Corticosteroids in Orthopaedics
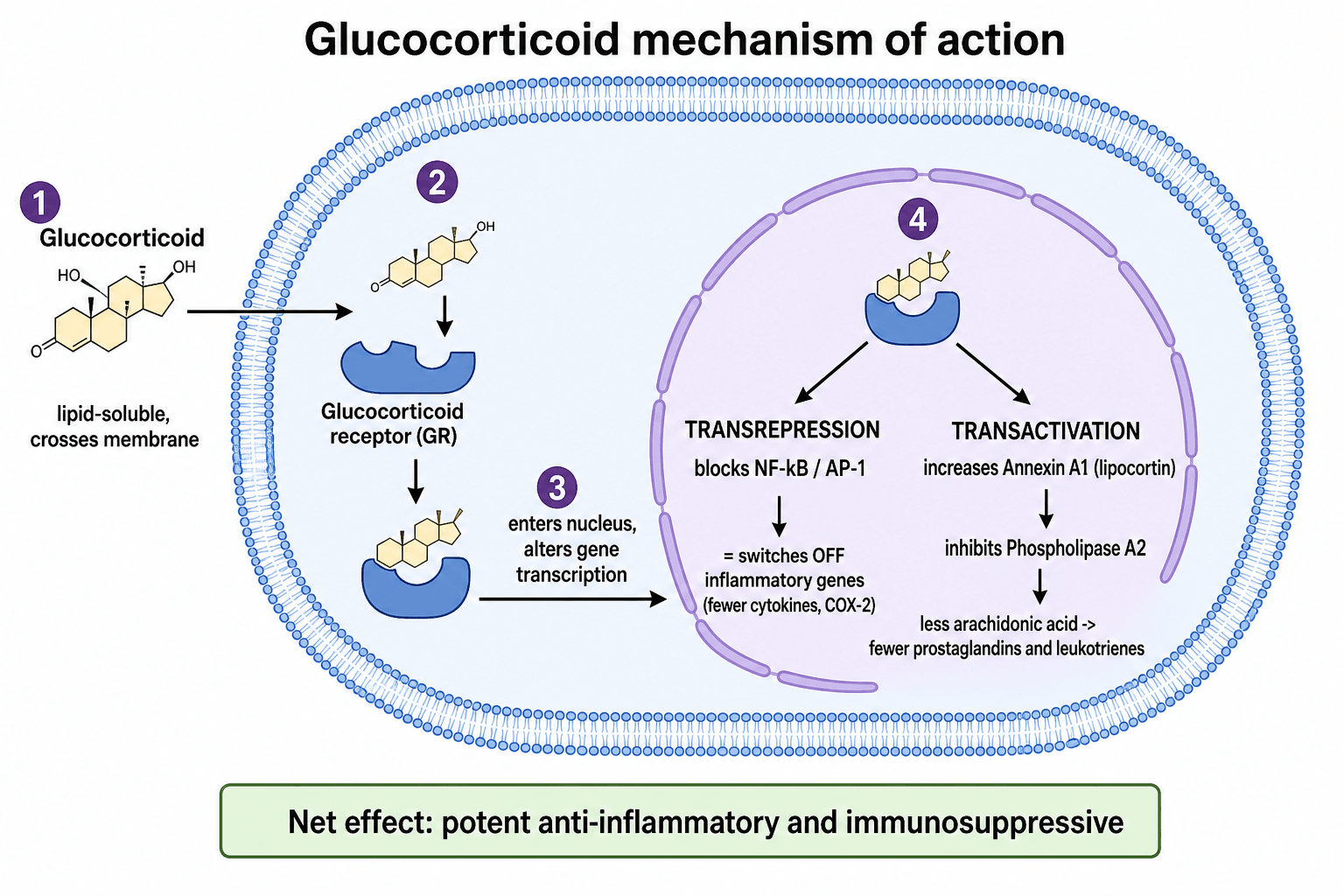
Glucocorticoids cross the cell membrane, bind the cytoplasmic glucocorticoid receptor, and the complex moves to the nucleus to change gene transcription. They switch off inflammatory genes and reduce production of cytokines, prostaglandins, and other mediators. The result is potent anti-inflammatory and immunosuppressive action - and the broad side-effect profile that comes with affecting so many tissues.
The commonest serious systemic harm. Steroids suppress bone formation and increase resorption, so bone is lost fastest in the first 3 to 6 months. Assess fracture risk early and treat - do not wait for a fracture.
Corticosteroids are the most common cause of non-traumatic osteonecrosis. The femoral head is the classic site, it can follow even short high-dose courses, and it is often bilateral. New hip or groin pain on steroids means MRI.
Long-term steroids impair wound and fracture healing, raise infection risk, and suppress the adrenal axis - so patients need perioperative stress-dose cover to avoid an adrenal crisis.
Overview
Corticosteroids (glucocorticoids) are among the most powerful anti-inflammatory drugs in medicine. In orthopaedics they appear in two very different ways: as systemic therapy for inflammatory and autoimmune disease (where the orthopaedic surgeon usually sees the side effects rather than prescribes the drug), and as local injections into joints, bursae, and tendon sheaths to relieve pain.
For the exam, the key is to understand both the benefit (rapid, strong suppression of inflammation) and the harm, because corticosteroids are heavily examined for their musculoskeletal complications. Three threads recur throughout this topic: how they work, what they do to bone (glucocorticoid-induced osteoporosis and osteonecrosis - the two headline harms), and how to use them safely, both as an injection and around surgery.
Indications in Orthopaedic Practice
Systemic steroids control flares of rheumatoid arthritis and other inflammatory or autoimmune joint disease; an intra-articular injection can settle a single hot joint.
An intra-articular injection gives short-term pain relief in a flaring osteoarthritic joint - useful as a bridge or for a special event, not as a long-term treatment.
Injection for subacromial bursitis, trigger finger, de Quervain tenosynovitis, and carpal tunnel syndrome, and for enthesopathies such as tennis elbow (where benefit is short-lived and may be no better than other options long term).
Patients are often on long-term steroids for asthma, inflammatory bowel disease, transplantation, or connective-tissue disease - the surgeon must manage the bone, healing, and adrenal consequences.
Mechanism of Action
Glucocorticoids are lipid-soluble and pass straight through the cell membrane. Inside the cell they bind the glucocorticoid receptor in the cytoplasm. The activated receptor-steroid complex then enters the nucleus and changes which genes are switched on and off.
The two ways they reduce inflammation:
- Switching off inflammatory genes (transrepression): the complex blocks transcription factors such as NF-kB and AP-1, so the cell makes fewer cytokines, fewer adhesion molecules, and less of the enzymes that drive inflammation.
- Switching on anti-inflammatory genes (transactivation): they increase production of proteins such as lipocortin (annexin A1), which inhibits phospholipase A2 and so reduces the release of arachidonic acid - the raw material for prostaglandins and leukotrienes.
The net effect is less inflammation, less immune activity, and less pain. Because the glucocorticoid receptor is present in almost every tissue, the same drug also affects bone, muscle, skin, blood vessels, glucose handling, and the immune system - which is exactly why the side-effect list is so long.
Effects on bone (the orthopaedic core):
- What the steroid does
- Reduce osteoblast number and activity and increase osteoblast and osteocyte apoptosis
- Result
- Less new bone is laid down - the dominant effect
- What the steroid does
- Increase osteoclast survival early on (partly via RANKL)
- Result
- More bone is removed, especially in the first months
- What the steroid does
- Reduce gut calcium absorption and increase urinary calcium loss
- Result
- A tendency to secondary hyperparathyroidism that further drives bone loss
- What the steroid does
- Cause osteocyte apoptosis that is cumulative and not repaired
- Result
- Loss of the bone's mechanosensors - a key step toward osteonecrosis
The osteocyte point is high-yield: unlike the gradual thinning of osteoporosis, osteocyte apoptosis is thought to disrupt the bone's ability to sense and repair damage, helping to explain why corticosteroids cause osteonecrosis and not just low bone density.
Agents, Potency and Routes
- Relative potency
- Low (short-acting)
- Typical use in or around orthopaedics
- Intravenous perioperative stress-dose cover; adrenal replacement
- Notes
- Has significant mineralocorticoid (salt-retaining) effect
- Relative potency
- Intermediate
- Typical use in or around orthopaedics
- Oral therapy for inflammatory arthritis and autoimmune disease
- Notes
- The standard oral maintenance steroid
- Relative potency
- Intermediate to high
- Typical use in or around orthopaedics
- Intra-articular and soft-tissue injection; intravenous pulses
- Notes
- Common depot injection agent
- Relative potency
- High
- Typical use in or around orthopaedics
- Intra-articular and soft-tissue injection (depot)
- Notes
- Widely used injectable; long local duration of action
- Relative potency
- Very high (long-acting)
- Typical use in or around orthopaedics
- Strong anti-inflammatory and anti-emetic uses; negligible salt retention
- Notes
- Most potent of the common agents, long duration
Relative anti-inflammatory potency runs dexamethasone greater than methylprednisolone greater than prednisolone greater than hydrocortisone. In general, the more potent and longer-acting agents have less mineralocorticoid (salt and water retaining) activity, which is why dexamethasone is favoured when fluid retention must be avoided.
Complications and How to Limit Them
- Who and when
- Long-term systemic use (most loss in first 3 to 6 months)
- What to do
- Assess fracture risk early, give calcium and vitamin D, add a bisphosphonate or other agent by risk
- Who and when
- High-dose or prolonged use; can follow short courses
- What to do
- New hip or groin pain - MRI even if the radiograph is normal; refer early
- Who and when
- Perioperative period in steroid-treated patients
- What to do
- Optimise where possible, watch wounds closely, low threshold to treat infection
- Who and when
- Long-term use, stopped abruptly or under surgical stress
- What to do
- Do not stop suddenly; give perioperative stress-dose cover
- Who and when
- Diabetics and after a steroid injection
- What to do
- Warn diabetics, monitor glucose around systemic dosing and injections
- Who and when
- Repeated local injection
- What to do
- Tendon weakening and skin or fat atrophy at the site - avoid injecting into a load-bearing tendon
Osteonecrosis of the Femoral Head
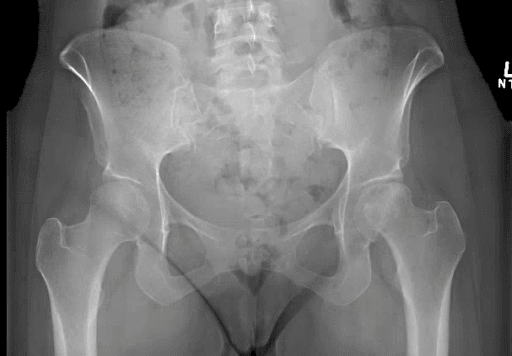
Corticosteroids are the most common cause of non-traumatic osteonecrosis, and the femoral head is the typical site. The bone dies through a combination of osteocyte apoptosis and impaired blood supply, the dead segment loses its ability to repair, and over time the subchondral bone collapses, leading to pain and secondary osteoarthritis. Early radiographs are often normal, so MRI is the key early investigation, and because the insult is systemic the disease is frequently bilateral.
New hip, groin, or thigh pain in a patient on (or recently on) corticosteroids is osteonecrosis until proven otherwise. A normal radiograph does not exclude it - request an MRI, and image both hips because the disease is often bilateral. Early disease (before collapse) may be amenable to joint-preserving surgery such as core decompression; collapse usually means arthroplasty.
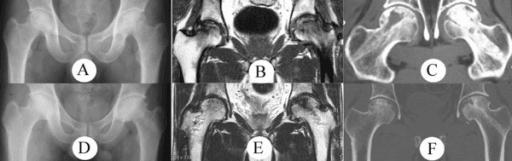
Staging the femoral head drives the joint-preserving-versus-arthroplasty decision and is a frequent viva follow-up. The classic Ficat and Arlet stages are:
- Stage 0 — normal radiograph and normal MRI (the asymptomatic "silent" at-risk hip, often the contralateral side).
- Stage I — radiograph normal but MRI positive (early marrow oedema and the characteristic double-line sign); the patient has pain.
- Stage II — radiographic change WITHOUT collapse — sclerosis and/or cysts, but the head is still spherical and the joint space preserved.
- Stage III — subchondral collapse: the crescent sign (a subchondral lucent fracture line) and/or flattening of the head, with the joint space still preserved.
- Stage IV — end-stage with head collapse, joint-space loss and secondary arthritis.
The watershed is the crescent sign / subchondral fracture (Stage III): before it, the head is intact and joint-preserving surgery (core decompression, with or without bone graft) can be offered; once the head has collapsed, arthroplasty is usually needed. The more modern ARCO system refines this with MRI and adds prognostic weight to the size and (especially lateral) location of the necrotic segment, which predict collapse.
Stopping and the Stress Response
A patient on long-term glucocorticoids has a suppressed adrenal axis and cannot mount the normal cortisol surge that surgery demands. Stopping suddenly, or operating without extra cover, can precipitate an adrenal crisis (hypotension, collapse). Continue the usual steroid, give perioperative stress-dose cover, and wean any long-term course gradually.
The topic keeps saying "give stress-dose cover" — examiners want the specifics.
- Who needs it: patients with a suppressed hypothalamic-pituitary-adrenal axis — conventionally those on more than about 5 mg/day of prednisolone (or equivalent) for longer than roughly three weeks, anyone with a cushingoid appearance, or a recent prolonged course. Patients on low doses or short courses usually need only their usual dose on the day.
- Graded by surgical stress (always continuing the patient's normal steroid):
- Minor surgery — the usual oral dose, with about 25 mg of hydrocortisone at induction if there is any concern.
- Moderate surgery — about 50 mg of hydrocortisone at induction, then roughly 25 mg every 8 hours for around 24 hours, then back to the usual dose.
- Major surgery — about 100 mg of hydrocortisone at induction, then of the order of 50 mg every 8 hours (or a continuous infusion) for 24 to 48 hours, tapering to the usual dose as the patient recovers.
- Recognise and treat adrenal crisis: hypotension unresponsive to fluids and vasopressors — give intravenous hydrocortisone immediately. Modern guidance also stresses that over-replacement is common, so match the cover to the surgical stress rather than reflexively giving very large doses.
Clinical Relevance
Corticosteroids run through every part of orthopaedic practice and the exam. In clinic they are the everyday injection for an osteoarthritic knee, a painful shoulder, or a trigger finger - so the indications, technique, and limits of intra-articular steroid are practical knowledge. In basic-science vivas the mechanism of action and the way steroids damage bone are classic questions. In trauma and arthroplasty the recognition of osteonecrosis of the femoral head and the management of a steroid-dependent patient (impaired healing, infection risk, and stress-dose cover) are common scenarios. Knowing when steroids help, what they damage, and how to use them safely is the core that examiners probe.
Guidelines, Registries and Global Practice
- Glucocorticoid-induced osteoporosis guidelines (for example the American College of Rheumatology, and equivalent guidance from NOGG in the UK and other national societies) agree on the core principles: assess fracture risk early, give calcium and vitamin D to all long-term users, and add an antifracture drug (oral bisphosphonate is the usual first choice) for those at moderate or higher risk, with anabolic agents reserved for the highest-risk patients.
- Osteoarthritis guidelines (for example AAOS and NICE) place intra-articular corticosteroid as an option for short-term symptom relief, not as disease-modifying treatment, reflecting trial evidence that the benefit is temporary and that repeated injection may harm cartilage.
- Where guidance differs is mainly the threshold for starting bone-protecting drugs and the place of newer anabolic agents, rather than any disagreement on the underlying harm of long-term steroids.
- Global practice variation largely reflects drug availability and cost (for example the choice between oral and intravenous bisphosphonates or anabolic agents) rather than differences in the principles of safe corticosteroid use.
Memory aids
BONESCorticosteroid Side Effects
Hook:Steroids hit the BONES - Bone loss, Osteonecrosis, Necrosis of healing, Endocrine effects, Soft tissue and muscle.
CUSHINGOIDCushingoid Picture of Long-Term Steroids
Hook:The long-term steroid patient looks CUSHINGOID - and the orthopaedic dangers are the bone ones: osteoporosis and osteonecrosis.
CLEANBefore You Inject a Joint
Hook:Keep it CLEAN before a steroid joint injection - Confirm, Look for infection, Explain, Aseptic, Note the limits.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient with rheumatoid arthritis is on long-term prednisolone. The examiner asks how corticosteroids work and what they do to bone.”
“A 35-year-old man who took high-dose steroids for a flare of inflammatory bowel disease six months ago now has several weeks of right groin pain, worse on weight-bearing. His hip radiograph is reported as normal. How do you proceed?”
Mechanism
- Bind cytoplasmic glucocorticoid receptor, alter gene transcription
- Switch off inflammatory genes; switch on anti-inflammatory proteins (lipocortin)
- Potent anti-inflammatory and immunosuppressive
- Affect almost every tissue - hence the wide side-effect list
Effects on Bone
- Reduce bone formation, increase early resorption - osteoporosis
- Most bone loss in the first 3 to 6 months
- Osteocyte apoptosis drives osteonecrosis
- Most common cause of non-traumatic osteonecrosis (femoral head, often bilateral)
Intra-Articular Use
- Short-term pain relief in osteoarthritis and soft-tissue conditions
- Repeated triamcinolone gave no pain benefit over saline at 2 years and more cartilage loss
- Strict aseptic technique; never inject a possibly septic joint
- Warn diabetics about a transient rise in glucose
Red Flags
- New hip or groin pain on steroids - MRI both hips for osteonecrosis
- Start bone protection early for courses of 3 months or more
- Give perioperative stress-dose cover; never stop long-term steroids abruptly
- Watch for impaired healing and infection after surgery
Evidence: Intra-Articular and Bone Effects
Every citation below has been checked against its source record in PubMed. The McAlindon RCT is why intra-articular steroid is a short-term, not a repeated long-term, treatment; the Weinstein review explains the osteocyte-apoptosis mechanism of osteonecrosis; and the ACR guideline sets the early, risk-matched approach to bone protection in long-term steroid users.
Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain (RCT)
- Two-year double-blind RCT, 140 patients with symptomatic knee osteoarthritis and ultrasound synovitis
- Triamcinolone 40mg every 12 weeks versus saline injection
- Triamcinolone caused significantly greater cartilage volume loss than saline (between-group difference about 0.11mm)
- There was no significant difference in knee pain between the two groups at 2 years
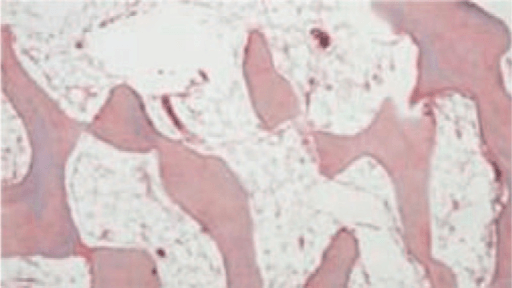
Glucocorticoid-Induced Osteonecrosis - Mechanism and Significance (Review)
- Glucocorticoids are the most common cause of non-traumatic osteonecrosis
- Osteonecrosis develops in roughly 9 to 40 percent of patients on long-term therapy and can follow short high-dose exposure or even intra-articular injection
- The primary lesion is osteocyte apoptosis - a cumulative, unrepairable defect - rather than a single vascular event
- This loss of osteocytes disrupts the bone's mechanosensing and leads to collapse of the femoral head
Preventing and Treating Glucocorticoid-Induced Osteoporosis (ACR Guideline)
- Applies to adults on glucocorticoids for more than 3 months at 2.5mg daily or more
- Strongly recommends early fracture-risk assessment (including bone density and FRAX where appropriate)
- Recommends calcium and vitamin D for all, with an antifracture drug (bisphosphonate, denosumab, or an anabolic agent) for those at medium to very high risk
- Anabolic agents are conditionally preferred as initial therapy for the highest-risk patients