Gout | Pseudogout (CPPD) | Tophi | Crystal Deposition
Crystalline Arthropathy Types
Critical Must-Knows
- Gout Crystals: Monosodium urate, negatively birefringent needles (yellow when parallel to polarizer).
- CPPD Crystals: Calcium pyrophosphate, positively birefringent rhomboids (blue when parallel).
- Tophaceous Gout: Chronic deposits in tendons/joints → nerve compression, erosions, skin breakdown.
- CPPD Wrist: Triangular fibrocartilage (TFCC) calcification classic finding on x-ray.
- Surgery Indications: Nerve compression (CTS), tendon rupture, skin ulceration, refractory pain.
Clinical Pearls
- "Negative birefringence = gout (urate needles)
- "Positive birefringence = CPPD (rhomboids)
- "Tophaceous gout: carpal tunnel syndrome common
- "CPPD: wrist TFCC calcification on x-ray
Clinical Imaging
Imaging Gallery




Critical Crystalline Arthropathy Exam Points
Crystal Identification
Joint aspiration with polarized light microscopy is diagnostic. Gout: negatively birefringent needle-shaped urate crystals (yellow when parallel). CPPD: positively birefringent rhomboid calcium pyrophosphate crystals (blue when parallel).
Tophaceous Gout Complications
Chronic tophi cause nerve compression, tendon rupture, skin ulceration, joint destruction. Carpal tunnel syndrome very common. Surgery indicated for nerve compression, tendon involvement, skin breakdown.
CPPD Wrist Involvement
Wrist is the most common hand site for CPPD. Triangular fibrocartilage (TFCC) calcification is classic x-ray finding (chondrocalcinosis). Can mimic other wrist arthropathies.
Medical Management First-Line
Optimize medical therapy before surgery. Acute attacks: NSAIDs, colchicine, steroids. Chronic gout: allopurinol/febuxostat to lower uric acid (target less than 6 mg/dL). Perioperative urate-lowering therapy essential.
Gout vs Pseudogout (CPPD)
| Feature | Gout (MSU) | Pseudogout (CPPD) | Key Difference |
|---|---|---|---|
| Crystal type | Monosodium urate (MSU) | Calcium pyrophosphate (CPP) | Chemical composition |
| Birefringence | Negative (yellow parallel) | Positive (blue parallel) | Polarized microscopy pattern |
| Crystal shape | Needle-shaped | Rhomboid/rectangular | Morphology under microscope |
| Classic joint (hand) | First MTP, MCP, wrist | Wrist (TFCC calcification) | Distribution pattern |
NYPDGout vs CPPD Crystal Identification
| N | Negatively birefringent Gout (monosodium urate crystals) |
| Y | Yellow when parallel Gout crystals appear yellow when parallel to polarizer |
| P | Positively birefringent Pseudogout (calcium pyrophosphate crystals) |
| D | bLue when parallel (D for CPPD) CPPD crystals appear blue when parallel to polarizer |
| N | Negatively birefringent Gout (monosodium urate crystals) | P | Positively birefringent Pseudogout (calcium pyrophosphate crystals) |
| Y | Yellow when parallel Gout crystals appear yellow when parallel to polarizer | D | bLue when parallel (D for CPPD) CPPD crystals appear blue when parallel to polarizer |
Hook:NYPD = Negative Yellow (gout), Positive bLue/D (CPPD) - remember crystal birefringence!
NSAIDGout Acute Attack Management
| N | NSAIDs First-line: indomethacin, naproxen (if no renal/GI contraindication) |
| S | Steroids Oral prednisone or intra-articular if NSAIDs contraindicated |
| A | Aspiration Joint aspiration relieves pain and confirms diagnosis |
| I | Ice and rest Symptomatic relief during acute attack |
| D | Do NOT start allopurinol Don't start urate-lowering during acute attack (worsens flare) |
| N | NSAIDs First-line: indomethacin, naproxen (if no renal/GI contraindication) | I | Ice and rest Symptomatic relief during acute attack |
| S | Steroids Oral prednisone or intra-articular if NSAIDs contraindicated | D | Do NOT start allopurinol Don't start urate-lowering during acute attack (worsens flare) |
| A | Aspiration Joint aspiration relieves pain and confirms diagnosis |
Hook:NSAID = management of acute gout attack - but don't start allopurinol during flare!
TENTSTophaceous Gout Surgical Indications
| T | Tendon rupture Tophus weakens tendons (extensor/flexor) → rupture |
| E | Erosive arthropathy Joint destruction, severe arthritis |
| N | Nerve compression Carpal tunnel syndrome, ulnar nerve compression |
| T | Tophus ulceration Skin breakdown, infection risk |
| S | Severe pain refractory Failed medical management, intractable pain |
| T | Tendon rupture Tophus weakens tendons (extensor/flexor) → rupture | T | Tophus ulceration Skin breakdown, infection risk |
| E | Erosive arthropathy Joint destruction, severe arthritis | S | Severe pain refractory Failed medical management, intractable pain |
| N | Nerve compression Carpal tunnel syndrome, ulnar nerve compression |
Hook:TENTS = indications for surgical tophus excision in chronic gout!
Overview and Epidemiology
Crystalline Arthropathy is joint inflammation from crystal deposition: monosodium urate (gout) or calcium pyrophosphate (CPPD/pseudogout).
Gout Epidemiology
Prevalence:
- 4% general population (increasing)
- Male greater than female (3:1)
- Peak onset: 40-60 years (men), post-menopausal (women)
Risk Factors:
- Hyperuricemia (uric acid greater than 7 mg/dL)
- Obesity, metabolic syndrome
- Alcohol (beer), purine-rich diet (red meat, seafood)
- Diuretics, chronic kidney disease
- Family history
Classic site: First MTP (podagra).
CPPD Epidemiology
Prevalence:
- 5-10% in elderly (over 65 years)
- Equal male:female
- Age-related: prevalence increases with age
Risk Factors:
- Advanced age (over 60 years)
- Osteoarthritis
- Hyperparathyroidism, hemochromatosis
- Hypomagnesemia, hypophosphatasia
- Prior joint trauma
Wrist is most common hand site.
Hand Involvement:
- Gout: 10-15% present with hand involvement (wrist, MCP, PIP, DIP)
- CPPD: Wrist most common hand site (TFCC calcification)
Pathophysiology
Crystal-Induced Inflammation
Both gout and CPPD cause acute inflammatory arthritis from crystal deposition. Crystals are phagocytosed by neutrophils → inflammatory cascade → intense pain, swelling, erythema (mimics septic arthritis). Joint aspiration with crystal identification is diagnostic.
Gout (Monosodium Urate) Pathophysiology:
- Hyperuricemia: Uric acid greater than 7 mg/dL (overproduction or underexcretion)
- Crystal Formation: Urate crystals precipitate in synovial fluid/tissue (lower temperature in extremities)
- Acute Attack: Crystals trigger inflammatory response (neutrophil activation, IL-1β release)
- Chronic Tophaceous Phase: Persistent hyperuricemia → tophus formation (aggregates of urate crystals with granulomatous reaction)
- Joint/Tendon Damage: Tophi erode bone, weaken tendons, compress nerves, ulcerate skin
Tophus Composition: Chalky white monosodium urate deposits surrounded by foreign body giant cells
CPPD (Calcium Pyrophosphate Deposition) Pathophysiology:
- Pyrophosphate Accumulation: Abnormal cartilage metabolism (age-related, genetic, metabolic)
- Crystal Deposition: Calcium pyrophosphate crystals deposit in cartilage (chondrocalcinosis)
- Acute Pseudogout: Crystal shedding into joint → acute inflammatory attack
- Chronic CPPD Arthropathy: Progressive cartilage/bone damage (OA-like pattern)
TFCC calcification in wrist is classic for CPPD.
Hand Sites:
| Condition | Common Hand/Wrist Sites |
|---|---|
| Gout | Wrist, first MCP (thumb), finger MCPs, PIPs, DIPs |
| Tophaceous Gout | Finger pulps, extensor tendons, olecranon bursa, carpal tunnel |
| CPPD/Pseudogout | Wrist (TFCC, radiocarpal), MCPs (less common) |
Clinical Presentation
Acute Gouty Arthritis
Classic Presentation:
- Sudden onset severe joint pain (often overnight, wakes patient)
- Monoarticular initially (can be polyarticular in recurrent attacks)
- Red, hot, swollen joint (mimics septic arthritis)
- Exquisitely tender - cannot tolerate touch, sheets
- Self-limited: Resolves in 7-10 days without treatment
Hand Manifestations:
- Wrist, MCP, PIP, DIP involvement
- Swelling and erythema
- Reduced ROM from pain
Triggers:
- Alcohol binge (beer)
- Dehydration
- Acute illness, surgery
- Starting allopurinol (paradoxical flare)
Podagra (First MTP): Classic presentation (70% of first attacks), but hand joints also common.
Examination
Inspection:
- Erythema, edema over affected joint
- Shiny, tense skin
- May have visible tophi (chronic cases)
Palpation:
- Marked tenderness (patient withdraws)
- Warmth
- Joint effusion
ROM: Severely limited by pain
Differential: Septic arthritis - must rule out with joint aspiration!
Medical Management
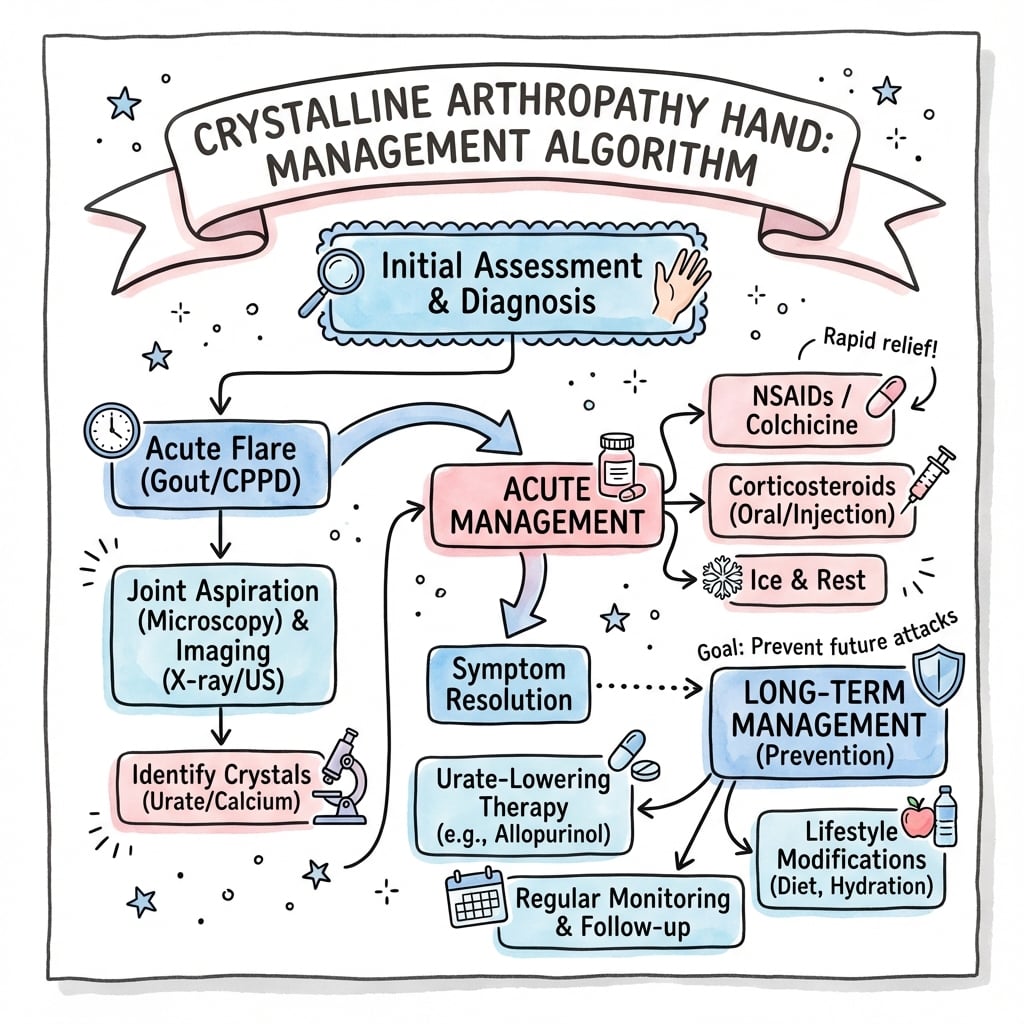
Acute Gout/Pseudogout Management
Goals: Reduce inflammation and pain rapidly
First-Line Therapy:
1. NSAIDs:
- Indomethacin 50mg TID or naproxen 500mg BID
- Start immediately at diagnosis
- Continue until attack resolves (7-10 days)
- Contraindications: Renal impairment, GI bleeding history, anticoagulation
2. Colchicine:
- Low-dose regimen: 1.2mg loading dose, then 0.6mg 1 hour later, then 0.6mg daily
- Effective if started early (within 24-48 hours)
- Side effects: Diarrhea, GI upset (dose-dependent)
- Contraindications: Severe renal/hepatic impairment
3. Corticosteroids:
- Intra-articular: Triamcinolone 10-40mg (if monoarticular, septic arthritis ruled out)
- Oral prednisone: 30-40mg daily for 5 days, then taper
- IM/IV methylprednisolone: If unable to take oral (hospitalized patients)
- Use if NSAIDs/colchicine contraindicated
Supportive Care:
- Rest and elevate affected joint
- Ice application
- Avoid weight-bearing if lower extremity
DO NOT:
- Start allopurinol/febuxostat during acute attack (worsens flare)
- Start urate-lowering therapy until attack resolves (wait 2-4 weeks)
Surgical Management
Surgical Indications in Crystalline Arthropathy
Gout:
| Indication | Surgical Procedure |
|---|---|
| Carpal tunnel syndrome | Carpal tunnel release + tophus excision |
| Tendon rupture (extensor/flexor) | Tendon repair/reconstruction + tophus removal |
| Skin ulceration/draining tophus | Tophus excision, wound closure/skin graft |
| Nerve compression (ulnar, radial) | Nerve decompression + tophus excision |
| Severe erosive arthropathy | Arthroplasty or arthrodesis |
| Cosmetically unacceptable tophi | Tophus excision (elective) |
CPPD:
- Usually non-operative
- Severe wrist arthritis: Proximal row carpectomy, wrist fusion, or arthroplasty
Principle: Optimize medical management (ULT for gout) before elective surgery. Perioperative uric acid control reduces wound complications.
Complications and Outcomes
Complications of Tophaceous Gout Surgery
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Wound dehiscence | 10-20% | Optimize uric acid control pre-op, meticulous closure, avoid tension |
| Infection | 5-10% | Sterile technique, antibiotics if signs of infection, continue ULT |
| Tendon rupture | 5% | Gentle dissection, preserve tendon, may need repair/reconstruction |
| Nerve injury | Less than 5% | Careful dissection if tophus adherent to nerve |
| Recurrence of tophus | 5-10% | Adequate ULT post-op (uric acid less than 6 mg/dL) |
Wound Dehiscence:
- Most common complication (10-20%)
- Mechanism: Gout impairs wound healing, skin often friable/atrophic from chronic tophus
- Prevention: Optimize uric acid control 3-6 months pre-op, avoid skin tension, delayed closure if needed
- Management: Local wound care, secondary intention healing, delayed closure/skin graft if large
Infection:
- Higher risk than standard hand surgery (5-10%)
- Draining tophi may be colonized
- Management: Antibiotics (cover Staph aureus), debridement if abscess, continue ULT
Outcomes:
- CTS with tophus excision: 80-90% symptom improvement
- Tophus excision for skin breakdown: Wound healing in 70-80% (delayed healing common)
- Recurrence: 5-10% if inadequate uric acid control post-op
Key to Success: Perioperative and long-term uric acid control with ULT (allopurinol/febuxostat). Target less than 6 mg/dL.
Evidence Base
- Data-driven classification criteria; MSU crystals in symptomatic joint/bursa or tophus is a sufficient criterion (no further scoring needed)
- Clinical, laboratory and imaging (ultrasound double-contour sign, urate on dual-energy CT, radiographic erosion) domains
- Overall sensitivity 92% and specificity 89%
- Developed when MSU crystal identification was the diagnostic gold standard
- Strong recommendation to start urate-lowering therapy for tophaceous gout, radiographic damage, or frequent flares
- Allopurinol preferred first-line ULT, including in moderate-to-severe CKD (stage 3 or higher)
- Treat-to-target strategy with serum urate target under 6 mg/dL (under 0.36 mmol/L)
- Anti-inflammatory flare prophylaxis for at least 3 to 6 months when starting ULT
- Multicentre randomised non-inferiority trial; 6128 gout patients aged 60+ with a CV risk factor
- Febuxostat non-inferior to allopurinol for the composite CV endpoint (adjusted HR 0.85, 95% CI 0.70 to 1.03)
- No increase in all-cause death or serious adverse events with febuxostat
- Tempered the cardiovascular signal previously raised by the CARES trial
- Ten studies pooled; person-based sensitivity 0.81 and specificity 0.91 for diagnosing gout
- Joint-based sensitivity 0.83 and specificity 0.88
- Sensitivity falls to ~0.55 in recent-onset gout (6 weeks or less)
- DECT most useful in established disease, not early presentation
- 12 patients, 24 periarticular tophi excised from MCP/IP joints (some wrist and elbow), all on urate-lowering therapy
- Restoration of tendon excursion and joint mobility in all patients
- No wound complications and no recurrence over follow-up up to 15 years
- Highlights that meticulous technique plus medical urate control optimises results
- Age-standardised prevalence in adults 65+ was ~3111 per 100,000 in 2021
- Disease burden in older men nearly twice that of women
- Burden projected to rise further by 2050, driven by ageing and metabolic risk
- Greatest increases in high-SDI/high-income regions
Controversies & Areas of Uncertainty
Timing of Surgery vs Medical Optimisation
The conventional teaching is to optimise serum urate (under 6 mg/dL) for 3-6 months before elective tophus excision. However, severe carpal tunnel syndrome with motor signs or an ulcerated/infected tophus mandates earlier surgery. There is no high-level evidence defining the exact urate threshold or duration that minimises wound complications - practice is extrapolated from case series.
Extent of Tophus Excision
Whether to aggressively debulk all tophus material (risking tendon/nerve injury and large soft-tissue defects) or to perform conservative decompression remains debated. Some series report excellent function with en masse excision and no recurrence; others favour limited removal relying on ULT to resolve residual deposits over time.
Febuxostat Cardiovascular Safety
The CARES trial signalled increased CV/all-cause mortality, but the larger FAST trial found non-inferiority to allopurinol. The discordance (open-label design, differing discontinuation rates, populations) leaves residual uncertainty, and febuxostat is still used cautiously in established CV disease.
Imaging vs Aspiration for Diagnosis
DECT and ultrasound (double-contour sign) are increasingly used, but sensitivity is low in early gout and a negative scan cannot exclude disease. Crystal identification on aspiration remains the reference standard; over-reliance on imaging risks missing both early gout and coexistent septic arthritis.
Unresolved questions:
- No disease-modifying therapy exists for CPPD - management remains symptomatic, and no agent reliably dissolves calcium pyrophosphate deposits.
- Optimal reconstruction after tophus-related tendon rupture (primary repair vs graft vs transfer) is not standardised.
- Whether to treat asymptomatic hyperuricaemia to prevent crystal arthropathy is not supported by current guidelines.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute Gout Attack
"A 55-year-old man presents with sudden onset severe pain and swelling in his right wrist. The wrist is red, hot, and exquisitely tender. He cannot move it. He has a history of gout affecting his great toe. What is your diagnosis and initial management?"
Scenario 2: Carpal Tunnel Syndrome in Tophaceous Gout
"A 60-year-old man with long-standing gout presents with progressive numbness in his thumb, index, and middle fingers. He has visible chalk-like deposits on his fingers and wrist. EMG shows severe carpal tunnel syndrome. His uric acid is 9 mg/dL despite allopurinol. What is your management?"
Scenario 3: CPPD vs Gout Differentiation
"A 70-year-old woman presents with acute wrist pain and swelling. X-ray shows calcification in the triangular fibrocartilage. You aspirate the joint and see rhomboid-shaped crystals under polarized microscopy. They appear blue when parallel to the polarizer. What is your diagnosis and management?"
Guidelines, Registries & Global Practice
Global Epidemiology:
- Gout is the most common inflammatory arthritis worldwide; prevalence is rising with ageing populations and metabolic syndrome
- Age-standardised prevalence in adults 65+ was ~3,100 per 100,000 (GBD 2021), with burden in older men nearly double that of women and projected to keep rising to 2050
- Marked ethnic variation: highest prevalence in Māori and Pacific Island populations of Oceania (genetic urate transporter variants); lower rates historically reported in parts of Africa and East Asia
- Hand/wrist involvement complicates roughly 10-15% of established gout; CPPD prevalence rises steeply with age
Side-by-Side Guidelines:
| Body | Diagnosis | First-line ULT | Serum urate target | Notable position |
|---|---|---|---|---|
| ACR (US, 2020) | MSU crystals; supports DECT/US when aspiration unavailable | Allopurinol (incl. CKD), low-dose start | under 6 mg/dL, treat-to-target | Strong: ULT for tophi/erosions/frequent flares; prophylaxis 3-6 months |
| EULAR (Europe) | Crystal confirmation preferred; imaging adjuncts | Allopurinol, titrate to target | under 6 mg/dL (under 5 for severe/tophaceous) | Endorses treat-to-target and patient education |
| BSR/BOA (UK) | Clinical plus crystal/imaging | Allopurinol first-line | under 6 mg/dL (under 5 for tophi) | Emphasises ULT offered to all after a diagnosis is confirmed |
| ACR/EULAR (2015 criteria) | Classification: clinical + lab + imaging | n/a (classification) | n/a | Sensitivity 92%, specificity 89% |
Registry & Evidence Notes:
- No dedicated arthroplasty registry stratum exists for crystalline hand arthropathy; surgical evidence is limited to case series, so consent must reflect this
- Pharmacovigilance data (FAST trial, EU regulator-mandated) reshaped febuxostat cardiovascular guidance globally
High- vs Limited-Resource Practice Variation:
- High-resource: ready access to polarised microscopy, DECT, biologic uricase (pegloticase) for refractory tophaceous disease, and elective hand surgery
- Limited-resource: diagnosis often clinical; allopurinol remains the affordable backbone; DECT and pegloticase frequently unavailable; patients may present later with advanced tophaceous deformity requiring surgery
- Universal priorities: confirm crystals where possible, rule out septic arthritis, and achieve sustained serum urate under 6 mg/dL before and after any surgery
Medicolegal / Consent Essentials:
- Document joint aspiration and crystal analysis before committing to a diagnosis
- Always exclude septic arthritis (Gram stain, culture) - a missed joint sepsis is a key litigation risk
- Consent for tophus excision must cover wound dehiscence (10-20%), infection (5-10%), possible skin graft, and recurrence if urate control fails
CRYSTALLINE ARTHROPATHY - HAND
Clinical summary
Crystal Types
- •Gout: Monosodium urate (MSU)
- •CPPD: Calcium pyrophosphate (CPP)
- •Birefringence distinguishes them
- •Joint aspiration is diagnostic
Crystal Identification
- •Gout: Negatively birefringent needles (yellow parallel)
- •CPPD: Positively birefringent rhomboids (blue parallel)
- •Polarized light microscopy essential
- •NYPD mnemonic: Negative Yellow, Positive bLue/D
Acute Gout Attack
- •Sudden severe pain, red/hot/swollen joint
- •Wrist, MCP, PIP involvement possible
- •Mimics septic arthritis (must rule out)
- •Self-limited 7-10 days
Acute Management
- •NSAIDs: Indomethacin, naproxen (first-line)
- •Colchicine: 1.2mg load, 0.6mg 1h later, 0.6mg daily
- •Steroids: Intra-articular or oral if NSAID contraindicated
- •Do NOT start allopurinol during attack
Chronic Gout (ULT)
- •Allopurinol 100-800mg daily (first-line)
- •Febuxostat 40-80mg (alternative)
- •Target: Uric acid less than 6 mg/dL (less than 5 for tophi)
- •Colchicine prophylaxis 3-6 months during ULT start
Tophaceous Gout
- •Chalky white deposits in joints/tendons
- •Complications: CTS, tendon rupture, skin ulceration
- •Punched-out erosions on x-ray (rat-bite)
- •Surgery for nerve compression, skin breakdown
Surgical Indications
- •Carpal tunnel syndrome (most common)
- •Tendon rupture (extensor/flexor)
- •Skin ulceration/draining tophus
- •Nerve compression (median, ulnar)
- •Severe erosive arthropathy
CTR in Tophaceous Gout
- •Standard CTR + tophus excision
- •Dissect tophi off median nerve carefully
- •Debulk extensively, irrigate
- •Wound dehiscence risk 10-20%
- •Continue ULT perioperatively
Tophus Excision Complications
- •Wound dehiscence: 10-20%
- •Infection: 5-10%
- •Tendon rupture: 5%
- •Nerve injury: Less than 5%
- •Recurrence: 5-10% if poor uric acid control
CPPD / Pseudogout
- •Wrist most common hand site
- •TFCC calcification (chondrocalcinosis) on x-ray
- •Acute: NSAIDs, colchicine, steroids
- •No disease-modifying therapy (no ULT equivalent)
Imaging
- •Gout: Punched-out erosions, overhanging edges
- •CPPD: Chondrocalcinosis (TFCC calcification)
- •Ultrasound: Double contour sign (gout)
- •X-ray normal in early gout
Exam Pearls
- •Rule out septic arthritis (joint aspiration mandatory)
- •Negative birefringence = gout (yellow parallel)
- •Positive birefringence = CPPD (blue parallel)
- •CTS in tophaceous gout: CTR + tophus excision
- •Target uric acid less than 6 mg/dL with ULT