Surgical Emergency | Clinical Diagnosis | Fasciotomy Within 6 Hours | Irreversible After 8 Hours
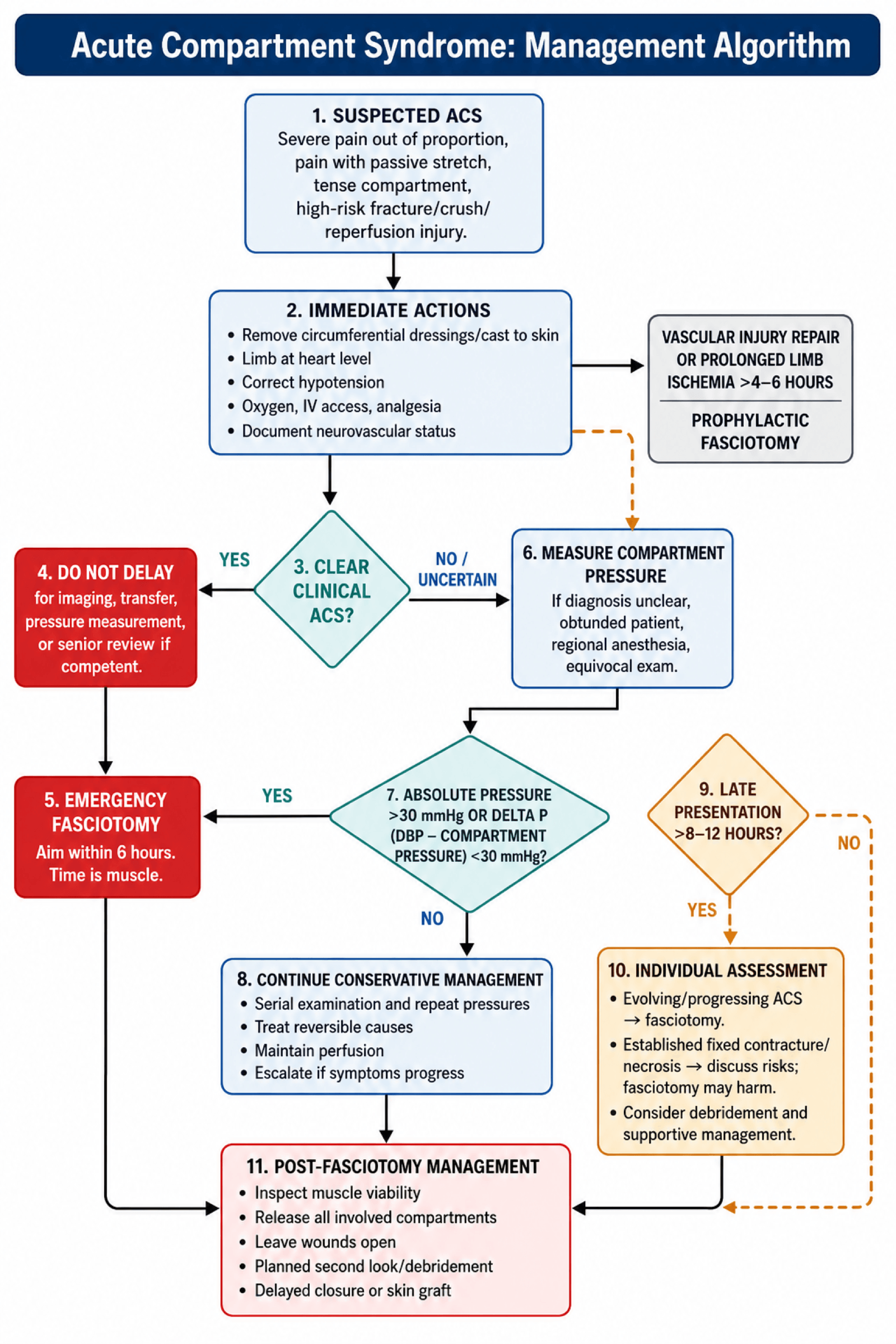
- Clinical diagnosis - do not wait for pressure measurement if clinical suspicion high
- Pain on passive stretch is the earliest and most sensitive clinical sign
- Absolute pressure over 30mmHg or delta P under 30mmHg are indications for fasciotomy
- Fasciotomy within 6 hours gives best outcomes - after 8 hours damage is irreversible
- All compartments must be released - leg has 4, forearm has 3, thigh has 3
- “Tibial fractures are the most common cause (36% of all ACS)
- “Absence of pulse does NOT rule out ACS - ACS occurs at pressures below arterial occlusion
- “Deep posterior compartment (leg) is most commonly missed
- “Volkmann's contracture is the end result of untreated forearm ACS
Clinical Imaging
Imaging Atlas




Do not delay fasciotomy waiting for pressure measurements if clinical suspicion is high. Pain out of proportion to injury and pain on passive stretch are the key early signs. A single normal pressure does not exclude ACS.
Absolute pressure over 30mmHg or Delta P (DBP minus compartment pressure) under 30mmHg indicate fasciotomy. Delta P is more reliable in hypotensive patients. Continuous monitoring more reliable than single measurement.
Fasciotomy within 6 hours gives best outcomes. Irreversible muscle necrosis begins at 8 hours. After 12 hours, 90% of patients have permanent deficits. Delay is the most common cause of litigation.
Release ALL compartments. Leg has 4 compartments (anterior, lateral, superficial posterior, deep posterior). The deep posterior compartment is most commonly missed. Use two-incision technique for complete release.
At a Glance
- Key Information
- Increased pressure within closed fascia causing microvascular compromise
- Key Information
- Tibial shaft fractures (36% of all ACS)
- Key Information
- Fasciotomy within 6 hours for best outcomes; irreversible after 8 hours
- Key Information
- Pain on passive stretch of affected muscles
- Key Information
- Absolute over 30mmHg OR Delta P under 30mmHg
- Key Information
- 4 compartments (anterior, lateral, superficial posterior, deep posterior)
- Key Information
- Deep posterior (most commonly incomplete in fasciotomy)
- Key Information
- Clinical diagnosis - do not delay for pressure if high suspicion
| Clinical Finding | Pressure Reading | Action | Timing |
|---|---|---|---|
| High clinical suspicion | Not measured / unavailable | Immediate fasciotomy | Do not delay for measurement |
| Moderate suspicion | Absolute over 30mmHg or ΔP under 30 | Fasciotomy | Within 1 hour |
| Low-moderate suspicion | Borderline (25-30mmHg) | Serial monitoring | Repeat every 1-2 hours |
| Unconscious/obtunded patient | Any elevation | Low threshold for fasciotomy | Cannot rely on clinical exam |
| Established ACS over 8 hours | Elevated | Consider risks of late fasciotomy | Discuss with patient/family |
6 P'sThe 6 P's of Compartment Syndrome
Hook:Pain and Pressure come first - Paralysis and Pulselessness are too late!
ADSLLeg Compartments - ADSL
Hook:ADSL like internet - need ALL 4 for the leg to work!
VDPForearm Compartments
Hook:VDP - Very Dangerous Pressure in the forearm
CASTCauses of ACS - CAST
Hook:Remove the CAST if compartment syndrome suspected!
Overview and Epidemiology
Acute compartment syndrome (ACS) is a surgical emergency where increased pressure within a closed fascial compartment compromises perfusion, leading to muscle and nerve ischemia. Without timely fasciotomy, irreversible necrosis occurs.
Definition:
- Elevated pressure within a closed osseofascial compartment
- Compromises local blood flow (capillary perfusion pressure approximately 25mmHg)
- Leads to ischemia of muscles and nerves
- Irreversible damage after 6-8 hours of ischemia
ACS occurs when compartment pressure exceeds capillary perfusion pressure (approximately 25mmHg). Arteries remain patent as arterial pressure is higher, so pulses are present until very late. The ischemia is at the microvascular level, not arterial occlusion.
Common causes:
- Fractures (75% of cases) - tibial shaft most common
- Soft tissue injury without fracture
- Arterial injury with ischemia-reperfusion
- Burns (especially circumferential)
- Crush injuries
- Tight casts/dressings (external compression)
- Extravasation of IV fluids
- Prolonged limb compression (drug overdose position)
High-risk scenarios:
- Tibial shaft fractures (especially high-energy)
- Forearm fractures in children (supracondylar)
- Vascular injury with delayed reperfusion
- Polytrauma patients (especially obtunded)
- Anticoagulated patients (compartment hematoma)
Anatomy - Compartments by Region
You MUST know the compartments in each region - a missed compartment leads to incomplete decompression and persistent ACS. The deep posterior compartment of the leg is most commonly missed.
The leg has 4 compartments:
| Compartment | Contents | At-Risk Nerve | Fasciotomy Access |
|---|---|---|---|
| Anterior | Tibialis anterior, EHL, EDL, peroneus tertius | Deep peroneal nerve | Anterolateral incision |
| Lateral | Peroneus longus, peroneus brevis | Superficial peroneal nerve | Anterolateral incision |
| Superficial posterior | Gastrocnemius, soleus, plantaris | Sural nerve | Posteromedial incision |
| Deep posterior | Tibialis posterior, FHL, FDL, popliteus | Tibial nerve, posterior tibial vessels | Posteromedial incision - MOST MISSED |
The deep posterior compartment is separated from superficial posterior by the deep transverse intermuscular septum. It contains tibialis posterior, FHL, FDL. Must be specifically released - most common cause of incomplete fasciotomy.

Pathophysiology
The ischemia cycle:
Fracture, crush, vascular injury, or reperfusion leads to bleeding and edema within closed compartment.
Increased compartment volume within non-compliant fascia causes pressure rise. Capillary perfusion pressure is approximately 25-30mmHg.
Capillaries and venules collapse. Arterial inflow continues briefly, worsening edema. Ischemia begins.
Muscle and nerve ischemia. Reversible if decompressed. Pain on passive stretch occurs.
Muscle necrosis begins. Nerve injury (neuropraxia initially, axonotmesis later). Myoglobin release.
Significant muscle death. Volkmann's contracture develops. Renal failure risk from myoglobinuria.
Systolic arterial pressure (typically over 90mmHg) exceeds compartment pressures, so arterial pulses remain until very late. ACS is a microvascular problem, not arterial occlusion. Never rule out ACS because pulses are present.
Pressure thresholds:
- Normal compartment pressure: under 10mmHg
- Capillary perfusion pressure: approximately 25-30mmHg
- Symptomatic ischemia: usually over 30mmHg absolute
- Delta P (diastolic BP minus compartment pressure): under 30mmHg indicates ischemia
Classification Systems
| Type | Onset | Features | Management |
|---|---|---|---|
| Acute | Minutes to hours | Surgical emergency, follows trauma or ischemia-reperfusion | Emergent fasciotomy |
| Chronic (exertional) | During exercise | Reversible with rest, typically in athletes | Conservative or elective fasciotomy |
| Crush syndrome | Hours post-release | Systemic effects dominant, reperfusion injury | Fasciotomy plus resuscitation |
Matsen's classification divides causes into: Increased content (bleeding, edema, IV extravasation) versus Decreased compartment size (tight casts, closure of fascial defects, MAST trousers). Both mechanisms lead to elevated compartment pressure.
Clinical Presentation and Assessment
ACS is a clinical diagnosis. Do not delay fasciotomy waiting for pressure measurements if clinical suspicion is high. Serial reassessment is essential in at-risk patients.
History:
- Mechanism of injury
- Time since injury (critical for prognosis)
- Pain character - out of proportion to injury
- Increasing analgesia requirements
- Numbness or weakness developing
The 6 P's - Clinical Signs:
| Sign | Timing | Mechanism | Reliability |
|---|---|---|---|
| Pain out of proportion | EARLY | Muscle ischemia | Most sensitive early sign |
| Pain on passive stretch | EARLY | Muscle ischemia | Most specific early sign |
| Pressure (tense compartment) | EARLY | Increased volume | Variable - subjective |
| Paresthesia | INTERMEDIATE | Nerve ischemia | Indicates progression |
| Paralysis | LATE | Muscle necrosis | Poor prognosis if present |
| Pallor/Pulselessness | VERY LATE | Complete vascular compromise | Do not wait for these |
Pain on passive stretch - location specific:
- Anterior leg: Pain on passive plantar flexion of toes/ankle
- Deep posterior leg: Pain on passive dorsiflexion of toes
- Volar forearm: Pain on passive extension of fingers
- Dorsal forearm: Pain on passive flexion of fingers
In unconscious, intubated, or heavily sedated patients, you cannot rely on pain assessment. Have a very low threshold for pressure measurement and fasciotomy. These patients are at highest risk of missed ACS.
Special populations at risk:
- Polytrauma patients (often sedated/ventilated)
- Regional anesthesia (masks pain)
- Pediatric patients (cannot articulate)
- Drug intoxication
- Neurological injury
Differential diagnosis:
| Condition | Distinguishing Features | Key Test | Pitfall |
|---|---|---|---|
| Acute compartment syndrome | Pain out of proportion, pain on passive stretch, tense compartment, pulses usually present | Delta P under 30mmHg / clinical | Waiting for pulselessness or pallor |
| Acute arterial occlusion / ischaemia | Cold, pulseless, pale limb; pain at rest; classic 6 P's of ischaemia | Doppler / CT angiography; ABPI | ACS can co-exist after reperfusion - both may be present |
| Deep vein thrombosis | Diffuse swelling, warmth, less pain on passive stretch, no tense fascial compartment | Duplex ultrasound | Calf swelling attributed to DVT delays ACS diagnosis |
| Cellulitis / necrotising fasciitis | Erythema, fever, systemic sepsis; crepitus and disproportionate pain in necrotising infection | Bloods, LRINEC, surgical exploration | Necrotising fasciitis also a surgical emergency - do not miss |
| Fracture / soft-tissue pain | Pain proportionate to injury, settles with analgesia and splintage, compartments soft | Serial clinical review | Rising analgesia requirement should prompt ACS reassessment |
| Peripheral nerve injury | Sensory/motor deficit in a single nerve territory, no compartment tension | Clinical mapping; nerve studies (late) | Isolated paraesthesia attributed to nerve injury masks early ACS |
Investigations and Pressure Measurement
Most commonly used in clinical practice.
Technique:
- Sterilize skin
- Insert needle into compartment at 90 degrees
- Inject small amount of saline
- Read pressure on digital display
- Measure at multiple points (within 5cm of fracture site)
Tips: Highest pressure is usually within 5cm of fracture. Measure all compartments and consider serial measurements in borderline cases.
Threshold values:
| Measurement | Threshold | Notes |
|---|---|---|
| Absolute pressure | Over 30mmHg | Traditional threshold |
| Delta P (DBP minus compartment) | Under 30mmHg | More reliable in hypotension |
| Mean arterial pressure minus compartment | Under 40mmHg | Alternative measure |
Delta P (diastolic pressure minus compartment pressure) under 30mmHg is more reliable than absolute pressure, especially in hypotensive trauma patients. A patient with DBP of 50mmHg and compartment pressure of 25mmHg has delta P of 25 - this indicates ACS even though absolute pressure is under 30.
Other investigations:
- Bloods: CK (elevated with muscle damage), renal function, coagulation
- Urine: Myoglobinuria (dark urine)
- No role for imaging in acute diagnosis - do not delay for CT/MRI
Management
While preparing for fasciotomy:
- Remove all circumferential dressings - split casts to skin
- Position limb at heart level - elevation reduces arterial inflow
- Correct hypotension - improves perfusion pressure
- Supplemental oxygen
- IV access - prepare for surgery
- Analgesia - but don't mask ongoing symptoms
- Document neurovascular status - before and after any intervention
Split cast completely to skin including padding. Studies show splitting cast and padding decreases compartment pressure by 30-65%. Bivalving alone is insufficient.
Surgical Technique - Fasciotomy
Gold standard for leg compartment syndrome.
Anterolateral Incision
Position: Supine, leg slightly externally rotated
Incision:
- Longitudinal incision from fibular head to lateral malleolus
- 2cm anterior to fibula
- Length: essentially entire leg (15-20cm minimum)
Release:
- Incise skin and subcutaneous tissue
- Identify fascia of anterior compartment
- Release anterior compartment - full length
- Identify intermuscular septum
- Release lateral compartment posterior to septum
The superficial peroneal nerve pierces the fascia approximately 10-12cm proximal to lateral malleolus. Identify and protect it during lateral compartment release.
Posteromedial Incision
Incision:
- Longitudinal incision 2cm posterior to medial tibial border
- Avoid saphenous vein and nerve anteriorly
- Length: match anterolateral incision
Release sequence: (1) Incise skin and subcutaneous tissue, (2) Release superficial posterior compartment fascia, (3) Identify and divide deep transverse intermuscular septum, (4) Release deep posterior compartment - THIS IS CRITICAL, (5) Detach soleus from tibia if needed for access.
The deep posterior compartment lies beneath the deep transverse intermuscular septum. It must be specifically identified and released. Failure to release this compartment is the most common cause of incomplete fasciotomy.
Complications
| Complication | Cause | Prevention/Management |
|---|---|---|
| Missed ACS / incomplete release | Delayed diagnosis, missed compartment | High index of suspicion, release all compartments |
| Volkmann's contracture | Untreated forearm ACS | Timely fasciotomy; reconstruction if established |
| Myoglobinuric renal failure | Rhabdomyolysis | Aggressive IV fluids, monitor CK/urine |
| Nerve injury | Direct injury or ischemic | Careful technique; neuropraxia may recover |
| Chronic pain | Muscle necrosis, scarring | Physiotherapy, pain management |
| Wound complications | Large open wound | VAC therapy, staged closure, skin graft |
| Weakness | Muscle necrosis | Physiotherapy; tendon transfers if needed |
| Amputation | Established necrosis, sepsis | Rare - occurs with massive tissue loss |
Volkmann's ischemic contracture:
- End result of untreated volar forearm ACS
- Flexed wrist, extended MCPs, flexed IPs
- Muscle fibrosis and contracture
- Treatment: reconstruction (muscle slide, tendon lengthening, free muscle transfer)

Rhabdomyolysis causes myoglobinuria (dark urine) and can lead to acute kidney injury. Manage with: aggressive IV fluids (target urine output over 1ml/kg/hr), alkalinize urine (sodium bicarbonate), monitor renal function and electrolytes (hyperkalaemia risk).
Postoperative Care
- Moist dressings to fasciotomy wounds
- Splint limb in functional position
- Elevate but not above heart (balance perfusion)
- Monitor neurovascular status
- IV fluids for renal protection
- Monitor CK, renal function, urine output
- Return to OR for wound inspection
- Debride any necrotic tissue
- Assess for delayed primary closure
- VAC/NPWT if wound not ready for closure
- Plan for skin grafting if needed
- Serial debridements if ongoing necrosis
- Staged closure or skin grafting
- Physiotherapy begins when wound stable
- Active and passive ROM
- Strengthening as tolerated
- May need tendon surgery for contractures
- Assess for permanent deficits
Monitoring parameters:
- CK levels (peak at 24-72 hours)
- Urine output and color
- Renal function (creatinine)
- Potassium (hyperkalaemia from cell lysis)
- Wound appearance
Outcomes and Prognosis
Prognostic factors:
- Time to fasciotomy (most important)
- Completeness of fasciotomy
- Underlying injury severity
- Patient factors (age, comorbidities)
Outcomes by timing:
- Expected Outcome
- Good recovery expected
- Expected Outcome
- Variable - some permanent deficits
- Expected Outcome
- Likely permanent deficits
- Expected Outcome
- 90% have permanent deficits
Missed or delayed compartment syndrome is a common cause of medical litigation in orthopaedics. Documentation of serial clinical assessments, pressure measurements, and timing of intervention is essential. Early involvement of senior colleagues is prudent.
Evidence Base
McQueen & Court-Brown - Delta P Threshold for Decompression
- Prospective study of 116 tibial diaphyseal fractures with 24-hour continuous anterior compartment monitoring
- Using a differential (delta) pressure threshold of under 30mmHg led to NO missed cases of acute compartment syndrome
- An absolute threshold of 30mmHg would have led to fasciotomy in 43% of patients; 40mmHg in 23% - most unnecessary
- Only 3 patients (2.6%) developed true acute compartment syndrome
McQueen, Christie & Court-Brown - Continuous Monitoring & Outcomes
- 25 tibial diaphyseal fractures complicated by acute compartment syndrome (13 monitored, 12 not)
- Mean delay to fasciotomy 16 hours (monitored) versus 32 hours (non-monitored), p under 0.05
- No sequelae in the monitored group versus definite weakness/contractures in 10 of 11 survivors not monitored, p under 0.01
- Significantly delayed tibial union in the non-monitored group
McQueen, Gaston & Court-Brown - Who Is at Risk?
- 164 patients with acute compartment syndrome over 8 years - the defining epidemiological series
- An associated fracture was present in 69%; about half of these were tibial shaft fractures (≈36% of all ACS)
- Most patients were young men, typically under 35 years; forearm ACS most often accompanied distal radius fractures
- Soft-tissue injury without fracture was the second commonest cause; ~10% had a bleeding disorder or were anticoagulated
McQueen et al - Predictors of ACS After Tibial Fracture
- Retrospective cohort of 1,388 tibial diaphyseal fractures; 160 (11.5%) developed acute compartment syndrome
- Youth was the strongest independent predictor (highest prevalence ages 12-29)
- Blue-collar occupation and implant type also predictive on adjusted analysis
- Male gender and sporting injury associated on univariate analysis
Whitesides et al - Tissue Pressure as Determinant for Fasciotomy
- Foundational description linking compartment pressure to diastolic blood pressure rather than an absolute number
- Inadequate perfusion when tissue pressure rises to within 10-30mmHg of diastolic BP
- No effective perfusion once tissue pressure equals or exceeds diastolic BP - even with palpable distal pulses
- Introduced the perfusion-pressure concept underpinning modern delta P thresholds
Mubarak, Owen et al - Wick Catheter Diagnosis & 30mmHg Threshold
- 65 compartments in 27 patients clinically suspected of ACS, measured by wick catheter
- Normal compartment pressure 0-8mmHg; 30mmHg used as the indication for decompressive fasciotomy
- No sequelae in 16 patients whose pressures stayed under 30mmHg and in whom fasciotomy was withheld
- Established the historical absolute 30mmHg threshold and the role of intra-operative monitoring of decompression
Shaikh et al - Acute Compartment Syndrome of the Upper Extremity
- Contemporary review of upper-limb ACS - forearm most common site, but arm and hand also affected
- Most cases follow trauma; non-traumatic causes include prolonged decubitus positioning, bleeding disorders and reperfusion injury
- Emergent fasciotomy is the cornerstone; delay risks myonecrosis, Volkmann's contracture and limb dysfunction
- Reviews controversies in delayed/missed presentation and advances in diagnosis
Lin et al - Risk Factors for Poor Outcome in Lower-Leg ACS
- Retrospective case-control study of 103 lower-leg ACS cases (44 poor, 59 good outcome)
- Associated arterial injury was an independent risk factor for poor outcome (OR 66.2)
- Lower haemoglobin associated with worse outcomes; open injury and high CK also significant on bivariate analysis
- Timing of fasciotomy was NOT independently associated with outcome in this cohort
Rothenberg et al - Delayed Fasciotomy & Amputation in Acute Limb Ischaemia
- 138 lower-extremity revascularisations for acute limb ischaemia; 42 (30.4%) underwent fasciotomy
- Delayed (rather than prophylactic) fasciotomy was associated with major amputation in 50% versus 5.9% at 30 days, p=0.002
- Higher Rutherford ischaemia class predicted need for fasciotomy
- Supports a liberal approach to prophylactic 4-compartment fasciotomy at revascularisation
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man presents 6 hours after a motorcycle accident with a closed tibial shaft fracture. His leg is in a plaster backslab. He is requiring increasing analgesia and describes severe pain in his leg. On examination, his toes are pink with sensation present, but he has pain on passive dorsiflexion of his great toe. What is your assessment and management?”
“You are called to ICU about a 45-year-old intubated patient 18 hours post-polytrauma with bilateral femur fractures, now fixed with IM nails. The ICU nurse is concerned the left leg looks swollen and tense. The patient cannot be assessed clinically. How do you approach this?”
“A 7-year-old boy presents 24 hours after a supracondylar humerus fracture was pinned at another hospital. He has severe pain, a tense forearm, cannot extend his fingers actively, and has decreased sensation in the median nerve distribution. The referring hospital did not perform fasciotomy. How do you manage this?”
“You are asked to see a patient in recovery who just had a popliteal artery repair after 5 hours of warm ischemia from a knee dislocation. The vascular surgeon asks if you want to do a prophylactic fasciotomy. What is your response?”
MCQ Practice Points
Q: Why are peripheral pulses typically present in acute compartment syndrome? A: ACS is a microvascular problem. Compartment pressures (over 30mmHg) exceed capillary perfusion pressure (approximately 25mmHg) but remain below systolic arterial pressure (typically over 90mmHg). Arterial inflow continues, actually worsening edema. Pulselessness is a very late sign.
Q: Which compartment is most commonly missed during leg fasciotomy? A: The deep posterior compartment, which contains tibialis posterior, FHL, and FDL. It is separated from the superficial posterior by the deep transverse intermuscular septum, which must be specifically divided. Accessed via posteromedial incision.
Q: A trauma patient has BP 80/50 and compartment pressure of 28mmHg. Does this require fasciotomy? A: Yes. The delta P (DBP minus compartment pressure) = 50 - 28 = 22mmHg, which is under the 30mmHg threshold. Delta P is more reliable than absolute pressure in hypotensive patients. Absolute pressure may look acceptable but perfusion is inadequate.
Q: What is the expected outcome if fasciotomy is performed at 12 hours? A: Poor outcome expected. Studies show fasciotomy under 6 hours gives normal muscle function. At 6-12 hours outcomes are variable. Beyond 12 hours, 90% have permanent neurological deficits. Time is muscle.
Q: What additional release must always be performed with forearm fasciotomy? A: The carpal tunnel must always be released. The median nerve passes through this confined space and will be compressed if not released. Failure to release carpal tunnel is a cause of ongoing median nerve symptoms.
Q: What is the earliest and most reliable clinical sign of compartment syndrome? A: Pain on passive stretch of the muscles in the affected compartment. For anterior leg compartment: pain on passive plantar flexion. For deep posterior: pain on passive toe dorsiflexion. For volar forearm: pain on passive finger extension.
Guidelines, Registries & Global Practice
Global epidemiology:
- Figure
- ~11.5% (160 of 1,388)
- Source
- McQueen et al 2015, J Orthop Trauma (PMID 25882967)
- Figure
- 69%; ~half tibial shaft (≈36% of all ACS)
- Source
- McQueen, Gaston, Court-Brown 2000, JBJS Br (PMID 10755426)
- Figure
- Youth (peak ages 12-29); male predominance
- Source
- McQueen et al 2015 (PMID 25882967)
- Figure
- 2.6% of monitored tibial fractures
- Source
- McQueen, Court-Brown 1996, JBJS Br (PMID 8898137)
- Figure
- Soft-tissue injury without fracture
- Source
- McQueen, Gaston, Court-Brown 2000 (PMID 10755426)
ACS is a worldwide trauma problem driven by high-energy mechanisms (road traffic, falls, sport, crush and industrial injury). Distribution shifts with regional injury patterns and the time-to-presentation differs sharply between well-resourced trauma systems and rural or limited-resource settings, where delayed transfer worsens outcomes.
Major guidance, side by side:
| Body (region) | Key recommendation | Diagnostic emphasis | Evidence level |
|---|---|---|---|
| BOA / BOAST (UK) | Emergency fasciotomy with documented time targets; hourly observation of at-risk limbs; escalate without delay | Primarily clinical (escalating analgesia, pain on passive stretch); pressure monitoring adjunctive | Consensus / expert (Grade D-equiv.) |
| AAOS / AO Foundation (US / international) | Clinical diagnosis paramount; delta P under 30mmHg triggers fasciotomy; continuous monitoring for obtunded/unreliable patients | Clinical + delta P; serial or continuous measurement when exam unreliable | Level II-III evidence-informed |
| EFORT / European consensus | Two-incision four-compartment leg release as standard; carpal tunnel release mandatory with forearm fasciotomy | Combined clinical and pressure; emphasis on completeness of release | Consensus |
| Vascular societies (limb ischaemia) | Liberal prophylactic fasciotomy at revascularisation after prolonged warm ischaemia (over ~4-6h) | Anticipatory, not reactive | Level III (PMID 31034949) |
All major bodies agree on the core principles: ACS is a clinical diagnosis, fasciotomy must not be delayed, delta P under 30mmHg is the most defensible pressure threshold, continuous monitoring is reserved for patients who cannot be examined, and all compartments must be released. Differences are largely of emphasis (how heavily to rely on pressure measurement) rather than substance.
Registry & population evidence:
There is no dedicated compartment-syndrome registry; the evidence base is built on prospective and cohort series (chiefly the Edinburgh series - PMIDs 8898137, 8898136, 10755426). National trauma registries (e.g. the UK TARN and equivalents) capture ACS as a complication of long-bone trauma and consistently identify young men with tibial shaft fractures as the highest-risk cohort, mirroring the published series.
Global practice variation:
- Continuous pressure monitoring (Stryker/arterial transducer) is widely available in high-resource trauma centres but scarce elsewhere
- In limited-resource settings, diagnosis is necessarily clinical and the threshold to operate is even lower
- Delayed transfer is a key driver of poor outcomes in rural/remote systems worldwide
- Do NOT delay fasciotomy for transfer - decompress where ACS is diagnosed, then transfer
- Release all compartments completely (deep posterior most missed in the leg)
- Document serial neurovascular assessments with times - the single most protective medicolegal step
Missed or delayed compartment syndrome is among the most frequent and costly sources of orthopaedic litigation in every jurisdiction studied. Protective practice is identical everywhere: a low diagnostic threshold, timed serial assessments, prompt decompression and early senior involvement.
PRESSURE THRESHOLDS
- Absolute pressure over 30mmHg = fasciotomy
- Delta P (DBP minus compartment) under 30mmHg = fasciotomy
- Delta P more reliable in hypotensive patients
- Do NOT wait for pressure if clinical diagnosis clear
TIMING
- Under 6 hours: best outcomes (normal function)
- 6-8 hours: variable outcomes
- Over 8 hours: irreversible damage beginning
- Over 12 hours: 90% permanent deficits
CLINICAL SIGNS
- EARLY: Pain out of proportion, pain on passive stretch
- EARLY: Tense compartment on palpation
- INTERMEDIATE: Paresthesia (nerve ischemia)
- LATE: Paralysis, pallor, pulselessness - TOO LATE
LEG COMPARTMENTS (4)
- Anterior: TA, EHL, EDL, deep peroneal nerve
- Lateral: peroneus longus/brevis, superficial peroneal
- Superficial posterior: gastroc, soleus
- Deep posterior: TP, FHL, FDL - MOST MISSED
FASCIOTOMY TECHNIQUE (LEG)
- Two-incision technique for complete release
- Anterolateral: anterior + lateral compartments
- Posteromedial: superficial + deep posterior
- MUST divide deep transverse septum for deep posterior
MEDICOLEGAL
- Common cause of orthopaedic litigation
- Document serial assessments with times
- Document decision-making rationale
- Early senior involvement is protective