Irreducible Dorsal Dislocation | Kaplan Lesion | Volar Plate Interposition
- Index MCP is most common site for complex dorsal dislocation
- Volar plate and sesamoids interpose between metacarpal head and proximal phalanx base
- Skin dimple at proximal palmar crease is pathognomonic for complex injury
- Traction alone tightens the noose around the metacarpal neck and fails
- Open reduction via volar approach allows direct volar plate release but risks neurovascular structures
- “Always examine for skin dimple before attempting reduction
- “Attempt closed reduction only once under adequate anaesthesia
- “Dorsal approach splits the volar plate or uses transverse capsulotomy
- “Post-reduction stability determines early motion versus immobilisation
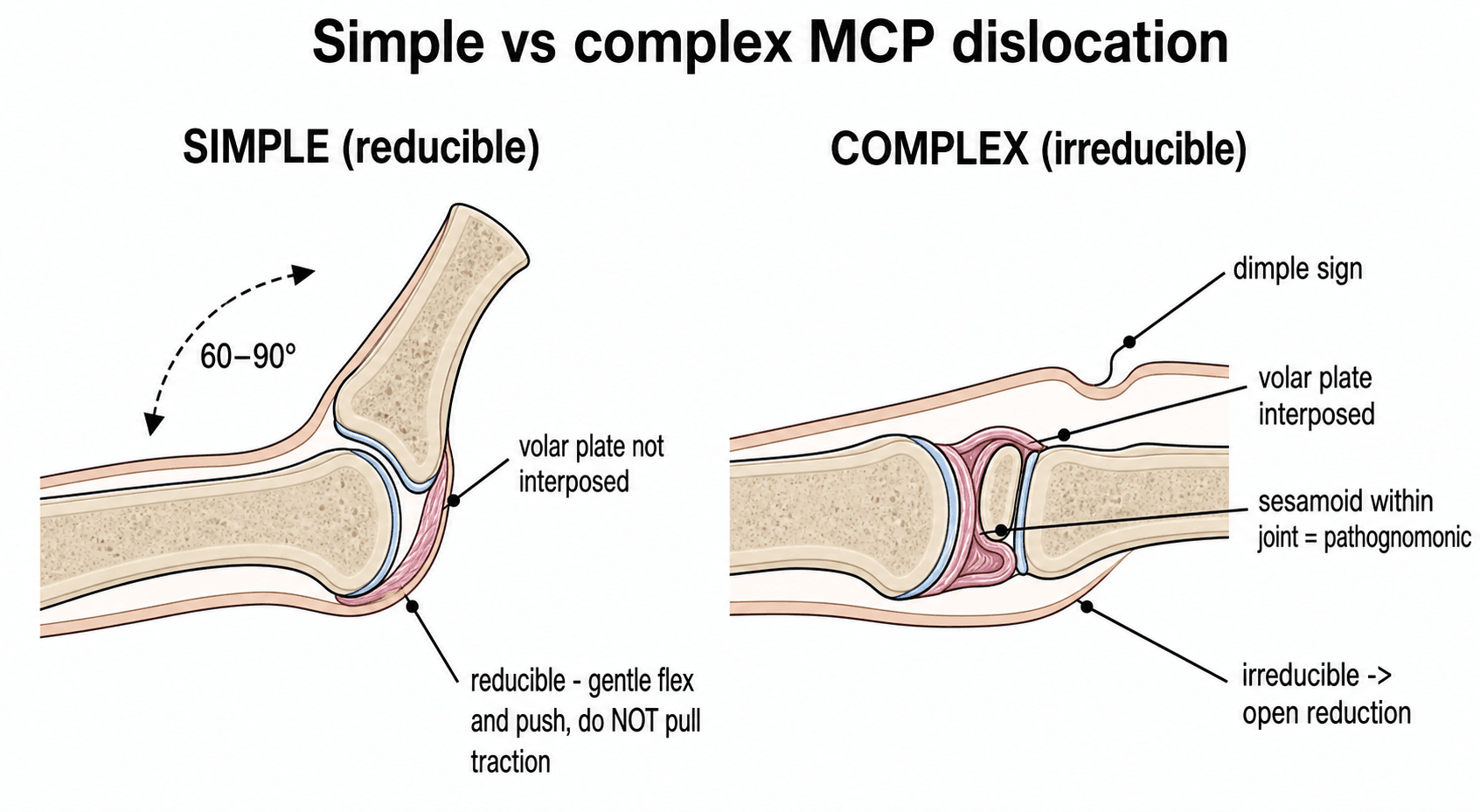
Skin dimple at the proximal palmar crease indicates volar plate interposition. This is a reliable marker that closed reduction will fail and open reduction is required.
Noose effect: Traction tightens the volar plate, flexor tendons and lumbricals around the metacarpal neck, locking the proximal phalanx in hyperextension. Repeated forceful traction worsens interposition.
Classic complex dislocation described by Kaplan: metacarpal head buttonholes through the volar structures with volar plate, sesamoids and flexor sheath acting as the irreducible block.
Volar approach preferred for direct visualisation of the interposed volar plate. Dorsal approach is an alternative when surgeon experience favours it and allows transverse division of the volar plate.
- Diagnosis
- Irreducible on gentle traction attempt
- Treatment
- Urgent open reduction (volar preferred)
- Key Pearl
- Do not repeat forceful closed attempts
- Diagnosis
- Reduces easily with traction and flexion
- Treatment
- Closed reduction, 3 weeks extension block splint
- Key Pearl
- Simple dislocation has excellent prognosis
- Diagnosis
- Possible radial collateral ligament interposition
- Treatment
- Dorsal approach for reduction
- Key Pearl
- Always confirm stability after reduction
VOLARKaplan Lesion Components
Hook:VOLAR structures create the Kaplan lesion - remember the anatomy to plan your approach!
V-DORSALSurgical Approach Choice
Hook:V-DORSAL guides the decision between volar visualisation and dorsal simplicity!
Overview and Epidemiology
Complex dorsal metacarpophalangeal dislocations are true orthopaedic emergencies in the hand. The index finger is involved in over 50 percent of cases. Misdiagnosis as a simple dislocation leads to repeated failed reduction attempts, cartilage damage, and ultimately open reduction that could have been planned from the outset. Recognition of the pathognomonic skin dimple allows immediate preparation for surgery and avoids iatrogenic injury from forceful traction.
- Hyperextension force: Fall on outstretched hand with MCP hyperextended
- Direct blow: Dorsal force driving proximal phalanx into hyperextension
- Sports injury: Ball sports, gymnastics, martial arts
- High-energy trauma: Road traffic accidents with associated fractures
- Irreducible without surgery: Volar plate interposition blocks closed reduction
- Neurovascular risk: Radial digital nerve stretched over metacarpal head
- Joint surface damage: Prolonged dislocation abrades articular cartilage
- Stiffness and pain: Delayed treatment leads to permanent loss of motion
Volar Plate Anatomy and the Mechanism of Interposition
The whole pathology turns on the anatomy of the volar plate, so it is worth setting out explicitly. The volar plate is a thick fibrocartilaginous structure on the palmar surface of the MCP joint with two very different attachments, and it is this asymmetry that explains why a hyperextension force makes it irreducible.
- Character
- Firm, fibrocartilaginous, strong
- Behaviour in hyperextension
- Stays attached to the phalanx and is dragged with it
- Character
- Thin, membranous, weak (the critical zone)
- Behaviour in hyperextension
- Avulses or ruptures here first
- Character
- Embedded within the volar plate substance
- Behaviour in hyperextension
- Add a bony wedge to the interposed block
In a dorsal dislocation the volar plate tears at its weak proximal (metacarpal) origin while remaining firmly attached distally to the proximal phalanx base. As the phalanx displaces dorsally the freed volar plate is carried with it and flips to lie dorsal to the metacarpal head, buttonholed between the metacarpal head and the phalangeal base. The deep transverse metacarpal ligament tethers it to its neighbours, and with the lumbrical on the radial side and the flexor tendons on the ulnar side it completes the constricting noose around the metacarpal neck.
The volar plate's strong distal and weak proximal attachments mean hyperextension avulses it from the metacarpal, not the phalanx. Because it stays tethered to the phalanx and flips over the metacarpal head, it becomes the irreducible interposed block - the anatomical basis of the simple-versus-complex distinction.
Pathophysiology
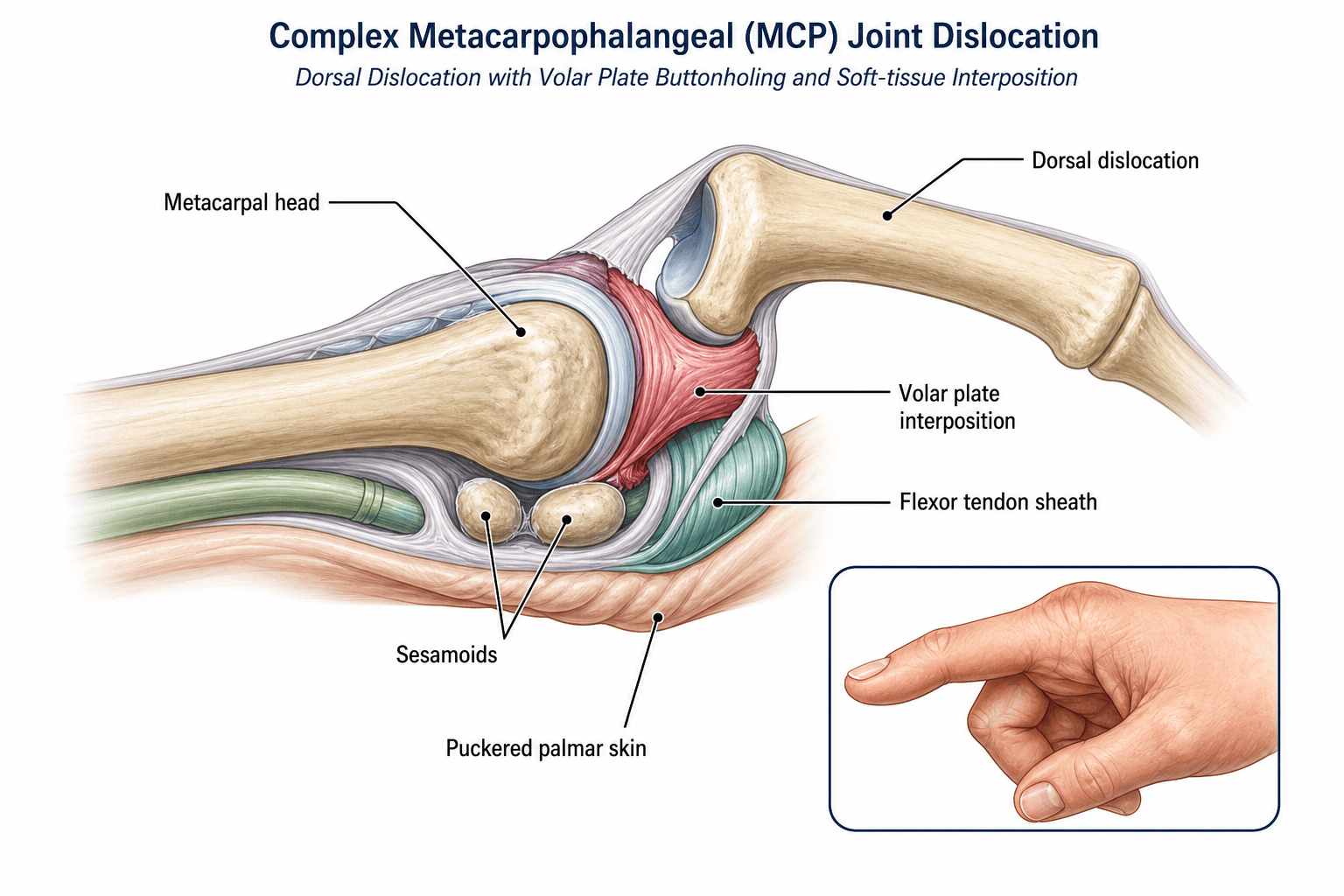
The metacarpal head is cam-shaped with a wider dorsal articular surface. In hyperextension the proximal phalanx base rides over the metacarpal head. The volar plate, which is fibrocartilaginous and contains the sesamoids in the index and middle fingers, folds into the joint space. The flexor tendons, lumbricals and deep transverse metacarpal ligament form a constricting noose around the metacarpal neck. This combination prevents any amount of traction or manipulation from achieving reduction.
- Role in Block
- Primary interposed structure
- Anatomic Location
- Folds between metacarpal head and phalanx base
- Release Method
- Longitudinal or transverse division
- Role in Block
- Bony component of volar plate
- Anatomic Location
- Embedded in volar plate substance
- Release Method
- Divided with volar plate or excised if fractured
- Role in Block
- Form constricting noose
- Anatomic Location
- Ulnar and radial to metacarpal neck
- Release Method
- A1 pulley release if required
- Role in Block
- Radial side interposition
- Anatomic Location
- Between metacarpal head and volar plate
- Release Method
- Gentle retraction or partial release
Traction increases tension on the volar structures already encircling the metacarpal neck. The proximal phalanx remains locked in hyperextension. Forceful or repeated attempts cause further cartilage abrasion and soft-tissue swelling, converting a surgical case into a more difficult one.
The radial digital nerve is stretched over the prominent metacarpal head in index finger dislocations. The ulnar digital nerve is less commonly at risk. Both must be identified and protected during any volar approach. The radial collateral ligament is frequently torn and should be repaired after reduction.
Classification and Types
Classification by Digit Involved
- Frequency
- Most common (over 50 percent)
- Anatomic Features
- Radial sesamoid present, narrow web space
- Surgical Notes
- Volar approach preferred, protect radial nerve
- Frequency
- Second most common
- Anatomic Features
- Two sesamoids, wider head
- Surgical Notes
- Similar volar plate interposition pattern
- Frequency
- Less common
- Anatomic Features
- No radial sesamoid in little finger
- Surgical Notes
- May reduce more easily, check for associated injury
The index finger predominance relates to its position at the radial border and the presence of a radial sesamoid that contributes to the bony block.
Clinical Assessment
- Mechanism: Hyperextension injury, fall onto outstretched hand
- Timing: Acute presentation versus delayed or missed injury
- Previous attempts: Number and force of closed reduction attempts
- Associated injuries: Other hand trauma, open wounds, nerve symptoms
- Inspect: Hyperextended MCP posture, skin dimple at proximal palmar crease
- Palpate: Metacarpal head prominence in palm, tender volar structures
- Neurovascular: Test radial and ulnar digital nerves, capillary refill
- Attempt reduction: Single gentle attempt only under digital block or sedation
Technique: Examine the palm with the MCP in maximal hyperextension. A transverse or oblique skin dimple at the proximal palmar crease directly over the metacarpal head indicates that the volar plate has buttonholed and is interposed.
Interpretation: Presence of the dimple = complex irreducible dislocation. Absence does not completely exclude complexity, but makes simple dislocation more likely.
Key point: Document the dimple before any reduction attempt. Its presence changes management from attempted closed reduction to planned open reduction.
- Posture
- MCP hyperextension, PIP flexed
- Discriminating Finding
- Skin dimple, irreducible on traction
- Key Test / Imaging
- Clinical diagnosis, X-ray confirms direction
- Posture
- MCP hyperextension, reducible
- Discriminating Finding
- No skin dimple, reduces with traction-flexion
- Key Test / Imaging
- Post-reduction X-ray, assess stability
- Posture
- MCP flexed, proximal phalanx volar
- Discriminating Finding
- Extensor interposition, rare
- Key Test / Imaging
- Dorsal approach usually required
- Posture
- PIP flexed, MCP neutral
- Discriminating Finding
- History of triggering, no trauma
- Key Test / Imaging
- A1 pulley injection trial
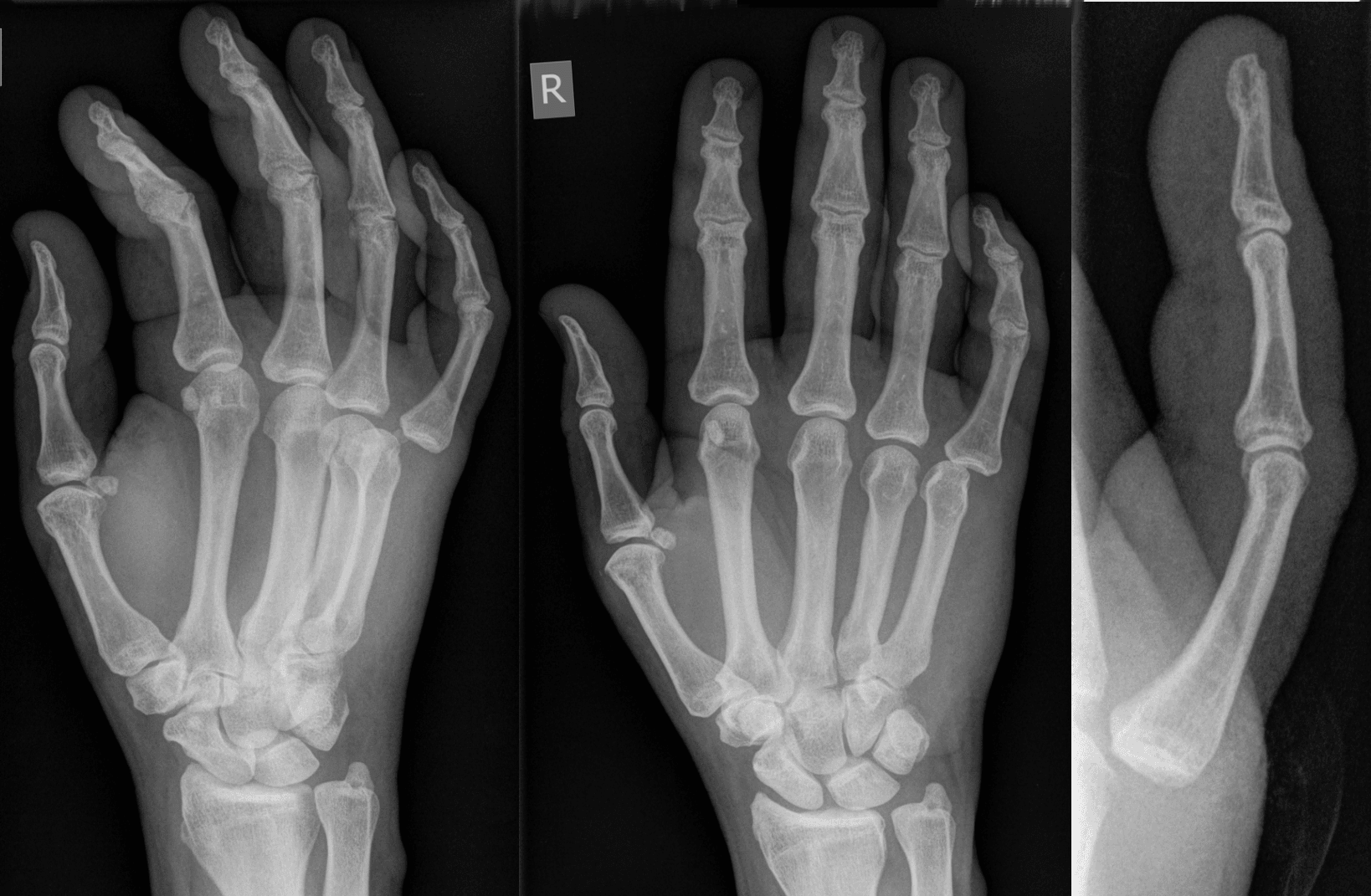
Always obtain orthogonal radiographs before and after any reduction attempt. Associated injuries include metacarpal head fracture, proximal phalanx base fracture, collateral ligament avulsion, and sesamoid fracture. These change the post-reduction protocol and may require internal fixation.
Investigations
Imaging Protocol
Views: PA, true lateral, and oblique of the affected ray
Look for: Direction of dislocation, associated fractures of metacarpal head or proximal phalanx base, sesamoid displacement, joint incongruity
Clinical correlation: The lateral view confirms dorsal versus volar displacement and guides approach planning
Indication: Intra-articular fracture, comminuted metacarpal head, or to assess sesamoid integrity
Threshold: Fragments involving greater than 20 percent of articular surface or with greater than 2 mm step-off warrant ORIF consideration
Pre-op planning: Helps decide between volar plate repair versus excision of comminuted fragments
Indication: Delayed presentation with fibrosis, to assess cartilage status and volar plate integrity
Findings: Interposed volar plate scarring, chondral loss, possible osteochondral defects
Surgical planning: Determines whether joint salvage or arthroplasty is more appropriate
X-rays are essential to confirm the diagnosis and exclude fracture, but the decision for open reduction is clinical based on the skin dimple and failed closed reduction attempt. Do not delay surgical exploration waiting for advanced imaging in an acute irreducible dislocation.
Closed Reduction Technique: One Gentle Attempt, Push Not Pull
A single gentle closed reduction attempt is appropriate for an acute dorsal MCP dislocation before complexity is confirmed - it is curative for a simple dislocation or subluxation and does no harm when done correctly. If a skin dimple is present, or this one gentle attempt fails, proceed to open reduction and do not repeat. The technique matters because the common instinct - longitudinal traction - is exactly what locks a complex injury.
- Do
- Wrist block or sedation; flex the wrist and IP joints to slacken the long flexors
- Avoid
- Manipulating an awake, guarding hand
- Do
- Accentuate MCP hyperextension first, then push the base of the proximal phalanx distally and volarly to roll it over the metacarpal head into flexion
- Avoid
- Longitudinal traction, which tightens the volar plate, flexor and lumbrical noose
- Do
- One gentle attempt only, then reassess
- Avoid
- Repeated forceful attempts that abrade cartilage and worsen interposition
- Do
- Confirm concentric reduction on radiographs, test stability, extension-block splint
- Avoid
- Discharge without a post-reduction film or stability check
The key manoeuvre is to keep the phalangeal base in contact with the metacarpal head and push it distally over the head with the wrist flexed - not to pull along the axis of the finger. Longitudinal traction tightens the noose around the metacarpal neck and can convert a reducible subluxation into an entrapped complex dislocation.
NOOSEReduction Failure Reasons
Hook:The NOOSE around the metacarpal neck explains why traction fails every time!
Management Algorithm
Acute Complex Dorsal Dislocation (Index or Middle Finger)
Goal: Achieve concentric reduction with minimal articular damage and restore stable motion
Surgical Protocol
Timing: Within 24 hours if possible, before swelling peaks Consent: Risk of stiffness, nerve injury, possible need for collateral repair, infection Equipment: Hand table, fluoroscopy, fine rongeurs, 3-0 or 4-0 nonabsorbable suture
Incision: Zigzag or Brunner incision centred over MCP, extending proximally and distally as needed Identify and protect: Radial and ulnar digital neurovascular bundles (radial nerve most at risk) Expose volar plate: Divide A1 pulley if needed, identify interposed volar plate and sesamoids Reduction sequence: Divide volar plate longitudinally or transversely, retract lumbricals, reduce phalanx with flexion and traction
Incision: Longitudinal or curvilinear dorsal incision over MCP Split extensor hood: Between central slip and sagittal band or split volar plate transversely through joint Reduce: Flex the MCP and push the proximal phalanx base over the metacarpal head Repair: Repair sagittal band or volar plate rent to restore stability
Splint: Extension block splint at 20-30 degrees flexion for 2-3 weeks Early motion: Protected active ROM from week 2-3 under therapist supervision Strengthening: Grip strengthening from week 6, return to sport at 10-12 weeks
After reduction, test passive MCP extension under fluoroscopy. If the joint tends to redislocate in extension, repair the radial collateral ligament and consider temporary K-wire stabilisation in 30 degrees flexion for 3 weeks. Document stability before closure.
Complications
- Incidence
- 30-50 percent of open reductions
- Risk Factors
- Delayed presentation, repeated reduction attempts
- Management
- Early protected motion, aggressive hand therapy
- Incidence
- 5-10 percent (mostly neuropraxia)
- Risk Factors
- Volar approach, stretched nerve over metacarpal head
- Management
- Meticulous identification, microsurgical repair if transected
- Incidence
- Less than 10 percent with proper repair
- Risk Factors
- Unrepaired collateral ligament, inadequate splinting
- Management
- Collateral repair, extension block splint, possible temporary pinning
- Incidence
- Less than 5 percent
- Risk Factors
- Open injury, delayed surgery, diabetes
- Management
- Prophylactic antibiotics, meticulous wound care
- Incidence
- Common after greater than 6 weeks delay
- Risk Factors
- Prolonged dislocation, cartilage abrasion
- Management
- Arthroplasty or arthrodesis if symptomatic
The radial digital nerve is at greatest risk during the volar approach to an index finger dislocation. It is stretched over the metacarpal head and can be mistaken for a fibrous band. Always identify and protect both digital nerves before dividing any volar structures. A missed nerve transection causes permanent sensory loss and is a common source of litigation.
Outcomes and Prognosis
- Treatment
- Open reduction, collateral repair if needed
- Expected Outcome
- 80-90 percent achieve functional ROM
- Long-term Function
- Excellent return to work and sport
- Treatment
- Open reduction, more extensive release
- Expected Outcome
- 60-75 percent functional ROM
- Long-term Function
- Good for daily activities, some stiffness
- Treatment
- Open reduction or salvage procedure
- Expected Outcome
- 40-60 percent useful arc, variable pain relief
- Long-term Function
- Functional improvement but rarely normal motion
Best prognosis: Acute presentation, single gentle reduction attempt, concentric reduction, repaired collateral ligament, compliant early motion protocol.
Poor prognosis: Delayed diagnosis greater than 3 weeks, multiple failed closed attempts, chondral damage on metacarpal head, patient non-compliance with therapy.
Key threshold: 3 weeks from injury - outcomes decline significantly after this window, with higher rates of stiffness and post-traumatic arthritis.
Guidelines, Registries & Global Practice
- Index finger MCP is the most common site worldwide for complex dorsal dislocation
- Hyperextension falls are the dominant mechanism across all regions and age groups
- Sports and occupational injuries account for the majority of presentations
- Missed diagnosis remains a problem in emergency settings where skin dimple is not routinely sought
- High-resource centres: early MRI, hand therapist involvement, fluoroscopic stability assessment
- Limited-resource settings: clinical diagnosis, plain radiographs only, volar approach with loupe magnification
- Universal principle: prompt recognition of the skin dimple and avoidance of repeated closed attempts determines outcome more than technology
- Surgery: concentrated in specialist hand units globally, with similar techniques reported from Europe, North America, Asia and Australia
- Diagnosis emphasis
- Skin dimple recognition, single closed attempt only
- Acute treatment
- Open reduction within 24 hours, nerve protection
- Surgical approach
- Volar preferred for direct volar plate release
- Diagnosis emphasis
- Clinical diagnosis, radiographs to exclude fracture
- Acute treatment
- Urgent referral to hand surgery, avoid repeated manipulation
- Surgical approach
- Volar or dorsal according to surgeon preference
- Diagnosis emphasis
- High index of suspicion in hyperextension injuries
- Acute treatment
- Open reduction, collateral ligament assessment
- Surgical approach
- Both approaches accepted, stability testing essential
- Diagnosis emphasis
- Assess for associated metacarpal head fracture
- Acute treatment
- Anatomic reduction, protect soft tissues
- Surgical approach
- Approach dictated by fracture pattern and surgeon experience
There is no dedicated international registry for MCP dislocations. Evidence is derived from small case series and anatomic studies. The consistent message across all guidelines is that recognition of the skin dimple changes management from closed to open reduction and that nerve protection during the volar approach is mandatory. Outcomes are time-dependent, with best results when reduction occurs within 24-48 hours.
Record in every dorsal MCP dislocation:
- Presence or absence of skin dimple at proximal palmar crease
- Number and result of closed reduction attempts
- Neurovascular status before and after any manipulation
- Intraoperative stability assessment and structures repaired
- Post-reduction splint position and rehabilitation plan
A missed complex dislocation leading to permanent stiffness or nerve injury is a recurring source of complaints worldwide. Always document the skin dimple examination and the rationale for proceeding to open reduction.
Controversies & Areas of Uncertainty
Both approaches report good outcomes in small series. The volar approach offers direct visualisation of the interposed structures but carries a risk of digital nerve injury. The dorsal approach is simpler for some surgeons and avoids nerve dissection, yet requires splitting the extensor mechanism or volar plate. Surgeon experience and training appear to influence choice more than clear evidence of superiority.
Some authors advocate routine repair of the radial collateral ligament after reduction, while others repair only when residual instability is demonstrated on stress testing. No comparative studies exist. Most surgeons repair obvious tears and test stability intraoperatively before deciding.
Extension block splinting at 20-30 degrees for 2-3 weeks is widely practised, but the precise angle and duration lack high-quality evidence. Early protected motion is favoured to minimise stiffness, yet too much motion risks recurrent subluxation. Therapist-led protocols vary between centres.
Temporary K-wire stabilisation across the reduced MCP joint is used by some when stability is marginal. Others avoid pinning to allow early motion. No randomised data exist. Decision is individualised based on intraoperative stability and patient compliance.
MCQ Practice Points
Q: Which structure is the primary block to reduction in a complex dorsal MCP dislocation? A: The volar plate with embedded sesamoids. In hyperextension the volar plate folds into the joint space between the metacarpal head and the base of the proximal phalanx. The sesamoids act as a bony wedge. The flexor tendons, lumbricals and deep transverse metacarpal ligament form a secondary constricting noose around the metacarpal neck.
Q: What is the pathognomonic clinical finding in a complex MCP dislocation? A: A skin dimple at the proximal palmar crease. This transverse or oblique dimple directly overlies the metacarpal head and indicates that the volar plate has buttonholed through the joint capsule. Its presence confirms that closed reduction will fail and open reduction is required.
Q: Why does longitudinal traction fail to reduce a complex MCP dislocation? A: Traction tightens the noose. The volar plate, flexor tendons and lumbricals already encircle the metacarpal neck. Longitudinal force increases tension on these structures, locking the proximal phalanx in hyperextension rather than disengaging the interposed tissue. A single gentle attempt is acceptable, but repeated traction causes further damage.
Q: What are the advantages of the volar versus dorsal approach for complex MCP dislocation? A: Volar approach provides direct visualisation of the interposed volar plate, sesamoids and lumbricals, allows precise division of the blocking structures, and facilitates collateral ligament repair. Dorsal approach is technically simpler for some surgeons, avoids nerve dissection, and permits transverse division of the volar plate through the joint. Both achieve similar outcomes when executed correctly.
Q: What is the recommended post-reduction protocol after open reduction of a complex MCP dislocation? A: Extension block splint at 20-30 degrees flexion for 2-3 weeks, followed by protected active motion under hand therapy supervision. Early motion prevents stiffness while the block splint maintains reduction. Strengthening begins at 6 weeks with return to full activity at 10-12 weeks. Stability must be confirmed intraoperatively before deciding on splint position.
Q: Which nerve is most at risk during the volar approach to an index finger MCP dislocation? A: The radial digital nerve. It is stretched over the prominent metacarpal head and can be mistaken for a fibrous band. Careful identification and protection of both digital nerves before dividing any volar structures is mandatory. Nerve injury causes permanent sensory loss on the radial border of the index finger.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old mechanic presents 6 hours after a fall onto his outstretched right hand. His index finger MCP is locked in 60 degrees of hyperextension. There is a clear skin dimple at the proximal palmar crease. Gentle traction under digital block fails to reduce the joint. What is your diagnosis and management plan?”
“A 45-year-old woman presents 5 weeks after a fall. She was told her index finger was 'sprained' and was treated with buddy strapping. She now has a stiff, painful MCP joint with 40 degrees hyperextension deformity, numbness on the radial side of the index finger, and a fixed skin dimple. Radiographs show early joint space narrowing. How would you manage this?”
Key Anatomy
- Volar plate with sesamoids is primary block to reduction
- Flexor tendons, lumbricals and deep transverse ligament form constricting noose
- Index finger most commonly affected due to radial sesamoid and border position
- Radial digital nerve stretched over metacarpal head and at risk in volar approach
Diagnosis
- Skin dimple at proximal palmar crease is pathognomonic for complex injury
- Irreducible on gentle traction confirms volar plate interposition
- X-ray: PA, lateral and oblique to confirm direction and exclude fracture
- High index of suspicion in any hyperextension MCP injury
Treatment Algorithm
- Simple dislocation: single closed reduction attempt, extension block splint 3 weeks
- Complex (skin dimple or failed reduction): open reduction, volar or dorsal approach
- Acute (under 24 hours): best outcomes with prompt open reduction
- Chronic (over 3 weeks): consider salvage arthroplasty if cartilage destroyed
Surgical Pearls
- Volar approach: protect radial digital nerve first, then divide volar plate longitudinally
- Dorsal approach: transverse split of volar plate through the joint
- After reduction: test stability, repair collateral ligament if torn
- Splint: extension block 20-30 degrees flexion for 2-3 weeks then early motion
Complications
- Residual stiffness: 30-50 percent, mitigated by early protected motion
- Digital nerve injury: 5-10 percent, mostly neuropraxia, prevent by identification
- Recurrent instability: less than 10 percent with proper collateral repair
- Post-traumatic arthritis: common after delayed presentation greater than 3 weeks
Evidence Base and Key Trials
Dorsal dislocation of the metacarpophalangeal joint of the index finger
- Classic early description of dorsal metacarpophalangeal dislocation of the index finger, distinguishing the simple (reducible) from the complex (irreducible) injury
- The complex/irreducible dislocation is characterised by interposition of the volar plate, which blocks closed reduction
- A puckered skin dimple in the proximal palm is a clinical sign of the complex injury
- Open reduction is required once a dislocation is irreducible by closed means
A simplified technique for treating the complex dislocation of the index MCP joint
- Described a direct dorsal longitudinal approach (through skin and extensor tendon) for the complex dislocation of the index MCP joint, as an alternative to Kaplan's volar approach
- The interposed fibrocartilaginous volar plate is brought into full view and split longitudinally, after which the dislocation reduces spontaneously as the flexor tendons and lumbrical slip past the metacarpal head
- Stated advantages over the volar approach: full exposure of the volar plate (the main block to reduction), less risk to the digital nerves, and the ability to fix the frequently-associated metacarpal-head osteochondral fracture
Irreducible metacarpophalangeal joint dislocations: Clinical characteristics, surgical approaches, and outcomes
- Retrospective series of 13 surgically-treated irreducible MCP dislocations; the index finger was most often involved (53.8%) and dorsal dislocations predominated (76.9%)
- A dorsal approach (used in 76.9%) gave greater MCP flexion and lower disability (QuickDASH), while a volar approach gave superior grip strength
- Return to sport was earlier after the dorsal approach; differences showed large effect sizes but did not reach statistical significance
Kaplan's Lesion: A Case Report On The Complex Dislocation Of The Index Finger In A Weightlifter
- Case report of complex index finger MCP dislocation (Kaplan lesion) in a weightlifter successfully managed with open reduction