Midfoot Trauma | Lisfranc Association | ORIF Required
- Cuneiform fractures = midfoot trauma involving medial, intermediate, or lateral cuneiform - often associated with Lisfranc injuries
- Medial cuneiform most common - Often associated with Lisfranc injury, Lisfranc ligament attaches to medial cuneiform
- ORIF required if displaced - Prevents midfoot instability and arthritis
- Lisfranc association - Cuneiform fractures suggest midfoot instability, always check for Lisfranc injury
- Midfoot stability - Cuneiforms are part of midfoot stability, displacement causes instability
- “Medial cuneiform most common, Lisfranc association
- “Often associated with Lisfranc injuries
- “ORIF required if displaced
- “Check for midfoot instability
Cuneiform fractures often associated with Lisfranc injuries - Medial cuneiform is attachment site for Lisfranc ligament. Cuneiform fracture suggests midfoot instability. Always check for Lisfranc injury if cuneiform fracture present.
Medial cuneiform most common - Often associated with Lisfranc injury. Lisfranc ligament attaches to medial cuneiform. Displacement causes midfoot instability requiring ORIF.
Cuneiforms are part of midfoot stability - Displacement causes midfoot instability and arthritis. ORIF required if displaced to restore stability and prevent collapse.
Displacement greater than 2mm requires ORIF - Prevents midfoot instability and arthritis. Screw or plate fixation depending on pattern. Goal is anatomic restoration of the medial and middle columns.
- Frequency
- Most common, Lisfranc association
- Treatment
- ORIF
- Outcome
- 80-85% good results
- Frequency
- Rare, often with Lisfranc
- Treatment
- ORIF
- Outcome
- 75-85% good results
- Frequency
- Rare, isolated or with Lisfranc
- Treatment
- ORIF
- Outcome
- 75-85% good results
CHECKLisfranc Association
Hook:CHECK: Cuneiform fracture, High association with Lisfranc, Examine for Lisfranc, CT to assess, Key to check!
Overview and Epidemiology
Cuneiform fractures are rare but important injuries involving the medial, intermediate, or lateral cuneiform bones of the midfoot. These fractures are often associated with Lisfranc injuries and require ORIF if displaced to restore midfoot stability.
Definition
Cuneiform fracture: Fracture of the medial, intermediate, or lateral cuneiform, which:
- Location: Midfoot, between navicular and metatarsals
- Function: Part of midfoot stability
- Association: Often with Lisfranc injuries
- Treatment: ORIF if displaced
Cuneiform bones:
- Medial cuneiform: Most common, Lisfranc ligament attachment
- Intermediate cuneiform: Rare, often with Lisfranc
- Lateral cuneiform: Rare, isolated or with Lisfranc
Epidemiology
- Incidence: Less than 1% of foot fractures
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: High-energy trauma, midfoot injury
- Associated injuries: Lisfranc injuries (30-40%), other midfoot trauma
Cuneiform fractures often associated with Lisfranc injuries - Medial cuneiform is attachment site for Lisfranc ligament. Cuneiform fracture suggests midfoot instability. Always check for Lisfranc injury if cuneiform fracture present (30-40% association).
Anatomy and Pathophysiology
Cuneiform Anatomy
Cuneiform bones:
- Medial cuneiform: Largest, articulates with navicular, 1st metatarsal, intermediate cuneiform
- Intermediate cuneiform: Smallest, articulates with navicular, 2nd metatarsal, medial and lateral cuneiforms
- Lateral cuneiform: Articulates with navicular, 3rd metatarsal, intermediate cuneiform, cuboid
Midfoot stability:
- Cuneiforms: Part of midfoot stability
- Lisfranc ligament: Attaches to medial cuneiform
- Function: Maintains midfoot alignment
Lisfranc association:
- Medial cuneiform: Lisfranc ligament attachment site
- Midfoot instability: Cuneiform fracture suggests instability
- 30-40% association: With Lisfranc injuries
Pathophysiology
Injury mechanism:
- High-energy trauma: Midfoot injury
- Lisfranc mechanism: Often associated
- Direct trauma: To midfoot
Why displacement matters:
- Midfoot instability: Displacement causes instability
- Arthritis risk: Malunion leads to midfoot arthritis
- Collapse risk: Instability causes midfoot collapse
Why ORIF required:
- Restore stability: Anatomic reduction restores midfoot stability
- Prevent collapse: Prevents midfoot collapse
- Lisfranc: Often requires addressing both injuries
Classification Systems
Bone-Based Classification
Medial cuneiform:
- Most common
- Often with Lisfranc
- Treatment: ORIF
- Outcome: 80-85% good results
Intermediate cuneiform:
- Rare
- Often with Lisfranc
- Treatment: ORIF
- Outcome: 75-85% good results
Lateral cuneiform:
- Rare
- Isolated or with Lisfranc
- Treatment: ORIF
- Outcome: 75-85% good results
Bone type guides treatment approach.
Clinical Assessment
History
Symptoms:
- Midfoot pain: Pain in midfoot
- Swelling: Localised to midfoot
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: High-energy trauma
Risk factors:
- High-energy trauma
- Lisfranc injury mechanism
- Midfoot instability
Physical Examination
Inspection:
- Swelling on midfoot
- Ecchymosis (may be delayed)
- Deformity (midfoot collapse if displaced)
Palpation:
- Tenderness over cuneiforms
- Lisfranc joint tenderness (if associated)
- Midfoot instability
Range of Motion:
- Midfoot ROM limited and painful
- Inversion/eversion painful
Special tests:
- Lisfranc stress test: Check for midfoot instability
- Midfoot stress: Pain with stress
- Midfoot alignment: Check for collapse
Always check for Lisfranc injury - Cuneiform fractures are often associated with Lisfranc injuries (30-40%). Perform Lisfranc stress test and check for midfoot instability. CT is often needed to assess both injuries.
Investigations
Standard X-ray Protocol
AP view:
- May show cuneiform fracture
- Check for Lisfranc injury
Lateral view:
- May show fracture
- Assess midfoot alignment
Oblique view:
- May show fracture better
- Lisfranc joint view
Key point: CT is often needed for diagnosis and planning.

Differential Diagnosis
The painful, swollen midfoot after trauma has a wide differential. The single most important distinction is whether the cuneiform fracture is isolated or a component of a Lisfranc injury, because that decision changes both stability assessment and fixation strategy.
- Key clinical clue
- Focal cuneiform tenderness, normal column alignment
- Best test
- CT (films often normal)
- Distinguishing feature
- No tarsometatarsal diastasis or instability
- Key clinical clue
- Plantar ecchymosis, pain on midfoot stress
- Best test
- Weight-bearing / stress films, CT
- Distinguishing feature
- First-second TMT diastasis, fleck sign, instability
- Key clinical clue
- Tenderness at the N-spot (dorsal navicular)
- Best test
- CT or MRI
- Distinguishing feature
- Fracture proximal to cuneiforms, talonavicular pain
- Key clinical clue
- Lateral midfoot tenderness, lateral column
- Best test
- CT
- Distinguishing feature
- Lateral column shortening, abduction mechanism
- Key clinical clue
- Tenderness at MT bases
- Best test
- AP/oblique films
- Distinguishing feature
- Fracture distal to TMT joints
- Key clinical clue
- Pain but no fracture on imaging
- Best test
- MRI / stress films
- Distinguishing feature
- Ligament signal change, possible dynamic instability
Treating a cuneiform fracture in isolation while missing the associated Lisfranc instability is the classic error. Any cuneiform fracture mandates a deliberate search for tarsometatarsal malalignment with weight-bearing or stress views, and CT if there is any doubt.
Bipartite Medial Cuneiform: the Cuneiform Fracture Mimic
The differential of a "cuneiform fracture" on imaging must include the bipartite medial cuneiform — a congenital normal variant that is the classic mimic and a well-recognised cause of over-diagnosis.
- What it is. In a bipartite (partitioned) medial cuneiform the bone forms as two ossicles - a dorsal and a plantar half - separated by a cartilaginous synchondrosis; it is uncommon (roughly 1% or fewer of feet) and is often bilateral.
- How to tell it from a fracture. The dividing line of a bipartite cuneiform is smooth, rounded and corticated on both sides and lies in a consistent (usually horizontal, dorsal-to-plantar) plane, whereas an acute fracture line is sharp, non-corticated and irregular, with adjacent bone-marrow oedema on MRI and a matching mechanism and point tenderness. Bilaterality and corticated margins point to the variant.
- Why it matters. Misreading a bipartite cuneiform as a fracture leads to needless immobilisation or surgery; conversely a genuinely symptomatic bipartite cuneiform (a painful synchondrosis) is a separate, uncommon entity. When in doubt, compare the contralateral foot and use MRI - oedema indicates an acute injury or a symptomatic synchondrosis, not an incidental variant.
Q: A CT shows a cleft in the medial cuneiform - fracture or not? A: Consider the bipartite medial cuneiform, a normal variant (dorsal + plantar ossicles separated by a synchondrosis, often bilateral). A smooth, corticated, consistent-plane cleft with no oedema and a matching cleft on the other foot is the variant; a sharp, non-corticated, irregular line with marrow oedema and focal tenderness is a fracture. Compare the contralateral side and use MRI when uncertain.
CUNEIFORMCuneiform Fracture Features
Hook:CUNEIFORM: Cuneiform bones, Usually associated with Lisfranc, Navicular articulation, Examine for Lisfranc, Instability risk, Fixation required, ORIF if displaced, Restore stability, Medial most common!
Management Algorithm
Management Pathway
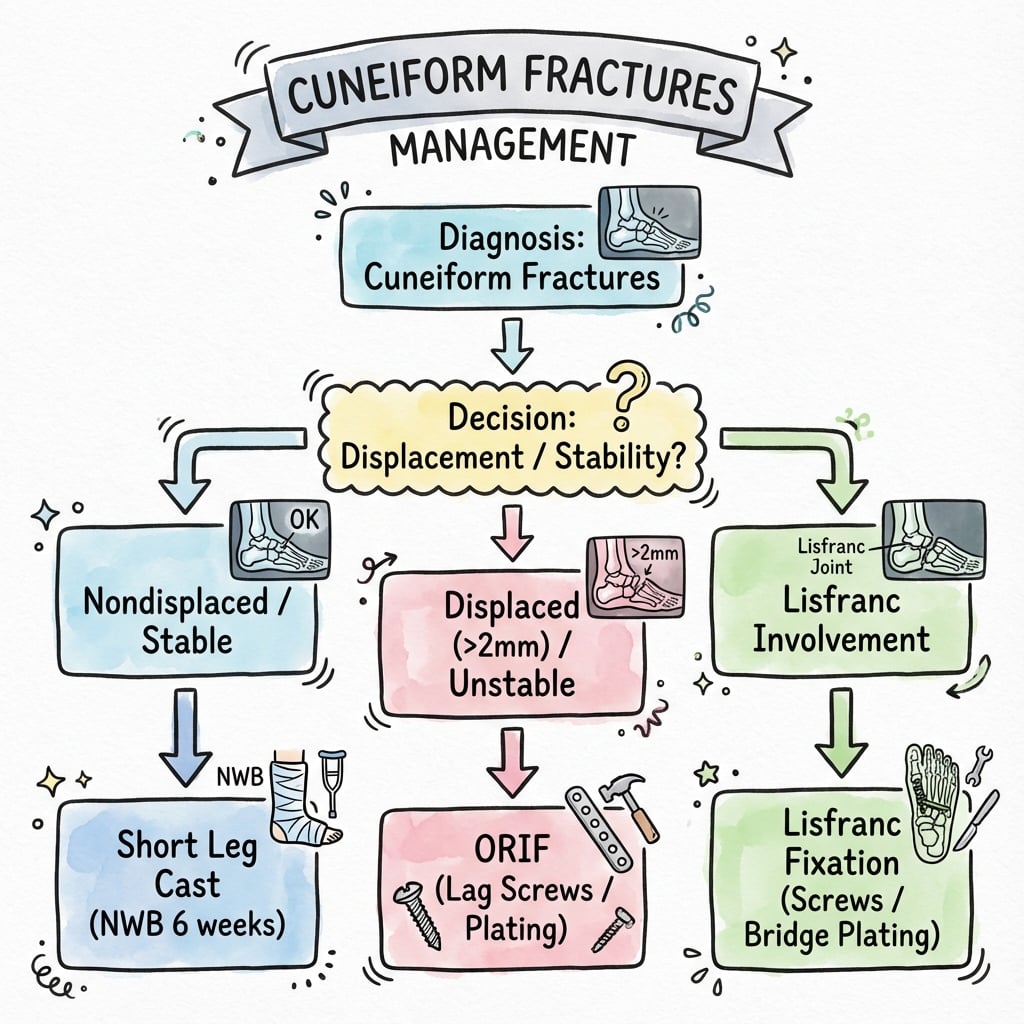
Cuneiform Fracture Management
CT is usually required for diagnosis - cuneiform fractures are difficult to see on X-ray alone. Assess displacement, associated Lisfranc injury, and midfoot instability. Check for midfoot collapse.
If non-displaced (less than 2mm step-off) and isolated, conservative treatment with cast and non-weight bearing for 6-8 weeks. Success rate 85-90%.
If displaced (greater than 2mm) or part of Lisfranc injury, ORIF required. Restore midfoot stability. Screw or plate fixation. Success rate 80-85%.
If part of Lisfranc injury, address both injuries. Cuneiform ORIF as part of Lisfranc fixation. Restore midfoot stability. Success rate 75-85%.
ORIFTreatment Decision
Hook:ORIF: ORIF Required if displaced, Restore midfoot stability, Instability prevention, Fixation with screws or plate!
Surgical Technique
ORIF Technique
Indications:
- Displaced cuneiform fractures
- Part of Lisfranc injury
- Midfoot instability
Approach:
- Dorsal approach to cuneiform
- Expose cuneiform
- Protect neurovascular structures
Technique:
- Exposure: Dorsal approach to cuneiform, expose fracture, protect neurovascular structures
- Reduction: Anatomic reduction of fracture to restore midfoot stability
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Verification: Confirm reduction and hardware position fluoroscopically, verify midfoot stability restored
Advantages:
- Restores midfoot stability
- Prevents collapse
- Allows early motion
ORIF restores midfoot stability.
The High-Energy Transcuneiform Fracture-Dislocation: Restore Column Length and the Arch
Beyond the isolated hairline fracture, the cuneiforms can be shattered as part of a high-energy transcuneiform fracture-dislocation — a pattern the evidence base describes but the body does not develop.
- The pattern. A high-energy midfoot injury (crush, road traffic) can comminute all three cuneiforms with dislocation of the medial three metatarsals and disruption of the Lisfranc ligament — the "transcuneiform" fracture-dislocation.
- The goal is the column and the arch, not the fragment. Reconstruction aims to restore the length and alignment of the medial and middle columns and the longitudinal and transverse (diagonal) arches of the foot, rather than to anatomically piece together every small cuneiform fragment — column length is what preserves function.
- Approach and fixation. An anterior/dorsal longitudinal approach exposes the cuneiforms and metatarsal bases; fixation is by K-wires and/or screws across the tarsometatarsal joints (or bridge plating) to hold length and alignment while the comminuted bone heals, with primary arthrodesis considered for irreconstructible articular destruction.
- Imaging. CT is essential to map the comminution and plan reconstruction of these complex injuries.
Q: How do you manage a high-energy fracture-dislocation shattering all three cuneiforms? A: This transcuneiform fracture-dislocation (all three cuneiforms + medial-ray dislocation + Lisfranc disruption) is reconstructed to restore medial/middle column length and the longitudinal and transverse arches rather than to reassemble every fragment - via an anterior longitudinal approach with K-wires/screws across the TMT joints (or primary arthrodesis for irreconstructible joints), planned on CT.
Complications
- Incidence
- 10-15%
- Risk Factors
- Displacement, inadequate reduction
- Prevention/Management
- Anatomic reduction, adequate fixation
- Incidence
- 10-15%
- Risk Factors
- Instability, inadequate fixation
- Prevention/Management
- Restore stability, adequate fixation
- Incidence
- 30-40%
- Risk Factors
- Focus on cuneiform only
- Prevention/Management
- Always check for Lisfranc
- Incidence
- 5-10%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation
Midfoot Instability
10-15% incidence (if untreated):
- Cause: Displacement, inadequate reduction, Lisfranc injury
- Prevention: Anatomic reduction, adequate fixation
- Management: Revision ORIF or midfoot fusion if severe
Midfoot Collapse
10-15% incidence (if untreated):
- Cause: Midfoot instability, inadequate fixation
- Prevention: Restore stability, adequate fixation
- Management: Revision ORIF or midfoot fusion if severe
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- CT to confirm healing
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF (isolated):
- Success rate: 80-85% (union, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Midfoot stability: 80-85% maintain stability
ORIF (part of Lisfranc):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-75% return to pre-injury level
- Midfoot stability: 75-80% maintain stability
Conservative (non-displaced):
- Success rate: 85-90% (union, pain relief)
- Functional outcomes: 80-85% return to pre-injury level
- Midfoot stability: 85-90% maintain stability
Long-Term Prognosis
Midfoot instability progression:
- With proper treatment: 10-15% develop instability
- Without treatment: 20-30% develop instability
- Risk factors: Displacement, Lisfranc injury, delayed treatment
Guidelines, Registries & Global Practice
Global Epidemiology
- Isolated cuneiform fractures are among the rarest foot fractures (the isolated medial cuneiform literature comprises fewer than 10 reported cases worldwide).
- Most cuneiform fractures occur as part of a midfoot/Lisfranc injury complex, which is more common in men in the third decade.
- Up to 20% of Lisfranc injuries are missed or diagnosed late globally, the single biggest driver of poor outcomes regardless of healthcare setting.
Guidance Across Major Bodies
There is no cuneiform-fracture-specific society guideline; practice is extrapolated from Lisfranc and general intra-articular foot fracture principles, which are broadly concordant across regions.
- Diagnosis emphasis
- Weight-bearing/stress views, CT for fracture mapping
- Operative position
- Anatomic reduction and stable fixation of medial/middle columns
- Diagnosis emphasis
- High suspicion; CT for occult injury; stress exam under anaesthesia
- Operative position
- ORIF for fracture patterns; primary arthrodesis for ligamentous
- Diagnosis emphasis
- Senior review of midfoot injuries; cross-sectional imaging if films equivocal
- Operative position
- Restore alignment; refer complex midfoot to foot and ankle service
- Diagnosis emphasis
- MRI gold standard for ligamentous injury; CT for subtle subluxation
- Operative position
- No proven superiority of ORIF vs PA; reduction quality is decisive
Registry and Trial Notes
- Arthroplasty-style joint registries (NJR, AJRR, AOANJRR) do not track cuneiform fractures; the relevant high-level data are the Lisfranc RCTs (Ly & Coetzee 2006; Henning 2009) and the ongoing multicentre BFF trial.
- These consistently show that reduction quality, not the specific implant, determines outcome.
High- vs Limited-Resource Practice
- Well-resourced settings: routine CT for mapping, MRI for occult/ligamentous injury, and a foot-and-ankle subspecialist performing column-based fixation or primary arthrodesis.
- Limited-resource settings: reliance on weight-bearing and stress radiographs with contralateral comparison; closed reduction with percutaneous K-wires or screws is a legitimate strategy when CT and implants are scarce, prioritising anatomic alignment and a stable, plantigrade foot.
Cuneiform fractures are a common viva springboard into the Lisfranc complex. Know that the medial cuneiform is the Lisfranc ligament attachment, that any cuneiform fracture mandates a search for tarsometatarsal instability, that anatomic reduction is the key prognostic factor worldwide, and be ready to cite Ly & Coetzee (AOFAS 88 vs 68.6) on primary arthrodesis versus ORIF.
Controversies and Areas of Uncertainty
Because isolated cuneiform fractures are vanishingly rare, almost every controversy is inherited from the Lisfranc literature that governs the combined injury.
For the associated Lisfranc injury, two RCTs (Ly & Coetzee 2006; Henning 2009) favoured primary arthrodesis on AOFAS scores and reoperation rates, particularly for primarily ligamentous patterns. The adequately powered multicentre BFF trial is designed to settle this; until then, ORIF remains widely used for bony fracture-dislocation patterns where the medial column can be anatomically reconstructed.
The widely quoted 2mm articular step-off / diastasis threshold for surgery is extrapolated from Lisfranc and other intra-articular foot injuries rather than from cuneiform-specific data. Stability under stress, not an absolute millimetre value, is the more defensible decision driver.
Transarticular screws are simple but damage articular cartilage; dorsal bridge plating spares the joint surface but is more dissection-heavy. There is no high-level evidence establishing superiority; choice is guided by fracture comminution and surgeon preference.
Whether to routinely remove transarticular hardware is unresolved. Routine removal inflates the reoperation rate (a major reason arthrodesis looked favourable in Henning 2009) but may relieve symptomatic hardware; many centres now retain or selectively remove.
MCQ Practice Points
Q: Why is medial cuneiform the most common cuneiform fracture? A: Medial cuneiform is attachment site for Lisfranc ligament - Often associated with Lisfranc injuries (30-40%). Largest cuneiform. Displacement causes midfoot instability requiring ORIF.
Q: Why are cuneiform fractures often associated with Lisfranc injuries? A: Cuneiform fracture suggests midfoot instability - 30-40% of cuneiform fractures are associated with Lisfranc injuries. Medial cuneiform is Lisfranc ligament attachment site. Always check for Lisfranc injury if cuneiform fracture present.
Q: Why is midfoot stability important in cuneiform fractures? A: Cuneiforms are part of midfoot stability - Displacement causes midfoot instability and arthritis. ORIF required if displaced to restore stability. Success rate 80-85% if stability restored.
Q: When is ORIF required for cuneiform fractures? A: Displacement greater than 2mm or part of Lisfranc injury - Prevents midfoot instability and collapse. Screw or plate fixation. Success rate 80-85% for isolated, 75-85% with Lisfranc.
Q: What is the treatment for cuneiform fractures? A: ORIF if displaced (greater than 2mm) or part of Lisfranc injury - Restores midfoot stability and prevents collapse. Conservative treatment for non-displaced isolated fractures (85-90% good results). Success rate 80-85% with ORIF.
Clinical Imaging
Imaging Atlas
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old patient presents with midfoot pain after high-energy trauma. CT shows displaced medial cuneiform fracture with 3mm displacement. No associated Lisfranc injury.”
“A 35-year-old patient has a medial cuneiform fracture as part of a Lisfranc injury. The examiner asks you to explain how you manage both injuries.”
“A 24-year-old runner has persistent dorsomedial midfoot pain and focal tenderness over the medial cuneiform. Two sets of plain radiographs taken over three weeks are reported as normal. The examiner asks how you would proceed.”
Key Concepts
- Medial cuneiform most common (Lisfranc ligament attachment)
- Often associated with Lisfranc injuries (30-40%)
- Cuneiforms are part of midfoot stability
- ORIF required if displaced (restores midfoot stability)
Classification
- Medial: Most common, Lisfranc association - ORIF (80-85% good results)
- Intermediate: Rare, often with Lisfranc - ORIF (75-85% good results)
- Lateral: Rare, isolated or with Lisfranc - ORIF (75-85% good results)
- Key Factor: Pattern dictates approach and Lisfranc evaluation
Treatment
- Non-displaced, isolated: Conservative (cast, NWB 6-8 weeks)
- Displaced, isolated: ORIF (80-85% good results)
- Part of Lisfranc: ORIF as part of Lisfranc fixation (75-85% good results)
- Displacement greater than 2mm: ORIF required
Surgical Technique
- Dorsal approach: Protect neurovascular structures
- Reduction: Anatomic reduction to restore midfoot stability
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Verify midfoot stability restored
- Verify reduction fluoroscopically
Complications
- Midfoot instability: 10-15% if untreated (prevent with anatomic reduction)
- Midfoot collapse: 10-15% if untreated (prevent with adequate fixation)
- Missed Lisfranc: 30-40% (prevent by always checking for Lisfranc)
- Nonunion: 5-10% (prevent with rigid fixation)
Evidence Base
Isolated cuneiform fractures are too rare to support randomised trials, so the evidence base for the cuneiform itself is built from case reports and series. The high-level evidence sits in the adjacent and frequently coexistent Lisfranc literature, which directly governs how a cuneiform fracture is managed when it forms part of a tarsometatarsal injury.
Ligamentous Lisfranc: Primary Arthrodesis vs ORIF (Landmark RCT)
- AOFAS 88 (arthrodesis) vs 68.6 (ORIF) at 2 years
- Anatomic reduction achieved in nearly all in both arms
- 5/20 ORIF patients required salvage arthrodesis
- Drove the case for primary fusion in ligamentous patterns
ORIF vs Primary Arthrodesis: Reoperation Burden (RCT)
- Secondary surgery 78.6% (ORIF) vs 16.7% (arthrodesis)
- No significant SF-36/SMFA difference between groups
- Difference largely driven by routine hardware removal
- Reframes the debate around reoperation, not function
BFF Study: Multicentre PA vs ORIF Trial (Protocol)
- Powered multicentre RCT (n=112), NCT04519242
- Primary outcome: quality of life
- Includes cost-effectiveness analysis
- Earlier trials were underpowered single-centre studies
Lisfranc Complex Injuries: Diagnosis and Missed Injury Rate (Review)
- Up to 20% of Lisfranc injuries missed/late-diagnosed
- CT for non-displaced fracture and subtle subluxation
- MRI is gold standard for ligamentous injury
- Anatomic reduction is the key determinant of outcome
Isolated Medial Cuneiform Stress Fracture (Case Report)
- Isolated cuneiform fracture is genuinely rare (fewer than 10 reported)
- Plain films were normal twice; MRI made the diagnosis
- Non-displaced fractures heal well non-operatively
- Delayed diagnosis is the main pitfall
Transcuneiform Fracture-Dislocation: Operative Restoration of Arch (Case Report)
- High-energy mechanism injures all three cuneiforms
- CT essential to map the comminution
- Goal is restoration of arch anatomy and column length
- Good outcome achievable with anatomic fixation