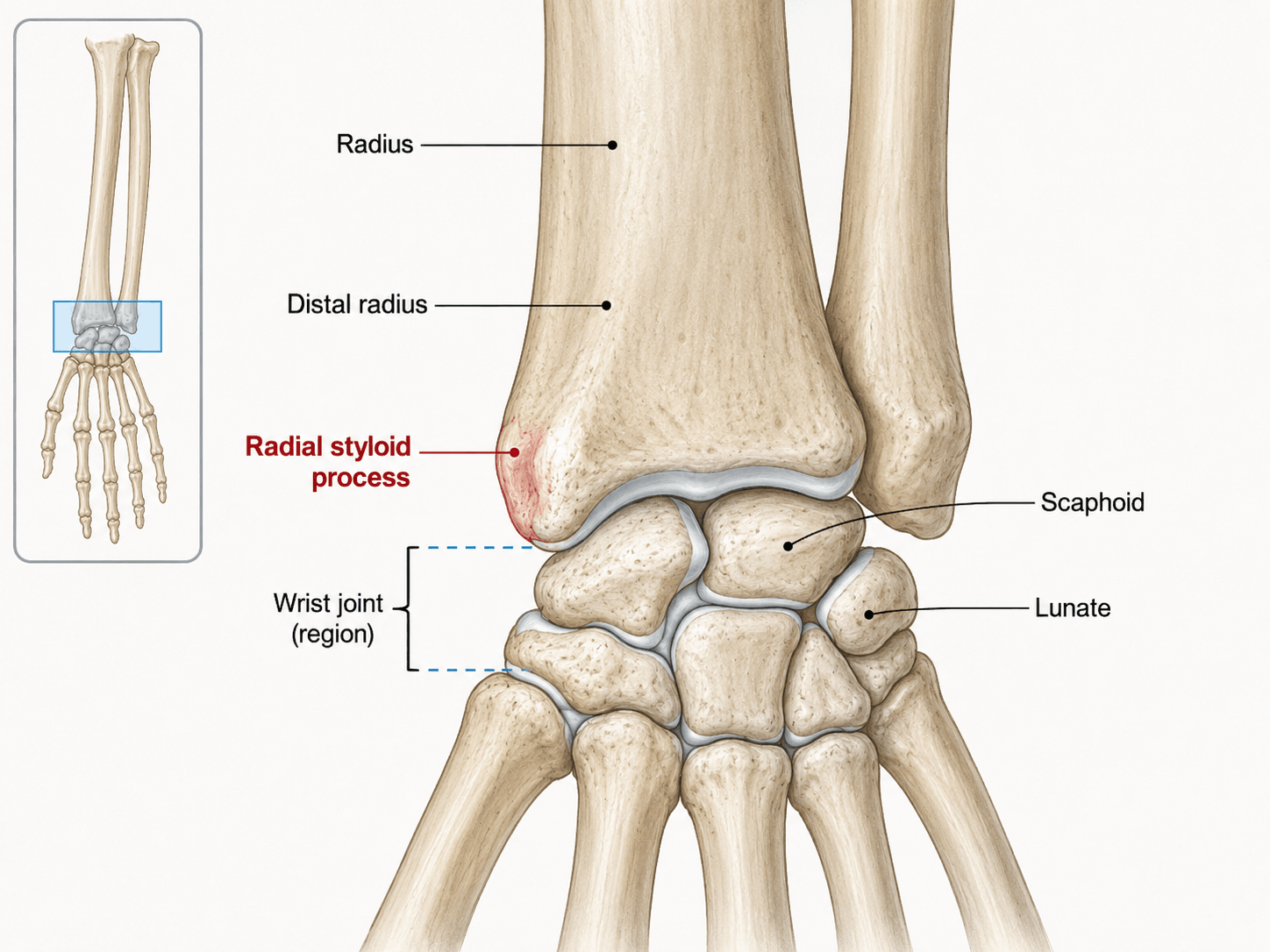
Radial Styloid Anatomy
The radial styloid is the distal lateral projection of the radius that articulates with the scaphoid fossa. It serves as the attachment point for critical ligamentous structures.
The radial styloid extends approximately 10-12mm distal to the ulnar margin of the articular surface. It provides a bony stop preventing excessive ulnar deviation. The styloid tip is covered by articular cartilage continuous with the scaphoid fossa. The styloid forms approximately 40% of the scaphoid fossa articular surface.
RSL ligament (radioscapholunate) and RSC ligament (radioscaphocapitate) attach to the volar aspect of the styloid. Brachioradialis tendon inserts on the lateral surface. The radial collateral ligament provides lateral stability. These attachments explain the ligament injury association.
Mechanism of Injury
Hand-crank starters on early automobiles would backfire, causing the crank to spin rapidly backwards. This delivered a direct blow to the radial aspect of the wrist, specifically impacting the radial styloid. This mechanism is now historical but gives the fracture its name.
The understanding of this mechanism highlights the injury pattern well.
Fracture Patterns
- Mechanism
- Ligament pull-off
- Fragment
- Small, cortical
- Prognosis
- Good if SL intact
- Mechanism
- Scaphoid impact
- Fragment
- Larger, articular
- Prognosis
- Requires anatomic reduction
- Mechanism
- High energy
- Fragment
- Multiple fragments
- Prognosis
- May need plate fixation
- Mechanism
- Perilunate spectrum
- Fragment
- Variable
- Prognosis
- Depends on overall injury
Classification Systems
The most clinically useful classification is based on fragment size, which directly guides treatment decisions.
Small Fragment (Under 5mm): Cortical avulsion with minimal articular involvement. May be managed non-operatively or with excision if symptomatic and SL ligament intact.
Medium Fragment (5-15mm): Articular involvement with variable stability. Requires ORIF with headless compression screws for anatomic reduction.
Large Fragment (Over 15mm): Significant articular surface, may be comminuted. Requires plate fixation or multiple screws for stable fixation.
Fragment size is the primary determinant of treatment strategy.

- Fragment Size
- Under 5mm
- Characteristics
- Cortical avulsion, minimal articular
- Treatment Approach
- Non-op or excision
- Fragment Size
- 5-15mm
- Characteristics
- Articular involvement, variable stability
- Treatment Approach
- Headless screw ORIF
- Fragment Size
- Over 15mm
- Characteristics
- Significant articular surface, may be comminuted
- Treatment Approach
- Plate or multiple screws
Clinical Assessment
History
- Fall on outstretched hand with ulnar deviation component
- Direct blow to radial wrist
- High-energy trauma (MVA, sports)
- Twisting injury to wrist
- Previous wrist injuries or instability symptoms
- Radial-sided wrist pain
- Swelling over radial styloid
- Weakness of grip
- Pain with ulnar deviation
- Associated numbness (median nerve)
Physical Examination
Swelling: Localized swelling over radial styloid is characteristic. More diffuse swelling suggests associated injuries.
Deformity: Obvious deformity may indicate significant displacement or associated perilunate injury.
Ecchymosis: Bruising over radial wrist develops within 24-48 hours.
Skin integrity: Assess for open injury, especially with high-energy mechanisms.
These inspection findings guide further examination.
Never clear a Chauffeur's fracture without assessing for scapholunate ligament injury. The radial styloid is the RSL ligament attachment - fracture here often indicates ligament stress. A negative Watson's test does not exclude partial tears. Consider MRI or arthroscopy if any clinical suspicion exists.
Differential Diagnosis
- Distinguishing feature
- Intra-articular styloid fragment, snuffbox/styloid tenderness
- Key investigation
- PA + pronated oblique radiograph
- Distinguishing feature
- Snuffbox and scaphoid tubercle tenderness, axial thumb pain
- Key investigation
- Scaphoid views; MRI/CT if occult
- Distinguishing feature
- No fracture; SL gap over 3mm, positive Watson test, DISI
- Key investigation
- Clenched-fist PA, MRI, arthroscopy
- Distinguishing feature
- Disrupted Gilula arcs, lunate malalignment on lateral
- Key investigation
- PA + lateral radiograph, CT
- Distinguishing feature
- Metaphyseal, dorsal/volar tilt, no articular styloid fragment
- Key investigation
- PA + lateral radiograph
- Distinguishing feature
- Chronic, positive Finkelstein, no trauma/fragment
- Key investigation
- Clinical; ultrasound
SLSL CHECK - Scapholunate Assessment
Hook:SL CHECK reminds you to thoroughly assess for scapholunate injury
Investigations
Imaging Protocol
PA, lateral, and oblique radiographs are mandatory. The 45° pronated oblique view best profiles the radial styloid. Look for fragment size, displacement, articular involvement, and associated injuries.
Clenched fist PA view assesses for dynamic scapholunate instability. Compare SL interval to contralateral side. Gap over 3mm or more than 2mm difference is abnormal.
Indicated for precise fragment measurement, assessing articular congruity, and surgical planning. Coronal and sagittal reconstructions helpful. 3D reconstructions aid in understanding complex patterns.
Gold standard for scapholunate ligament assessment. Also evaluates TFCC, other intercarpal ligaments, and occult fractures. Consider if any clinical suspicion of ligament injury.
Radiographic Assessment
- Size: Measure in mm on PA view
- Displacement: Distance from parent bone
- Articular step-off: Incongruity at joint surface
- Comminution: Single vs multiple fragments
- Orientation: Fracture line direction
- Scapholunate gap: Over 3mm (Terry Thomas sign)
- SL angle: Over 70° indicates DISI
- Lunate alignment: Assess for perilunate injury
- Ulnar styloid: Associated fracture common
- Carpal alignment: Greater arc injury pattern
Management Algorithm

STYLOIDSTYLOID - Surgical Indications
Hook:STYLOID helps remember when to operate on radial styloid fractures
Management
Indications for Conservative Treatment:
- Undisplaced fracture with under 2mm displacement
- Small fragment under 5mm without significant articular involvement
- Minimal articular step-off under 2mm
- Intact scapholunate ligament confirmed on imaging or examination
- Low-demand patient with minimal symptoms
Protocol:
- Short arm cast or splint for 4-6 weeks
- Wrist position in neutral or slight radial deviation
- Serial radiographs at 1, 2, and 4 weeks to monitor for displacement
- Transition to removable splint then hand therapy at 4-6 weeks
Non-operative management is only appropriate when SL ligament integrity is confirmed.
The most important management decision is NOT whether to operate on the styloid fracture, but whether there is associated scapholunate ligament injury. A well-fixed styloid fracture with a missed SL injury will have poor outcomes. Always assess SL integrity before finalizing management plan.
Surgical Technique
Preoperative Planning
- CT scan for precise fragment assessment
- MRI if ligament injury suspected
- Measure fragment size and displacement
- Assess articular surface involvement
- Identify comminution pattern
- Headless compression screws (Herbert, Acutrak) - multiple sizes
- Mini-fragment plate (2.0-2.4mm) as backup
- K-wires for provisional fixation
- Fluoroscopy unit
- Arm table and tourniquet
Surgical Approaches
Positioning: Supine with arm on hand table, tourniquet to upper arm.
Incision: Longitudinal incision over FCR tendon, curving radially at wrist crease.
Dissection: Incise FCR sheath, retract tendon ulnarly. Incise floor of sheath to expose pronator quadratus.
Exposure: Elevate pronator quadratus radially to expose fracture. Extend incision distally as needed for radial styloid visualization.
Advantages: Protects superficial radial nerve, excellent visualization, familiar approach.
This approach is preferred for most cases.
Fixation Techniques
Indications: Medium fragments (5-15mm), non-comminuted fractures.
Technique:
- Reduce fragment anatomically under direct vision
- Hold reduction with K-wire
- Insert guidewire perpendicular to fracture line
- Measure screw length (typically 18-24mm)
- Countersink screw head below articular cartilage
- Remove K-wire after final tightening
Tips: Use cannulated system, bury head completely to avoid chondral damage.
Headless screws provide excellent compression with minimal hardware prominence.
A percutaneous radial styloid screw is tempting and often appropriate, but the tip of the radial styloid is crowded with structures that a blind percutaneous guidewire/screw can injure:
- The superficial (sensory) branch of the radial nerve crosses the radial styloid subcutaneously - tethered or transfixed by a percutaneous wire it produces a painful neuroma and dorsoradial numbness.
- The radial artery passes just volar-radial to the styloid (toward the snuffbox).
- The first dorsal extensor compartment (APL and EPB) lies directly over the styloid.
So for any percutaneous styloid screw, make a small open incision and bluntly spread down to bone (mini-open), protecting the superficial radial nerve and the first-compartment tendons, before drilling - do not pass the wire through a stab incision blind. Direct the screw perpendicular to the fracture, from the styloid tip proximally and ulnarward into the radial metaphysis, with subchondral but not intra-articular purchase (confirm on multiple fluoroscopic views).
Exam point: the radial styloid entry endangers the superficial radial nerve, radial artery and first dorsal compartment - use a mini-open, soft-tissue-protected technique for the styloid screw, not a blind percutaneous pass.
Scapholunate Ligament Repair
When SL injury is identified at surgery:
Determine tear pattern: partial dorsal, partial volar, or complete. Assess tissue quality - acute tears are amenable to repair, chronic may require reconstruction.
Reduce scapholunate interval to anatomic position using K-wires or reduction clamp. Confirm reduction fluoroscopically.
Place K-wires from scaphoid to lunate (2 wires) and scaphoid to capitate (1 wire). For acute tears, repair with suture anchors to dorsal capsule.
K-wires remain for 6-8 weeks. Longer immobilization compared to isolated styloid fractures.
Complications
- Infection: Standard surgical site infection risk
- Nerve injury: Superficial radial nerve at risk with dorsal approach
- Tendon injury: Extensor tendons with dorsal approach
- Hardware prominence: Especially with screws not countersunk
- Loss of reduction: If fixation inadequate
- Radiocarpal arthritis: From articular incongruity or chondral damage
- Carpal instability: Missed or inadequately treated SL injury
- Malunion: Radial shortening, altered kinematics
- Nonunion: Rare with adequate fixation
- Stiffness: From prolonged immobilization
Missed SL Injury: Leads to SLAC wrist. The most significant complication.
Assess First: Well-fixed styloid + Missed SL = Failure.
Styloid-Scaphoid: Arthritis at the radial styloid articulation.
Sequential Collapse: RS → Capitolunate → Pancarpal arthritis.
- Pathology
- Styloid-scaphoid arthritis
- Radiographic Finding
- Osteophytes at radial styloid
- Treatment
- Styloidectomy + SL procedure
- Pathology
- Radioscaphoid arthritis
- Radiographic Finding
- Joint space narrowing RS joint
- Treatment
- Scaphoid excision + 4-corner fusion
- Pathology
- Capitolunate arthritis
- Radiographic Finding
- CL joint involvement
- Treatment
- Scaphoid excision + 4-corner fusion
- Pathology
- Pancarpal arthritis
- Radiographic Finding
- Radiolunate involvement
- Treatment
- Wrist fusion or PRC (limited)
Postoperative Care and Rehabilitation
Postoperative Protocol
Immobilization: Volar splint or short arm cast. Elevation and ice for swelling. Finger range of motion exercises encouraged. Wound check at 10-14 days, suture removal.
Protected mobilization: Removable wrist splint. Begin gentle wrist ROM exercises. Avoid forceful gripping or loading. If SL repair performed, maintain K-wires and splint.
Progressive therapy: K-wire removal if used for SL repair (typically 6-8 weeks). Progress ROM exercises. Begin strengthening as tolerated. Wean from splint.
Strengthening phase: Progressive grip strengthening. Gradual return to activities. Sport-specific training if applicable.
Return to activity: Full activities when strength 80% of contralateral side. Contact sports may require longer. Consider protective splint for high-risk activities.
- Full wrist range of motion
- Grip strength within 80% of contralateral
- Pain-free activities of daily living
- Return to work/sport
- No signs of carpal instability
- 2 weeks: Wound check, suture removal
- 6 weeks: Radiographs, K-wire removal if applicable
- 3 months: Clinical and radiographic assessment
- 6 months: Final assessment, discharge if stable
- PRN: If symptoms recur
Outcomes and Prognosis
Expected Outcomes
- Union Rate
- Over 95%
- ROM Recovery
- Near full
- Return to Activity
- 6-8 weeks
- Satisfaction
- High
- Union Rate
- Over 95%
- ROM Recovery
- Near full
- Return to Activity
- 8-12 weeks
- Satisfaction
- High
- Union Rate
- Over 95%
- ROM Recovery
- Near full
- Return to Activity
- 10-14 weeks
- Satisfaction
- High
- Union Rate
- Over 90%
- ROM Recovery
- 80-90% of normal
- Return to Activity
- 12-16 weeks
- Satisfaction
- Moderate-High
- Union Rate
- Variable
- ROM Recovery
- Progressive decline
- Return to Activity
- N/A
- Satisfaction
- Poor
Prognostic Factors
- Isolated styloid fracture without SL injury
- Fragment over 5mm (allows stable fixation)
- Anatomic reduction achieved
- Early treatment (under 2 weeks)
- Compliant patient with rehabilitation
- Associated scapholunate ligament injury
- Greater arc perilunate injury
- Delayed diagnosis (over 2 weeks)
- Articular step-off over 2mm
- Comminuted fracture pattern
- Osteoporotic bone quality
The single most important prognostic factor is the presence or absence of scapholunate ligament injury. Isolated styloid fractures have excellent outcomes with over 90% patient satisfaction. However, unrecognized SL injury leads to progressive carpal instability and SLAC wrist, with markedly worse long-term outcomes.
Guidelines, Registries & Global Practice
Radial styloid (chauffeur's) fractures sit within the broader distal radius fracture population, the second commonest fracture treated after the proximal femur. The figures below give the candidate a worldwide picture plus the regional guidance differences they may be examined on.
Global Epidemiology
- Incidence
- Distal radius 203/100,000/yr
- Key demographic finding
- Female 323 vs male 93/100,000/yr; sharp rise in women over 50
- Incidence
- 22/10,000/yr (women 34, men 10)
- Key demographic finding
- Incidence fell 24% from 2001 to 2016, driven by patients over 50
- Incidence
- Among most common fractures, 2nd to hip in elderly
- Key demographic finding
- Bimodal: high-energy young adults and fragility falls in elderly
Radial styloid fractures account for roughly 5% of distal radius fractures and show a bimodal pattern: high-energy shear in young adults (sport, motor vehicle, fall on outstretched hand in ulnar deviation) and low-energy fragility avulsions in older, osteoporotic patients. The strong female predominance and the post-menopausal surge seen for distal radius fractures overall apply to the fragility subgroup.
- Overall distal forearm fracture incidence 207.7/100,000/yr
- Distal radius fracture incidence 203.0/100,000/yr
- Female incidence 323.4 vs male 93.3/100,000/yr
- Most common mechanism a fall from standing height (76%)
Guidelines Side by Side
- Position relevant to radial styloid
- Operative fixation suggested for post-reduction articular step / displacement; weak evidence for any single fixation construct
- Evidence level
- Moderate to limited
- Position relevant to radial styloid
- Senior assessment, CT for intra-articular patterns, fix displaced articular fractures to restore congruity, document neurovascular status
- Evidence level
- Consensus / good practice
- Position relevant to radial styloid
- Anatomic reduction of the articular surface; lag/headless screw for the styloid fragment, plate if comminuted; address carpal ligament injury
- Evidence level
- Expert / technique standard
- Position relevant to radial styloid
- Individualised: tolerate minor displacement in low-demand patients, fix displaced articular fractures in active patients
- Evidence level
- Consensus
Across all bodies the recurring quantitative thresholds are an articular step-off over 2mm and fragment displacement over 2mm as triggers for fixation - the Knirk and Jupiter step-off evidence underpins this internationally.
Registry and Practice Variation
No joint registry tracks isolated radial styloid fractures (registries capture arthroplasty and major fracture-fixation implants rather than wrist trauma), so registry-grade implant survival data are not available for this injury - a point worth stating rather than fabricating. Practice variation instead centres on three areas:
- Fixation choice - headless compression screws dominate in high-resource settings for the small/medium styloid fragment; K-wire fixation remains a valid, lower-cost option and predominates in resource-limited settings.
- Ligament work-up - routine MRI or wrist arthroscopy for scapholunate assessment is common in specialist hand units but selective elsewhere, reflecting access rather than disagreement on the 30-50% association.
- Threshold for surgery - more aggressive operative management of articular fractures in younger, active populations versus acceptance of minor displacement in elderly low-demand patients, consistent across guidelines.
For any board worldwide, candidates should quote the over 2mm articular step / displacement surgical threshold, the 30-50% scapholunate association, and the principle of addressing carpal ligament injury at the index procedure.
Chauffeur's fractures are NOT just radial styloid fractures - they are markers for potential scapholunate ligament injury in 30-50% of cases. The radial styloid is the RSL ligament attachment, so fracture here means the ligament has been stressed. Always obtain stress views or advanced imaging, and be prepared to address ligament pathology at surgery. Missing scapholunate injury leads to SLAC wrist and poor long-term outcomes. Fragment size over 5mm with over 2mm displacement requires ORIF - headless compression screws are preferred. Remember: treat the fracture AND the ligament.
MCQ Practice Points
High-Yield MCQ Topics
- Radial styloid extends 10-12mm beyond ulnar articular margin
- RSL and RSC ligaments attach to volar styloid
- Brachioradialis inserts on lateral styloid
- Scaphoid fossa articulates with scaphoid
- Styloid provides buttress against ulnar deviation
- Small fragment: under 5mm
- Medium fragment: 5-15mm
- Large fragment: over 15mm
- Greater arc: injury through bone
- Lesser arc: injury through ligaments
- Terry Thomas sign: SL gap over 3mm
- DISI pattern: SL angle over 70°
- Articular step-off threshold: 2mm
- Pronated oblique view best profiles styloid
- Clenched fist view for dynamic SL instability
- Surgical threshold: fragment over 5mm with displacement
- Headless screws preferred for most cases
- SL repair: K-wires 6-8 weeks
- Non-op: under 2mm displacement, SL intact
- Fragment excision: only if SL confirmed intact
Key Exam Pearls for MCQs
Q: What percentage of Chauffeur's fractures have associated scapholunate ligament injury? A: 30-50% of Chauffeur's fractures have associated scapholunate ligament injury. This is one of the highest rates among distal radius fracture patterns and must be actively assessed in every case.
Q: What fragment sizes guide treatment in Chauffeur's fractures? A: The key numbers are 5mm and 15mm. Under 5mm fragments may be excised if SL is intact. 5-15mm fragments require headless screw fixation. Over 15mm fragments may need plate fixation.
Q: What is the scapholunate gap threshold for diagnosis on plain radiographs? A: The scapholunate gap threshold is 3mm (not 2mm) on PA view. Named after the gap-toothed British comedian. Dynamic widening on clenched fist view is also significant.
Q: What type of perilunate injury is Chauffeur's fracture classified as? A: Chauffeur's fracture is a greater arc injury component where energy travels through bone instead of ligament. Lesser arc injuries are pure ligamentous with perilunate dislocation.
Q: What is the articular step-off threshold for surgical intervention? A: Greater than 2mm of articular step-off is an absolute surgical indication. This threshold is based on studies showing correlation with post-traumatic arthritis.
Q: When should associated SL ligament injury be addressed? A: All associated pathology should be addressed at the index surgery. Staged procedures for SL ligament injury have demonstrably worse outcomes than primary repair.
Common MCQ Traps
- Trap: Assuming isolated styloid fracture without checking SL ligament
- Trap: Treating based on fragment size alone without assessing SL
- Trap: Missing greater arc injury component
- Trap: Using Terry Thomas sign threshold of 2mm (correct is 3mm)
- Trap: Excising fragment without confirming SL integrity
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old male presents after a fall while snowboarding. Radiographs show a displaced radial styloid fracture with a 12mm fragment. How would you assess and manage this patient?”
“During surgery for a Chauffeur's fracture, you find the scapholunate ligament is torn. How do you manage this?”
“A patient returns 2 years after a Chauffeur's fracture that was treated non-operatively. They have radial wrist pain with gripping. Radiographs show Stage II SLAC wrist. Discuss the pathophysiology and management options.”
Definition & Mechanism
- Chauffeur's = radial styloid avulsion/shear fracture
- Also known as Hutchinson's fracture
- Historical: hand-crank car starter backfire injury
- Modern: forced ulnar deviation, direct trauma, greater arc injury
- RSL/RSC ligament attachment site explains ligament injury association
Critical Associations
- 30-50% have scapholunate ligament injury
- May be part of greater arc perilunate spectrum
- RSL ligament attaches at radial styloid
- ALWAYS assess SL ligament in every case
Surgical Indications
- Fragment over 5mm with displacement
- Articular step-off over 2mm
- Any displacement over 2mm
- Associated scapholunate injury
- Greater arc / perilunate injury
Treatment Options
- Small undisplaced: cast 4-6 weeks
- Small displaced: excision if SL intact
- Medium/large: headless screw ORIF
- Comminuted: plate fixation
- With SL injury: ORIF + SL repair
Key Numbers
- 5mm = fragment size threshold for ORIF
- 2mm = displacement and step-off surgical threshold
- 3mm = SL gap (Terry Thomas sign)
- 70° = SL angle indicating DISI
- 30-50% = SL ligament injury incidence
Complications
- Missed SL injury → SLAC wrist
- SLAC Stage I: styloid-scaphoid arthritis
- SLAC Stage II-III: scaphoid excision + 4-corner fusion
- Hardware prominence with non-countersunk screws
- Radiocarpal arthritis from step-off
Evidence and Guidelines
- Prospective arthroscopic study of 51 patients with displaced distal radius fractures
- Grade-3 scapholunate tears in 20% (10/51); SL injury of any grade reported in up to 54%
- Ulnar variance increase over 2mm gave a fourfold risk of grade-3 SL injury
- Radial styloid fractures were predictive of SL injury
- Arthroscopic evaluation recommended for 'at risk' patterns
- Landmark study on articular congruity
- Accurate restoration of articular surface is critical
- Step-off >2mm inevitably leads to arthritis
- Long-term outcomes correlate directly with reduction quality
- Multicentre series of 166 perilunate dislocations / fracture-dislocations
- Greater arc (transosseous) vs lesser arc (purely ligamentous) classification
- Radial styloid fracture classified as greater arc injury
- 25% of perilunate injuries are missed initially
- Emphasized need for vigilant radiographic assessment
- Classic classification of 4 parts: shaft, styloid, dorsal medial, volar medial
- Described the 'die-punch' mechanism
- Highlighted the instability of the radial styloid fragment
- Basis for modern fragment-specific fixation