First Dorsal Compartment | APL and EPB | Finkelstein Test | Injection
TREATMENT
Critical Must-Knows
- First dorsal compartment contains APL and EPB
- Finkelstein test is pathognomonic
- Injection success 70-80%
- Watch for aberrant EPB septum
- Common in new mothers (repetitive lifting)
Clinical Pearls
- "Finkelstein: fist over thumb, ulnar deviate wrist
- "New mothers: repetitive baby lifting
- "Superficial radial nerve at risk during surgery
- "Separate septum for EPB in 30-50%
Clinical Imaging
Imaging Gallery




Critical De Quervain Concepts
Anatomy
First dorsal compartment contains APL and EPB. These tendons pass over radial styloid. Stenosing tenosynovitis causes pain with thumb/wrist movement.
The tendons may have a separate septum which must be released at surgery.
Finkelstein Test
Make fist over thumb, ulnar deviate wrist. Positive test reproduces radial wrist pain. Pathognomonic for de Quervain.
The test stretches the APL and EPB tendons.
Injection
Corticosteroid injection is first-line treatment. 70-80% success rate. Inject into tendon sheath, not tendon.
May repeat once if partial response.
Septum
Separate septum for EPB in 30-50% of cases. If EPB in separate compartment, both compartments must be released at surgery.
This is the most common cause of failed release.
At a Glance
De Quervain Tenosynovitis At a Glance
| Feature | Key Points |
|---|---|
| Definition | Stenosing tenosynovitis of 1st dorsal compartment (APL, EPB) |
| Classic presentation | New mother with radial wrist pain, worse with lifting |
| Key test | Finkelstein test - fist over thumb, ulnar deviate - reproduces pain |
| First-line treatment | Corticosteroid injection (70-80% success) |
| Surgical indication | Failed conservative treatment (2 injection trials) |
| Critical surgical point | Check for separate EPB septum (30-50%) - release both compartments |
APL EPBFirst Dorsal Compartment
| A | Abductor Pollicis Longus Abducts thumb |
| P | |
| L | |
| E | Extensor Pollicis Brevis Extends thumb MCP |
| P | |
| B |
| A | Abductor Pollicis Longus Abducts thumb | L | P | ||
| P | E | Extensor Pollicis Brevis Extends thumb MCP | B |
Hook:APL and EPB are in first dorsal compartment!
SQUEEZEDEQUERVAIN - Key Facts
| S | Stenosing tenosynovitis First dorsal compartment |
| Q | Quite common in new mothers Repetitive lifting |
| U | Ulnar deviation Finkelstein test |
| E | EPB septum 30-50% Critical surgical finding |
| E | Excellent injection response 70-80% success |
| Z | Zone over radial styloid Tenderness location |
| E | Extensor pollicis brevis + APL First compartment contents |
| S | Stenosing tenosynovitis First dorsal compartment | E | EPB septum 30-50% Critical surgical finding | E | Extensor pollicis brevis + APL First compartment contents |
| Q | Quite common in new mothers Repetitive lifting | E | Excellent injection response 70-80% success | ||
| U | Ulnar deviation Finkelstein test | Z | Zone over radial styloid Tenderness location |
Hook:SQUEEZE thumbs up for de Quervain!
1-2-3-4-5-6Dorsal Compartments
| 1 | APL, EPB Abductor/extensor of thumb |
| 2 | ECRL, ECRB Radial wrist extensors |
| 3 | EPL Extensor pollicis longus |
| 4 | EDC, EIP Finger extensors |
| 5 | EDM Small finger extensor |
| 6 | ECU Ulnar wrist extensor |
| 1 | APL, EPB Abductor/extensor of thumb | 3 | EPL Extensor pollicis longus | 5 | EDM Small finger extensor |
| 2 | ECRL, ECRB Radial wrist extensors | 4 | EDC, EIP Finger extensors | 6 | ECU Ulnar wrist extensor |
Hook:Six dorsal compartments - know them all!
Overview and Epidemiology
De Quervain tenosynovitis is a stenosing tenovaginitis of the first dorsal extensor compartment, where the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons become entrapped beneath a thickened extensor retinaculum at the radial styloid. Despite the historical name "tenosynovitis", the dominant histological finding is myxoid degeneration and fibrocartilaginous thickening of the retinaculum with little true inflammatory infiltrate - it is a degenerative/mechanical overload process rather than a primary inflammatory synovitis.
Who gets it
- Population prevalence roughly 0.5 to 1.3 percent
- Female predominance (around 4 to 6 : 1)
- Peak in the fourth to sixth decades
- Postpartum and lactating women, occupational repetitive users, and heavy smartphone users are over-represented
Risk factors
- Repetitive thumb abduction/extension with ulnar wrist deviation (lifting an infant, texting, gripping)
- Postpartum hormonal change plus repetitive lifting (often bilateral)
- Female sex, age 40 to 60
- Associations reported with diabetes and inflammatory arthropathy
Classic patient
New mothers are the classic patients due to repetitive lifting of babies with the thumb extended and the wrist ulnar-deviated; it is frequently bilateral in this group. The same repetitive-loading mechanism explains the rising incidence among heavy smartphone and digital-device users.
Pathophysiology and Mechanisms
First Dorsal Compartment
Contents:
- Abductor pollicis longus (APL)
- Extensor pollicis brevis (EPB)
Location: Over radial styloid
Septum variant: EPB in separate compartment in 30-50%
Understanding anatomy is key to successful treatment.
Classification Systems
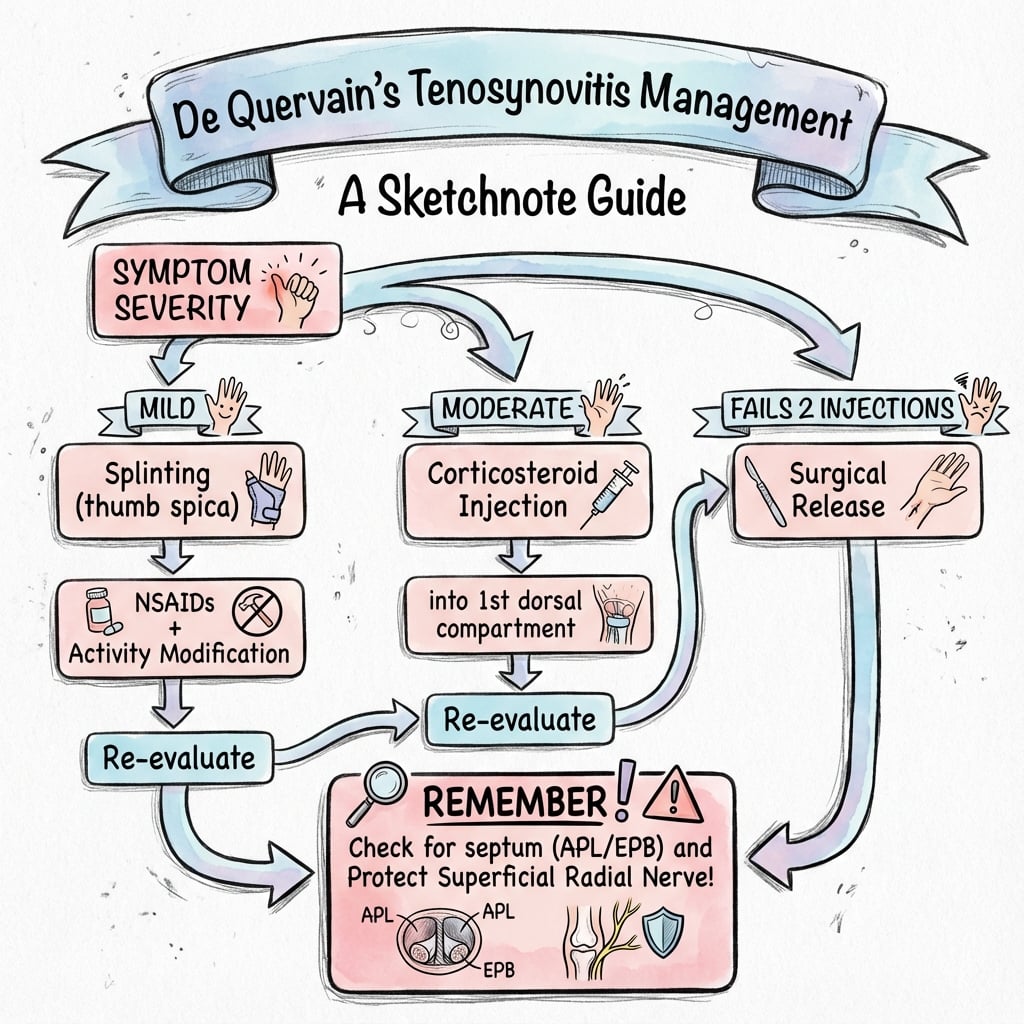
Clinical Staging
| Stage | Description | Management |
|---|---|---|
| Mild | Intermittent pain with activity | Splinting, activity modification |
| Moderate | Constant pain, positive Finkelstein | Corticosteroid injection |
| Severe | Failed injection, chronic symptoms | Surgical release |
Clinical staging helps guide treatment intensity.
Clinical Assessment
History
- Radial wrist pain
- Pain with thumb use
- Worse with gripping
- Swelling over radial styloid
- New parent or repetitive work
Ask about repetitive thumb/wrist activities.
Examination
- Tenderness over first dorsal compartment
- Positive Finkelstein test
- May have visible swelling
- Crepitus with movement
Finkelstein is the key diagnostic test.
Finkelstein Test Technique
Make fist over thumb, then ulnar deviate wrist. This stretches APL and EPB over the radial styloid. Reproduction of radial wrist pain is positive.
This test is pathognomonic for de Quervain tenosynovitis.
Differential Diagnosis
Radial-Sided Wrist and Thumb Pain - Key Differentials
| Condition | Distinguishing features | Discriminating test |
|---|---|---|
| De Quervain tenosynovitis | Pain/tenderness over radial styloid, swelling of first dorsal compartment | Finkelstein / Eichhoff positive; WHAT (wrist hyperflexion and abduction of thumb) test |
| Thumb carpometacarpal (basal joint) osteoarthritis | Pain at base of thumb, more distal and volar; squaring of thumb base | Grind test positive; radiographs show CMC joint OA |
| Intersection syndrome | Pain and crepitus roughly 4 cm proximal to wrist where second compartment crosses first | Tenderness proximal to the radial styloid, not over it |
| Wartenberg syndrome (superficial radial nerve entrapment) | Dorsoradial numbness/paraesthesia, no true tendon swelling | Positive Tinel over the nerve; sensory not tendon-stretch pain |
| Scaphoid fracture / nonunion | History of trauma, anatomic snuffbox tenderness | Snuffbox tenderness, axial thumb load pain; radiographs/MRI |
| Scaphotrapeziotrapezoid (STT) arthritis | Pain at the STT joint, just distal to scaphoid | Localised STT tenderness; radiographs |
Finkelstein vs Eichhoff
The test most clinicians call "Finkelstein" is technically the Eichhoff manoeuvre: the patient makes a fist over a flexed thumb and the examiner ulnar-deviates the wrist. The true Finkelstein test has the examiner grasp the thumb and longitudinally pull while ulnar-deviating the wrist. Both stress the APL/EPB. The Eichhoff can be falsely positive; the WHAT test (resisted thumb extension/abduction with the wrist in hyperflexion) has been proposed as more specific.
Investigations
Usually Not Required
De Quervain is a clinical diagnosis.
Finkelstein test + radial styloid tenderness is sufficient.
Imaging rarely needed unless diagnosis uncertain.
Management Algorithm
First-Line Treatment
Splint:
- Thumb spica splint
- Rest the first dorsal compartment
Injection:
- Corticosteroid into tendon sheath
- Success rate 70-80%
- May repeat once
Activity modification:
- Avoid aggravating activities
- Ergonomic advice
Conservative treatment is effective in majority of cases.
Surgical Technique
First Dorsal Compartment Release
Incision: Transverse or longitudinal over first DC
Steps:
- Protect superficial radial nerve branches
- Identify first dorsal compartment
- Release retinaculum longitudinally
- CHECK for separate EPB septum (30-50%)
- Release EPB compartment if present
- Ensure both tendons glide freely
Always look for separate EPB compartment.
Separate EPB Septum
Always look for separate EPB compartment. Present in 30-50% of patients. If only APL compartment released, EPB remains stenosed and symptoms persist. This is the most common cause of failed surgery.
Complications
| Complication | Incidence | Prevention/Management |
|---|---|---|
| Superficial radial nerve injury | 5-10% | Careful dissection and protection |
| Incomplete release | 5-10% | Check for EPB septum |
| Subluxation of tendons | Rare | Preserve some retinaculum dorsally |
| Scar sensitivity | Variable | Proper incision placement |
Postoperative Care
Recovery Timeline
Soft dressing. Gentle ROM immediately. Avoid forceful gripping.
Remove sutures. Progressive thumb use. Return to light duties.
Full activity as tolerated. Complete recovery expected.
Outcomes and Prognosis
Prognostic Factors
Better outcomes: Shorter symptom duration, successful injection response, complete surgical release.
Worse outcomes: Missed EPB septum at surgery, nerve injury, delayed treatment.
Controversies and Areas of Uncertainty
Ultrasound-guided vs landmark injection
The 2023 network meta-analysis ranked ultrasound-guided injection highest for pain, and a septum predicts failure of a single blind injection. However, blind injection remains effective and far cheaper, and no adequately powered head-to-head RCT has shown a clinically meaningful functional difference. Reasonable to reserve guidance for failed blind injection or a known septum.
Role and timing of splinting
Adding 3-4 weeks of thumb spica to injection improves function statistically but the difference may not reach a clinically important threshold, and splints are poorly tolerated by caregivers. The optimal duration and whether splinting alone has any durable role remain unsettled.
Open vs minimally invasive release
Mini-open, percutaneous and ultrasound-guided releases report fewer wound issues, but evidence is largely low-level (case series). Open release with direct visualisation of any EPB septum and protection of the superficial radial nerve remains the reference standard.
The injection success figure
Commonly quoted single-injection cure rates of 70 to 80 percent derive from observational and mixed cohorts; the only included trial in the Cochrane review was tiny and confined to pregnant/lactating women. True durable single-injection success is likely lower when a septum is present (around 30 percent recurrence at six weeks in one ultrasound cohort).
Evidence Base and Key Studies
- 30 randomised trials, 1663 patients (mean age 46 years, 80% female)
- Adding 3-4 weeks of thumb spica immobilisation to corticosteroid injection (CSI) gave statistically (not clinically) significant short- and mid-term functional benefit (Q-DASH mid-term mean difference 9.4 points)
- Ultrasound-guided CSI ranked highest for pain relief in the network analysis
- CSI plus thumb spica had the highest probability of being the most effective option for short- and mid-term function
- Only one small controlled trial met inclusion criteria (18 pregnant or lactating women)
- All patients given methylprednisolone plus bupivacaine injection achieved complete pain relief (9/9) versus none with thumb spica splinting alone (0/9), number needed to treat = 1
- No injection side effects or local complications observed
- Authors stressed limited applicability owing to the single small, methodologically weak trial
- Reviewed 15 randomised controlled trials in de Quervain disease (plus trigger finger and Dupuytren)
- Moderate evidence for very-short-term benefit of corticosteroid injection
- A thumb splint added to corticosteroid injection was effective at short and mid term (moderate evidence)
- Called for more high-quality RCTs to support evidence-based practice
- 87 embalmed cadaveric wrists dissected (Thai population)
- Complete intracompartmental septum in 17.2% and incomplete septum in 42.5% (roughly 60% had some septation)
- Superficial radial nerve crossed over the first extensor compartment in 59.5% of specimens
- Two APL tendon slips were most common (54%); a single EPB slip in 97.7%, with EPB absent bilaterally in one cadaver
- 50 consecutive patients given a single ultrasound-assessed corticosteroid injection
- Symptom recurrence in 15 patients (30%) within six weeks
- An intracompartmental septum (adjusted OR 18.4) and a greater number of tendon slips (adjusted OR 24.7 per slip) independently predicted recurrence
- Mean DASH improved from 74.1 to 19.3 and VAS pain from 8.5 to 2.0
- Cross-sectional study of 508 university students
- 36.8% had a positive Finkelstein test, 95.6% in the dominant hand
- Positivity rose with screen time, from 12.5% at under 2 hours/day to 46.2% at 8 hours/day or more
- Wrist ulnar deviation during device use was strongly associated with a positive test
- Cross-sectional study of 190 infant caregivers screened with Finkelstein test
- 26.8% prevalence of de Quervain disease
- Infant age, lifting frequency and hand dominance were significant risk factors
- Caregiver age, infant weight and relationship to the infant were not significant
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: De Quervain in New Mother
"A 32-year-old new mother has 2 months of radial wrist pain. It is worse when lifting her baby. Finkelstein test is positive. There is tenderness over the radial styloid. What is your diagnosis and management?"
Scenario 2: Failed Surgical Release
"A 45-year-old woman had surgical release for de Quervain 6 weeks ago but her symptoms have not improved. The wound healed well. Finkelstein test remains positive. What is the most likely cause and how would you manage?"
Scenario 3: Injection Technique
"You are about to perform a corticosteroid injection for de Quervain tenosynovitis. Describe your technique and what complications you would warn the patient about."
MCQ Practice Points
Contents Question
Q: What tendons are in the first dorsal compartment? A: APL (abductor pollicis longus) and EPB (extensor pollicis brevis).
Test Question
Q: What is the Finkelstein test? A: Fist over thumb, ulnar deviate wrist. Positive when this reproduces radial wrist pain.
Surgical Failure Question
Q: What is the most common cause of failed surgical release? A: Missed separate EPB septum. Present in 30-50%; both compartments must be released.
Injection Success Question
Q: What is the success rate of corticosteroid injection for de Quervain? A: 70-80% success rate. It is first-line treatment. May be repeated once if partial response.
Nerve at Risk Question
Q: What nerve is at risk during de Quervain release? A: Superficial radial nerve. Branches cross the surgical field. Injury causes numbness over dorsal thumb web or painful neuroma.
Guidelines, Registries & Global Practice
Global epidemiology:
- Overall population prevalence is roughly 0.5 to 1.3 percent, with a female-to-male ratio of about 4 to 6 to 1 and a peak in the fourth to sixth decades.
- High-risk groups consistently identified across studies: postpartum and lactating women, occupational repetitive thumb/wrist users, and a newer cohort of high-intensity smartphone and digital-device users.
- Reported prevalence in infant caregivers reached 26.8 percent in one cross-sectional study, and a positive Finkelstein test was found in 36.8 percent of heavy device users among university students - far higher than the general population, underlining the role of repetitive loading.
Guidelines side by side: No single orthopaedic society publishes a dedicated, named de Quervain guideline, so practice is anchored by high-level synthesis rather than a formal guideline document.
How major bodies frame first-line treatment
| Source | Position | Notes |
|---|---|---|
| JAMA Network Open network meta-analysis (2023) | Corticosteroid injection (ideally ultrasound-guided) plus 3-4 weeks thumb spica | Strongest current evidence base; 30 trials, 1663 patients |
| AAOS / American Society for Surgery of the Hand (US) | Stepwise: splint and activity modification, then injection, then release | Emphasis on counselling re repeat injection and surgical anatomy |
| BOA / BSSH (UK) | Conservative first; injection in primary or secondary care; release if refractory | Pragmatic, primary-care-led injection pathways common in the NHS |
| AO Foundation / EFORT (Europe) | Conservative-first, surgery reserved for failed injection | Consistent with above; mini-open release widely taught |
Registry note: De Quervain release is a soft-tissue decompression and is not captured by joint-replacement registries (NJR, AJRR, AOANJRR). Outcome data therefore come from RCTs, systematic reviews and institutional series rather than national implant registries.
High- vs limited-resource practice variation:
- In well-resourced settings ultrasound-guided injection is increasingly standard, improving accuracy and allowing both subcompartments to be targeted when a septum is seen.
- In limited-resource settings landmark-guided (blind) injection remains the norm and is effective; the diagnosis is clinical (Finkelstein test) so no imaging is required to start treatment.
- Surgical release is a low-cost, high-yield day-case procedure under local or regional anaesthesia, making it feasible across resource levels.
Global Exam Focus
Know the Finkelstein test technique, the injection approach (sheath not tendon), and the importance of the separate EPB septum. Be able to describe surgical release with superficial radial nerve protection, and cite that injection plus short thumb-spica immobilisation is the best-supported first-line strategy.
Additional Quiz Questions
DE QUERVAIN TENOSYNOVITIS
Clinical summary
Anatomy
- •First dorsal compartment
- •APL and EPB
- •Over radial styloid
- •Separate EPB septum 30-50%
Clinical
- •Radial wrist pain
- •New mothers classic
- •Finkelstein test positive
- •Tender over radial styloid
Conservative Treatment
- •Injection: 70-80% success
- •Thumb spica splint
- •Activity modification
- •May repeat injection once
Surgery
- •Release first dorsal compartment
- •Check for EPB septum
- •Protect superficial radial nerve
- •Confirm both tendons glide
Complications
- •Superficial radial nerve injury
- •Missed EPB septum (failure)
- •Tendon subluxation (rare)
- •Scar sensitivity
- •Recurrence: usually missed septum
Key Points
- •Finkelstein is pathognomonic
- •Injection first-line
- •EPB septum is key at surgery
- •90%+ success with proper release
- •New mothers: postpartum hormones