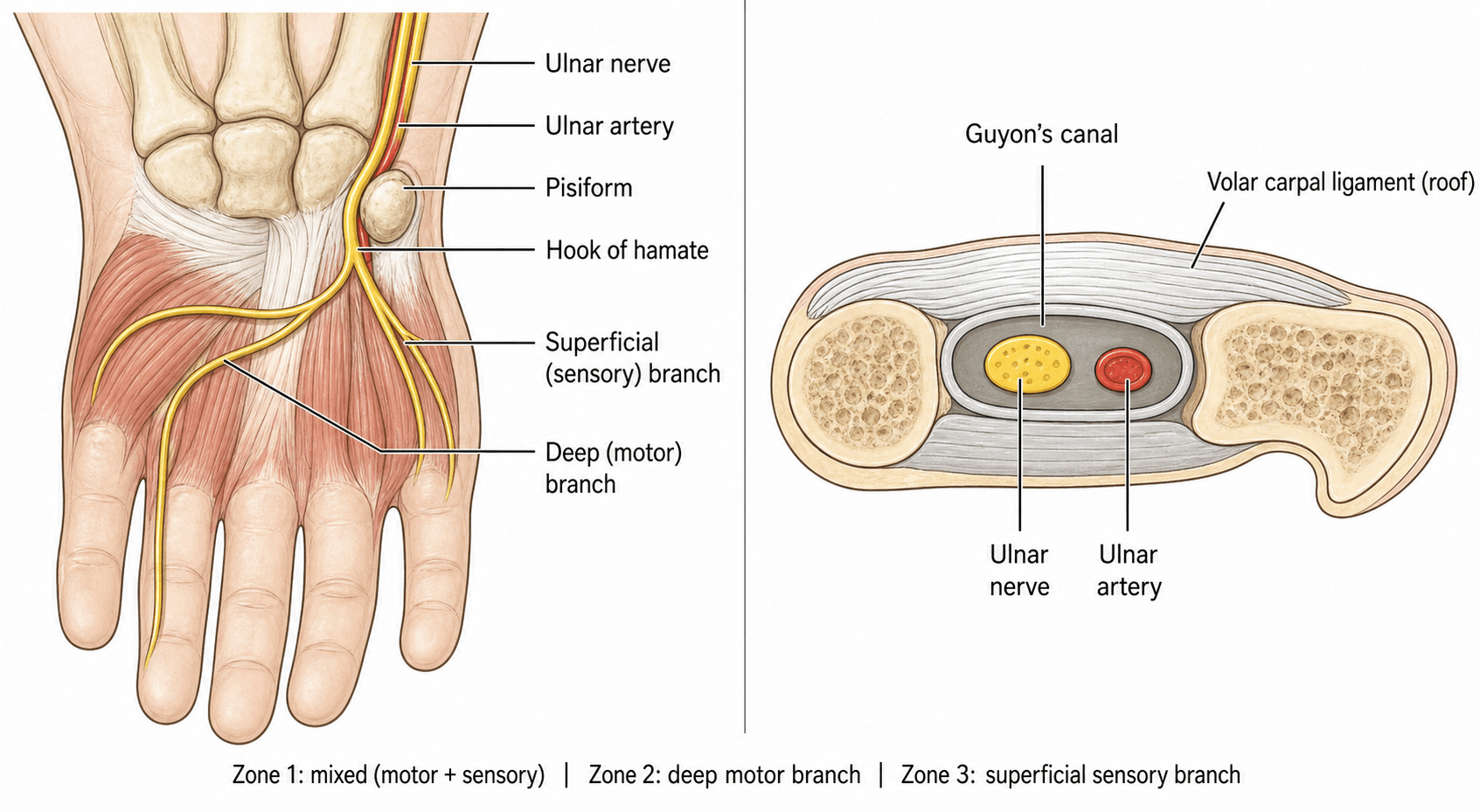
Guyon's Canal Compression | Ulnar Nerve at Wrist | Zone-Specific Deficits
- Guyon's Canal Boundaries: Floor = pisiform/hamate/pisohamate ligament, Roof = palmaris brevis + palmar carpal ligament
- Zone 2 = Pure Motor Deficit: Most common presentation (50%) - weakness with NORMAL sensation
- Ganglion Cyst = #1 Cause: 85-90% of Zone 2 compression from ganglion arising from pisotriquetral joint
- Hook of Hamate Fracture: Classic cause - cyclists, golfers - palpate for tenderness
- NO Froment's Sign: Adductor pollicis supplied BEFORE Guyon's canal - Froment's indicates proximal ulnar lesion
- “Zone 2 compression = interosseous weakness WITHOUT sensory loss (DDx from CuTS)
- “Ganglion cyst most common space-occupying lesion in Guyon's
- “Hook of hamate fracture = missed on standard radiographs, need carpal tunnel view or CT
- “Guyon's vs cubital tunnel: Guyon's has normal Froment's sign (adductor spared)
MUST know Shea-McClain zones:
- Zone 1: Before bifurcation (motor + sensory)
- Zone 2: Deep motor branch (pure motor)
- Zone 3: Superficial branch (pure sensory)
Zone determines clinical presentation!
Interosseous weakness WITHOUT sensory loss
This is pathognomonic for Zone 2 compression. Differentiates from cubital tunnel syndrome.
Ganglion cyst most common cause.
Froment's NEGATIVE in Guyon's compression
Adductor pollicis nerve branches BEFORE Guyon's canal. Positive Froment's = proximal lesion (elbow or above).
Critical for localization!
- Guyon's Canal (Wrist)
- Ulnar tunnel at wrist
- Cubital Tunnel (Elbow)
- Cubital tunnel at elbow
- Clinical Significance
- Physical examination localization
- Guyon's Canal (Wrist)
- NEGATIVE (adductor spared)
- Cubital Tunnel (Elbow)
- POSITIVE (adductor weak)
- Clinical Significance
- Key differentiating feature
- Guyon's Canal (Wrist)
- Hypothenar only (Zone 1/3)
- Cubital Tunnel (Elbow)
- Hypothenar + ulnar 1.5 digits
- Clinical Significance
- Dorsal ulnar cutaneous spared in Guyon's
- Guyon's Canal (Wrist)
- Ganglion cyst, hamate fracture
- Cubital Tunnel (Elbow)
- Chronic pressure, anatomic
- Clinical Significance
- Imaging often diagnostic in Guyon's
Overview
Ulnar Tunnel Syndrome (Guyon's Canal Syndrome) is compression of the ulnar nerve at the wrist within the fibro-osseous tunnel formed by the pisiform, hook of hamate, and overlying soft tissues.
Unlike cubital tunnel syndrome, it presents WITHOUT elbow symptoms and with zone-specific motor/sensory deficits.
Essential Features:
- Rare compared to carpal tunnel and cubital tunnel syndromes
- Zone-dependent presentation (motor, sensory, or mixed)
- Ganglion cyst most common cause (85-90%)
- Negative Froment's sign differentiates from cubital tunnel
- 90% surgical success rate
Anatomy and Pathophysiology
Anatomical Boundaries
Guyon's canal (ulnar tunnel) is a fibro-osseous tunnel at the wrist where the ulnar nerve enters the hand.
- Palmaris brevis muscle
- Palmar carpal ligament (volar carpal ligament)
- Skin and subcutaneous tissue
- Pisiform bone (ulnar)
- Hook of hamate (radial)
- Pisohamate ligament
- Transverse carpal ligament (deeper)
- Pisiform bone
- Flexor carpi ulnaris tendon
- Hook of hamate
- Flexor digitorum superficialis tendons
- Ulnar nerve (divides within canal)
- Ulnar artery (radial to nerve)
- Ulnar veins
- Deep motor branch: Curves around hook of hamate into palm
- Superficial sensory branch: Continues distally to supply hypothenar and ulnar 1.5 digits
Canal length approximately 4cm.
The ulnar nerve bifurcates into deep motor and superficial sensory branches within Guyon's canal. This anatomical fact explains zone-specific presentations - compression can affect trunk (Zone 1), motor branch alone (Zone 2), or sensory branch alone (Zone 3).
Classification
Shea-McClain Classification (1969)
- Location
- Before bifurcation
- Motor
- All intrinsics weak
- Sensory
- Hypothenar + ulnar 1.5 digits
- Cause
- Ganglion, fracture, aneurysm
- Location
- Deep motor branch
- Motor
- All intrinsics weak
- Sensory
- NORMAL (no sensory loss)
- Cause
- Ganglion (85-90%)
- Location
- Superficial sensory
- Motor
- NORMAL (no weakness)
- Sensory
- Hypothenar + ulnar 1.5 digits
- Cause
- Ulnar artery pathology
Key Points:
- Zone 2 is most common (50% of cases)
- Zone 2 = Pure motor = Pathognomonic presentation
- Zone determines imaging and surgical approach
Clinical Presentation and Diagnosis
Clinical Assessment
- Onset (acute vs gradual)
- Hand dominance and occupation
- Trauma history (fall on hand, hook of hamate fracture)
- Cycling, tool use, wheelchair use
- Palpable mass in hypothenar region
- Weakness vs numbness (zone localization)
- Zone 1: Motor weakness + hypothenar numbness
- Zone 2: Motor weakness ONLY (no sensory symptoms)
- Zone 3: Hypothenar numbness ONLY (no weakness)
Physical Examination
- Hypothenar wasting (Zone 1 or 2)
- Interosseous wasting (dorsal hand)
- Claw deformity of ring/small fingers
- Visible or palpable mass
- Hook of hamate tenderness (fracture)
- Palpable ganglion cyst (may be subtle)
- Tinel's sign over Guyon's canal
- Allen's test (ulnar artery patency)
- Interosseous function: Finger spread/adduction (Wartenberg's sign)
- Froment's sign: Should be NEGATIVE (adductor spared)
- Hypothenar strength: Abduction and opposition of small finger
- FCU and FDP ring/small: Should be normal (localize to wrist)
- Hypothenar eminence (superficial branch)
- Ulnar 1.5 digits palmar surface (small finger + ulnar ring)
- Dorsal ulnar cutaneous: Should be NORMAL (branches proximal to wrist)
- Hypothenar Wasting
- Present
- Interosseous Wasting
- Present
- Hypothenar Numbness
- Present
- Froment's Sign
- Negative
- Hypothenar Wasting
- Present
- Interosseous Wasting
- Present
- Hypothenar Numbness
- Absent
- Froment's Sign
- Negative
- Hypothenar Wasting
- Absent
- Interosseous Wasting
- Absent
- Hypothenar Numbness
- Present
- Froment's Sign
- Negative
The Riche-Cannieu anastomosis is a common communication in the palm between the deep motor branch of the ulnar nerve and the recurrent (thenar) motor branch of the median nerve. Because it shifts motor supply across the usual median/ulnar boundary in the hand, the motor findings of a distal (Guyon's) ulnar lesion can be atypical and may not match the sensory pattern. Where ulnar-territory intrinsics receive median fibres through the anastomosis, intrinsic weakness can be milder than expected despite genuine compression; in the "all-ulnar hand" the thenar muscles are ulnar-innervated, so a Guyon's lesion can add unexpected thumb (thenar) weakness. A coexisting forearm Martin-Gruber anastomosis (median fibres crossing into the ulnar nerve, producing an "all-median hand") can further mask intrinsic loss. The practical message: when the motor deficit does not fit the sensory deficit or the imaging, suspect a crossover anastomosis and interpret nerve conduction studies with this anatomy in mind.
Investigations
Essential Investigations Summary
- Indication
- All patients
- Key Findings
- Hook of hamate fracture, arthritis
- Indication
- Suspected hamate fracture
- Key Findings
- Gold standard for bony pathology
- Indication
- Soft tissue mass suspected
- Key Findings
- Ganglion cyst, nerve pathology
- Indication
- All surgical candidates
- Key Findings
- Confirms level, severity, prognosis
Mandatory Before Surgery:
- NCS confirms wrist-level slowing (not elbow)
- Imaging to identify treatable cause
Management

Non-Operative Management
- Mild symptoms, short duration (less than 3 months)
- No muscle wasting
- Idiopathic (no mass lesion on imaging)
- Occupational cause with modifiable activity
- Avoid repetitive hypothenar pressure
- Padded gloves for cyclists
- Ergonomic tool handles
- Wheelchair cushion padding
- Wrist splint in neutral position
- Night splint (6-8 weeks)
- Reduces pressure in Guyon's canal
- Evidence limited but low risk
- Short course (2-4 weeks)
- Anti-inflammatory effect
- Minimal evidence for nerve compression
- Nerve gliding exercises
- Strengthening when symptoms improve
- No evidence for benefit but commonly prescribed
- 30-40% improve with conservative treatment
- Best results in idiopathic, occupational causes
- Poor results if ganglion or structural lesion present
Surgical indications: (1) Progressive motor weakness, (2) Muscle atrophy present, (3) Mass lesion identified on imaging, (4) No improvement after 3 months conservative treatment, (5) Acute onset with severe deficit.
Steroid injection NOT recommended for Guyon's canal syndrome. Unlike carpal tunnel, injection into confined space near ulnar artery is risky. May damage nerve or artery. Not supported by evidence.
Surgical Technique
Guyon's Canal Decompression Summary
- Supine, arm on hand table
- Tourniquet, hand supinated
- Loupe magnification recommended
- Longitudinal along ulnar hypothenar border
- 1cm proximal to wrist crease, 3-4cm distally
- Identify ulnar artery (RADIAL to nerve) - protect first
- Identify ulnar nerve
- Follow nerve to bifurcation
- Release all three zones as needed
- Excise ganglion/pathology to origin
Complications and Special Situations
Problems and Management
Intraoperative Complications:
Most serious complication (1-2%)
Prevention:
- Careful identification of artery before nerve decompression
- Ulnar artery is RADIAL to nerve
- Use loupe magnification
- Avoid monopolar cautery near artery
Management:
- Primary repair with 8-0 or 9-0 suture
- May need microvascular expertise
- Ligation as last resort (risk hypothenar ischemia)
Superficial sensory branch most at risk
Prevention:
- Identify all branches before division
- Protect palmar cutaneous branch in subcutaneous tissue
- Careful dissection of bifurcation
Management:
- Primary repair if recognized
- Neuroma excision if symptomatic later
- May cause permanent sensory deficit
Early Postoperative (0-6 weeks):
-
Hematoma (2-3%): Risk near ulnar artery
- Prevention: Meticulous hemostasis, consider drain
- Management: Evacuate if symptomatic, compressive dressing
-
Infection (less than 1%): Rare with clean technique
- Antibiotics, washout if severe
- Risk to nerve recovery if deep
-
Wound dehiscence: Incision in mobile area of palm
- Prevention: Careful closure, immobilize 1-2 weeks
- Management: Local wound care, may need re-closure
Late Complications (greater than 6 weeks):
- Incidence
- 10-20%
- Prevention
- Early surgery (less than 6 months symptoms)
- Treatment
- Tendon transfers if severe
- Incidence
- 5-10%
- Prevention
- Complete excision to joint origin
- Treatment
- Revision excision
- Incidence
- 5%
- Prevention
- Protect palmar cutaneous nerve
- Treatment
- Scar massage, desensitization
- Incidence
- 10-15%
- Prevention
- Less aggressive retinaculum release
- Treatment
- Therapy, usually resolves by 3 months
Ulnar artery injury or ligation can cause hypothenar ischemia, especially if palmar arch incomplete. Always assess Allen's test preoperatively. If abnormal, ulnar artery must be preserved. Consider vascular surgery consultation if injured.
Postoperative Care
Rehabilitation Protocol
Week 0-2: Protection
- Bulky soft dressing
- Finger ROM exercises immediately
- Suture removal 10-14 days
Week 2-6: Active Motion
- Remove splint, active wrist ROM
- Light ADLs permitted
- Avoid forceful gripping
Week 6-12: Strengthening
- Progressive grip strengthening
- Return to light duty work
- Sport-specific training begins
Outcomes
Outcome Summary
- Symptom duration less than 6 months
- No preoperative atrophy
- Identifiable and removable cause (ganglion)
- Younger patient age
- Symptom duration greater than 12 months
- Severe muscle wasting
- Axonal loss on NCS
- Chronic arthritis or fibrosis
Guidelines, Registries & Global Practice
Global Epidemiology
Ulnar tunnel syndrome is an uncommon, well-described entity that is substantially rarer than both carpal tunnel and cubital tunnel syndrome, and it is frequently mis-diagnosed because its symptoms overlap with carpal tunnel syndrome, cubital tunnel syndrome, thoracic outlet syndrome, C8-T1 radiculopathy and peripheral neuropathy (Chen & Tsai, J Hand Surg Am 2014, DOI; Bachoura & Jacoby, Orthop Clin North Am 2012, DOI). The hook of hamate fracture - a classic structural cause - is itself uncommon with an unclear true prevalence and is often diagnosed late (Tian & Goldfarb, Hand Clin 2021, DOI). Vascular causes such as hypothenar hammer syndrome arise in people who repeatedly use the hypothenar eminence as a hammer (Schröttle et al, Vasa 2015, DOI).
- Stance Relevant to Ulnar Tunnel Syndrome
- Electrodiagnostic confirmation and targeted imaging (MRI/US for mass, CT for hook) before decompression; surgery for confirmed compressive or structural lesion
- Evidence Level
- Expert consensus / Level V
- Stance Relevant to Ulnar Tunnel Syndrome
- Localise lesion clinically and electrophysiologically; exclude proximal (elbow) ulnar neuropathy first; decompression for structural cause or failed conservative care
- Evidence Level
- Expert consensus / Level V
- Stance Relevant to Ulnar Tunnel Syndrome
- Zone-based (Shea-McClain) assessment guides exploration; address underlying cause (ganglion excision, hook excision, vascular repair)
- Evidence Level
- Expert consensus / Level V
- Stance Relevant to Ulnar Tunnel Syndrome
- No high-level RCT evidence; management driven by cause-specific case series and anatomical principles
- Evidence Level
- Level IV-V
- Contribution
- Defining three-zone classification (PMID 5805411)
- Limitation
- Small original series; descriptive
- Contribution
- Outcomes for ganglion excision, hook excision, vascular repair
- Limitation
- Level IV; no comparative RCTs
- Contribution
- Ulnar tunnel syndrome is not tracked in arthroplasty-style registries (e.g. AOANJRR/NJR cover joint replacement, not peripheral nerve decompression)
- Limitation
- Epidemiology relies on hospital and surgeon series
Practice Variation & Global Notes
- Diagnostic work-up is broadly consistent worldwide: clinical localisation, nerve conduction studies/EMG, then targeted imaging (MRI/ultrasound for soft-tissue masses, CT for the hook of hamate). The dorsal ulnar cutaneous nerve and Froment's sign are universally used to separate wrist-level from elbow-level lesions.
- Surgical thresholds vary by structural cause and patient demand: an identified ganglion, hook of hamate fracture, or vascular lesion lowers the threshold for surgery, whereas idiopathic mild cases are managed conservatively first.
- Hook of hamate management converges on excision across regions for symptomatic fractures and nonunions, particularly in athletes (golf, racquet sports, baseball) and cyclists.
- Vascular causes require Allen's test and duplex ultrasound first-line with angiography as reference standard; smoking cessation is a universal adjunct.
- Cycling (handlebar pressure), wheelchair use and repetitive tool use are recognised occupational/recreational drivers worldwide.
- Hook of hamate injuries cluster in golf, racquet sports and baseball internationally; document occupational exposure for compensation pathways.
Exam Viva Point - Global Practice: Management worldwide rests on cause-specific Level IV evidence and anatomical principles rather than randomised trials. Nerve conduction studies are standard of care before decompression in all major systems. Hook of hamate injuries are seen in baseball, golf and cyclists; the dorsal ulnar cutaneous nerve and Froment's sign are the universal clinical tools for localising the lesion to the wrist rather than the elbow.
Shea & McClain: Ulnar-Nerve Compression Syndromes at and Below the Wrist (Landmark Classification)
Hook of Hamate Excision in Athletes (Symptomatic Partial Union / Nonunion)
Ulnar Tunnel Syndrome: Contemporary Review of Anatomy, Diagnosis and Treatment
Zone-Based Approach to Ulnar Tunnel Syndrome
Hook of Hamate Fractures: Diagnosis and Excision
Hypothenar Hammer Syndrome (Vascular Cause of Ulnar Tunnel Pathology)
MCQ Practice Points
Q: What are the boundaries of Guyon's canal?
A: Floor: Pisiform, hook of hamate, pisohamate ligament, hypothenar muscles. Roof: Volar carpal ligament (not the transverse carpal ligament) and palmaris brevis. Contents: Ulnar nerve and ulnar artery. The artery lies radial to the nerve. Canal is approximately 4 cm long from proximal wrist to palm.
Q: Describe the Shea-McClain classification of ulnar tunnel syndrome.
A: Zone 1 (proximal): Before bifurcation - mixed motor and sensory deficit. Zone 2 (deep): Deep motor branch only - pure motor deficit (intrinsic weakness, no sensory loss) - accounts for 50% of cases. Zone 3 (superficial): Superficial sensory branch - pure sensory deficit (ulnar 1.5 digits). Ganglion from pisotriquetral joint is most common Zone 2 cause.
Q: How do you differentiate Guyon's canal syndrome from cubital tunnel syndrome?
A: Dorsal ulnar cutaneous nerve: NORMAL in Guyon's (branches proximal to wrist), ABNORMAL in cubital tunnel. Froment's sign: Often NEGATIVE in pure Zone 2 Guyon's (FPL compensation intact), typically POSITIVE in cubital tunnel. FCU weakness: Absent in Guyon's, may be present in cubital tunnel. NCS localization: Wrist segment in Guyon's, elbow segment in cubital tunnel.
Q: What is the most common cause of Zone 2 (pure motor) ulnar tunnel syndrome?
A: Ganglion cyst arising from the pisotriquetral joint accounts for 85-90% of Zone 2 lesions. Other causes include hook of hamate fracture (especially in racquet sports, baseball, golf), ulnar artery aneurysm/thrombosis, lipoma, and direct trauma from cycling ("handlebar palsy"). MRI or ultrasound is diagnostic.
Q: What clinical finding is pathognomonic for Zone 2 ulnar tunnel syndrome?
A: Intrinsic hand weakness WITHOUT sensory loss. Patient has weak finger abduction/adduction, weak thumb adduction, interosseous atrophy, and potential clawing (4th/5th fingers), but normal sensation in the ulnar 1.5 digits. This pattern cannot occur with cubital tunnel syndrome (sensory fibers would also be affected at elbow level).
At a Glance
Ulnar tunnel syndrome involves compression of the ulnar nerve within Guyon's canal at the wrist. The Shea-McClain zones determine clinical presentation: Zone 1 (proximal, before bifurcation) causes mixed motor and sensory loss, Zone 2 (deep motor branch - most common, 50%) causes pure motor weakness without sensory loss, and Zone 3 (superficial sensory branch) causes pure sensory deficit. Ganglion cysts from the pisotriquetral joint are the most common cause (85-90%), followed by hook of hamate fractures in cyclists and golfers. Critically, Froment's sign is negative in Guyon's canal compression because adductor pollicis is innervated before the canal - a positive Froment's indicates proximal ulnar lesion at the elbow.
Floor = PPPGuyon's Canal Boundaries
Hook:Floor PPP = Pisiform, Pisohamate, Pisotriquetral. Ganglion cysts arise from PT joint!
IPABZone 2 Pure Motor Deficits
Hook:IPAB muscles affected in Zone 2 - all supplied by deep motor branch AFTER bifurcation!
GUNSHOTCauses of Ulnar Tunnel Syndrome
Hook:GUNSHOT to Guyon's canal causes compression - ganglion most common!
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old cyclist presents with a 6-month history of weak grip and inability to spread fingers. Examination shows interosseous wasting, positive Wartenberg's sign, but normal sensation throughout the hand including hypothenar and ring/small fingers. Froment's sign is negative. What is your diagnosis and management?”
“A 24-year-old baseball player presents 3 months after a foul tip injury to his catching hand. He has hypothenar pain, weak grip, and numbness in the small finger. Examination shows tenderness over the hook of hamate and intrinsic weakness. What is your diagnosis and how would you manage this?”
“A patient presents with ulnar-sided hand numbness and weak grip. How do you differentiate between Guyon's canal syndrome and cubital tunnel syndrome on clinical examination?”
Guyon's Canal Anatomy (Memorize!)
- **Floor**: Pisiform, hook of hamate, pisohamate ligament
- **Roof**: Palmaris brevis muscle, palmar carpal ligament
- **Contents**: Ulnar nerve + artery (artery is RADIAL to nerve)
- **Nerve bifurcates**: Deep motor + superficial sensory branches
- **Length**: Approximately 4cm from wrist to palm
Shea-McClain Classification (Essential)
- **Zone 1**: Proximal to bifurcation → Motor + Sensory deficit
- **Zone 2**: Deep motor branch → Pure MOTOR deficit (50% of cases)
- **Zone 3**: Superficial sensory branch → Pure SENSORY deficit
- **Zone 2 pathognomonic**: Weakness WITHOUT sensory loss
- **Ganglion cyst**: 85-90% cause of Zone 2 (from pisotriquetral joint)
Guyon's vs Cubital Tunnel (High Yield)
- **Froment's sign**: NEGATIVE Guyon's, POSITIVE cubital
- **Dorsal ulnar cutaneous**: NORMAL Guyon's, ABNORMAL cubital
- **FCU/FDP strength**: NORMAL Guyon's, WEAK cubital (if severe)
- **Elbow symptoms**: ABSENT Guyon's, PRESENT cubital
- **Pure motor/sensory**: Possible Guyon's (zone-dependent), NOT cubital
- **NCS localization**: Wrist slowing vs elbow slowing
Common Causes (GUNSHOT Mnemonic)
- **G**anglion cyst (85-90% of masses - from PT joint)
- **U**lnar artery thrombosis/aneurysm (hypothenar hammer)
- **N**eurofibroma (rare nerve sheath tumor)
- **S**pindle cell lipoma or other mass
- **H**ook of hamate fracture (cyclists, baseball catchers)
- **O**ccupational pressure (handlebar, wheelchair)
- **T**hrombosed ulnar artery
Investigations
- **Radiographs**: PA, lateral, **carpal tunnel view** (for hamate)
- **CT scan**: Gold standard for hook of hamate fracture
- **MRI**: Best for ganglion cyst and soft tissue masses
- **Ultrasound**: Dynamic assessment, Doppler for ulnar artery
- **NCS/EMG**: Confirms ulnar neuropathy, localizes to wrist segment
- **Must do NCS before surgery** - confirms diagnosis and location
Surgical Technique Pearls
- **Incision**: Ulnar border hypothenar, 1cm proximal to wrist crease, 3-4cm distal
- **Identify ulnar artery FIRST** - radial to nerve, protect from injury
- **Decompress all three zones** completely
- **Ganglion**: Excise to joint origin (pisotriquetral) or recurs
- **Hook of hamate**: Excise fragment (NOT fix), smooth edges
- **Outcomes**: 90% success, motor recovery 6-12 months, sensory 3-6 months
Common Viva Questions
- **Describe Guyon's canal anatomy** (Boundaries, contents, bifurcation)
- **What are the three zones?** (Shea-McClain: Zone 1/2/3, motor/sensory deficits)
- **How differentiate from cubital tunnel?** (Froment's, dorsal sensation, FCU/FDP)
- **Most common cause Zone 2?** (Ganglion cyst from pisotriquetral joint)
- **Hook of hamate treatment?** (Excision NOT fixation, poor blood supply)
- **Why is Froment's negative?** (Adductor pollicis branches proximal to Guyon's)
Exam Day Traps
- **DON'T assume Froment's positive in all ulnar neuropathy** - negative = wrist lesion!
- **DON'T forget to check dorsal hand sensation** - normal = Guyon's, abnormal = proximal
- **DON'T operate without NCS** - confirms level, severity, axonal vs demyelination
- **DON'T injure ulnar artery** - radial to nerve, injury causes hypothenar ischemia
- **DON'T fix hook of hamate** - excision is treatment of choice, fixation fails
- **DON'T incompletely excise ganglion** - must trace to PT joint or recurs
Evidence Base
Key Evidence Summary
- Landmark paper defining three anatomical zones
- Basis for all subsequent classification systems
- Guides surgical approach and prognostication
- Multiple case series: 78-91% of Zone 2 lesions
- Arise from pisotriquetral joint
- Complete excision to origin prevents recurrence
- Level IV evidence supports excision over ORIF
- Excision: 95% success, return to sport 10 weeks
- ORIF: 67% nonunion, conversion to excision common
References
-
Shea JD, McClain EJ. Ulnar-nerve compression syndromes at and below the wrist. J Bone Joint Surg Am. 1969;51(6):1095-1103.
-
Murata K, Tamai M, Gupta A. Anatomic study of variations of hypothenar muscles and arborization patterns of the ulnar nerve in the hand. J Hand Surg Am. 2004;29(3):500-509.
-
Kleinert JM, Mehta S. Radial, ulnar, and median nerve entrapment at the wrist and forearm. J Hand Surg Am. 1996;21(4):532-559.
-
Bozkurt MC, Tagil SM, Ozçakar L, Ersoy M, Tekdemir I. Anatomical variations as potential risk factors for ulnar tunnel syndrome: a cadaveric study. Clin Anat. 2005;18(4):274-280.
-
Gross MS, Gelberman RH. The anatomy of the distal ulnar tunnel. Clin Orthop Relat Res. 1985;(196):238-247.
-
Depukat P, Mizia E, Kuniewicz M, Bonczar M, Mazur M, Długosz-Chrzanowska E. Anatomy of Guyon's canal - a systematic review. Folia Med Cracov. 2014;54(2):81-86.
-
Bachoura A, Jacoby SM. Ulnar tunnel syndrome. Orthop Clin North Am. 2012;43(4):467-474.
-
Aguiar PH, Pereira CU, Lobo IJ, Matushita H, Cardoso AC, Martins RS. Ulnar nerve entrapment at Guyon's canal: report of 28 cases. Arq Neuropsiquiatr. 2001;59(3-B):728-732.
-
Netscher D, Cohen V. Ulnar nerve entrapment at the wrist. Hand Clin. 2002;18(2):329-338.
-
Friedman RJ, Cochran TP. A clinical and electrophysiological investigation of anterior transposition for ulnar neuropathy at the elbow. Arch Orthop Trauma Surg. 1987;106(6):375-380.
-
Sarris IK, Papadimitriou NG, Sotereanos DG. Ulnar nerve compression at the wrist: Guyon's canal syndrome. Techniques in Hand & Upper Extremity Surgery. 2002;6(3):109-114.
-
Antoniadis G, Scheglmann K. Posterior interosseous nerve entrapment: etiology, diagnosis, and treatment. Clin Orthop Relat Res. 2008;466(5):1225-1232.
-
Harvie P, Patel N, Ostlere SJ. Prevalence and epidemiological variation of CT-detected hamate hook fractures. J Hand Surg Eur Vol. 2011;36(9):737-739.
-
Hirano K, Inoue G. Classification and treatment of hamate fractures. Hand Surg. 2005;10(2-3):151-157.
-
Cohen SB, Mont MA, Campbell KR, Vogelstein BN, Loewy JW. Upper extremity physical factors affecting tennis serve velocity. Am J Sports Med. 1994;22(6):746-750.