CAVE Deformity | Ponseti Method Gold Standard | Tenotomy in 90% | Bracing Critical
PIRANI SEVERITY SCORING
Critical Must-Knows
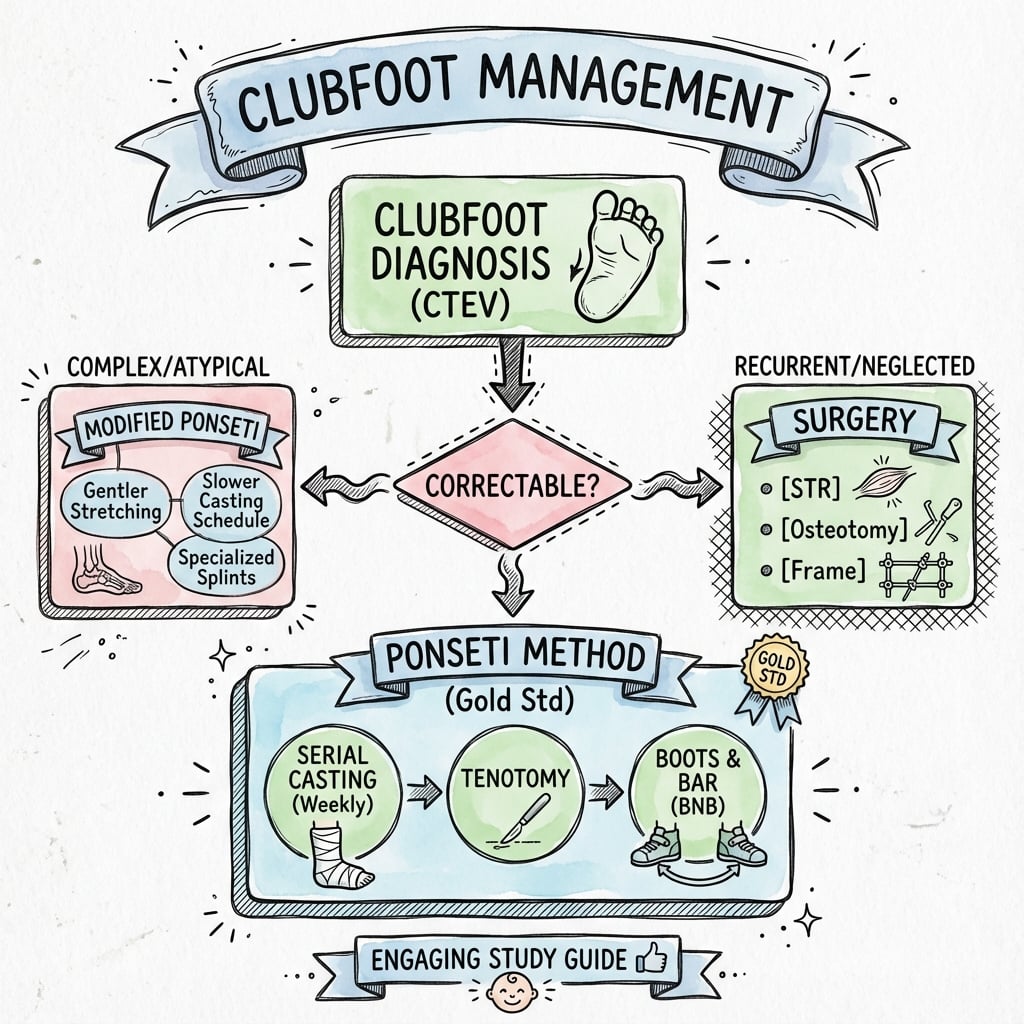
- CAVE deformity: Cavus, Adductus, Varus, Equinus - corrected in this specific order
- Ponseti method: Gold standard - serial casting corrects all except equinus, then tenotomy
- Tenotomy timing: After foot corrected to 60-70 degrees abduction, perform percutaneous Achilles tenotomy
- Bracing critical: FAO (foot abduction orthosis) prevents recurrence - 23hrs/day for 3 months then nighttime until age 4-5
- Recurrence causes: Non-compliance with bracing is the #1 cause, occurs in 30-40% without proper bracing
Clinical Pearls
- "Correct cavus FIRST by supinating the forefoot to align with hindfoot
- "Never pronate the forefoot - worsens cavus and creates rocker-bottom deformity
- "Talar head is the fulcrum for correction - thumb pressure over lateral talar head
- "Abduction occurs at calcaneocuboid joint, NOT midfoot
Clinical Imaging
Imaging Gallery



Critical Clubfoot Exam Points
Ponseti Order of Correction
CAVE order is critical: Correct Cavus first (supinate forefoot), then Adductus and Varus together (abduct around talar head), then Equinus last (Achilles tenotomy). Never dorsiflex before foot is abducted - creates rocker-bottom deformity.
Talar Head Fulcrum
Thumb pressure on lateral talar head is the key to correction. The talar head can be palpated anterolateral to the ankle. All abduction and varus correction occurs by rotating the foot around this fixed point. Do NOT apply countertraction on calcaneus.
Tenotomy Indications
Percutaneous Achilles tenotomy required in 90% of cases. Indications: Foot abducted to 60-70 degrees but cannot dorsiflex past neutral. Perform under local anesthesia as outpatient procedure. Tendon regenerates in 3 weeks in long leg cast.
Bracing Prevents Recurrence
Foot Abduction Orthosis (FAO) is mandatory for 4-5 years. Boots fixed to bar at 70 degrees external rotation (60 degrees for unilateral). Shoulder-width apart. Non-compliance causes 80% of recurrences. Educate parents extensively.
Quick Decision Guide - Clubfoot Management
| Clinical Scenario | Findings | Treatment | Key Pearl |
|---|---|---|---|
| Newborn with typical idiopathic clubfoot | CAVE deformity, Pirani 4-6, flexible | Ponseti casting starting week 1-2, tenotomy, FAO | Start early, parents as partners in treatment |
| Syndromic clubfoot (arthrogryposis, myelomeningocele) | Rigid, associated anomalies, resistant | Extended Ponseti, often surgical release needed | Stiffer feet need more casts, higher recurrence |
| Relapsed clubfoot after initial Ponseti | Recurrent equinus or varus, loss of abduction | Repeat casting, tenotomy, tibialis anterior transfer if over 2.5 years | Check bracing compliance first |
| Neglected clubfoot (older child, walking age) | Rigid deformity, callosities, adapted gait | Soft tissue release or osteotomies depending on age/rigidity | Ponseti less effective after walking age |
CAVECAVE - Clubfoot Deformity Components
| C | Cavus High medial arch from plantar-flexed 1st ray |
| A | Adductus Forefoot adducted (deviated medially) at midfoot |
| V | Varus Hindfoot in varus (heel turned inward) |
| E | Equinus Ankle in plantar flexion (foot points down) |
| C | Cavus High medial arch from plantar-flexed 1st ray | V | Varus Hindfoot in varus (heel turned inward) |
| A | Adductus Forefoot adducted (deviated medially) at midfoot | E | Equinus Ankle in plantar flexion (foot points down) |
Hook:CAVE - the foot is hiding in a cave, all curled up. Correct in this exact order during Ponseti treatment.
PIRANIPIRANI - Severity Score Components
| P | Posterior crease Deep posterior heel crease (0, 0.5, 1) |
| I | Inflexible equinus Rigid equinus deformity (0, 0.5, 1) |
| R | Rigid hindfoot Empty heel - calcaneus not palpable (0, 0.5, 1) |
| A | Adduction of forefoot Curved lateral border (0, 0.5, 1) |
| N | No talar head coverage Lateral talar head palpable (0, 0.5, 1) |
| I | Inflexible medial crease Deep medial crease (0, 0.5, 1) |
| P | Posterior crease Deep posterior heel crease (0, 0.5, 1) | R | Rigid hindfoot Empty heel - calcaneus not palpable (0, 0.5, 1) | N | No talar head coverage Lateral talar head palpable (0, 0.5, 1) |
| I | Inflexible equinus Rigid equinus deformity (0, 0.5, 1) | A | Adduction of forefoot Curved lateral border (0, 0.5, 1) | I | Inflexible medial crease Deep medial crease (0, 0.5, 1) |
Hook:PIRANI scores 0-6 total (3 hindfoot + 3 midfoot signs). Higher score = more severe. Guide treatment intensity.
PONSETIPONSETI - Treatment Steps
| P | Position Supinate forefoot to correct cavus first |
| O | Outward rotation Abduct foot around talar head (correct varus/adductus) |
| N | No countertraction Do not push on calcaneus or evert foot |
| S | Serial casting 5-7 casts, changed weekly |
| E | Equinus last Percutaneous Achilles tenotomy corrects equinus |
| T | Tendon regeneration Cast 3 weeks post-tenotomy in maximum dorsiflexion |
| I | Insist on bracing FAO bracing for 4-5 years prevents recurrence |
| P | Position Supinate forefoot to correct cavus first | S | Serial casting 5-7 casts, changed weekly | I | Insist on bracing FAO bracing for 4-5 years prevents recurrence |
| O | Outward rotation Abduct foot around talar head (correct varus/adductus) | E | Equinus last Percutaneous Achilles tenotomy corrects equinus | ||
| N | No countertraction Do not push on calcaneus or evert foot | T | Tendon regeneration Cast 3 weeks post-tenotomy in maximum dorsiflexion |
Hook:PONSETI is the name and the method - follow his exact technique for 95%+ success rate.
Overview and Epidemiology
Clubfoot (Congenital Talipes Equinovarus - CTEV) is one of the most common congenital musculoskeletal deformities. It is a complex three-dimensional deformity of the foot and ankle characterized by equinus, varus, adduction, and cavus (CAVE).
Epidemiology:
- Incidence varies by ethnicity: Maori/Polynesian 6-7:1000, Caucasian 1:1000, Asian 0.5:1000
- Male to female ratio 2:1
- Bilateral in 50% of cases
- Positive family history in 25% (multifactorial inheritance)
Idiopathic vs Syndromic
80% of clubfoot is idiopathic (isolated deformity in otherwise normal child). 20% is associated with syndromes (arthrogryposis, myelomeningocele, Larsen syndrome, diastrophic dysplasia) or other anomalies. Syndromic clubfoot is more rigid, has higher recurrence rates, and often requires surgical intervention.
Etiology:
Genetic Factors
- Multifactorial inheritance: 25% have affected family member
- Concordance: 33% in monozygotic twins, 3% in dizygotic
- Genes implicated: PITX1, TBX4, muscle contractile proteins
- Risk: 3-4% if one sibling affected, 10-20% if parent affected
Environmental Factors
- Intrauterine crowding: Oligohydramnios association
- Smoking: Maternal smoking increases risk 1.5-2x
- Neuromuscular imbalance: Theory of muscle abnormality
- Vascular disruption: Proposed mechanism in some cases
Associated Conditions (screen all patients):
- Hip dysplasia (DDH): 3-5% association - clinical hip exam required
- Torticollis: 5% association - examine neck
- Myelomeningocele: Examine spine for dimple, tuft, lipoma
- Syndromes: Look for multiple congenital anomalies
Pathophysiology and Mechanisms
Three-Dimensional Deformity
The clubfoot deformity involves abnormal relationships between the talus, calcaneus, navicular, and cuboid. Understanding the pathoanatomy is essential for correction.
Bones and Their Positions in Clubfoot
| Bone | Normal Position | Clubfoot Position | Correction Goal |
|---|---|---|---|
| Talus | 90 degrees tibiotalar articulation | Plantar flexed, externally rotated, laterally tilted in mortise | Cannot be directly manipulated - other bones rotate around it |
| Calcaneus | Below talus, neutral alignment | Inverted (varus), adducted, rotated under talus | Abduct and evert by stretching medial structures |
| Navicular | Aligned with talar head | Severely medially displaced, may abut medial malleolus | Reduce onto talar head with abduction |
| Cuboid | Aligned with calcaneus | Medially displaced relative to calcaneus | Follows correction of calcaneus |
Talus is the Key
The talus is the fixed point around which all correction occurs. In clubfoot, the talus is plantar flexed in the ankle mortise and externally rotated relative to the leg. You cannot directly manipulate the talus. Instead, the navicular, calcaneus, and cuboid are rotated laterally around the talar head through Ponseti manipulation.
Soft Tissue Contractures
Contracted Structures (Medial/Posterior)
- Achilles tendon: Causes equinus - requires tenotomy
- Posterior tibial tendon: Contributes to varus and adduction
- Toe flexors (FDL, FHL): May contribute to cavus
- Tibionavicular ligament: Tethers navicular medially
- Plantar fascia: Contributes to cavus
- Deltoid ligament: Fibrosed, limits valgus
Attenuated Structures (Lateral)
- Peroneal tendons: Stretched over lateral malleolus
- Lateral ligaments: Attenuated from varus position
- Calcaneofibular ligament: May be lax
- Anterior talofibular ligament: Stretched
Muscle and Tendon Abnormalities
Muscle Fiber Abnormalities
Histological studies show increased Type 1 muscle fibers (slow twitch) in clubfoot muscles, with smaller fiber diameter and increased collagen content. This contributes to the stiffness of the deformity. The posterior compartment muscles (gastrocnemius, soleus) are particularly affected.
Biomechanics of Correction:
- Cavus is corrected by supinating the forefoot (aligning 1st ray with hindfoot)
- This creates a single fulcrum for correction at talar head
- Abduction stretches contracted medial structures
- Calcaneus derotates and everts beneath talus
- Equinus is addressed last via Achilles tenotomy
Classification Systems
Pirani Severity Scoring System
Most widely used clinical scoring system - assesses 6 clinical signs to guide treatment and predict outcomes.
| Category | Sign | 0 (Normal) | 0.5 (Moderate) | 1 (Severe) |
|---|---|---|---|---|
| Hindfoot | Posterior crease | Multiple fine creases | 1-2 moderate creases | Single deep crease |
| Hindfoot | Empty heel | Calcaneus easily palpable | Partially palpable | Calcaneus not palpable |
| Hindfoot | Rigidity of equinus | Foot dorsiflexes | Slight dorsiflexion | No dorsiflexion possible |
| Midfoot | Curved lateral border | Straight lateral border | Mild curve | Severe curve/comma shape |
| Midfoot | Medial crease | Multiple fine creases | 1-2 moderate creases | Single deep crease |
| Midfoot | Talar head coverage | Navicular covers talar head | Partial coverage | Talar head fully palpable laterally |
Using Pirani Score
Total score 0-6 (3 hindfoot + 3 midfoot). Score decreases with successful treatment. Use midfoot score to predict number of casts needed. Use hindfoot score (especially empty heel) to predict need for tenotomy. Tenotomy indicated when hindfoot score reaches 0.5-1 but equinus persists.
Clinical Assessment
History:
Prenatal History
- Ultrasound diagnosis: Can be seen from 12-16 weeks gestation
- Oligohydramnios: Associated with clubfoot
- Family history: First-degree relatives with clubfoot
- Other anomalies seen: Hip dysplasia, spina bifida
Birth and Neonatal History
- Gestational age: Prematurity not protective
- Birth trauma: Not a cause of idiopathic clubfoot
- Other congenital anomalies: Hands, spine, hips
- Syndrome features: Multiple anomalies suggest syndromic
Physical Examination:
Systematic Examination
Clubfoot Examination Sequence
Visual assessment:
- Confirm CAVE deformity components present
- Compare bilateral (50% bilateral, may be asymmetric)
- Look for skin creases (medial and posterior - severity markers)
- Assess calf size (smaller on affected side - 1-2cm difference persists)
- Examine spine for stigmata of spinal dysraphism (dimple, tuft, lipoma)
Key palpable landmarks:
- Talar head: Should be covered by navicular - in clubfoot, palpable laterally
- Calcaneus (empty heel sign): Posterior calcaneus difficult to palpate in severe cases
- Forefoot-hindfoot alignment: Is forefoot supinated relative to hindfoot?
- Muscle bulk: Calf wasting, anterior compartment
Ponseti manipulation test:
- Supinate forefoot to correct cavus - does arch flatten?
- Abduct forefoot with talar head as fulcrum - how much correction?
- DO NOT test dorsiflexion until foot is corrected - will create rocker-bottom
- Score flexibility using Pirani or Dimeglio
Screen for associated conditions:
- Hips: Barlow and Ortolani tests for DDH (3-5% association)
- Spine: Midline stigmata - dimple, tuft, lipoma (spinal dysraphism)
- Neck: Torticollis (5% association)
- Full neurological exam: Syndromic clubfoot may have other findings
Rule Out Syndromic Causes
20% of clubfoot is syndromic. Red flags include: bilateral severe rigid clubfoot, other limb anomalies, facial dysmorphism, multiple joint contractures (arthrogryposis), spine abnormalities (myelomeningocele). Syndromic clubfoot has higher recurrence rates and often requires surgical intervention despite initial Ponseti success.
Differential Diagnosis
The key clinical task is separating true (structural) idiopathic clubfoot from postural/positional foot deformities that resolve, and from rigid feet that are syndromic or genuinely different pathology. Reducibility and rigidity are the discriminating features.
Differential Diagnosis of the Equinovarus / In-Turned Newborn Foot
| Condition | Key Distinguishing Features | Rigidity / Reducibility | Management Difference |
|---|---|---|---|
| Idiopathic clubfoot (CTEV) | Full CAVE deformity, calf wasting, medial/posterior creases, talar head palpable laterally | True fixed deformity but responds to Ponseti manipulation | Ponseti casting, tenotomy in most, then bracing |
| Postural (positional) talipes equinovarus | Foot looks turned in but no true cavus or fixed equinus; from intrauterine packing | Fully passively correctable to neutral and beyond | Reassurance and stretching; resolves without casting |
| Metatarsus adductus | Forefoot adduction only; normal hindfoot, NO equinus or hindfoot varus | Usually flexible; convex lateral border | Observation/stretching; casting only if rigid |
| Congenital vertical talus (rocker-bottom) | Convex plantar surface, dorsiflexed/abducted forefoot - the opposite of equinus | Rigid dorsal dislocation of navicular on talus | Reverse Ponseti casting then surgery; often syndromic |
| Syndromic / arthrogrypotic clubfoot | Multiple joint contractures, other limb anomalies, very stiff feet | Markedly rigid, resistant to casting | Extended Ponseti, higher tenotomy/surgery and relapse rates |
| Neurological clubfoot (myelomeningocele, tethered cord) | Spinal stigmata, sensory loss, muscle imbalance | Rigid, insensate, prone to skin breakdown in casts | Cautious casting, address neurological cause, higher relapse |
Investigations
Clinical Diagnosis
Clubfoot is a CLINICAL diagnosis. Imaging is NOT required for diagnosis or routine management. X-rays are reserved for atypical cases, assessment of correction post-treatment, or evaluation of relapse/recurrence.
Imaging Indications:
When to Order X-rays
- Atypical clubfoot: Features not consistent with idiopathic
- Post-treatment assessment: Confirm correction achieved
- Relapse evaluation: Assess bone deformity vs soft tissue recurrence
- Pre-operative planning: Before surgical correction
- Research purposes: Radiographic outcome measures
X-ray Views
- AP foot: Talocalcaneal angle (normally 20-40°, reduced in clubfoot)
- Lateral foot: Tibiocalcaneal angle, talus-1st MT alignment
- Stress views: Maximal dorsiflexion lateral to assess equinus correction
- Kite's angle: Talus-calcaneus parallelism indicates persistent deformity
Radiographic Measurements:
Key Radiographic Angles in Clubfoot
| Measurement | Normal Value | Clubfoot Finding | Clinical Significance |
|---|---|---|---|
| AP talocalcaneal angle | 20-40 degrees | Less than 20 degrees (parallel) | Hindfoot varus - bones parallel |
| Lateral talocalcaneal angle | 25-50 degrees | Less than 25 degrees | Persistent equinus/varus |
| AP talo-1st MT angle | 0-20 degrees | Negative (overlapping) | Forefoot adduction |
| Lateral tibiocalcaneal angle | 10-40 degrees | Less than 10 degrees | Equinus deformity |
Other Investigations:
- Genetic testing: If syndromic features present (karyotype, specific gene panels)
- Spine MRI: If sacral dimple, tuft, or other spinal dysraphism stigmata
- Hip ultrasound: If clinical exam concerning for DDH (routine US not required)
Management Algorithm
Ponseti Technique - Gold Standard
95% success rate when performed correctly and bracing compliance achieved.
Ponseti Treatment Steps
Supinate the forefoot relative to hindfoot:
- Elevate the 1st ray to align with lesser rays
- This flattens the arch and creates a single lever
- DO NOT dorsiflex or pronate the forefoot
- First cast holds this position
Correct adductus and varus together:
- Thumb pressure on lateral talar head (NOT calcaneus)
- Abduct forefoot and midfoot as a unit
- Calcaneus follows and everts beneath talus
- Progressive abduction each cast (60-70 degrees goal)
- Casts changed weekly - each gains 10-15 degrees
Required in 90% of cases when:
- Foot abducted to 60-70 degrees
- Cannot dorsiflex past neutral
- Performed under local anesthetic as outpatient
- Complete tenotomy 1cm above insertion
- Final cast in maximum dorsiflexion for 3 weeks
Dennis-Browne bar with boots:
- 70 degrees external rotation (60 degrees unilateral)
- Shoulder-width bar
- 23 hours/day for 3 months
- Then nighttime only (12 hours) until age 4-5 years
- Non-compliance causes 80% of recurrences
Never Dorsiflex Before Abduction
Dorsiflexing the uncorrected clubfoot creates a rocker-bottom deformity. The talus remains in equinus and the midfoot breaks instead. Always correct cavus first, then abduct to 60-70 degrees, THEN address equinus with tenotomy.

Surgical Technique
Percutaneous Achilles Tenotomy
Indicated in 90% of Ponseti-treated clubfeet after adequate abduction achieved.

Tenotomy Procedure
Outpatient procedure:
- Local anesthesia (0.5-1ml 1% lidocaine) or EMLA cream
- No sedation typically required
- Hold foot in dorsiflexion to identify tight cord
- Mark tenotomy site 1cm above calcaneal insertion
Technique:
- 11 or 15 blade scalpel
- Enter skin medial to Achilles tendon
- Blade parallel to tendon, then rotate 90 degrees
- Cut from anterior (deep) to posterior (superficial)
- Audible/palpable pop when tendon divides
- Foot should immediately dorsiflex 15-20 degrees
Final casting:
- Long-leg cast in maximum dorsiflexion (aim 15 degrees above neutral)
- Maintain 70 degrees abduction
- Leave cast 3 weeks for tendon regeneration
- Tendon heals in lengthened position
Tenotomy Safety
Posterior tibial artery and nerve are located anteromedial to Achilles tendon. By entering medially with blade parallel to tendon, then rotating, the blade moves away from neurovascular structures. Complete tenotomy is important - incomplete section leads to inadequate correction.
Complications
Complications of Clubfoot Treatment
| Complication | Cause | Prevention | Management |
|---|---|---|---|
| Recurrence (30-40%) | Non-compliance with bracing, inadequate initial correction | Parent education, proper bracing protocol, regular follow-up | Repeat Ponseti casting, tenotomy, TATT if over 2.5 years |
| Rocker-bottom deformity | Dorsiflexion before abduction corrected | Correct CAVE in proper order, never dorsiflex early | Difficult - may need plantar release, casting, or osteotomy |
| Flat-top talus | Excessive dorsiflexion, repeated aggressive manipulation | Gentle manipulation, proper tenotomy timing | Avoid continued dorsiflexion, may need osteotomy later |
| Skin complications | Tight casts, pressure sores, slippage | Proper padding, well-molded casts, weekly changes | Cast removal, local wound care, delay recasting if needed |
| Tibialis anterior weakness post-TATT | Surgical technique, scarring | Careful tendon handling, appropriate rehabilitation | Physiotherapy, usually mild and improves |
| Overcorrection (calcaneus deformity) | Excessive surgical release | Use Ponseti method, avoid extensive release | Difficult to treat - may need posterior ankle block |
Recurrence Timeline
Recurrence typically occurs between 6 months and 4 years of age, corresponding to the period of active bracing. Recurrence after age 5 is rare if proper treatment achieved. Most recurrences are due to bracing non-compliance. First signs: loss of dorsiflexion, returning heel varus, dynamic forefoot supination.
Postoperative Care and Rehabilitation
Post-Treatment Protocol
Final long-leg cast:
- Maximum dorsiflexion (15+ degrees)
- 70 degrees abduction
- Cast remains 3 weeks for tendon healing
- Tendon regenerates in lengthened position
Full-time bracing (23 hours/day):
- Fit FAO immediately upon cast removal
- Remove only for bathing
- Check skin daily for pressure areas
- Proper sock application prevents blisters
Gradual weaning:
- Reduce to 18-20 hours/day
- Allow out of brace for supervised play
- Continue night and nap time wear
- Regular clinic follow-up every 2-3 months
Nighttime bracing:
- 12-14 hours overnight (including naps)
- Continue until age 4-5 years
- Check brace fit as feet grow
- Annual or bi-annual follow-up
Parent Education Points:
- Bracing is the most important factor for success
- Recurrence is preventable with proper compliance
- Signs to watch for: tightness, loss of dorsiflexion, in-toeing
- Calf size difference is permanent (1-2cm smaller)
- Foot size may be 0.5-1.5 sizes smaller on affected side
Outcomes
Clinical Outcomes After Ponseti Treatment
Long-Term Outcomes:
- Ponseti-treated feet have better function, motion, and strength than surgically released feet
- Most patients achieve plantigrade, pain-free, functional feet
- Calf size difference persists (smaller on affected side)
- Foot size difference may persist (0.5-1.5 sizes smaller)
- Full sports participation usually possible
Predictors of Poor Outcome:
- Syndromic clubfoot (arthrogryposis, myelomeningocele)
- Severe initial Pirani score with rigid deformity
- Non-compliance with bracing
- Delayed treatment initiation (after 6 months of age)
- Extensive surgical release
Ponseti vs Surgical Release
Long-term studies show Ponseti-treated feet are stronger, more flexible, and have less pain than surgically released feet. Surgery should be reserved for failed Ponseti treatment only. The "French functional method" (physiotherapy-based) is an alternative but requires more resources and has similar outcomes to Ponseti.
Evidence Base
Ponseti & Smoley - Congenital Club Foot: The Results of Treatment (Classic)
- The foundational long-term series describing manipulation, serial casting and limited surgery (reprinted 2009 as a Classic; originally J Bone Joint Surg Am 1963)
- Reported good or excellent results in the large majority of feet treated with the specific manipulation and casting sequence
- Identified relapse, particularly with inadequate post-correction bracing, as the principal threat to a durable result
- Established that the great majority of feet require percutaneous Achilles tenotomy for residual equinus
Dobbs - Factors Predictive of Outcome After Ponseti Treatment
- Retrospective analysis of 51 infants (86 idiopathic clubfeet) treated with the Ponseti method
- Brace non-compliance was the factor most strongly associated with recurrence (odds ratio 183, p less than 0.00001)
- Lower parental educational level (high-school or less) was also an independent risk factor for recurrence (odds ratio 10.7)
- Initial deformity severity, age at starting treatment and previous treatment did NOT predict recurrence
Haft - Early Recurrence After Ponseti Method (New Zealand)
- Prospective cohort of 51 babies (73 clubfeet) followed for a minimum of two years
- Overall recurrence requiring surgery was 41%, but only 3 of 26 brace-compliant children had a major recurrence
- Compliance with abduction bracing gave the greatest risk reduction for recurrence (odds ratio 0.2, p = 0.009)
- Non-compliant families had roughly a five-fold higher chance of recurrence; severity, ethnicity and cast number did not predict relapse
Corbu - Posteromedial Release vs Ponseti, Long-Term Into Adolescence
- Retrospective comparison of Ponseti (34 feet) versus posteromedial surgical release (31 feet) followed to adolescence
- Excellent or good ICFSG results in 76% of Ponseti feet versus 45% of surgically released feet
- Ponseti was superior for final, functional and radiological scores (all p less than 0.001) and preserved better foot and ankle mobility
- Flat-top talus was less frequent after Ponseti (relative risk 0.49 versus surgery, p = 0.002)
Gray - Tibialis Anterior Tendon Transfer for Recurrent Clubfoot
- Prospective controlled study of 20 children with recurrent (dynamic supination) clubfoot undergoing tibialis anterior tendon transfer
- By three months post-transfer, eversion-to-inversion strength ratio, plantar loading and function/satisfaction were no longer different from non-relapsed controls
- Improvements were maintained at 12 months
- Confirms TATT is indicated for recurrent dynamic supination once the foot is passively correctable
Lampasi - Dimeglio vs Pirani Score Predicting Casts and Tenotomy
- Prospective study of 91 feet (54 patients) scored at presentation with both the Dimeglio and Pirani systems
- Both scores correlated with the number of casts needed (Dimeglio r = 0.73; Pirani r = 0.56)
- Both scores were significantly associated with the need for tenotomy (p less than 0.0001)
- The Dimeglio score showed slightly better accuracy for predicting casts and tenotomy, though not significantly so
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 2-week-old baby boy is referred with bilateral clubfeet diagnosed on prenatal ultrasound. Describe your assessment and management plan."
"A 3-year-old child presents with recurrent clubfoot deformity 2 years after initially successful Ponseti treatment. The parents report they stopped using the brace at 18 months because the child refused to wear it."
"You are performing a percutaneous Achilles tenotomy on a 6-week-old infant with clubfoot. Describe your technique and how you would manage a complication."
MCQ Practice Points
Pirani Score Interpretation
Q: What does a Pirani hindfoot score of 2.5 indicate? A: Moderate-severe hindfoot involvement with at least two of three signs significantly present (posterior crease, empty heel, rigid equinus). This predicts need for percutaneous Achilles tenotomy. A hindfoot score approaching 0 with persistent equinus is the classic indication for tenotomy.
Order of Correction
Q: Why must cavus be corrected before other components in Ponseti method? A: Correcting cavus first (by supinating the forefoot) creates a single lever arm for correction. If cavus is not corrected, the forefoot and hindfoot are misaligned, and attempting abduction will increase midfoot deformity. Supinating the forefoot aligns the 1st ray with the hindfoot, allowing the entire foot to rotate as a unit around the talar head.
Rocker-Bottom Prevention
Q: What causes iatrogenic rocker-bottom deformity in clubfoot treatment? A: Dorsiflexing the foot before adequate abduction is achieved. The talus is fixed in equinus in the ankle mortise. If you dorsiflex without first abducting and derotating the calcaneus, the midfoot breaks dorsally while the talus remains plantarflexed, creating a convex plantar surface (rocker-bottom). This is why equinus is corrected LAST via tenotomy.
Bracing Non-Compliance
Q: A 2-year-old with prior Ponseti treatment presents with returning varus and loss of dorsiflexion. What is the most likely cause? A: Non-compliance with foot abduction orthosis (FAO) bracing. This is responsible for 80% of recurrences. Management includes repeat Ponseti casting and emphasizing bracing importance. For children over 2.5 years with dynamic supination, tibialis anterior transfer should be considered.
Syndromic Clubfoot
Q: What features distinguish syndromic from idiopathic clubfoot? A: Syndromic clubfoot is associated with other congenital anomalies, tends to be more rigid, has higher recurrence rates, and often requires surgical intervention despite initial Ponseti success. Look for: bilateral severe rigid feet, other limb anomalies, facial dysmorphism, joint contractures (arthrogryposis), spine abnormalities (myelomeningocele).
Medicolegal Considerations
Consent Points for Clubfoot Treatment:
- Recurrence risk: 5-10% with proper bracing, 30-40% without
- Calf size difference: Affected side remains smaller (1-2cm)
- Foot size difference: May be 0.5-1.5 sizes smaller
- Need for prolonged bracing: 4-5 years commitment
- Possible need for further procedures: Tenotomy, TATT, other surgery
Documentation Requirements:
- Initial assessment including Pirani score
- Cast number and position achieved at each change
- Tenotomy performed and outcome
- Bracing prescription and compliance documentation
- Evidence of screening for associated conditions (hips, spine)
Bracing Compliance Documentation
Document bracing compliance and any non-compliance at each visit. If recurrence occurs, documentation of counseling about bracing importance protects against litigation. Photograph feet in brace showing proper fit.
Guidelines, Registries & Global Practice
Clubfoot is a worldwide problem, and the Ponseti method is now the agreed first-line standard of care across every health system. The clinically important differences between regions are not in the technique itself but in access, follow-up infrastructure, and how brace compliance is supported - particularly the large share of cases that occur in low- and middle-income countries.
Global Epidemiology
Birth Prevalence and Population Variation
| Parameter | Figure | Note |
|---|---|---|
| Overall birth prevalence | Roughly 1 per 1000 live births | Most widely quoted figure for idiopathic clubfoot in populations of European ancestry |
| Ethnic variation | Lowest in East-Asian populations; highest in Polynesian/Pacific populations | Polynesian rates reported several-fold higher; supports a strong genetic contribution |
| Sex ratio | Approximately 2:1 male predominance | Consistent across populations |
| Laterality | Bilateral in around half of cases | Unilateral feet more often right-sided |
| Idiopathic vs syndromic | Around 80% idiopathic | Syndromic feet (arthrogryposis, myelomeningocele) are stiffer with higher relapse |
| Burden location | The large majority of new cases arise in low- and middle-income countries | Drives the need for scalable, non-specialist-deliverable treatment |
Guidance and Programmes, Side by Side
What Major Bodies Recommend
| Body / Programme | Position on first-line treatment | Emphasis |
|---|---|---|
| AAOS / POSNA (North America) | Ponseti serial casting as initial standard for idiopathic clubfoot | Percutaneous tenotomy for residual equinus; foot abduction orthosis to prevent relapse |
| British / European paediatric orthopaedic practice (BSCOS, EFORT-aligned) | Ponseti method as first-line; reserve extensive surgery for failure | Early referral, structured cast pathways, dedicated clubfoot clinics and brace surveillance |
| WHO / global child-health programmes | Endorse Ponseti as a cost-effective, scalable intervention | Recognise neglected clubfoot as a preventable cause of disability in LMICs |
| Ponseti International Association / GCI / Hope Walks | Train non-specialist health workers to deliver Ponseti at scale | National programmes, brace supply chains, and follow-up registries |
The strength of evidence is consistent: comparative and long-term cohort data place Ponseti above extensive surgical release for function and mobility, and prospective studies repeatedly identify brace non-compliance - not deformity severity - as the dominant driver of relapse.
Registries, Surveillance and Practice Variation
- Birth-defect surveillance, not arthroplasty-style implant registries, is the relevant registry evidence for clubfoot. National and programme registries (for example WHO-linked surveillance and large LMIC programmes) track incidence and treatment coverage; trained midwives can diagnose talipes equinovarus with high positive predictive value where surveillance systems exist.
- High-resource settings: near-universal Ponseti uptake, antenatal ultrasound detection, dedicated clubfoot clinics, and structured brace-compliance monitoring. The main challenge is sustaining bracing through to age 4-5 years.
- Limited-resource settings: the dominant challenge is late presentation (neglected clubfoot) and loss to follow-up. Task-shifting to trained non-specialists, local brace manufacture, and community follow-up are the key adaptations; outcomes approach high-income results when bracing compliance is maintained.
- Universal principle: regardless of setting, the determinants of success are early start, correct CAVE-order casting, timely tenotomy, and relentless brace compliance.
Clinical summary
CAVE Deformity Order
- •Cavus first: supinate forefoot to flatten arch
- •Adductus + Varus: abduct around talar head
- •Equinus last: percutaneous Achilles tenotomy
- •NEVER dorsiflex before abduction - causes rocker-bottom
Ponseti Key Numbers
- •5-7 casts: typical number for initial correction
- •60-70 degrees: target abduction before tenotomy
- •90%: percentage requiring tenotomy
- •3 weeks: final cast duration post-tenotomy
- •4-5 years: bracing duration
FAO Bracing Protocol
- •70 degrees external rotation (60 degrees unilateral)
- •23 hours/day for first 3 months
- •Nighttime only (12 hours) until age 4-5
- •Non-compliance causes 80% of recurrences
Recurrence Management
- •First: repeat Ponseti casting
- •Tenotomy if equinus persists
- •TATT if over 2.5 years with dynamic supination
- •Surgical release reserved for failures only
Pirani Score Components
- •Midfoot (3): curved border, medial crease, talar head
- •Hindfoot (3): posterior crease, empty heel, rigid equinus
- •Total 0-6: higher = more severe
- •Guides cast number and tenotomy timing