Chronic Nonbacterial Osteomyelitis and CRMO
Recognise sterile recurrent bone inflammation, exclude dangerous mimics and treat disease burden
Practical Disease Spectrum
Critical Must-Knows
- CNO is a sterile autoinflammatory bone disease, not recurrent bacterial osteomyelitis.
- The usual presentation is recurrent bone pain, sometimes with swelling, limp or back pain.
- Blood tests may be normal or mildly inflammatory; no single blood test confirms the diagnosis.
- Whole-body MRI detects multifocal and silent lesions and is central for diagnosis and monitoring.
- Biopsy is appropriate when disease is unifocal, aggressive, atypical or not safely distinguished from infection or malignancy.
Clinical Pearls
- "Do not label a solitary aggressive bone lesion as CRMO until malignancy and infection have been excluded.
- "Spinal disease matters because vertebral height loss can lead to kyphosis, scoliosis or neurological risk.
- "Antibiotics are not disease-modifying treatment for CNO unless bacterial infection is proven.
- "The orthopaedic role is recognition, safe biopsy when needed, fracture or deformity protection, and avoiding unnecessary operations.
- "Ask about psoriasis, palmoplantar pustulosis, inflammatory bowel symptoms, arthritis and family inflammatory disease.
The key error is treating sterile inflammatory disease as repeated infection
Persistent or recurrent multifocal bone pain with negative cultures should not automatically lead to repeated antibiotic courses and repeated debridement. The dangerous balance is to recognise CNO early while still excluding infection, malignancy and other mimics when the pattern is atypical.
STERILECNO Safety Check
| S | Spine Look for back pain and vertebral lesions. |
| T | Tumour Exclude malignancy when imaging is aggressive or unifocal. |
| E | Exclude infection Cultures and clinical sepsis features still matter. |
| R | Rheumatology Early multidisciplinary care improves treatment decisions. |
| I | Inflammatory associations Ask about skin, gut, joints and family history. |
| L | Lesion burden Whole-body MRI maps silent disease. |
| E | Escalate when high risk Spine, mandible, destructive lesions and NSAID failure need action. |
| S | Spine Look for back pain and vertebral lesions. | R | Rheumatology Early multidisciplinary care improves treatment decisions. | E | Escalate when high risk Spine, mandible, destructive lesions and NSAID failure need action. |
| T | Tumour Exclude malignancy when imaging is aggressive or unifocal. | I | Inflammatory associations Ask about skin, gut, joints and family history. | ||
| E | Exclude infection Cultures and clinical sepsis features still matter. | L | Lesion burden Whole-body MRI maps silent disease. |
Hook:STERILE keeps the assessment focused on diagnosis safety and disease burden.
ATYPICWhen to Biopsy
| A | Aggressive imaging Permeative destruction, mass or rapid progression. |
| T | Toxic child Fever, sepsis or systemic illness argues against simple CNO. |
| Y | Young or unusual pattern Very atypical age or site reduces diagnostic confidence. |
| P | Persistent single lesion Unifocal disease often needs tissue diagnosis. |
| I | Infection not excluded Culture and histology may be required. |
| C | Cytopenia or cancer concern Do not miss leukaemia, Ewing sarcoma or osteosarcoma. |
| A | Aggressive imaging Permeative destruction, mass or rapid progression. | Y | Young or unusual pattern Very atypical age or site reduces diagnostic confidence. | I | Infection not excluded Culture and histology may be required. |
| T | Toxic child Fever, sepsis or systemic illness argues against simple CNO. | P | Persistent single lesion Unifocal disease often needs tissue diagnosis. | C | Cytopenia or cancer concern Do not miss leukaemia, Ewing sarcoma or osteosarcoma. |
Hook:ATYPIC is the biopsy trigger: atypical, aggressive or unsafe-to-label disease.
SPINETreatment Escalation
| S | Spinal lesions Vertebral disease can collapse and deform. |
| P | Persistent pain Pain despite first-line therapy suggests active disease. |
| I | Imaging progression MRI progression means disease is not controlled. |
| N | Non-functional child Limp, school absence or activity loss changes urgency. |
| E | Erosive or destructive site Mandible, vertebrae or structural lesions need escalation. |
| S | Spinal lesions Vertebral disease can collapse and deform. | N | Non-functional child Limp, school absence or activity loss changes urgency. |
| P | Persistent pain Pain despite first-line therapy suggests active disease. | E | Erosive or destructive site Mandible, vertebrae or structural lesions need escalation. |
| I | Imaging progression MRI progression means disease is not controlled. |
Hook:SPINE highlights the high-risk situations where watchful waiting may be unsafe.
Overview and Epidemiology
Chronic nonbacterial osteomyelitis, or CNO, is a sterile autoinflammatory disorder of bone. Chronic recurrent multifocal osteomyelitis, or CRMO, describes the recurrent multifocal end of the same spectrum. The name is confusing because it contains the word osteomyelitis, but the disease is not primarily bacterial.
The practical clinical problem is a child or adolescent with recurrent bone pain, imaging evidence of osteitis and no microbiological proof of infection. Some children have a single symptomatic lesion. Others have multiple symptomatic and silent lesions in the long-bone metaphyses, clavicle, spine, pelvis, sternum, mandible or foot.
What CNO Explains
Recurrent focal bone pain, waxing and waning symptoms, multifocal MRI lesions, negative cultures, sterile biopsy inflammation and associated inflammatory conditions.
What CNO Must Not Hide
Ewing sarcoma, osteosarcoma, leukaemia, Langerhans cell histiocytosis, bacterial osteomyelitis, stress fracture, non-accidental injury and spinal infection.
Why It Matters
CNO is commonly delayed because the first X-ray can be normal, the symptoms can resemble injury or infection, and the child may look well between flares. Delay matters because untreated disease can cause chronic pain, functional limitation, pathological fracture, vertebral collapse, angular deformity, limb-length problems or unnecessary surgery.
The topic is important for orthopaedics because the child often enters the system through fracture clinic, tumour clinic, emergency department or infection pathway. The orthopaedic surgeon must know when to biopsy, when not to debride, when to protect a painful bone, and when to involve paediatric rheumatology early.
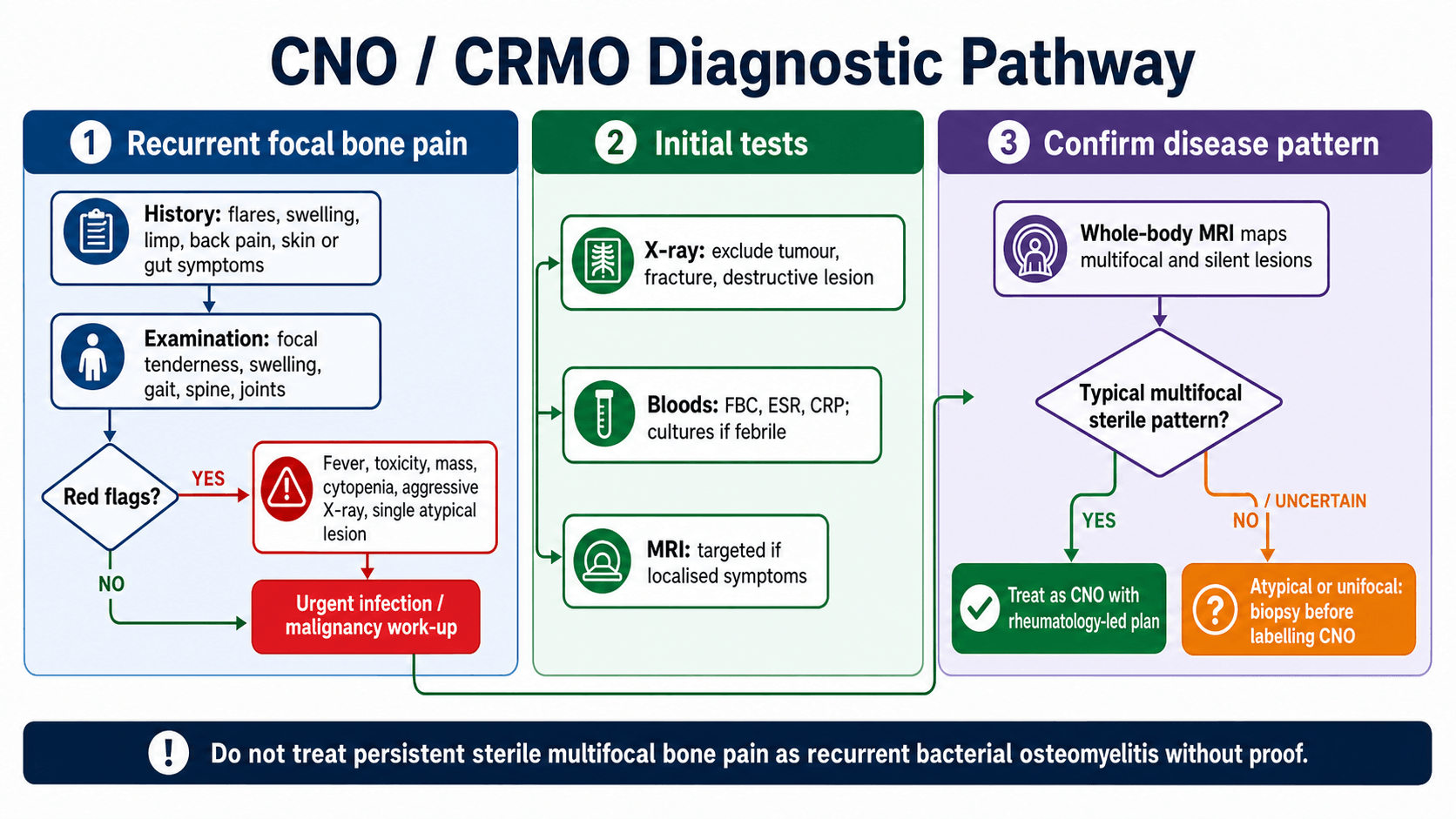
The Three Decisions
| Decision | Question to answer | Why it matters |
|---|---|---|
| Is it safe to call this CNO? | Is the clinical and MRI pattern typical, or are infection and malignancy still plausible? | A missed tumour or bacterial infection is the serious diagnostic failure. |
| How much disease is present? | Are there silent lesions on whole-body MRI, especially spine or pelvis? | Clinical symptoms underestimate burden in many children. |
| How aggressive should treatment be? | Is pain controlled, function preserved and MRI stable? | Spine, mandible, destructive lesions and NSAID failure justify escalation. |
Pathophysiology
CNO is best understood as disordered innate immune regulation causing sterile bone inflammation. The exact pathway is not one single gene or one single cytokine for most children. Contemporary reviews describe imbalance between pro-inflammatory and anti-inflammatory signalling, inflammasome activation and osteoclast-mediated bone injury as important themes.
The pathology is osteitis without a proven bacterial driver. Bone biopsy, when performed, may show inflammatory infiltrate, chronic sterile osteomyelitis-like change, fibrosis or sclerosis, but it does not provide a pathognomonic signature. This is why the diagnosis is made from the whole clinical, laboratory, imaging and sometimes histological pattern.
Disease Biology in Practical Terms
| Concept | Meaning | Clinical implication |
|---|---|---|
| Autoinflammatory disease | Innate immune dysregulation produces bone inflammation. | Anti-inflammatory and immunomodulatory treatment is logical when infection is excluded. |
| Sterile osteitis | Cultures are negative unless there is a separate infection. | Antibiotics do not treat CNO itself. |
| Multifocal tendency | Silent lesions may exist away from the painful site. | Whole-body MRI can change both diagnosis and risk stratification. |
| Growth-related distribution | Lesions often involve metaphyseal, epiphyseal or apophyseal regions. | Pain near growth plates should not be dismissed as growing pains when recurrent or focal. |
| Spinal vulnerability | Vertebral inflammation may lead to height loss or deformity. | Back pain or spinal lesions justify urgent MRI review and treatment escalation. |
Classification
CNO is best classified clinically by distribution, risk and diagnostic certainty. This is more useful than trying to force the condition into a fracture-style grading system.
Distribution Pattern
| Pattern | Meaning | Use |
|---|---|---|
| Unifocal CNO | One apparent lesion. | Treat the diagnosis as less secure unless the pattern is classic; biopsy is often needed. |
| Multifocal CNO | Several symptomatic or MRI-detected lesions. | Supports CNO when infection and malignancy are not suggested. |
| CRMO | Recurrent multifocal disease with flares over time. | Longitudinal treatment and monitoring are needed. |
| Silent disease | MRI lesions without local symptoms. | Explains why whole-body MRI changes diagnosis and follow-up. |
Clinical Presentation
Typical History
Children usually present with recurrent or persistent bone pain. The pain may flare, settle and recur at the same or different sites. Limp, activity limitation, focal swelling and local tenderness are common. Fever is absent or low-grade in many children; marked toxicity is a warning against uncomplicated CNO.
Important history points are not generic. They are chosen to separate CNO from infection, malignancy, stress injury and inflammatory disease:
History That Changes the Diagnosis
| History domain | Ask about | Interpretation |
|---|---|---|
| Pain pattern | Focal recurrent bone pain, night pain, flare duration, rest pain, activity link and response to NSAIDs. | Recurrent flares fit CNO; progressive relentless pain or severe night pain needs tumour and infection exclusion. |
| Systemic symptoms | Fever, weight loss, anorexia, night sweats, lethargy or recurrent infection. | Toxicity, weight loss or cytopenia pattern should not be attributed to CNO without work-up. |
| Inflammatory associations | Psoriasis, palmoplantar pustulosis, acne, arthritis, enthesitis, inflammatory bowel symptoms and family history. | CNO may coexist with inflammatory skin, gut or joint disease. |
| Site-specific symptoms | Back pain, stiffness, jaw pain, clavicular swelling, chest wall pain, foot pain or pelvic pain. | Spine, mandible, clavicle and pelvis are important CNO sites and may alter treatment urgency. |
| Infection clues | Recent skin infection, puncture wound, bacteremia risk, immunosuppression, antibiotics and culture results. | A bacterial source changes the pathway completely. |
| Trauma and loading | Sports load, recent increase in training, single-site mechanical pain and fracture history. | Stress injury can mimic CNO, especially in adolescents. |
Examination
Examination should localise symptomatic lesions and look beyond the painful bone. Inspect gait, posture, spine, limb alignment, local swelling, warmth, tenderness, joint motion and neurovascular status. Examine skin and nails for psoriasis or pustulosis. Check jaw opening, clavicles, sternoclavicular joints and spine when symptoms suggest those regions.
Examine the spine deliberately
Back pain in suspected CNO is not a minor symptom. Vertebral lesions can be silent or painful and may progress to height loss, kyphosis or scoliosis. Whole-body MRI should include adequate sagittal spinal assessment.
Imaging and Investigations
Plain Radiographs
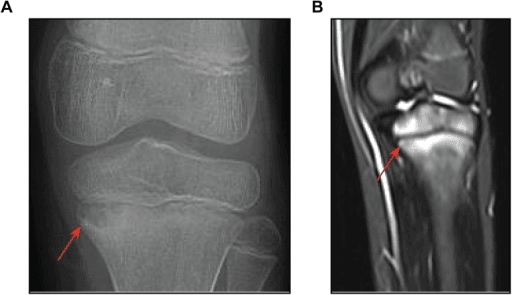
Radiographs are often the first test because they are accessible and help exclude fracture, aggressive tumour, chronic infection and structural damage. Early radiographs may be normal. Established lesions may be lytic, sclerotic, mixed, expansile or show periosteal reaction. Radiographs are useful for structural complications, but they do not map disease burden.
Blood Tests
Order full blood count, ESR and CRP. Results can be normal, mildly raised or inflammatory. The absence of a marked inflammatory response does not exclude CNO. However, cytopenia, very high inflammatory markers, bacteremia, toxic appearance or persistent fever should push the assessment back toward infection, malignancy or systemic disease.
MRI
MRI is the central imaging test. Targeted MRI defines a symptomatic site, marrow oedema, periosteal reaction, soft-tissue inflammation, abscess-like appearances and structural damage. Whole-body MRI is preferred when CNO is suspected because it detects silent lesions and typical distribution patterns.
MRI Interpretation
| MRI issue | Typical CNO finding | Why it matters |
|---|---|---|
| Distribution | Multifocal lesions, often metaphyseal or periphyseal, with clavicle, spine, pelvis, sternum or mandible possible. | Multifocal typical distribution supports CNO and may avoid biopsy in selected cases. |
| STIR signal | Bright marrow signal at active lesions. | STIR whole-body MRI is sensitive for disease burden and follow-up. |
| Spine | Vertebral body oedema, endplate involvement or height loss may be seen. | Spinal lesions require careful monitoring because collapse and deformity can occur. |
| Soft-tissue mass | A large mass is not typical for uncomplicated CNO. | Mass, aggressive destruction or atypical unifocal disease should trigger biopsy. |
| Abscess | True pus collection is not expected in sterile CNO. | Abscess shifts the diagnosis toward bacterial infection until proven otherwise. |
Biopsy
Biopsy is not required for every child, but it is mandatory when the diagnosis is not secure. The biopsy should be planned like a tumour or infection biopsy: correct compartment, safe tract, cultures and histology, and avoidance of contaminating future surgical planes.
When to Biopsy
Biopsy is appropriate for unifocal disease, aggressive radiographic appearance, soft-tissue mass, systemic illness, cytopenia, persistent fever, unusual age, atypical site, poor response to initial treatment or any case where infection or malignancy remains plausible.
Differential Diagnosis
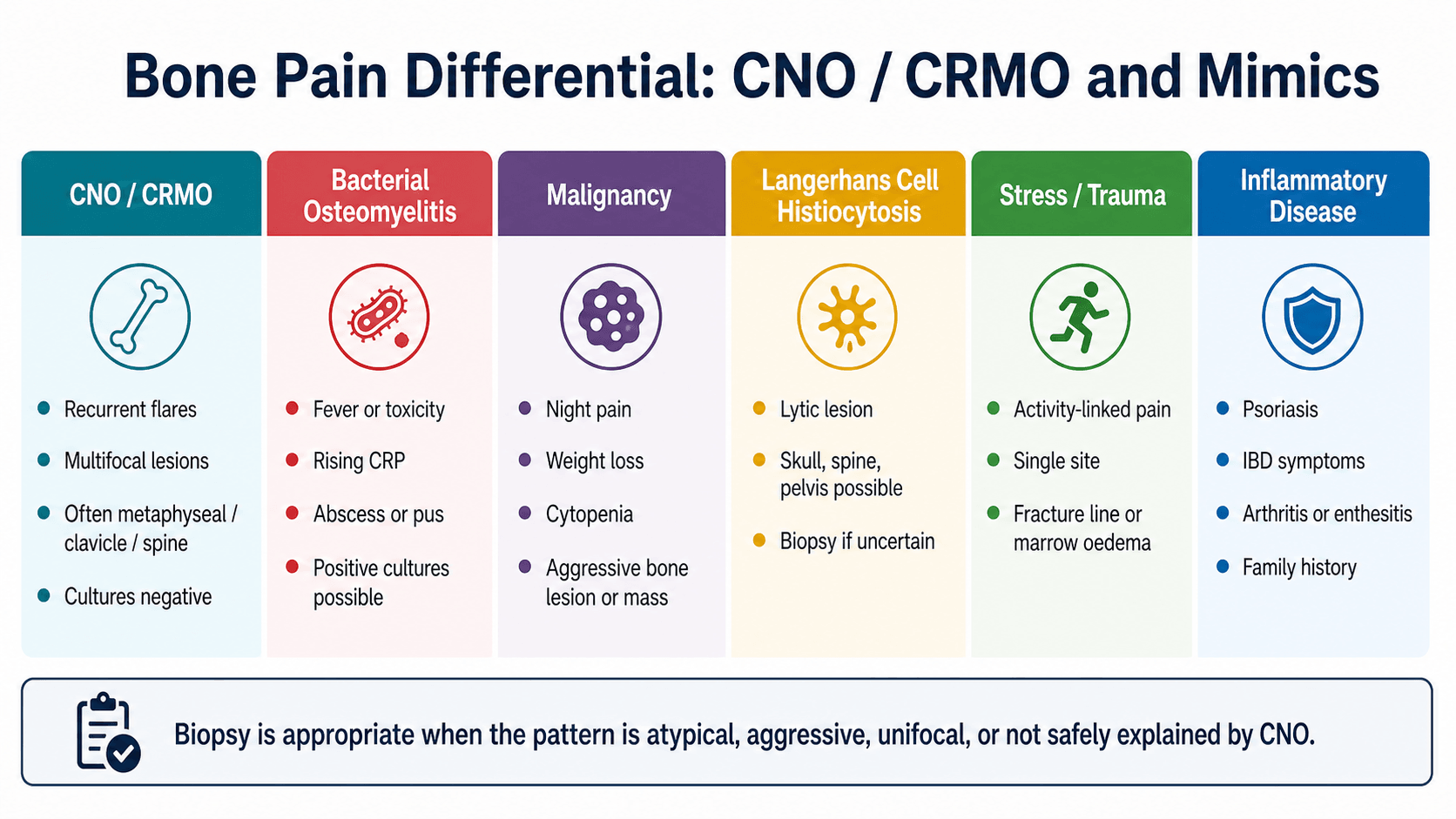
Key Mimics
| Diagnosis | Clues against uncomplicated CNO | Action |
|---|---|---|
| Bacterial osteomyelitis | Fever, toxicity, abscess, positive cultures, rising CRP or clear portal of infection. | Culture and treat infection; drain pus when present. |
| Ewing sarcoma or osteosarcoma | Aggressive lesion, soft-tissue mass, constitutional symptoms or progressive destructive pattern. | Urgent tumour-safe imaging and biopsy. |
| Leukaemia | Bone pain with bruising, pallor, infection, cytopenia or systemic illness. | Full blood count and haematology pathway. |
| Langerhans cell histiocytosis | Lytic skull, spine, pelvis or long-bone lesion; vertebra plana can overlap. | Biopsy if the pattern is uncertain. |
| Stress fracture | Single-site load-related pain with training history and fracture line. | Activity modification and fracture management. |
| Juvenile idiopathic arthritis or enthesitis-related arthritis | Dominant synovitis, enthesitis, inflammatory back pain or sacroiliitis pattern. | Rheumatology assessment; CNO may coexist. |
Disease Burden and Risk
CNO is not classified by one universally used orthopaedic fracture-style system. It is more useful to describe disease by burden, risk and certainty of diagnosis.
Burden Description
| Pattern | Meaning | Clinical use |
|---|---|---|
| Unifocal | One apparent lesion. | Higher need for biopsy unless the clinical and imaging pattern is very typical. |
| Multifocal | Several lesions on symptoms or MRI. | Supports CNO when infection and tumour are not otherwise suggested. |
| Recurrent | Flares over time, often at changing sites. | Explains CRMO pattern and need for longitudinal treatment. |
| Silent lesions | MRI lesions without local symptoms. | Whole-body MRI can reveal disease burden missed by examination. |
Management Principles
Management has two parallel aims: keep the diagnosis safe and control inflammation enough to preserve function and prevent structural damage. The child should usually be managed with paediatric rheumatology, paediatrics, radiology and orthopaedics rather than orthopaedics alone.
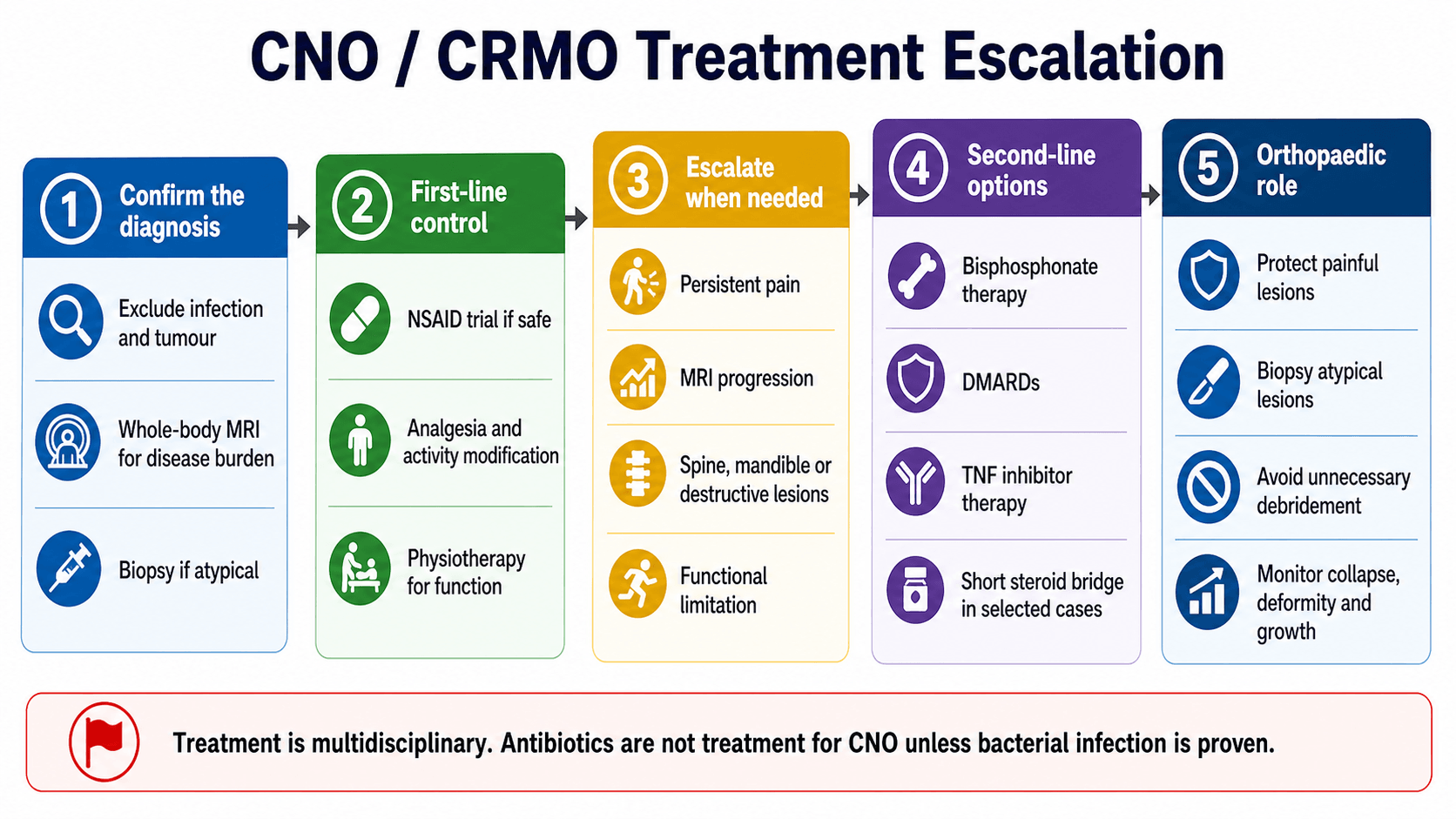
First-line Treatment
NSAIDs are commonly used as first-line anti-inflammatory treatment when safe and appropriate. They are not just analgesics in this setting; they may control inflammatory bone pain in a proportion of children. The child also needs activity modification, physiotherapy for gait and function, school and sport planning, and monitoring for flare recurrence.
First-line treatment is reasonable when the diagnosis is secure, the child is clinically well, there is no high-risk spinal collapse, no aggressive lesion, no fracture risk and symptoms are tolerable.
Biopsy and Operative Details
When biopsy is required, plan it properly. A poorly planned biopsy can contaminate compartments, miss the lesion or create misleading results.
Biopsy Principles
| Step | Practical point | Reason |
|---|---|---|
| Pre-biopsy planning | Review radiographs, MRI and any suspected tumour pathway requirements. | A biopsy tract must be placed where it can be excised if malignancy is diagnosed. |
| Sample target | Target active representative lesion, preferably the most diagnostically useful site. | Necrotic or sclerotic tissue alone may be non-diagnostic. |
| Specimens | Send histology and microbiology, including bacterial cultures; add fungal or mycobacterial tests when clinically indicated. | The aim is to exclude infection and malignancy, not merely prove inflammation. |
| Technique | Use image guidance or open biopsy depending site, safety and diagnostic need. | Accurate sampling matters more than making the smallest incision. |
| Interpretation | Sterile inflammation supports CNO only when clinical and imaging context fits. | Histology alone is not pathognomonic. |
Surgery is not a standard treatment for CNO inflammation. Operative intervention is reserved for diagnostic biopsy, fracture management, deformity correction, treatment of true infection if present, or rare structural complications. Repeated washouts without pus or culture-positive infection usually represent a management error.
Complications and Follow-up
Follow-up should track symptoms, function, inflammatory markers when useful, medication response, adverse effects and imaging activity. Whole-body MRI is used for disease burden and monitoring, but imaging should be interpreted with the clinical picture; persistent signal change does not always mean the child needs the same escalation if symptoms and structure are stable.
Complications
| Complication | Mechanism | Follow-up focus |
|---|---|---|
| Chronic pain and disability | Persistent inflammatory bone pain and deconditioning. | Pain control, physiotherapy, school participation and mental health impact. |
| Vertebral collapse | Active spinal osteitis weakens vertebral body. | Sagittal spinal MRI review, deformity monitoring and early escalation. |
| Pathological fracture | Destructive lesion or weakened bone. | Activity restriction, protection and fracture management. |
| Growth disturbance or deformity | Periphyseal inflammation and structural damage. | Limb length, alignment and joint function surveillance. |
| Unnecessary operations | Misdiagnosis as recurrent bacterial osteomyelitis. | Reassess diagnosis when cultures are negative and disease is multifocal. |
| Delayed tumour diagnosis | Overconfidence in CNO label. | Biopsy atypical, aggressive or unifocal disease. |
Evidence Summary
Largest CRMO Cohort and Prognostic Phenotypes
- National French cohort of 178 paediatric CRMO patients, mean age at diagnosis 10.9 years, with female predominance (123 of 178).
- Only 12 of 178 (7 percent) remained unifocal at last visit, confirming the multifocal nature of established disease.
- Remission was reached in only 73 of 171 (43 percent) after a mean of 47.9 months, and 44 of 171 (26 percent) had sequelae; cluster analysis defined severe, intermediate and mild phenotypes.
Contemporary Cohort: Presentation and Spinal Prognosis
- In 30 children, bone pain was the leading symptom (29 of 30) and lesions clustered at metaphyses and epiphyses adjacent to growth plates.
- NSAID monotherapy achieved remission in nearly half (14 of 30); the remainder needed bisphosphonates, DMARDs or biologics.
- Patients with spinal involvement had a worse prognosis and more long-term sequelae.
Registry Link Between CNO and Inflammatory Bowel Disease
- Among 8244 children with IBD versus 82,400 non-IBD comparators, CNO risk was almost 6-fold higher (adjusted hazard ratio 5.87, 95 percent CI 2.95 to 11.66).
- Children with IBD plus CNO had younger age at IBD onset and far more extraintestinal manifestations (62 versus 21 percent).
- Biologic use was higher in the IBD plus CNO group (78 versus 44 percent).
Clinical Pitfalls
Common Errors
| Pitfall | Why it is wrong | Safer approach |
|---|---|---|
| Calling every recurrent bone pain CRMO | Stress fracture, tumour, infection and LCH can mimic it. | Use imaging pattern, labs and biopsy when atypical. |
| Repeating antibiotics without proof | CNO is sterile and antibiotics do not control autoinflammation. | Reassess diagnosis and disease burden. |
| Ignoring spine | Spinal disease can cause collapse and deformity. | Whole-body MRI should include adequate spinal assessment. |
| Using biopsy as treatment | Debridement does not treat sterile inflammatory osteitis. | Biopsy only for diagnosis or when another surgical indication exists. |
| Missing inflammatory associations | Skin, gut and joint disease can coexist and change treatment. | Screen for psoriasis, pustulosis, IBD symptoms, arthritis and enthesitis. |
Clinical Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Recurrent Tibial Pain
"A 10-year-old has recurrent proximal tibial pain over several months. X-ray shows a mixed metaphyseal lesion. The child is well, CRP is mildly raised, and symptoms improved temporarily with NSAIDs. How do you approach this?"
Spinal Lesion in CNO
"A child with known multifocal CNO develops thoracic back pain. Whole-body MRI shows vertebral body oedema and early height loss. What changes in management?"
Unifocal Clavicular Lesion Referred as Possible Tumour
"A 9-year-old is referred to the tumour clinic with a painful, swollen medial clavicle and a single sclerotic, expansile lesion on plain film. Inflammatory markers are mildly elevated and the child is systemically well. The referring team has already started oral antibiotics. How do you proceed?"
Guidelines, Registries and Global Practice
CNO and CRMO are recognised worldwide but remain rare, under-coded and without internationally validated diagnostic criteria, so epidemiology and practice vary by region and resource setting.
Global Epidemiology
Epidemiology Summary
| Measure | Typical finding | Source context |
|---|---|---|
| Peak onset | School-age and early adolescence; mean age at diagnosis around 10 to 11 years. | French national cohort (mean 10.9 years) and Belgian cohort (mean onset 10.3 years). |
| Sex distribution | Modest female predominance in most cohorts. | French cohort 123 of 178 female; Belgian and Saudi cohorts also female-predominant. |
| Distribution | Multifocal in the large majority once established; lower limbs, spine, clavicle and pelvis common. | Only 7 percent stayed unifocal at last visit in the French cohort. |
| Outcome | Remission in roughly 40 to 50 percent on NSAIDs alone; sequelae in about a quarter. | French cohort sequelae 26 percent; spinal disease worsens prognosis. |
| Associations | Overlap with IBD, psoriasis, palmoplantar pustulosis, acne and arthritis (SAPHO in adults). | Swedish registry: nearly 6-fold higher CNO risk in childhood-onset IBD. |
Society Guidance Side by Side
There is no single global guideline; the most structured guidance comes from paediatric rheumatology consensus groups rather than orthopaedic societies.
Comparative Guidance
| Body | Diagnostic emphasis | Treatment emphasis |
|---|---|---|
| CARRA (North America) consensus treatment plans | Diagnosis of exclusion; baseline imaging and labs before escalation. | Three plans for NSAID-refractory or spinal disease: methotrexate/sulfasalazine, TNF inhibitor with optional methotrexate, or bisphosphonates. |
| GKJR (German paediatric rheumatology) recommendations | Whole-body MRI for skeletal mapping; CNO remains a diagnosis of exclusion. | First-line NSAIDs and short steroids; second-line DMARDs, biologics and bisphosphonates; rapid bisphosphonate and/or TNF inhibitor for vertebral disease. |
| European paediatric rheumatology and radiology reviews | STIR whole-body MRI including dedicated sagittal spine imaging. | Escalation driven by site, structural threat and treatment response, not pain alone. |
| Orthopaedic / oncology contribution (AO, tumour-service principles) | Tumour-safe biopsy planning for unifocal or aggressive lesions. | Structural protection, deformity surveillance and avoidance of unnecessary debridement. |
No orthopaedic registry tracks CNO directly
Unlike arthroplasty, there is no implant registry for CNO. The best registry-level evidence is epidemiological and association data from national health registers, such as the Swedish IBD-CNO linkage. Quote cohorts and consensus plans, not implant survival figures.
High- versus Limited-resource Practice
Practice Variation by Setting
| Setting | Reality | Consequence |
|---|---|---|
| Well-resourced centres | Ready access to whole-body MRI and paediatric rheumatology. | Earlier mapping, fewer biopsies in typical disease, structured escalation to biologics and bisphosphonates. |
| Limited-resource settings | Whole-body MRI and biologics may be scarce; reliance on radiographs and regional MRI. | Higher biopsy and empirical antibiotic use; risk of repeated infection-directed treatment and delayed diagnosis. |
| Any setting | CNO is rare and easily mislabelled as infection or tumour. | Pattern recognition and exclusion of mimics remain the universal safety principle. |
Controversies and Areas of Uncertainty
Unresolved Questions
| Issue | Why it is uncertain | Practical stance |
|---|---|---|
| Diagnostic criteria | No prospectively validated international criteria or biomarker exists; several clinical scores compete. | Use the whole clinical, laboratory, imaging and (when needed) histological pattern, not a single rule. |
| When biopsy is mandatory | Typical multifocal disease may avoid biopsy, but thresholds differ between centres. | Biopsy unifocal, aggressive or atypical lesions and any case where infection or tumour stays plausible. |
| Best second-line agent | No head-to-head trials establish a single best drug after NSAID failure. | Choose bisphosphonate, DMARD or TNF inhibitor by site, severity and specialist practice. |
| Treating MRI activity in a well child | Silent residual signal may persist without symptoms. | Do not escalate on imaging alone when pain, function and structure are stable. |
| Monitoring intensity and duration | Optimal whole-body MRI frequency and stop-treatment timing are not standardised. | Individualise follow-up, with closer surveillance for spinal and destructive disease. |
Summary
CNO is sterile inflammatory osteitis, and CRMO is its recurrent multifocal form. The safe approach is to recognise the pattern, exclude infection and malignancy, map disease with whole-body MRI, biopsy atypical or unifocal lesions, and treat according to pain, function, disease burden and high-risk sites. Orthopaedics contributes most by making the diagnosis safe, protecting structure, monitoring deformity and avoiding unnecessary infection surgery when cultures and imaging support sterile inflammatory disease.
CNO and CRMO Quick Review
Clinical summary
Definition
- •CNO is sterile autoinflammatory osteitis.
- •CRMO is the recurrent multifocal end of the CNO spectrum.
- •The diagnosis requires exclusion of infection, malignancy and important mimics.
Presentation
- •Recurrent focal bone pain, limp, swelling or back pain.
- •Fever is absent or low-grade in many cases; toxicity is a red flag.
- •Ask about psoriasis, pustulosis, inflammatory bowel symptoms, arthritis and enthesitis.
Imaging
- •X-ray may be normal early or show lytic, sclerotic or mixed change.
- •MRI is the key test for active osteitis and structural risk.
- •Whole-body MRI maps multifocal and silent lesions, especially spine.
Biopsy Triggers
- •Unifocal, aggressive or atypical lesion.
- •Soft-tissue mass, cytopenia, persistent fever or toxic child.
- •Any case where infection or malignancy remains plausible.
Treatment
- •NSAIDs are commonly first-line when diagnosis is secure and risk is low.
- •Escalate for persistent pain, MRI progression, spine, mandible or destructive lesions.
- •Second-line options include bisphosphonates, DMARDs and TNF inhibitor therapy under specialist care.
Orthopaedic Role
- •Recognise the pattern and arrange safe biopsy when needed.
- •Protect painful or structurally weak lesions.
- •Monitor spine, growth, alignment and deformity.
- •Avoid repeated debridement when there is no pus or bacterial infection proof.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.