L1-L2 Cord-Tip Lesion | Mixed UMN and LMN | Early Sphincter Dysfunction
- Conus medullaris typically ends at the L1-L2 disc level in adults (T12-L3 range)
- Early and prominent bladder and bowel dysfunction is the clinical hallmark
- Symmetric saddle anaesthesia (S2 to S5) distinguishes conus from cauda equina
- Mixed UMN signs (Babinski, hyperreflexia) and LMN signs (flaccid weakness, areflexia) coexist
- Urgent MRI of the whole spine and surgical decompression within 48 hours optimise recovery
- “Conus = cord injury, therefore UMN signs may be present (Babinski) alongside LMN signs
- “Cauda = pure LMN, asymmetric, radicular pain dominant, sphincter loss later
- “Saddle anaesthesia is symmetric in conus, often patchy in cauda equina
- “Ankle jerk (S1) preserved, but anal wink (S2-S4) and bulbocavernosus (S2-S4) lost
- “Always examine perineum and perform PR on any suspected cord/cauda lesion
Conus medullaris = terminal end of the spinal cord, located at the L1-L2 disc in adults. Contains sacral cord segments S2 to S5 and the coccygeal segments. The lumbosacral enlargement above (L1-S2) gives rise to the lumbar and sacral nerve roots that form the cauda equina below.
Early, symmetric sphincter dysfunction with saddle anaesthesia. Bladder retention or incontinence, loss of anal tone, and erectile dysfunction are often the presenting features - sometimes before overt motor weakness is recognised.
UMN signs (Babinski, brisk reflexes, spasticity) reflect corticospinal tract involvement within the cord. LMN signs (flaccid weakness, areflexia, wasting) reflect anterior horn cell or sacral root damage at the conus tip. Both patterns coexist.
Urgent MRI of the whole spine (not just lumbar) to exclude higher lesions, then surgical decompression within 48 hours where there is a compressive lesion. Steroids only if metastasis or trauma per protocol.
- Conus Medullaris
- Cord tip at L1-L2 (cord tissue)
- Cauda Equina
- Lumbosacral nerve roots below conus
- Conus Medullaris
- Mixed UMN plus LMN
- Cauda Equina
- Pure LMN only
- Conus Medullaris
- Early, symmetric, S2 to S5
- Cauda Equina
- Late, often patchy or unilateral
- Conus Medullaris
- Early and prominent
- Cauda Equina
- Late and may be incomplete
- Conus Medullaris
- Less prominent, bilateral
- Cauda Equina
- Dominant feature, unilateral or bilateral
- Conus Medullaris
- Hyperreflexia possible with Babinski plus absent ankle jerk
- Cauda Equina
- Areflexia (knee or ankle) without Babinski
MIXEDMixed UMN and LMN Pattern
Hook:MIXED signs = think cord-tip lesion - conus medullaris has UMN and LMN together!
SPINALConus versus Cauda Equina - Key Distinguishing Features
Hook:SPINAL exam: Conus is the cord-tip - symmetric, mixed, early sphincter loss!
Overview and Epidemiology
Conus medullaris syndrome is a surgical emergency. Outcomes depend on the cause, the completeness of sphincter loss at presentation, and the time to decompression. A delayed diagnosis (often missed because the patient has minimal back pain) is a recurring source of complaints and litigation worldwide. The key cognitive trap is to label every acute sphincter disturbance as a "cauda equina syndrome" - the cord-tip lesions behave differently and warrant equally urgent imaging.
- Adult conus tip: L1-L2 disc in 65 to 75 percent of adults, range T12 to L3
- Trauma: burst fractures at the thoracolumbar junction are the classic cause
- Tumour: metastases (breast, lung, prostate, kidney, lymphoma) and primary tumours (ependymoma, astrocytoma, haemangioblastoma)
- Disc herniation: large central disc at L1-L2 can compress the conus
- Tethered cord, lipoma, dermoid, cyst: relevant in younger patients
- Ischaemia: anterior spinal artery infarct at the conus
- Bladder and bowel dysfunction dominate and persist even after surgery
- Sexual dysfunction in 50 to 70 percent of men after conus injury
- Permanent saddle anaesthesia impairs continence, hygiene and seating comfort
- Pressure sores from loss of sensation plus immobility
- Psychosocial burden: depression, loss of independence, relationship strain
Pathophysiology
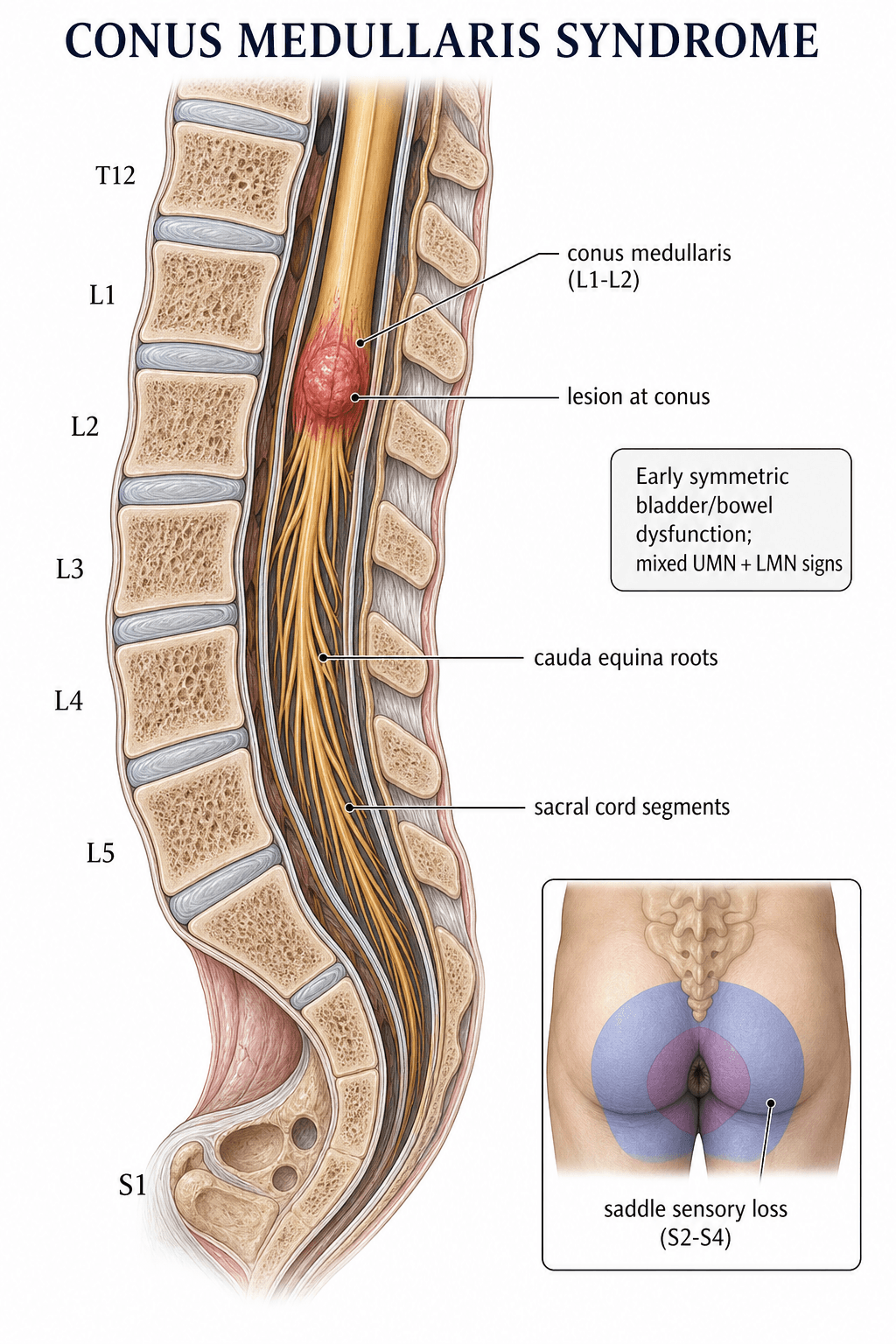
The spinal cord ends as the conus medullaris at the L1-L2 disc in adults. Within the conus sit the sacral cord segments S2 to S5 and the coccygeal segments, which supply the perineum, bladder, bowel and sexual function. The lumbosacral nerve roots (L2-S5) descend within the cauda equina to exit at their respective neural foramina. A lesion at the conus damages both cord tracts (UMN) and sacral anterior horn cells or roots (LMN) - hence the mixed clinical signature.
- Type of Tissue
- Upper motor neuron
- Sign When Injured
- Spasticity, hyperreflexia, Babinski
- Pattern
- UMN - may be present in conus
- Type of Tissue
- Lower motor neuron
- Sign When Injured
- Flaccid weakness, wasting, areflexia of S2-S5
- Pattern
- LMN - present in conus and cauda equina
- Type of Tissue
- Autonomic (intermediolateral cell column)
- Sign When Injured
- Bladder retention, erectile dysfunction
- Pattern
- Autonomic - hallmark of conus lesion
- Type of Tissue
- Sensory tract
- Sign When Injured
- Loss of vibration and proprioception
- Pattern
- May be preserved in pure conus lesion
- Type of Tissue
- Sensory tract
- Sign When Injured
- Loss of pain and temperature
- Pattern
- May be preserved in pure conus lesion
Sacral cord segments S2 to S4 carry parasympathetic fibres to the detrusor
Pudendal nerve (S2-S4) controls the external urethral and anal sphincters
Compressive conus lesion interrupts both preganglionic and somatic outflow
Result: Detrusor areflexia with retention, then overflow incontinence; loss of anal tone
Midline compression of the conus affects both halves equally
Saddle area is innervated by bilateral S2 to S5 dermatomes
Sphincter loss is bilateral because both pudendal nerves are equally compromised
Contrasts with cauda equina: roots are lateralised within the thecal sac, so cauda lesions are often patchy
Classification and Types
Classification by Cause
- Mechanism
- Acute compression by retropulsed bone fragments
- Typical Presentation
- Acute onset, often with incomplete spinal cord injury pattern
- Treatment Notes
- Urgent surgical decompression plus stabilisation
- Mechanism
- Large central disc compresses conus
- Typical Presentation
- Subacute back pain, progressive saddle symptoms
- Treatment Notes
- Discectomy; outcome depends on duration of symptoms
- Mechanism
- Vertebral body collapse and epidural mass
- Typical Presentation
- Painful, often in known cancer patient
- Treatment Notes
- Urgent MRI; steroids; radiotherapy or surgery (NOMS framework)
- Mechanism
- Slow cord expansion
- Typical Presentation
- Insidious onset, often misdiagnosed as lumbar stenosis
- Treatment Notes
- Surgical resection; outcomes better with ependymoma
- Mechanism
- Traction injury, often in paediatric or young adult
- Typical Presentation
- Long history, cutaneous stigmata, mixed UMN plus LMN
- Treatment Notes
- Detethering surgery
- Mechanism
- Ischaemia of conus (watershed zone)
- Typical Presentation
- Sudden painless sphincter loss, no compressive lesion on MRI
- Treatment Notes
- Supportive; steroids not indicated; prognosis guarded
Aetiology drives prognosis: trauma and disc respond best to urgent surgery; tumour and infarct are less predictable.
Clinical Assessment
- Onset: acute (trauma, disc), subacute (tumour), or chronic (intramedullary lesion)
- Pain: back pain, bilateral leg pain, perineal discomfort
- Sensory: saddle numbness (perineum, buttocks, posterior thighs), often bilateral
- Bladder: retention with overflow, urgency, frequency, incontinence
- Bowel: constipation, loss of awareness of rectal fullness
- Sexual: erectile dysfunction, loss of ejaculation, loss of genital sensation
- Motor: assess L2-S1 myotomes; record weakness pattern (proximal vs distal)
- Reflexes: knee jerk (L3-L4) often preserved, ankle jerk (S1) often absent
- Pathological signs: Babinski (UMN), ankle clonus
- Sacral reflexes: anal wink (S2-S4), bulbocavernosus (S2-S4) - always test
- Per rectal exam: anal tone, voluntary squeeze, post-void residual
- Sensory: perineum, buttocks, posterior thigh - map the deficit
Do not omit the per-rectal exam - it is the only way to assess anal tone and S2-S4 function. Do not stop at the lumbar spine - always include the thoracolumbar junction. Do not rely on absence of pain to exclude a conus lesion; compressive conus lesions can present with painless sphincter loss. Do not delay MRI waiting for urological investigations; an indwelling catheter with post-void residual is a reasonable bedside screen.
- Level
- S2 to S4
- Method
- Streak perianal skin, watch anal sphincter contract
- Significance
- Absent in conus and cauda equina lesions
- Level
- S2 to S4
- Method
- Squeeze glans or clitoris, feel anal sphincter contract
- Significance
- Absent in conus and cauda equina; also absent in sacral cord injury
- Level
- S1 (root)
- Method
- Achilles tendon strike
- Significance
- Often absent in conus (LMN) and cauda equina
- Level
- L3 to L4 (root)
- Method
- Patellar tendon strike
- Significance
- Preserved in pure conus lesion - helps localise
- Level
- Corticospinal tract (cord)
- Method
- Stroking lateral sole
- Significance
- Positive in conus (UMN tract involved) - not in pure cauda equina
- Pattern
- Symmetric saddle loss, mixed UMN plus LMN, early sphincter loss
- Discriminating Finding
- Babinski plus absent ankle jerk; painful or painless
- Key Test
- MRI whole spine (T12-L2 cord)
- Pattern
- Asymmetric saddle loss, pure LMN, severe radicular pain
- Discriminating Finding
- Areflexia (knee or ankle) without Babinski
- Key Test
- MRI lumbar spine (thecal sac compression)
- Pattern
- Sensory level on trunk, paraplegia, urinary retention
- Discriminating Finding
- Trunk sensory level, brisk reflexes below lesion
- Key Test
- MRI of lesion level
- Pattern
- Sudden painful or painless cord signs
- Discriminating Finding
- No compressive lesion on MRI; DWI may show cord signal change
- Key Test
- MRI with diffusion-weighted sequence
- Pattern
- No saddle numbness, no leg signs
- Discriminating Finding
- Benign prostatic hyperplasia, post-op retention, drugs
- Key Test
- Catheter, post-void residual, bladder scan
- Pattern
- Variable - depends on cause
- Discriminating Finding
- Look for disc, mass, pus, blood on MRI
- Key Test
- MRI with contrast and diffusion
Conus medullaris is a cord lesion at L1-L2; cauda equina is a root lesion below. The practical discriminators are: (1) symmetry - conus is symmetric, cauda often patchy; (2) sphincter timing - conus loses sphincter function earlier; (3) pain - cauda is more painful; (4) UMN signs - Babinski indicates conus; (5) reflexes - hyperreflexia of knees with absent ankles favours conus. The imaging must include the conus tip at L1-L2 even if a lumbar disc is suspected.
The single most important prognostic discriminator in any cord-tip injury is whether the injury is complete or incomplete, and that is defined by sacral sparing - assessed at exactly the most caudal segments the conus contains:
- The three components of sacral sparing (ISNCSCI): (1) light touch and pin-prick at S4-5; (2) deep anal pressure (DAP) felt on rectal examination; and (3) voluntary anal contraction (VAC). The presence of any of these means the injury is incomplete.
- Why it matters: an injury is ASIA Impairment Scale (AIS) A = complete only when there is NO motor or sensory function in the lowest sacral segments (S4-5). Any sacral sparing makes it at least AIS B (sensory incomplete) and carries a substantially better prognosis for recovery.
- The spinal-shock caveat: you cannot reliably call an injury complete until spinal shock has resolved - the return of the bulbocavernosus reflex signals the end of spinal shock, after which a persistent absence of sacral sparing genuinely indicates a complete injury.
- Practical message: in a conus lesion, formally document S4-5 sensation, DAP and VAC - not just "saddle numbness". Sacral sparing is the finding that converts a grim "complete" prognosis into a hopeful "incomplete" one and must be recorded before and after decompression.
SADDLEClinical Features of Conus Medullaris Syndrome
Hook:SADDLE the S2-S5 dermatomes with early sphincter loss - the conus syndrome signature!
Investigations
Imaging and Adjunct Protocol
Sequences: sagittal T2, axial T2 through conus, T1 pre and post gadolinium
Look for: cord expansion, conus oedema, intramedullary lesion, epidural mass, disc, haematoma, abscess, fracture fragment
Whole spine: to exclude skip lesions and higher cord compression
Gadolinium: improves detection of tumour, abscess, leptomeningeal disease
Indication: pacemaker, severe claustrophobia, metal contraindicating MRI
Technique: intrathecal contrast via lumbar puncture, then CT
Look for: block at the conus level, cord expansion indirectly, mass effect
Disadvantage: invasive, risk of post-dural-puncture headache
Post-void residual: bladder scan after voiding - greater than 200 mL suggests retention
Urodynamics: assess detrusor areflexia, sphincter dyssynergia, capacity
Urethral catheter: insert early to protect upper tracts and document retention
Useful for prognosis: complete areflexia carries poorer bladder recovery
Indication: suspected vascular malformation (dural AV fistula)
Look for: enlarged perimedullary veins, early venous filling
Treatment: endovascular embolisation is first line for many dural AV fistulas
Prognosis: better recovery if treated before irreversible cord damage
Always image the whole spine, not just the lumbar region. A patient with saddle anaesthesia and negative lumbar MRI may harbour a dorsal cervicothoracic lesion (e.g. dural AV fistula) presenting with conus-type signs. In the trauma setting, CT plus MRI of the thoracolumbar junction is mandatory when neurological signs are present, even with a normal lumbar MRI.
Management Algorithm
Acute Compressive Conus Syndrome (Trauma, Disc, Haematoma, Abscess)
Goal: urgent decompression to maximise neurological and sphincter recovery
Treatment Protocol
ATLS protocol for trauma: airway, breathing, circulation, disability
Spinal precautions: log roll, hard collar, manual in-line stabilisation
Catheterise: indwelling urinary catheter to protect bladder and document retention
Steroids: per institutional protocol (methylprednisolone controversial in penetrating trauma)
MRI whole spine with contrast as first line
CT if MRI contraindicated or to delineate bony injury
Identify: compressive lesion, level, extent, cause (disc, bone, mass, blood, pus)
Plan: surgical approach (posterior, transpedicular, costotransversectomy as needed)
Target: decompression within 24 to 48 hours from onset of complete sphincter loss
Approach: laminectomy plus decompression; pedicle screw fixation for instability
Disc at L1-L2: discectomy with or without interbody fusion
Tumour: debulking plus stabilisation, then oncological treatment
Bowel and bladder programme: timed voiding, intermittent self-catheterisation
Pressure care: 2-hourly turns, pressure-relieving mattress
Mobilise: physiotherapy, occupational therapy, gait aids as needed
Psychology: early referral for adjustment support, sexual function counselling
The strongest evidence supports surgical decompression within 48 hours of onset of complete conus or cauda equina syndrome. Beyond 48 hours, bladder recovery rates fall significantly. Even partial benefit may justify urgent surgery; do not refuse surgery because some hours have elapsed.
Complications
- Incidence
- 40 to 70 percent after complete conus syndrome
- Risk Factors
- Complete loss at presentation, delayed surgery
- Management
- Intermittent self-catheterisation, anticholinergics, sacral neuromodulation
- Incidence
- 30 to 60 percent
- Risk Factors
- Loss of anal tone, neurogenic bowel
- Management
- Bowel programme, transanal irrigation, diet, suppositories
- Incidence
- 50 to 70 percent of men
- Risk Factors
- S2 to S4 parasympathetic injury
- Management
- Phosphodiesterase-5 inhibitors, intracavernosal injections, penile prosthesis
- Incidence
- Common in immobile patients
- Risk Factors
- Loss of sensation plus immobility
- Management
- 2-hourly turns, pressure-relieving mattress, education
- Incidence
- 20 to 40 percent
- Risk Factors
- Catheter use, incomplete emptying
- Management
- Hygiene, fluid management, intermittent self-catheterisation
- Incidence
- 5 to 15 percent without prophylaxis
- Risk Factors
- Immobility, motor weakness
- Management
- Mechanical plus chemical prophylaxis from admission
- Incidence
- 20 to 30 percent
- Risk Factors
- Root or cord damage, central sensitisation
- Management
- Gabapentinoids, duloxetine, multidisciplinary pain team
The bladder dysfunction is the dominant disability, so be able to TYPE the neurogenic bladder - it differs fundamentally by where the lesion sits relative to the sacral cord:
- Suprasacral (UMN) lesion (cord injury ABOVE the conus): a spastic / hyperreflexic ("automatic") bladder - the detrusor contracts reflexively, often with detrusor-sphincter dyssynergia (DSD), generating high intravesical pressures that threaten the upper tracts (reflux, hydronephrosis).
- Conus / cauda (LMN) lesion (this topic): a flaccid / areflexic ("autonomous") bladder - the sacral parasympathetic outflow (S2-4) and pudendal control are destroyed, so the detrusor does not contract; the result is retention with overflow incontinence and a large post-void residual.
- Why the distinction matters: it dictates management - the flaccid LMN bladder is managed with clean intermittent self-catheterisation (CISC) to empty it and protect the kidneys, whereas the spastic UMN bladder needs anticholinergics/antimuscarinics (or onabotulinumtoxinA) to lower storage pressure.
- The universal imperative: whatever the type, the goal is low-pressure storage and complete emptying to protect the upper urinary tracts - renal failure was historically a leading cause of death in spinal cord injury, so urology follow-up and urodynamics are essential.
Exam point: a conus lesion gives an LMN flaccid areflexic bladder (retention + overflow) managed by CISC, distinct from the spastic high-pressure UMN bladder of a higher cord lesion.
The single most important complication to prevent is permanent sphincter and sexual dysfunction. Once complete conus syndrome has been present for greater than 48 hours, recovery of bladder, bowel and sexual function is uncommon. The window for intervention is short. Document the time of onset, request MRI urgently, and escalate to the operating team on the same admission - do not defer imaging to the next available outpatient slot.
Outcomes and Prognosis
- Favourable
- Disc, fracture fragment, abscess
- Unfavourable
- Tumour, ischaemia, tethered cord
- Expected Recovery
- Compressive lesions recover better with surgery
- Favourable
- Decompression within 24 hours of complete loss
- Unfavourable
- Decompression after 48 hours of complete loss
- Expected Recovery
- Earlier surgery = better sphincter recovery
- Favourable
- Incomplete syndrome with partial sparing
- Unfavourable
- Complete dense saddle loss, no voluntary sphincter
- Expected Recovery
- Incomplete lesions recover more reliably
- Favourable
- Recovery of ambulation in 60 to 80 percent
- Unfavourable
- Permanent paraplegia in 10 to 20 percent
- Expected Recovery
- Motor recovery is more likely than sphincter recovery
- Favourable
- 20 to 50 percent regain useful bladder control
- Unfavourable
- Permanent catheterisation in 30 to 60 percent
- Expected Recovery
- Sphincter recovery is the most variable outcome
Best prognosis: incomplete conus syndrome, decompression within 24 hours, traumatic or disc cause, intact sacral reflexes on presentation, young age.
Poor prognosis: complete conus syndrome, decompression after 48 hours, tumour or ischaemia, absent sacral reflexes, advanced age, comorbidities.
Key threshold: 24 to 48 hours from complete loss to surgical decompression. Outcomes decline sharply after this window.
Guidelines, Registries & Global Practice
- Spinal cord injury affects an estimated 250 000 to 500 000 people per year worldwide (WHO), with thoracolumbar injuries overrepresented in low-fall and high-energy trauma
- Conus medullaris syndrome accounts for a small but clinically critical subset of all spinal cord and lumbosacral injuries
- Metastatic epidural spinal cord compression occurs in 5 to 10 percent of cancer patients, with the thoracolumbar junction (and therefore the conus) the most common site
- Cauda equina syndrome from disc herniation occurs in 1 to 3 per 100 000 adults per year; the same anatomical region is the typical target of conus compression
- High-resource: rapid access to MRI within hours, dedicated spinal surgery on-call rotas, indwelling catheter and intermittent self-catheterisation programmes
- Limited-resource: MRI may be unavailable; CT myelography remains a useful alternative; transfer to a tertiary spine centre is often required
- Steroid use for tumour-related compression (dexamethasone) is widely available and inexpensive
- Rehabilitation: spinal cord injury units concentrate in high-income settings; in low-resource settings, community-based rehabilitation is the mainstay
- Diagnosis emphasis
- Neurological, Oncological, Mechanical, Systemic staging for tumour cases
- Acute treatment
- Corticosteroids, urgent surgery plus radiotherapy or radiotherapy alone
- Surgery and rehabilitation
- Separation surgery plus stereotactic body radiotherapy for radioresistant tumours
- Diagnosis emphasis
- MRI whole spine for suspected cord or conus compression; document sphincter function
- Acute treatment
- Surgical decompression within 24 to 48 hours of complete loss
- Surgery and rehabilitation
- Multidisciplinary rehabilitation from day 1
- Diagnosis emphasis
- Thoracolumbar injury classification (AOSpine TLICS) for trauma
- Acute treatment
- Urgent decompression and stabilisation for incomplete cord or conus injury
- Surgery and rehabilitation
- Early mobilisation and rehabilitation
- Diagnosis emphasis
- International standards for neurological classification of spinal cord injury
- Acute treatment
- Standardised neurological examination including sacral segments
- Surgery and rehabilitation
- Rehabilitation planning aligned with the International Classification of Functioning
There is no dedicated registry for conus medullaris syndrome, but spinal cord injury registries (e.g. the National Spinal Cord Injury Database, the Rick Hansen Spinal Cord Injury Registry) capture neurological level, completeness and outcome, and provide population-level data on the conus subset. The conus medullaris is classified as an injury at the T12 neurological level on the ISNCSCI scale; completeness (AIS A versus B versus C, D, E) drives outcome reporting.
Record in every patient with suspected conus medullaris syndrome:
- Time of onset of sphincter dysfunction
- Post-void residual volume (catheter or bladder scan)
- Per-rectal examination findings (anal tone, voluntary squeeze)
- Sacral reflexes (anal wink, bulbocavernosus)
- Documented neurological level on the ISNCSCI scale
- MRI whole spine requested and time of scan
- Time to surgical decompression (where applicable)
- Patient and family counselling regarding prognosis
A missed conus medullaris syndrome leading to permanent sphincter and sexual dysfunction is a recurring source of complaints and litigation worldwide. Always perform and document the per-rectal examination and sacral reflexes in any patient with back pain plus lower limb or sphincter symptoms.
Controversies and Areas of Uncertainty
Corticosteroids are clearly indicated for tumour-related cord or conus compression. In acute traumatic conus injury, the NASCIS II evidence for methylprednisolone is now considered weak because of methodological concerns and the small functional benefit seen in some subgroups. Most current guidelines (AO Spine, AANS) do not mandate steroids for acute traumatic spinal cord injury, and many centres have abandoned them. Steroids remain standard for metastatic compression.
The 24 to 48 hour window is supported by retrospective data; a randomised trial is ethically and logistically difficult. Some centres decompress incomplete conus syndromes urgently, others accept stable incomplete deficits. There is growing support for individualised timing based on serial MRI and clinical reassessment, with surgery reserved for progression or persistent compression.
Minimally invasive decompression and percutaneous pedicle screw fixation may reduce soft tissue morbidity and blood loss, but visualisation of the conus and epidural space is more limited. In tumour and trauma, the open approach is still the standard. In disc-related conus compression, tubular or endoscopic discectomy is increasingly used where appropriate.
Sacral neuromodulation and tibial nerve stimulation are established for refractory lower urinary tract dysfunction but are not standard for acute conus syndrome. Early small studies suggest that early neuromodulation after decompression may improve bladder outcomes, but the evidence is preliminary and longer-term studies are awaited.
MCQ Practice Points
Q: At what vertebral level does the conus medullaris typically end in adults? A: L1-L2 disc in 65 to 75 percent of adults, with a normal range from T12 to L3. Below the conus, the lumbosacral nerve roots descend within the cauda equina to exit at their respective neural foramina. A lesion at L1-L2 may therefore affect the conus, the cauda equina, or both, depending on its craniocaudal extent.
Q: How do you clinically distinguish a conus medullaris syndrome from a cauda equina syndrome? A: Conus medullaris presents with early symmetric sphincter dysfunction, saddle anaesthesia, and mixed UMN plus LMN signs (Babinski may be present with absent ankle jerk). Cauda equina presents with severe radicular pain, asymmetric perineal numbness, and pure LMN signs (areflexia without Babinski). The lesion in conus is a cord lesion at L1-L2; in cauda equina, it is a lumbosacral root lesion below the conus.
Q: What is the surgical target time for decompression in an acute conus or cauda equina syndrome? A: Within 24 to 48 hours of onset of complete sphincter loss. Decompression within 24 hours gives the best chance of bladder recovery. Decompression between 24 and 48 hours still offers benefit in selected patients. Beyond 48 hours from complete loss, bladder recovery is uncommon. Incomplete syndromes should also be decompressed urgently because progression can occur.
Q: What do the anal wink and bulbocavernosus reflexes test, and when are they lost? A: Both reflexes depend on S2 to S4 cord segments and the pudendal nerve. The anal wink is elicited by stroking the perianal skin and observing contraction of the external anal sphincter. The bulbocavernosus reflex is elicited by squeezing the glans penis or clitoris and feeling for contraction of the bulbocavernosus muscle. They are lost in conus medullaris syndrome and in cauda equina syndrome, and are a key bedside test for sacral cord and root integrity.
Q: Why is whole-spine MRI recommended in suspected conus medullaris syndrome? A: Because skip lesions occur (especially in tumour and dural arteriovenous fistula) and because the cord lesion responsible for conus-type signs may be above the lumbar region (e.g. a cervicothoracic dural AV fistula can present with conus signs). MRI of the lumbar spine alone can miss a higher lesion. Contrast-enhanced T1 helps differentiate tumour, abscess, and inflammatory lesions.
Q: What is the most reliable prognostic factor for sphincter recovery after conus medullaris syndrome? A: The completeness of the syndrome at the time of surgical decompression, combined with the time from onset to decompression. Patients with incomplete conus syndrome decompressed within 24 hours have the best chance of regaining useful bladder, bowel and sexual function. Complete dense saddle loss plus decompression after 48 hours carries a poor prognosis for sphincter recovery, although motor recovery may still occur.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old man falls from a ladder and lands on his feet. He has mid-back pain, cannot feel his perineum, and has not passed urine for 12 hours. On examination, he has weak hip flexion bilaterally, absent ankle jerks, and a patulous anus. Plantar responses are equivocal. What is your immediate assessment and management?”
“A 68-year-old woman with known metastatic breast cancer presents with a 3-week history of worsening low back pain, numbness over the buttocks, difficulty initiating micturition, and constipation. On examination, she has reduced perianal sensation bilaterally, a weak anal sphincter, and a post-void residual of 450 mL. MRI shows an epidural mass at T12-L1 compressing the conus. How would you manage this patient?”
Key Anatomy
- Conus medullaris = terminal cord tip at L1-L2 in adults (range T12 to L3)
- Contains sacral cord segments S2 to S5 and the coccygeal segments
- Below the conus, lumbosacral nerve roots form the cauda equina
- Corticospinal tracts within the cord give UMN signs; sacral anterior horn cells give LMN signs
Clinical Hallmarks
- Early, symmetric saddle anaesthesia (S2 to S5) with bladder and bowel dysfunction
- Mixed UMN plus LMN signs (Babinski may coexist with absent ankle jerk)
- Symmetric pattern (conus) versus patchy (cauda equina)
- Per-rectal exam is mandatory - anal tone, voluntary squeeze, anal wink, bulbocavernosus
Conus versus Cauda Equina
- Conus = cord lesion at L1-L2, mixed UMN plus LMN, early sphincter loss, symmetric, less pain
- Cauda equina = root lesion below conus, pure LMN, severe radicular pain, asymmetric, later sphincter loss
- Babinski sign favours conus; absent Babinski and areflexia favours cauda equina
- Imaging must include the conus tip even if a lumbar disc is suspected
Investigations
- MRI whole spine with gadolinium as first line - sagittal and axial T2 plus contrast T1
- CT myelography if MRI contraindicated
- Spinal angiography if dural arteriovenous fistula is suspected
- Post-void residual by bladder scan; urodynamic studies for prognosis
Management
- Urgent surgical decompression within 24 to 48 hours of complete sphincter loss
- Steroids for tumour-related compression (dexamethasone), not routine in trauma
- Multidisciplinary team for tumour (NOMS framework: Neurological, Oncological, Mechanical, Systemic)
- Early bladder and bowel programme, pressure care, sexual function counselling
Complications and Outcomes
- Permanent bladder dysfunction in 40 to 70 percent after complete conus syndrome
- Sexual dysfunction in greater than 50 percent of men
- Pressure sores and urinary tract infections from catheter use
- Motor recovery more likely than sphincter recovery
Evidence Base and Key Trials
Cauda equina syndrome: what is the relationship between timing of surgery and outcome?
- Surgical decompression within 24 hours of complete cauda equina syndrome gives the best bladder recovery
- Decompression between 24 and 48 hours still offers benefit in selected patients
- Beyond 48 hours from complete loss, bladder recovery is uncommon but not impossible
- Incomplete syndrome should also be decompressed urgently because progression can occur
Timing of surgical intervention in cauda equina syndrome: a systematic critical review
- Systematic review confirmed that early decompression (within 24 hours) is associated with better urological outcomes
- Patients with incomplete deficits recover better than those with complete deficits regardless of timing
- The 48-hour threshold is a useful clinical benchmark but should not preclude later surgery in selected patients
- Motor recovery is more likely than sphincter recovery across all timing groups
Definitions of traumatic conus medullaris and cauda equina syndrome: a systematic literature review
- Conus medullaris syndrome is defined by mixed UMN and LMN signs with early symmetric sphincter dysfunction
- Cauda equina syndrome is defined by pure LMN signs with asymmetric radiculopathy and later sphincter loss
- Considerable overlap exists in clinical practice, and standardised diagnostic criteria are lacking
- Accurate distinction is essential for prognosis, surgical planning and medicolegal documentation
Spinal dural arteriovenous fistulas: clinical features in 80 patients
- Spinal dural arteriovenous fistula frequently presents as a progressive conus-type myelopathy in middle-aged men
- MRI shows conus oedema with enlarged perimedullary veins, often initially misread as degenerative change
- Spinal angiography is the gold standard for diagnosis and guides endovascular or surgical treatment
- Endovascular embolisation is first-line treatment, with surgical disconnection for failures or recurrences