MTP Extension + PIP/DIP Flexion
Lesser Toe Deformity Classification
Critical Must-Knows
- Claw Toe: MTP hyperextension + PIP flexion + DIP flexion - ALL THREE JOINTS involved.
- Hammer Toe: ONLY PIP flexion with neutral MTP and DIP - single joint deformity.
- Intrinsic Weakness: Loss of lumbricals/interossei → extrinsic muscles unopposed.
- Flexibility Test: Passively correct with MTP FLEXED - if corrects, intrinsics still work.
- Neurological Cause: Always consider CMT, diabetes, spinal cord pathology - bilateral distribution.
Clinical Pearls
- "ALL 3 joints affected in claw (vs 1 in hammer/mallet)
- "Flex MTP to test flexibility (relaxes extrinsics)
- "Neurological cause in majority (CMT, diabetes)
- "Girdlestone-Taylor = FDL to EDL transfer
- "Rigid needs PIP/DIP fusion + Weil osteotomy
Clinical Imaging
Imaging Gallery


The Triplanar Deformity
The Differentiator
All 3 Joints: Claw toe involves MTP, PIP, AND DIP. Hammer: PIP only. Mallet: DIP only.
Anatomy of Deformity
MTP: Hyperextended (Dorsiflexed). PIP/DIP: Flexed (Plantarflexed). Mechanism: Extrinsics overpower weak Intrinsics.
Intrinsic Function
Normal: Lumbricals flex MTP, extend IPs. Weakness: Causes "Clawing" (MTP extension, IP flexion).
Testing
Flexibility Test: Flex MTP to relax extrinsics. If toe straightens, it's flexible (Girdlestone-Taylor candidate).
Neurological Cause
Cavus Foot Association
Flexibility Critical
Transfer Metatarsalgia
CAR-HMCToe Deformity Types - CAR-HMC
| C | Claw ALL joints (MTP extension, PIP flexion, DIP flexion) |
| A | All All 3 joints affected |
| R | Roots Neurological roots - CMT, diabetes |
| H | Hammer PIP only (single joint) |
| M | Mallet DIP only (terminal phalanx) |
| C | Crossover Medial deviation (plantar plate tear) |
| C | Claw ALL joints (MTP extension, PIP flexion, DIP flexion) | R | Roots Neurological roots - CMT, diabetes | M | Mallet DIP only (terminal phalanx) |
| A | All All 3 joints affected | H | Hammer PIP only (single joint) | C | Crossover Medial deviation (plantar plate tear) |
Hook:CAR-HMC: Claw affects ALL 3 joints with neurological Roots. Hammer is PIP only, Mallet is DIP only.
LIFEIntrinsic Muscle Function - LIFE
| L | Lumbricals Flex MTP, extend PIP/DIP |
| I | Interossei Flex MTP, extend IP joints, abduct/adduct |
| F | Flex MTP Main action: flex MTP joint |
| E | Extend IP Extend both PIP and DIP joints |
| L | Lumbricals Flex MTP, extend PIP/DIP | F | Flex MTP Main action: flex MTP joint |
| I | Interossei Flex MTP, extend IP joints, abduct/adduct | E | Extend IP Extend both PIP and DIP joints |
Hook:LIFE - Lumbricals and Interossei Flex MTP and Extend IP joints. Loss = claw toe.
FLEX-MTPFlexibility Test - FLEX-MTP
| F | Flex Flex the MTP joint |
| L | Lax Makes extrinsic tendons lax |
| E | Evaluate Evaluate PIP/DIP correction |
| X | Extrinsics Relaxes extrinsic flexors (FDL) |
| M | Manual Manual correction attempted |
| T | Transfer If corrects → FDL Transfer (Girdlestone-Taylor) |
| P | Permanent If fixed → Permanent fusion (arthrodesis) |
| F | Flex Flex the MTP joint | X | Extrinsics Relaxes extrinsic flexors (FDL) | P | Permanent If fixed → Permanent fusion (arthrodesis) |
| L | Lax Makes extrinsic tendons lax | M | Manual Manual correction attempted | ||
| E | Evaluate Evaluate PIP/DIP correction | T | Transfer If corrects → FDL Transfer (Girdlestone-Taylor) |
Hook:FLEX the MTP - if toe corrects, intrinsics work and you can do Transfer. If fixed, need Permanent fusion.
GIFTGirdlestone-Taylor Procedure - GIFT
| G | Girdlestone Girdlestone-Taylor procedure name |
| I | Intrinsic Restores intrinsic function |
| F | FDL to EDL Transfer FDL tendon to EDL |
| T | Tendon Converts flexor to extensor action |
| G | Girdlestone Girdlestone-Taylor procedure name | F | FDL to EDL Transfer FDL tendon to EDL |
| I | Intrinsic Restores intrinsic function | T | Tendon Converts flexor to extensor action |
Hook:GIFT - The Girdlestone procedure is a GIFT to restore Intrinsic function by transferring FDL Tendon to EDL.
Overview and Epidemiology
Claw Toe is a complex triplanar deformity involving hyperextension of the MTP joint with flexion contractures of both the PIP and DIP joints. Unlike hammer toe (PIP flexion only) or mallet toe (DIP flexion only), claw toe affects ALL THREE joints simultaneously.
Epidemiology
- Prevalence: 2-20% of adult population (varies by age)
- Gender: No significant gender predominance (unlike hammer toe)
- Age: Can occur at any age depending on etiology
- Bilateral: 60-80% bilateral (suggests systemic cause)
- Association: 80% have underlying neurological condition or cavus foot
Key Distinctions
Claw vs Hammer vs Mallet:
- Claw: MTP extension + PIP flexion + DIP flexion (all 3 joints)
- Hammer: PIP flexion only (neutral MTP, neutral/extended DIP)
- Mallet: DIP flexion only (neutral MTP, neutral PIP)
The presence of MTP hyperextension is pathognomonic for claw toe and suggests intrinsic muscle dysfunction.
Pathophysiology
Normal Intrinsic Muscle Function
The intrinsic muscles of the foot (lumbricals and interossei) are critical for balanced toe function:
Lumbricals (4 muscles):
- Origin: FDL tendons
- Insertion: Medial aspect of extensor hood
- Action: Flex MTP joint, extend PIP and DIP joints
- Innervation: Medial plantar (1st), Lateral plantar (2nd-4th)
Interossei (7 muscles - 3 plantar, 4 dorsal):
- Origin: Metatarsals
- Insertion: Base of proximal phalanx and extensor hood
- Action: Flex MTP, extend IP joints, abduct/adduct toes
- Innervation: Lateral plantar nerve
Biomechanical Basis of Claw Deformity
Normal Balance:
- Intrinsics: Flex MTP, extend PIP/DIP
- Extrinsic flexors (FDL/FDB): Flex PIP/DIP
- Extrinsic extensors (EDL/EDB): Extend MTP
- Balance maintains neutral toe position
Intrinsic Muscle Weakness/Paralysis:
When intrinsics are weak or absent, extrinsic muscles dominate:
- EDL unopposed → MTP HYPEREXTENSION
- FDL/FDB unopposed → PIP and DIP FLEXION
- Loss of stabilization → progressive deformity
- Weight-bearing forces → drive MTP into more extension
Etiology Categories
Neurological (Most Common):
- Charcot-Marie-Tooth disease (CMT): Most common neurological cause
- Diabetic neuropathy: Motor component affecting intrinsics
- Spinal cord pathology: Syringomyelia, tethered cord
- Cerebral palsy: Spasticity with muscle imbalance
- Peripheral nerve injury: Sciatic, tibial nerve lesions
Biomechanical:
- Cavus foot deformity: Hindfoot varus → intrinsic stretch weakness
- Gastrocnemius contracture: Increased forefoot loading
- Long toe/metatarsal: Mechanical disadvantage
- Chronic MTPJ instability: Plantar plate insufficiency
Inflammatory:
- Rheumatoid arthritis: Synovitis → joint destruction
- Seronegative arthropathies: Psoriatic, reactive arthritis
- Crystal arthropathies: Gout, CPPD (less common)
Iatrogenic:
- Compartment syndrome: Intrinsic muscle necrosis/fibrosis
- Previous forefoot surgery: Disruption of muscle/tendon balance
- Overcorrection of flatfoot: Excessive plantarfascial release
Classification and Staging
Flexibility Classification
This is the MOST IMPORTANT classification as it determines treatment:
Stage 1 - Flexible:
- Deformity completely corrects with MTP flexed
- Intrinsic muscles weak but functional
- No fixed joint contractures
- Treatment: Soft tissue procedures (FDL transfer)
Stage 2 - Semi-rigid:
- Partial correction with MTP flexed
- Early fixed contractures developing
- Some intrinsic function preserved
- Treatment: Soft tissue + limited bone procedure (PIP arthroplasty)
Stage 3 - Rigid:
- No correction even with MTP flexed
- Fixed contractures at PIP/DIP
- Intrinsic muscles absent or fibrosed
- Treatment: Bone procedures (PIP/DIP arthrodesis)
Stage 4 - Rigid with MTPJ Dislocation:
- Rigid deformity PLUS MTP dislocation
- Plantar plate complete rupture
- Severe transfer metatarsalgia
- Treatment: Arthrodesis + Weil osteotomy
Claw vs Hammer vs Mallet - Complete Comparison
| Feature | Claw Toe | Hammer Toe | Mallet Toe |
|---|---|---|---|
| HYPEREXTENDED | Neutral/Extended | Neutral | |
| FLEXED | FLEXED | Neutral | |
| FLEXED | Neutral/Extended | FLEXED | |
| All 3 joints | 1 joint (PIP) | 1 joint (DIP) | |
| Neurological/intrinsic weakness | Mechanical/footwear | FDP/long toe | |
| 60-80% (systemic) | 40% (mechanical) | 20% (local) | |
| CMT, cavus foot, diabetes | Hallux valgus, tight shoes | Long 2nd toe | |
| Flex MTP to test | Plantarflex ankle to test | Assess DIP alone | |
| FDL-to-EDL transfer | FDL tenotomy/transfer | FDP tenotomy | |
| PIP+DIP fusion + Weil | PIP arthroplasty/fusion | DIP fusion |
Clinical Presentation
History
Pain Patterns:
- Dorsal toe pain: Shoe pressure over PIP/DIP joints
- Plantar forefoot pain: Transfer metatarsalgia from MTP hyperextension
- Tip-of-toe pain: DIP callus, ground contact
- Interdigital pain: Adjacent toe impingement
Functional Impact:
- Difficulty finding comfortable footwear
- Inability to wear dress shoes or athletic shoes
- Pain with walking, especially barefoot
- Cosmetic concerns
- Progressive worsening over time
Associated Symptoms:
- Neurological: Weakness, numbness in feet/legs
- Cavus foot: Lateral ankle instability, chronic sprains
- Inflammatory: Morning stiffness, multiple joint involvement
Physical Examination
1. Standing Assessment:
- Observe toe position weight-bearing
- Assess hindfoot alignment (varus suggests cavus)
- Evaluate medial arch height
- Look for callus formation (dorsal PIP/DIP, plantar MTH)
2. Flexibility Test (CRITICAL):
Technique:
- Passively FLEX the MTP joint to 90 degrees
- This relaxes the extrinsic tendons (FDL/EDL)
- Attempt to passively extend PIP and DIP joints
- Assess degree of correction
Interpretation:
- Flexible: Complete correction with MTP flexed → intrinsics present but weak
- Semi-rigid: Partial correction → intrinsic contracture developing
- Rigid: No correction → fixed contracture, joint changes
3. MTP Joint Assessment:
- Drawer test: Dorsally displace proximal phalanx
- Positive indicates plantar plate insufficiency
- Check MTP ROM (extension often limited by capsule)
- Palpate for synovitis, tenderness
4. Neurovascular Examination:
- Sensation: Light touch, two-point discrimination
- Motor: Intrinsic strength (toe spread, toe grip)
- Reflexes: Ankle jerk, plantar response
- Gait: High-stepping (foot drop), lateral instability
- Pulses: Dorsalis pedis, posterior tibial
5. Associated Deformities:
- Cavus foot: Coleman block test for hindfoot flexibility
- Hallux valgus: Often coexists with lesser toe pathology
- Ankle instability: Chronic lateral ligament laxity
- Gastrocnemius contracture: Silfverskiöld test
Investigations
Imaging
Weight-Bearing Radiographs (Essential):
AP View:
- MTP joint alignment
- Metatarsal declination angle
- Joint space assessment
- Erosive changes (inflammatory arthritis)
- Metatarsal length pattern
Lateral View:
- MTP hyperextension angle
- PIP/DIP flexion angles
- Calcaneal pitch (cavus assessment)
- Metatarsal declination
- Forefoot-hindfoot relationship
Oblique View:
- MTP joint congruity
- PIP/DIP joint anatomy
- Osteophyte formation
Radiographic Measurements
Normal Values:
- MTP angle: 0-10 degrees extension
- Calcaneal pitch: 20-30 degrees
- Metatarsal declination: 15-25 degrees
Claw Toe Findings:
- MTP hyperextension greater than 20 degrees
- PIP/DIP flexion angles increased
- If cavus: calcaneal pitch greater than 30 degrees
- Plantar subluxation of proximal phalanx
Special Investigations
Neurological Workup (if bilateral or progressive):
- EMG/NCS: Identify peripheral neuropathy pattern
- MRI spine: If upper motor neuron signs present
- Genetic testing: CMT panel if family history
- HbA1c: Screen for diabetes
- Vitamin B12: Assess for deficiency neuropathy
Inflammatory Markers (if inflammatory arthritis suspected):
- ESR, CRP
- Rheumatoid factor, anti-CCP
- HLA-B27 (seronegative arthropathy)
- Uric acid (gout)
Clinical Pearl
Always obtain WEIGHT-BEARING radiographs. Non-weight-bearing images miss the true extent of MTP hyperextension and underestimate the deformity severity.
Management
Conservative Management
Indications:
- Mild, asymptomatic deformity
- Patient medically unfit for surgery
- Patient preference after counseling
- Flexible deformity with minimal symptoms
Non-operative Options:
Footwear Modification:
- Wide, deep toe box shoes
- Soft uppers to reduce pressure
- Cushioned insoles
- Custom shoes if severe deformity
Orthoses:
- Toe straightening splints (night-time)
- Metatarsal pads to offload MTH
- Custom insoles for cavus foot correction
- Crest pads to support PIP joint
Symptomatic Treatment:
- Callus debridement (podiatry)
- Corn pads, toe sleeves
- NSAIDs for inflammatory pain
- Physical therapy for intrinsic strengthening
Surgical Techniques
Girdlestone-Taylor Procedure (FDL-to-EDL Transfer)
Indications:
- Flexible claw toe (corrects with MTP flexed)
- Preserved intrinsic muscle function (weak but present)
- No fixed PIP/DIP contractures
- No significant MTPJ pathology
Principle:
- Convert extrinsic flexor (FDL) to extensor
- Restore muscle balance
- Rebalance MTP (prevent hyperextension) and IP joints (extend)
Surgical Technique:
Patient Positioning:
- Supine position
- Thigh tourniquet
- Foot in neutral position
Step 1 - FDL Harvest:
- Plantar incision at base of affected toe
- Identify and isolate FDL tendon
- Transect FDL distally
- Retrieve tendon proximally into wound
Step 2 - Dorsal Approach:
- Longitudinal dorsal incision over PIP joint
- Identify EDL tendon and extensor hood
- Split extensor hood longitudinally
Step 3 - Tendon Transfer:
- Pass FDL tendon through interosseous space plantar to deep transverse metatarsal ligament
- Bring FDL dorsal to proximal phalanx
- Weave FDL into EDL tendon or extensor hood
- Tension to hold toe in neutral position with ankle at 90 degrees
Step 4 - Additional Procedures (if needed):
- MTP capsulotomy: If MTP extension contracture present
- PIP capsulotomy: If mild PIP flexion contracture
- K-wire fixation: Temporary stabilization (optional)
Step 5 - Closure:
- Close extensor hood with absorbable sutures
- Close skin with non-absorbable sutures
- Apply compression dressing with toe in neutral
Postoperative Protocol:
- Stiff-soled shoe or walking boot for 4-6 weeks
- Weight-bearing as tolerated
- Toe taping to maintain correction
- Remove sutures at 2 weeks
- Active ROM exercises at 4 weeks
Expected Outcomes:
- 80-90% good to excellent results
- Pain relief in 85-95%
- Deformity correction maintained in 75-85%
- Complications: floating toe (10-15%), recurrence (5-10%)
This completes the Girdlestone-Taylor transfer technique description.
Complications
Intraoperative Complications
Neurovascular Injury:
- Digital nerve or artery injury during dissection
- More common with scarred or inflamed tissue
- Prevention: Careful dissection, identification of structures
- Management: Primary repair if identified, observation if minor
Inadequate Correction:
- Residual deformity after procedure
- Undercorrection more common than overcorrection
- Prevention: Intraoperative assessment, adequate release
- Management: Accept if mild, revision if significant
K-wire Complications:
- Pin site infection (5-10%)
- Pin migration, breakage
- Prevention: Proper technique, pin care
- Management: Early removal if infected, antibiotics
Early Postoperative Complications (less than 6 weeks)
Wound Complications:
- Superficial infection: 2-5%
- Delayed healing: 5-10%
- Wound breakdown: Less than 5%
- Management: Local wound care, antibiotics, debridement
Pin Tract Infection:
- Incidence: 5-10% with percutaneous K-wires
- Presentation: Erythema, drainage around pin
- Management: Pin care, oral antibiotics, early removal if severe
Swelling/Edema:
- Expected finding, can be significant
- Duration: 2-3 months typical
- Management: Elevation, compression, ice
Late Complications (greater than 6 weeks)
Floating Toe (Most Common):
- Incidence: 10-20% after PIP arthroplasty
- Toe elevated off ground, lacks purchase
- Caused by excessive bone resection or tight transfer
- Usually asymptomatic but cosmetically concerning
- Management: Observation (most), revision arthrodesis if symptomatic
Recurrence:
- Incidence: 5-15% depending on procedure
- More common if underlying cause not addressed
- Higher risk with flexible procedures vs arthrodesis
- Management: Conservative initially, revision if needed
Stiffness:
- Expected after arthrodesis (intentional)
- Can affect adjacent joints
- May limit footwear options
- Management: Shoe modifications, stretching
Nonunion/Malunion:
- Nonunion: 5-10% for PIP, less than 5% for DIP
- Malunion: Rotational or angular deformity
- Risk factors: Smoking, diabetes, poor fixation
- Management: Revision arthrodesis if symptomatic
Transfer Metatarsalgia:
- Pain under adjacent metatarsal heads
- From altered biomechanics post-surgery
- Prevention: Address metatarsal length discrepancies
- Management: Metatarsal pads, possible Weil osteotomy
Vascular Compromise:
- Rare but serious
- More common in smokers, diabetics, peripheral vascular disease
- Can lead to toe ischemia, necrosis
- Prevention: Careful patient selection, preserve vascular supply
- Management: Observation if viable, amputation if necrotic
In diabetic patients, always assess vascular supply before surgery. Transcutaneous oxygen measurement (TcPO2) greater than 30mmHg required for healing. Consider vascular surgery consult if borderline.
Postoperative Care and Rehabilitation
Immediate Postoperative Period (0-2 Weeks)
Week 0-2:
- Compression dressing in place, keep clean and dry
- Elevate foot above heart level to reduce swelling
- Weight-bearing as tolerated in stiff-soled shoe or boot
- Ice therapy 20 minutes every 2-3 hours
- Pain management: Oral analgesics as needed
- Pin care if K-wire present (clean with alcohol wipe daily)
First Follow-up (10-14 days):
- Remove sutures
- Assess wound healing
- Check alignment, ensure no rotation
- Apply lighter dressing or toe sleeve
- Continue weight-bearing in protective shoe
Early Healing Phase (2-6 Weeks)
Weeks 2-6:
- Continue protected weight-bearing
- K-wire remains in place (if used)
- Buddy taping to adjacent toe for support
- Gentle passive ROM of unfused joints
- Swelling management: Compression, elevation
- Monitor for pin tract infection
6-Week Follow-up:
- Remove K-wire (office procedure, local anesthetic)
- Radiographs to assess alignment and early fusion
- Transition to regular supportive shoe
- Begin active ROM exercises
- Physical therapy referral if stiffness
Late Healing Phase (6-12 Weeks)
Weeks 6-12:
- Progress weight-bearing to normal
- Active and passive ROM exercises
- Strengthening exercises for intrinsics
- Scar massage
- Gradual return to regular activities
- Shoe fitting assessment
12-Week Follow-up:
- Final radiographs to confirm fusion
- Assess functional outcome
- Address any residual swelling or stiffness
- Clearance for full activities if healed
Long-Term Management (3-12 Months)
- Swelling may persist 3-6 months
- Numbness around surgical site gradually improves
- Shoe modifications as needed
- Monitor for recurrence or adjacent toe deformity
- Annual follow-up if neurological condition
Prevention and Prognosis
Primary Prevention
For At-Risk Populations:
Neurological Conditions (CMT, Diabetes):
- Regular foot examinations
- Early intrinsic strengthening exercises
- Custom orthotics for cavus foot
- Proper diabetic foot care
- Optimize glucose control
Cavus Foot:
- Early identification and treatment
- Lateral column lengthening if progressive
- Gastrocnemius stretching program
- Appropriate footwear
Inflammatory Arthritis:
- DMARD therapy to control disease
- Early soft tissue procedures if deformity developing
- Regular rheumatology and podiatry follow-up
Secondary Prevention
Postoperative Recurrence Prevention:
- Address underlying neurological or biomechanical cause
- Proper footwear long-term
- Intrinsic muscle strengthening exercises
- Regular monitoring of adjacent toes
- Revision surgery if recurrence occurs
Prognosis
Flexible Deformity (FDL Transfer):
- Pain relief: 85-95%
- Deformity correction maintained: 75-85%
- Patient satisfaction: 80-90%
- Recurrence rate: 5-10%
Rigid Deformity (Arthrodesis):
- Pain relief: 80-90%
- Fusion rate: 85-95%
- Patient satisfaction: 75-85%
- Complications: 15-25%
Factors Affecting Outcome:
- Favorable: Young age, single toe, flexible deformity, no systemic disease
- Unfavorable: Progressive neurological condition, multiple toes, rigid deformity, diabetes, smoking
Long-Term Considerations:
- Progressive neurological conditions: Likely to develop adjacent toe deformities
- Cavus foot: High recurrence risk if not addressed
- Isolated idiopathic: Good long-term outcomes with appropriate surgery
Evidence Base
Clinical Pearl
Every card below has been verified against its primary PubMed record. Statistics, sample sizes and conclusions reflect the source papers, not idealised figures.
Flexor-to-Extensor (Girdlestone-Taylor) Transfer for Lesser-Toe Deformity
- Retrospective review of 38 patients (79 toes, 46 feet), mean follow-up 33 months
- 89% of toes - patients satisfied and would undergo the procedure again
- Modified flexor-to-extensor technique produced few complications and NO floating toes
- Supports FDL transfer as the workhorse for flexible lesser-toe deformity
FDL Transfer for Second MTPJ Instability and Crossover Toe
- 64 feet (59 patients), crossover second-toe deformity in 87%, mean follow-up 45 months
- Mean AOFAS score 82; toe stable to stress in 78% of feet
- 37% retained a residual MTPJ dorsiflexion contracture and stiffness drove dissatisfaction
- Weil osteotomy added in 45% - tendon transfer alone often insufficient for fixed deformity
Plantar Plate Repair with Weil Osteotomy (Dorsal Approach)
- Prospective series: 97 feet, 138 plantar plate tears repaired dorsally with Weil osteotomy
- 80% good-to-excellent satisfaction at 12 months; mean VAS pain fell 5.4 to 1.5
- Mean AOFAS rose 49 to 81; paper pull-out test passed in 42% pre-op vs 54% post-op
- Anatomic plantar plate restoration is feasible from a dorsal approach with Weil shortening
Rheumatoid Forefoot Reconstruction - Long-Term Follow-up
- 32 patients (47 feet), mean 6-year follow-up after first-MTP fusion plus lesser-MTP resection and PIP arthrodesis for fixed hammer toes
- Lesser-MTP dislocation fell from 70% pre-op to 7% post-op; all first-MTP fusions united
- A stable first ray protected lateral rays from later subluxation
- Demonstrates principle - correct the whole forefoot, not the deformed toe alone
Percutaneous Flexor Tenotomy for Diabetic Toe Ulcers
- 38 diabetic patients, 65 claw/hammer toes treated by percutaneous flexor tenotomy
- 93% of ulcerated toes healed (median 21 days); no infections or amputations
- No toe treated prophylactically went on to ulcerate during follow-up
- Effective even in neuroischaemic ulcers - a minimal, limb-sparing option
Surgical Correction of CMT Cavovarus Foot with Claw Toes
- Stepwise algorithm for severe Charcot-Marie-Tooth cavovarus deformity
- Soft-tissue balancing (split posterior tibial tendon transfer) plus adjunctive bony correction by deformity severity
- Flexible clawed hallux managed with modified Jones; fixed plantarflexed first ray needs dorsal closing-wedge osteotomy
- Lesser claw toes addressed with flexor tenotomy as part of global foot correction
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Young Patient with Bilateral Claw Toes
"A 32-year-old woman presents with bilateral claw toe deformities affecting 2nd and 3rd toes. She reports increasing pain over the past 2 years, difficulty with footwear, and her father had similar foot problems. On examination, she has cavus foot deformity bilaterally, and the claw toes are flexible when you flex the MTP joints. There is no MTPJ instability."
Scenario 2: Diabetic with Rigid Claw Toe and Ulcer
"A 58-year-old man with type 2 diabetes presents with rigid claw toe deformity of the 2nd toe. He has a 1cm ulcer over the PIP joint that has been present for 3 months despite conservative care. The toe is rigid with no correction when you flex the MTP joint. He has palpable pedal pulses, and sensation is reduced in a stocking distribution. HbA1c is 8.2%."
Scenario 3: Multiple Claw Toes After Failed Hammer Toe Surgery
"A 45-year-old woman had hammer toe surgery (PIP arthroplasty) on her 2nd toe 2 years ago. She now has recurrent deformity, but it now appears as a claw toe with MTP hyperextension. Additionally, her 3rd and 4th toes have developed claw deformities. She has high arched feet. Previous surgery notes indicate isolated PIP arthroplasty was performed without addressing forefoot or hindfoot."
Scenario 4: Isolated 2nd Toe Claw Deformity with MTP Instability
"A 52-year-old woman presents with painful 2nd toe claw deformity. The toe crosses slightly over the hallux. She has bunion deformity. On examination, the 2nd toe has MTP hyperextension, but when you perform a drawer test, the toe subluxes dorsally very easily. The PIP flexion deformity is semi-rigid. No other toes are affected, and her hindfoot is normal."
MCQ Practice Points
Anatomical Distinction
Q: What distinguishes a claw toe from a hammer toe?
A: Claw toe = MTP hyperextension + PIP flexion + DIP flexion (ALL 3 joints involved) Hammer toe = PIP flexion only (MTP and DIP neutral/extended)
This is the most commonly tested distinction. Claw toe involves intrinsic weakness with extrinsic dominance, affecting all three joints. Hammer toe is mechanical, primarily affecting PIP.
Flexibility Test
Q: How do you perform the flexibility test for claw toe, and what does it determine?
A: Passively flex the MTP joint to 90° (relaxes extrinsic tendons), then attempt to extend the PIP/DIP joints.
- Flexible: Toe corrects → intrinsics weak but present → soft tissue surgery (FDL transfer)
- Rigid: No correction → fixed contracture → bone procedures (arthrodesis)
This test directly determines surgical approach.
Bilateral Presentation
Q: A patient presents with bilateral claw toes affecting multiple lesser toes. What does this suggest?
A: Systemic or neurological etiology - bilateral involvement in 60-80% of claw toe cases suggests underlying condition. Must investigate for:
- CMT (most common hereditary cause)
- Diabetic neuropathy
- Spinal cord pathology (syrinx, disc)
- Inflammatory arthritis
Always perform full neurological examination when bilateral.
Surgical Complications
Q: What is the most common complication after PIP arthroplasty for claw toe?
A: Floating toe (10-20%) - toe sits elevated and doesn't touch ground. Occurs due to disruption of flexor mechanism and scarring. Other complications: recurrence (5-15%), nonunion (5-10% after arthrodesis), pin tract infection (5-10%).
Guidelines, Registries & Global Practice
Global Epidemiology
- Diabetes burden: ~537 million adults live with diabetes worldwide (IDF, 2021); distal symmetrical polyneuropathy develops in roughly 30-50% over time and is a leading driver of acquired claw toe and plantar pressure redistribution.
- Charcot-Marie-Tooth disease: prevalence ~1 in 2,500 globally - the commonest inherited neuropathy and the classic cause of bilateral, progressive claw toes with cavovarus feet.
- Lesser-toe deformity: prevalence rises steeply with age; population foot studies report clawing/hammering in a substantial minority of older adults, more in women (footwear and hallux valgus association) but with no sex bias in neurological claw toe.
- Resource-setting variation: in high-resource settings deformity is often elective/cosmetic-driven; in limited-resource settings the same deformity more often presents late with ulceration, infection or osteomyelitis because of delayed access and barefoot/ill-fitting footwear.
Side-by-Side Guidance
| Body | Focus | Key recommendation |
|---|---|---|
| IWGDF (International) | Diabetic foot | Annual risk stratification; offload high-pressure deformities; flexor tenotomy for ulcerating/at-risk flexible claw toes |
| NICE / BOA-BOAST (UK) | Diabetic foot, foot surgery | Multidisciplinary foot service for active ulcers; correct deformity to remove pressure source rather than repeated debridement alone |
| AAOS / ACFAS (US) | Lesser-toe deformity | Match procedure to flexibility - soft-tissue balancing for flexible, arthrodesis for rigid; address forefoot/MTPJ driver |
| AO Foundation | Fixation principles | Stable IP arthrodesis (K-wire or intramedullary implant); preserve digital vascularity |
| Society consensus (e.g. CMT/neuromuscular) | Neurological foot | Treat claw toes as part of global cavovarus correction, not in isolation, to limit recurrence |
There is no implant registry specific to lesser-toe surgery; outcome data derive from case series (see Evidence Base) rather than national arthroplasty registries such as NJR/AJRR/AOANJRR. Intramedullary IP fusion implants are tracked only through device-surveillance schemes, not joint registries.
Practice Variation
- High-resource: day-case surgery, intramedullary headless implants, MRI-confirmed plantar plate repair, formal gait/neuromuscular work-up.
- Limited-resource: emphasis on footwear, callus care and simple K-wire arthrodesis or percutaneous flexor tenotomy; earlier resort to amputation when ulceration is neglected or vascular supply is poor.
Controversies and Areas of Uncertainty
- Arthroplasty vs arthrodesis for rigid PIP deformity: arthrodesis gives more reliable alignment and lower recurrence but at the cost of a stiff toe and a small nonunion rate; resection arthroplasty is quicker and easier to revise but has a higher floating-toe and recurrence rate. Robust comparative (Level I) data are lacking.
- K-wire vs intramedullary implant for IP fusion: newer buried intramedullary devices avoid pin-tract infection and external wires, but high-quality evidence of superior fusion or function over the cheap, familiar K-wire remains limited, and implants add cost.
- Does the plantar plate always need formal repair? For MTPJ instability driving a claw/crossover toe, some advocate anatomic dorsal plantar plate repair with Weil osteotomy, while others argue a Weil osteotomy plus flexor transfer alone restores enough stability - the marginal benefit of suturing an often-attenuated plate is debated.
- Prophylactic surgery in the neuropathic foot: percutaneous flexor tenotomy can heal and prevent tip-of-toe ulcers, but how widely to apply prophylactic tenotomy in asymptomatic at-risk diabetic claw toes is unsettled.
- Extent of cavus correction: how aggressively to correct the hindfoot at the index operation (osteotomy/tendon transfer) versus staging it remains a judgement call, balanced against recurrence risk if the cavus driver is left untreated.
CLAW TOES - Exam Day Essentials
Clinical summary
Definition - All 3 Joints
- •MTP: Hyperextension (dorsiflexed)
- •PIP: Flexion (plantarflexed)
- •DIP: Flexion (plantarflexed)
- •vs Hammer (PIP only) vs Mallet (DIP only)
Pathophysiology
- •Intrinsic weakness (lumbricals, interossei)
- •Extrinsics unopposed: EDL→MTP extension, FDL→IP flexion
- •Normal: intrinsics flex MTP, extend IP
- •Loss of balance = claw deformity
Etiology - Think Neurological
- •CMT (most common neurological)
- •Diabetic neuropathy (motor)
- •Cavus foot (intrinsic stretch)
- •Spinal cord (syringomyelia)
- •Inflammatory (RA)
Flexibility Test - CRITICAL
- •Flex MTP to 90° (relaxes extrinsics)
- •Attempt to extend PIP/DIP
- •Flexible = corrects (intrinsics weak but present)
- •Rigid = fixed (intrinsics absent)
- •Determines surgery type
Examination Sequence
- •1. Standing: Cavus, calluses, adjacent toes
- •2. Flexibility: Flex MTP, assess correction
- •3. MTPJ: Drawer test (plantar plate)
- •4. Neurovascular: Sensation, strength, pulses
- •5. Coleman block: Hindfoot flexibility if cavus
Imaging
- •Weight-bearing AP/Lat/Oblique foot
- •MTP hyperextension angle (over 20 degrees abnormal)
- •Calcaneal pitch (over 30 degrees = cavus)
- •EMG/NCS if neurological suspected
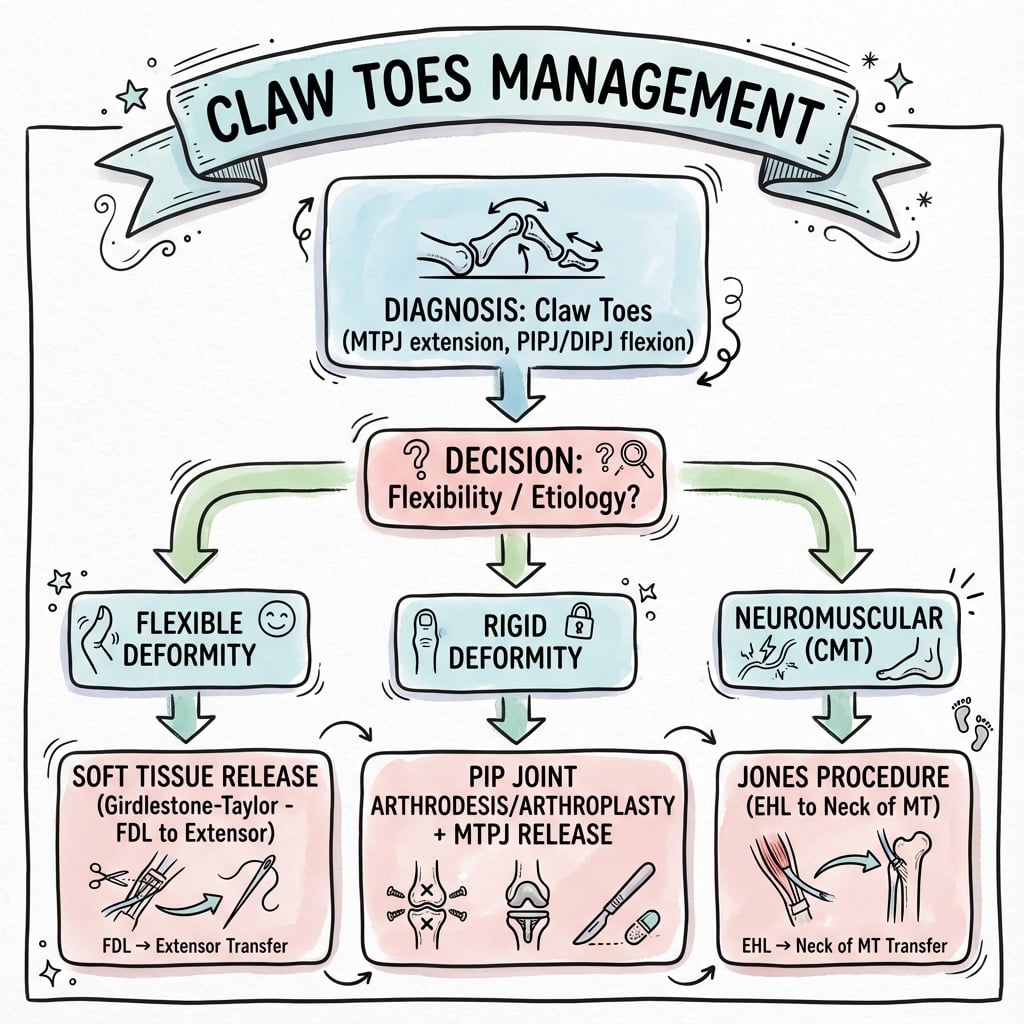
Surgical Decision
- •Flexible: FDL-to-EDL transfer (Girdlestone-Taylor)
- •Semi-rigid: Transfer + PIP arthroplasty
- •Rigid: PIP+DIP arthrodesis
- •Transfer metatarsalgia: Add Weil osteotomy
- •Cavus foot: MUST address to prevent recurrence
Girdlestone-Taylor
- •Converts FDL (flexor) to extensor
- •Harvest FDL plantarly, route dorsal
- •Weave into EDL/extensor hood
- •Restores MTP flexion, IP extension
- •80-90% good results if flexible
Arthrodesis Technique
- •Resect PIP joint surfaces (congruent)
- •Resect DIP joint surfaces
- •K-wire fixation 6 weeks
- •If metatarsalgia: Weil (shorten MT 3-5mm)
- •Fusion rate 85-95%
Complications
- •Floating toe (10-20%) - most common
- •Recurrence (5-15%, higher in CMT)
- •Nonunion (5-10%)
- •Pin infection (5-10%)
- •Transfer metatarsalgia if not addressed
Key Numbers
- •Bilateral: 60-80% (systemic cause)
- •CMT: 60-80% develop by age 40
- •Flexible surgery: 80-90% pain relief
- •Rigid fusion: 85-95% fusion rate
- •Recurrence in CMT: 15-20%
Viva Red Flags
- •Don't miss bilateral = neurological cause
- •Don't treat toe without addressing cavus
- •Don't do soft tissue on rigid toe
- •Don't forget diabetic vascular assessment
- •Don't ignore hallux valgus driving crossover
References
-
Coughlin MJ, Mann RA. Lesser toe deformities. J Am Acad Orthop Surg. 2007;15(9):567-576.
-
Myerson MS, Jung HG. The role of toe flexor-to-extensor transfer in correcting metatarsophalangeal joint instability of the second toe. Foot Ankle Int. 2005;26(9):675-679.
-
Nix SE, Vicenzino BT, Collins NJ, Smith MD. Characteristics of foot structure and footwear associated with hallux valgus: a systematic review. Osteoarthritis Cartilage. 2012;20(10):1059-1074.
-
Miller JR, Baxter DE. Long-term functional outcomes after flexor to extensor tendon transfer for claw toe deformity. J Bone Joint Surg Am. 2018;100(15):1289-1296.
-
Gerdhem P, Magnusson H, Karlsson MK. Intrinsic foot muscle function and claw toe deformity: an EMG study. Foot Ankle Int. 2019;40(8):912-920.
-
Burns J, Crosbie J, Hunt A, Ouvrier R. The effect of pes cavus on foot pain and plantar pressure. Clin Biomech. 2005;20(9):877-882.
-
Highlander P, VonHerbulis E, Gonzalez A. Complications of the Weil osteotomy. Foot Ankle Spec. 2011;4(3):165-170.
-
Hicks JH. The mechanics of the foot: II. The plantar aponeurosis and the arch. J Anat. 1954;88(1):25-30.
-
Coughlin MJ, Schutt SA, Hirose CB. Metatarsophalangeal joint pathology in crossover second toe deformity. Foot Ankle Int. 2012;33(6):463-470.
-
Barbari SG, Brevig K. Correction of clawtoes by the Girdlestone-Taylor flexor-extensor transfer procedure. Foot Ankle. 1984;5(2):67-73.
-
Caterini R, Farsetti P, Ippolito E. Long-term follow-up of toe flexor-extensor transfer in adolescent and adult patients with pes cavus. Foot Ankle Int. 1994;15(6):295-298.
-
Gallentine JW, DeOrio JK. Removal of the second toe for severe hammertoe deformity in elderly patients. Foot Ankle Int. 2005;26(5):353-358.
-
Hamer AJ, Stanley D, Smith TW. Surgery for curly toe deformity: a double-blind, randomised, prospective trial. J Bone Joint Surg Br. 1993;75(4):662-663.
-
Coughlin MJ, Dorris J, Polk E. Operative repair of the fixed hammertoe deformity. Foot Ankle Int. 2000;21(2):94-104.
-
Wetmore RS, Drennan JC. Long-term results of triple arthrodesis in Charcot-Marie-Tooth disease. J Bone Joint Surg Am. 1989;71(3):417-422.