Congenital unilateral absence of the sternocostal pectoralis major with a variably affected ipsilateral hand
- Poland syndrome is congenital absence of the sternocostal (lower) head of pectoralis major, almost always unilateral, with a variably affected ipsilateral hand.
- The most accepted cause is the subclavian artery supply disruption sequence around the sixth to eighth week of gestation, which explains why the chest and hand on the same side are affected together.
- It is usually sporadic; most children have normal life expectancy and the main issues are appearance, chest wall stability and hand function.
- Hand involvement ranges from a normal hand to symbrachydactyly with short, webbed or absent digits; the hand, not the chest, usually drives early management.
- Assess the whole spectrum: pectoralis major and minor, ribs and costal cartilages, breast and nipple, latissimus dorsi and the hand.
- Chest reconstruction is mainly for cosmesis and chest wall stability, often using the latissimus dorsi flap, custom implants or autologous tissue; the hand is treated on its own functional merits.
- “The safe opening line is: unilateral absence of the sternocostal pectoralis major plus an ipsilateral hand difference, on the same side, from a vascular disruption sequence.
- “Most cases are right-sided and male, but never quote that as a rule that excludes left-sided or female cases.
- “Do not promise a normal chest or a normal hand; the aim is improved contour, stability and function.
- “If the latissimus dorsi is also absent, your chest wall reconstruction plan must change because you cannot rely on that flap.
Poland Syndrome
Confirm what is actually missing before planning surgery. Where ribs or costal cartilages are deficient there may be paradoxical chest wall movement or a lung hernia, and the latissimus dorsi may also be absent. Operating on assumptions about the anatomy is unsafe.
- Lower Concern
- Ribs and costal cartilages intact
- Higher Concern
- Rib or costal cartilage hypoplasia or aplasia
- Practical Effect
- Skeletal deficiency raises the need for stabilisation and lung protection.
- Lower Concern
- Normal or mild hand difference
- Higher Concern
- Symbrachydactyly with functional limitation
- Practical Effect
- Significant hand involvement is usually treated first and on its own merit.
- Lower Concern
- Present and usable
- Higher Concern
- Absent or hypoplastic on the same side
- Practical Effect
- Loss of the usual donor flap forces an alternative reconstruction plan.
- Lower Concern
- Symmetric or minor difference
- Higher Concern
- Marked breast or nipple hypoplasia or amastia
- Practical Effect
- Drives timing and choice of breast reconstruction, usually after puberty.
- Lower Concern
- Mainly cosmetic concern
- Higher Concern
- Function, breathing or major psychosocial impact
- Practical Effect
- Sets the urgency, sequence and type of reconstruction.
POLANDFeatures | CHESTReconstruction Aim | TRAPSPitfalls |
|---|---|---|
P Pectoralis Absent sternocostal head of pectoralis major (and often pectoralis minor). | C Contour Restore the anterior chest and axillary fold shape. | T Thinking it is isolated Always check the hand, ribs, breast and latissimus dorsi. |
O One side Almost always unilateral, classically right-sided. | H Harvest wisely Use latissimus dorsi only if it is present and healthy. | R Relying on latissimus It may also be absent on the affected side. |
L Limb (hand) Ipsilateral hand difference, often symbrachydactyly. | E Even out breast Add implant or autologous tissue for breast symmetry after puberty. | A Assuming a side or sex Right and male are common, not universal. |
A Artery Subclavian artery supply disruption sequence is the leading theory. | S Stabilise skeleton Reconstruct deficient ribs and protect the lung. | P Promising normality Aim for improvement, not a perfectly normal chest or hand. |
N Nipple and breast Hypoplasia or absence of the breast and nipple-areolar complex. | T Timing Treat the hand early; stage chest and breast work to growth and maturity. | S Skipping lung protection Deficient ribs can mean paradoxical movement or lung hernia. |
D Deficient ribs Costal cartilage or rib hypoplasia in more severe cases. | ||
Spell out what is missing and what is affected. | Rebuild a stable, symmetric chest. | Do not be caught out by missing anatomy. |
Overview and Epidemiology
Poland syndrome is a rare congenital condition defined by unilateral absence of the sternocostal (lower) head of the pectoralis major muscle, usually combined with a variably affected hand on the same side. It is also called Poland anomaly because the findings are a developmental field defect rather than a true genetic syndrome.
The condition is uncommon and almost always sporadic. Reported incidence varies widely, from roughly 1 in 7,000 to 1 in 100,000 live births, with a commonly quoted figure of about 1 in 30,000 newborns. It is described more often on the right side and more often in males, but left-sided and female cases occur and must not be excluded by these tendencies.
The clinical picture is extremely variable. At the mild end, a person has only a missing portion of pectoralis major and may not be diagnosed until adolescence or adulthood, sometimes incidentally. At the severe end, there is rib and costal cartilage deficiency, breast and nipple hypoplasia, and a markedly affected hand. The condition matters for appearance, chest wall stability and, most importantly for the orthopaedic and hand surgeon, hand function.
Congenital unilateral absence of the sternocostal head of pectoralis major with a variably affected ipsilateral hand.
A same-side chest wall and hand field defect, attributed to disrupted subclavian artery blood supply in early development.
Pathophysiology and Anatomy
The most widely accepted explanation is the subclavian artery supply disruption sequence. Around the sixth to eighth week of gestation, a temporary reduction in blood flow through the developing subclavian artery and its branches is thought to impair growth of the structures supplied on that side. Because the subclavian artery and its branches supply both the anterior chest wall and the developing upper limb, a single vascular insult can explain why the chest and the hand on the same side are affected together. This theory is supported by case reports showing similar disruption patterns in other vascular territories.
The defining anatomical feature is absence of the sternocostal head of pectoralis major. The clavicular head is usually preserved, which is why some shoulder function is retained. The spectrum of structures that may be involved includes:
- Pectoralis major: absence of the sternocostal head, sometimes with the whole muscle absent.
- Pectoralis minor: frequently absent or hypoplastic.
- Ribs and costal cartilages: hypoplasia or aplasia, classically of the second to fourth or third to fifth segments.
- Breast and nipple: hypoplasia or complete absence (amastia and athelia).
- Subcutaneous tissue and skin: thinning over the affected chest.
- Other muscles: latissimus dorsi, serratus anterior and other shoulder-girdle muscles can be hypoplastic or absent.
- Hand: symbrachydactyly with short, webbed or absent middle phalanges and digits.
The functional consequences depend on what is missing. Absence of pectoralis major alone causes mainly cosmetic asymmetry with surprisingly preserved strength. Rib deficiency can cause paradoxical chest wall motion or a lung hernia. Hand involvement determines grasp, pinch and overall upper-limb function.
Associated Anomalies and Malignancy Risk
Because the underlying mechanism is a vascular disruption sequence, Poland syndrome belongs to a family of conditions attributed to early vascular insults, and it carries a small number of recognised associations that examiners like to probe.
- Note
- Classically described with LEFT-sided Poland syndrome - examine/image the heart, especially in left-sided cases
- Note
- Congenital facial (VII) and abducens (VI) palsy, often with bilateral symbrachydactyly - the Poland-Mobius overlap, part of the same vascular-disruption spectrum
- Note
- Congenital undescended/high scapula - a recognised skeletal association
- Note
- Congenital cervical vertebral fusion - reported in the same disruption spectrum
- Note
- Terminal transverse limb defects and diaphragmatic eventration have been reported with the same subclavian-disruption mechanism
The single most quotable association is dextrocardia with left-sided Poland syndrome. When the left chest is affected, actively look for and image the heart (and great vessels), because the same vascular-disruption mechanism can involve cardiac position/anatomy. This is also why an atypical or extensive case warrants vascular/echocardiographic assessment (as in the investigation table).
Poland syndrome carries reported (rare) associations with malignancy that are worth knowing: childhood leukaemia and non-Hodgkin lymphoma, and breast carcinoma arising in the hypoplastic breast (and the carcinoma can be harder to detect against an abnormal, asymmetric breast). The practical message is awareness and individualised, age-appropriate breast screening/self-examination, not routine intensive surveillance - the absolute risk remains low and the associations come from case reports and small series.
Classification
Classification describes severity and helps plan reconstruction, but it does not replace an individual functional assessment. Chest wall classifications describe the skeletal and soft-tissue deficit, while hand classifications describe the digital deficiency.
- What Is Present
- Absent sternocostal pectoralis major; ribs intact
- Reconstructive Implication
- Soft-tissue or flap reconstruction for contour; no skeletal repair needed.
- What Is Present
- Pectoral aplasia with breast and nipple hypoplasia
- Reconstructive Implication
- Add breast reconstruction (implant or autologous) after puberty.
- What Is Present
- Rib or costal cartilage hypoplasia or aplasia, possible lung hernia
- Reconstructive Implication
- Skeletal stabilisation and lung protection in addition to soft-tissue cover.
Several named classifications exist (for example the Foucras radiological grouping), but they are descriptive tools. Examiners are more interested in whether you can categorise a patient as muscle-only, muscle-plus-breast or skeletal-deficiency and act accordingly.

Clinical Presentation
Presentation depends on severity and age. A newborn may be noted to have an asymmetric chest, an absent anterior axillary fold or an abnormal hand. An older child or adult may present for cosmetic reasons, with breast asymmetry at puberty, or even incidentally on imaging done for another reason. Adults occasionally present when the chest wall defect is mistaken for trauma or another pathology.
History should define:
- when the difference was first noticed and whether it has changed with growth;
- which structures are involved: chest contour, breast, nipple and the hand;
- hand function: grasp, pinch, dressing, writing, sport and any aids used;
- breathing symptoms or a visible bulge that changes with coughing or straining;
- the patient's and family's main concern: appearance, function or psychosocial impact;
- family history (usually negative, since most cases are sporadic).
Examination should be deliberate:
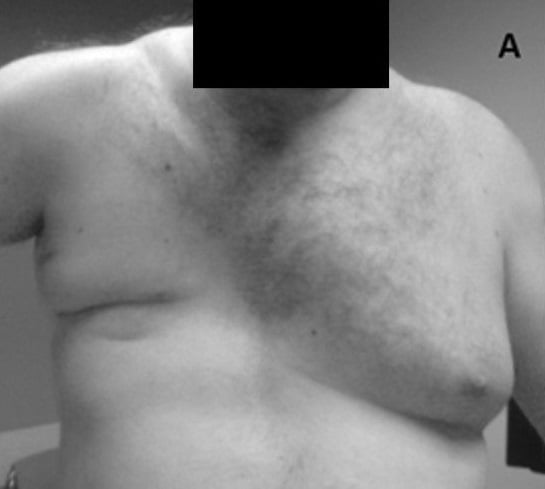
- Inspect both sides of the chest with the patient relaxed and then with the hands pushed onto the hips to contract pectoralis major. The absent sternocostal head and lost anterior axillary fold become obvious.
- Palpate for the pectoral muscle mass, the costal cartilages and any rib step-off or soft, pulsatile defect.
- Look for paradoxical chest wall movement or a bulge on coughing that suggests a lung hernia.
- Assess the breast and nipple-areolar complex, especially in females after puberty.
- Examine the same-side latissimus dorsi by resisted shoulder extension or adduction, because it may also be deficient.
- Examine the hand in detail: number, length and webbing of digits, nail size, grasp, pinch and overall function.
- Assess shoulder and upper-limb strength; clavicular head preservation often keeps function reasonable.
- Note any other anomalies, since rare associations are reported.
Asking the patient to press their hands firmly onto their hips contracts pectoralis major and unmasks an absent sternocostal head and a missing anterior axillary fold. This simple manoeuvre is the quickest bedside confirmation.

Investigations and Imaging
Investigations should answer four questions:
- Which muscles are absent or hypoplastic, and is the latissimus dorsi usable?
- Is the rib and costal cartilage skeleton deficient, and is there a lung hernia?
- What is the breast and soft-tissue deficit?
- What is the precise hand anatomy if reconstruction is planned?
- What It Shows
- Muscle absence, contour, hand function, latissimus dorsi status
- When It Helps
- Always; it is the foundation of assessment.
- What It Shows
- Rib anomalies, hyperlucent lung from absent soft tissue, gross asymmetry
- When It Helps
- Baseline skeletal screen and to flag rib deficiency.
- What It Shows
- Phalangeal length, missing or fused bones, carpal anatomy
- When It Helps
- When the hand is involved and surgery is considered.
- What It Shows
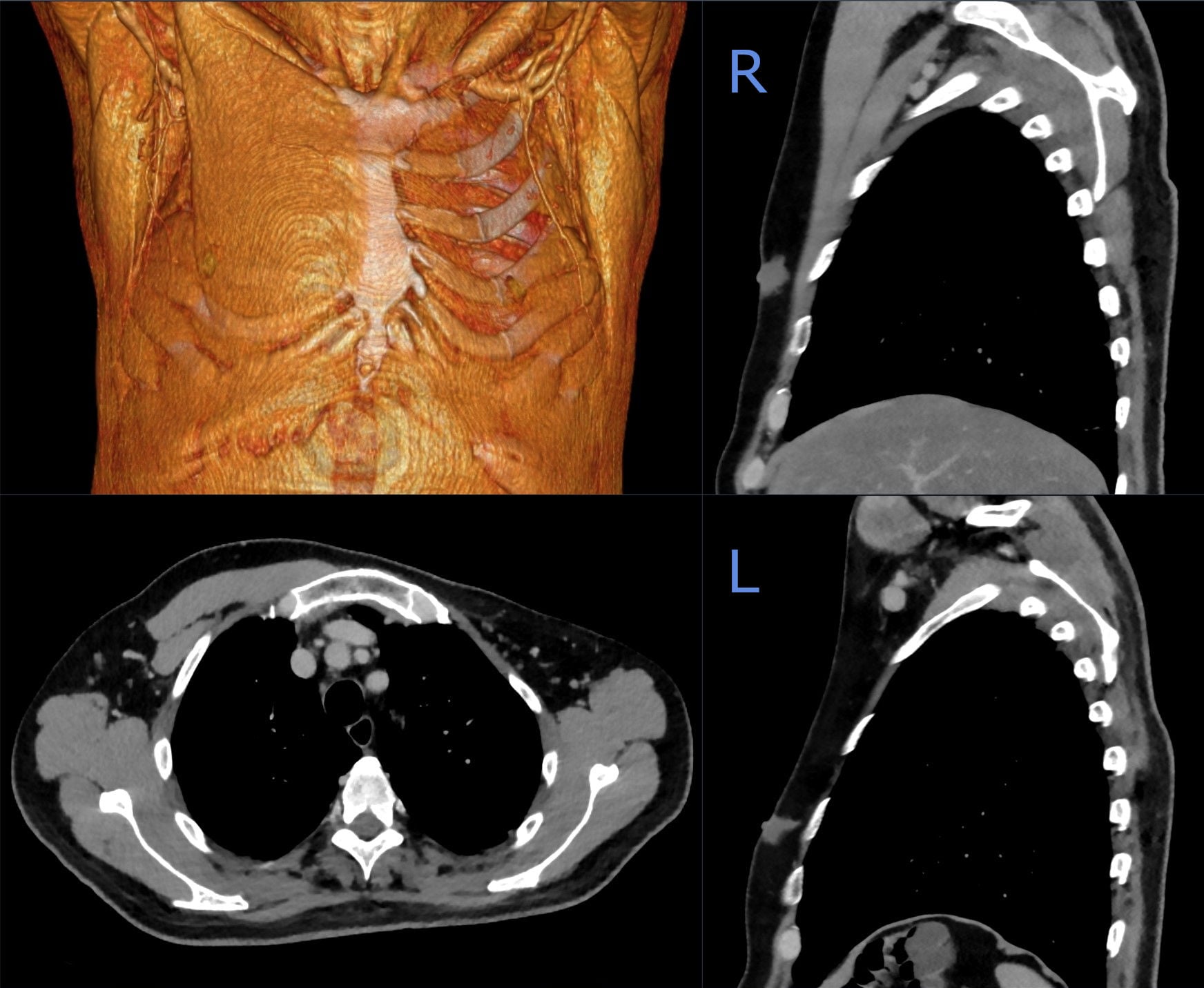
- Detailed muscle, rib and costal cartilage anatomy and chest wall volume
- When It Helps
- Preoperative planning of chest wall and skeletal reconstruction.
- What It Shows
- Soft-tissue muscle map, breast tissue and donor muscle quality
- When It Helps
- Mapping muscle deficits and planning flap reconstruction.
- What It Shows
- Subclavian and great-vessel anatomy, cardiac status
- When It Helps
- Atypical or extensive cases and before major reconstruction.
Imaging is most valuable when it changes the plan: confirming whether the latissimus dorsi can be used, mapping the rib and cartilage deficit, and defining the hand skeleton before reconstruction. Do not order advanced imaging simply to label the condition when the diagnosis is clinical.
Differential Diagnosis
Not every absent pectoral muscle or chest asymmetry is Poland syndrome, and the hand difference can be confused with other congenital limb conditions. The distinction matters because management and associated risks differ.
- Distinguishing Features
- Unilateral absent sternocostal pectoralis major with an ipsilateral hand difference, classically right-sided
- Key Discriminator
- Same-side chest and hand field defect from vascular disruption.
- Distinguishing Features
- Absent pectoral muscle with a completely normal hand and no other field defect
- Key Discriminator
- No ipsilateral hand or skeletal involvement.
- Distinguishing Features
- Symmetric or central sternal depression or protrusion, normal pectoral muscles and hand
- Key Discriminator
- Sternal shape abnormality rather than muscle absence.
- Distinguishing Features
- Facial diplegia and abducens palsy with symbrachydactyly, often bilateral
- Key Discriminator
- Cranial nerve palsies and bilateral hand involvement.
- Distinguishing Features
- Short-finger hand difference with a normal chest wall and pectoral muscles
- Key Discriminator
- Hand difference without any chest wall component.
- Distinguishing Features
- Acquired defect with a relevant history, scars or prior surgery
- Key Discriminator
- History of trauma or operation rather than a congenital pattern.
Breathing difficulty, paradoxical chest wall movement, a soft pulsatile bulge that enlarges on coughing, or a rapidly changing chest mass should prompt urgent assessment for lung hernia or another pathology rather than routine cosmetic referral.
Management Decision-Making
Management is shaped by severity, age, function and the patient's priorities. The aim is not to make the chest and hand perfectly normal; it is to improve contour, restore chest wall stability where the skeleton is deficient, and maximise hand function. A multidisciplinary team of paediatric, plastic, thoracic and hand surgeons, with psychology and developmental support, gives the best results.
Two principles guide sequencing. First, the hand is usually addressed early because grasp and pinch develop in childhood and influence the whole upper limb. Second, chest and breast reconstruction are usually staged to growth and puberty, since adding an implant or shaping the breast before maturity risks asymmetry as the child grows.
Conservative management is appropriate when the deformity is mild, function is good, the skeleton is stable and the patient does not want surgery.
It includes:
- explanation that the condition is congenital, usually sporadic and not progressive;
- reassurance that absence of pectoralis major alone often leaves good strength;
- monitoring of chest contour and breast development through growth;
- occupational therapy and adaptive strategies for any hand limitation;
- psychological support for body image and confidence;
- discussion of reconstructive options for later, if and when the patient wants them.
Conservative care does not regrow the muscle or correct the skeleton; its role is to support function and let the patient choose reconstruction at the right time.
Operative Principles
The operative plan must be explicit before the incision: which deficit is being corrected, whether the latissimus dorsi is available, whether the skeleton needs stabilisation, and the timing relative to growth and puberty.
Purpose: restore the anterior chest contour and, where needed, a stable skeleton.
Stepwise principles:
- Confirm anatomy: review imaging for muscle, rib and cartilage deficit and latissimus dorsi availability.
- Plan the donor: if the latissimus dorsi is present, plan a pedicled flap; if absent, plan an implant or an autologous free flap.
- Address the skeleton first: reconstruct deficient ribs or cartilages with graft, struts or mesh and protect the lung where there is a hernia.
- Recreate soft-tissue contour: transfer the latissimus dorsi or place a custom implant to rebuild the anterior chest and axillary fold.
- Restore symmetry: balance with the opposite side, planning breast work separately in females.
- Close carefully: meticulous haemostasis, drains as needed and a tension-free, well-contoured closure.
Endoscopic or minimal-access latissimus dorsi harvest through a hidden axillary incision is described and can reduce scarring while still recontouring the chest, particularly in males.
Complications
Complications relate to the deformity itself, to reconstruction and to expectations.
- Mechanism
- Deficient ribs and costal cartilages
- Prevention or Response
- Skeletal stabilisation and lung protection during reconstruction.
- Mechanism
- Compromised pedicle or absent or marginal latissimus dorsi
- Prevention or Response
- Confirm donor anatomy, careful dissection and consider alternative flaps.
- Mechanism
- Custom or breast implant malposition, capsular contracture or extrusion
- Prevention or Response
- Adequate soft-tissue cover, correct sizing and staged revision if needed.
- Mechanism
- Growth, severe deficit or incomplete correction
- Prevention or Response
- Stage to maturity, set realistic goals and plan revision surgery.
- Mechanism
- Severe digital deficiency with limited reconstructable tissue
- Prevention or Response
- Realistic counselling, prioritise grasp and pinch, consider prosthetics.
- Mechanism
- Visible difference affecting body image and confidence
- Prevention or Response
- Early psychological support and patient-centred decision-making.
- Mechanism
- Narrow assessment ignoring ribs, breast or latissimus dorsi
- Prevention or Response
- Structured assessment of all potentially involved structures.
Clinical Relevance and Case Approach
When shown a patient with an absent pectoral muscle or chest asymmetry, structure the answer in this order:
- Diagnosis: unilateral absence of the sternocostal pectoralis major with an ipsilateral hand difference, consistent with Poland syndrome.
- Cause: mention the subclavian artery supply disruption sequence as the leading theory and that it is usually sporadic.
- Define the deficit: pectoralis major and minor, ribs and cartilages, breast and nipple, latissimus dorsi and the hand.
- Assess function: chest wall stability and breathing, plus detailed hand grasp and pinch.
- Imaging: clinical diagnosis confirmed; CT or MRI with 3D reconstruction and hand radiographs when reconstruction is planned.
- Plan: treat the hand early for function; stage chest and breast reconstruction to growth and puberty.
- Counsel: aim for improved contour, stability and function rather than a perfectly normal chest or hand, with multidisciplinary and psychological support.
Guidelines, Registries and Global Practice
There is no high-level society guideline or implant registry specific to Poland syndrome; it is a rare, non-arthroplasty congenital condition, so practice is guided by paediatric, plastic and hand surgical principles, narrative reviews and surgical series rather than registry data. The points below frame a globally consistent approach.
Global epidemiology
- Poland syndrome is rare, with reported incidence ranging from about 1 in 7,000 to 1 in 100,000 and a commonly quoted figure near 1 in 30,000 newborns.
- It is usually sporadic and unilateral, described more often on the right side and in males, although left-sided and female cases occur and should not be excluded by these tendencies.
- The hand difference sits within the symbrachydactyly spectrum and is the feature most relevant to early function.
Side-by-side principles across practice settings
- Emphasis
- Treat the hand early; stage the chest wall
- Practical Position
- Correct functional hand problems first; reconstruct the chest later for cosmetic or functional reasons.
- Emphasis
- Restore contour and symmetry
- Practical Position
- Latissimus dorsi flap, custom implant or autologous perforator flap depending on the deficit and donor availability.
- Emphasis
- Skeletal stability and lung protection
- Practical Position
- Reconstruct deficient ribs or cartilages and address lung hernia where the skeleton is deficient.
- Emphasis
- Categorise the hand difference precisely
- Practical Position
- Place symbrachydactyly within a malformation framework to guide hand reconstruction.
Registry note
- Arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not capture Poland syndrome because no joint implant is used. Outcome evidence comes from single-centre and multicentre surgical cohorts and case series, which is why reporting is heterogeneous and complication rates, although generally low, are imprecise.
High- versus limited-resource practice variation
- In well-resourced settings, CT and MRI with 3D reconstruction, custom implants, microsurgical free flaps and toe-to-hand transfer expand the reconstructive options.
- In limited-resource settings, clinical assessment and plain radiographs drive decisions, and reconstruction may rely on pedicled latissimus dorsi flaps or simpler implants. The core principle, treat the hand for function and stage the chest for contour and stability, is universal.
Controversies and Areas of Uncertainty
Most Poland syndrome evidence is observational, so several practical questions remain genuinely unsettled. Examiners reward a candidate who can name the uncertainty rather than overstate the data.
- Cause. The subclavian artery supply disruption sequence is the leading theory and is supported by case reports, but it is not proven for every case and some atypical phenotypes are hard to explain by a single vascular event.
- Timing of chest reconstruction. There is no agreed age; many surgeons stage definitive work to puberty and skeletal maturity, but the evidence is observational and confounded by severity.
- Best reconstructive technique. Latissimus dorsi flap, custom implant and autologous perforator flaps all report good outcomes; comparative data are weak and choice depends on the deficit, donor availability and surgeon experience.
- Management of the latissimus-absent chest. When the usual donor is also missing, the optimal alternative (implant versus distant autologous flap) is not settled.
- Hand reconstruction thresholds. When to lengthen, transfer toes or use prosthetics in severe hands depends on function and family goals rather than a fixed algorithm.
- Cancer awareness. Rare reports link the hypoplastic breast and the condition with malignancy; the practical message is awareness and individualised screening, not routine intensive surveillance.
Clinical Reasoning Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old is referred with a flat chest on one side and a smaller hand on the same side. How do you assess this patient?”
“The parents ask why both the chest and the hand on the same side are affected. How do you explain the cause?”
“A young woman with Poland syndrome wants chest reconstruction. Imaging shows rib hypoplasia and an absent latissimus dorsi on the affected side. How do you plan treatment?”
“A newborn has severe Poland syndrome with absent ribs and a soft bulge over the chest that enlarges on crying. What is your priority?”
Definition
- Congenital absence of the sternocostal pectoralis major.
- Almost always unilateral, classically right-sided.
- Variably affected ipsilateral hand (symbrachydactyly).
Cause
- Subclavian artery supply disruption sequence at six to eight weeks.
- Shared blood supply links the chest and hand on the same side.
- Usually sporadic with low recurrence risk.
Assess
- Pectoralis major and minor and the latissimus dorsi.
- Ribs, costal cartilages, breast and nipple.
- Hand digits, grasp and pinch.
Treatment
- Treat the hand early for function.
- Stage chest and breast reconstruction to growth and puberty.
- Latissimus dorsi flap, custom implant or autologous free flap; stabilise deficient ribs.
Complications
- Lung hernia or paradoxical chest movement.
- Flap or implant problems and persistent asymmetry.
- Psychosocial impact and limited hand reconstruction.
Evidence Base
Poland's syndrome revisited
- Poland syndrome is a rare congenital anomaly of unilateral chest wall hypoplasia with ipsilateral hand abnormalities, and is largely sporadic.
- The prevailing aetiological theory is hypoplasia of the subclavian artery or its branches, producing a range of developmental changes.
- Reported incidence ranges from about 1 in 7,000 to 1 in 100,000 live births and varies by sex and familial versus congenital status.
- In a series of 27 patients, repair was suggested in two stages in children and a single stage in adults, using bone grafts or prosthetic mesh for ribs and muscle flaps with implants for soft-tissue and breast deficits.
Poland syndrome: a thoracic surgical overview
- Poland syndrome features hypoplasia or absence of the breast or nipple, absent costosternal pectoralis major, absent pectoralis minor and absence of costal cartilages or ribs in the second to fourth or third to fifth segments.
- The chest wall defect is often associated with a lung hernia.
- Clinical features are extremely variable and rarely all present in one individual, and the condition is invariably unilateral, which simplifies reconstruction.
- Single-stage chest wall reconstruction with augmentation and a latissimus dorsi island myocutaneous flap improves on older multi-stage procedures.
Consultations for Poland syndrome: essentials for the surgeon
- Poland syndrome occurs in approximately 1 in 30,000 newborns and manifests with variable symbrachydactyly, costochondral deformities, absent pectoral muscles and breast underdevelopment.
- Phenotypic variability means strict management guidelines are lacking, with decisions often based on specialist experience rather than published evidence.
- Comprehensive imaging with CT and MRI with 3D reconstruction is crucial for assessing the musculoskeletal defect.
- Management is multidisciplinary, involving thoracic, plastic, paediatric and hand surgeons alongside psychologists and growth specialists.