Disc Degeneration and Lower Back Pain
Classification Systems
Critical Must-Knows
- Discogenic Pain: Axial, deep, worse with flexion/loading
- MRI Findings: Degeneration is common in asymptomatic people - clinical correlation is key
- Modic Changes: Type I (inflammatory) correlates best with pain
- Kirkaldy-Willis Cascade: Dysfunction to Instability to Stabilization
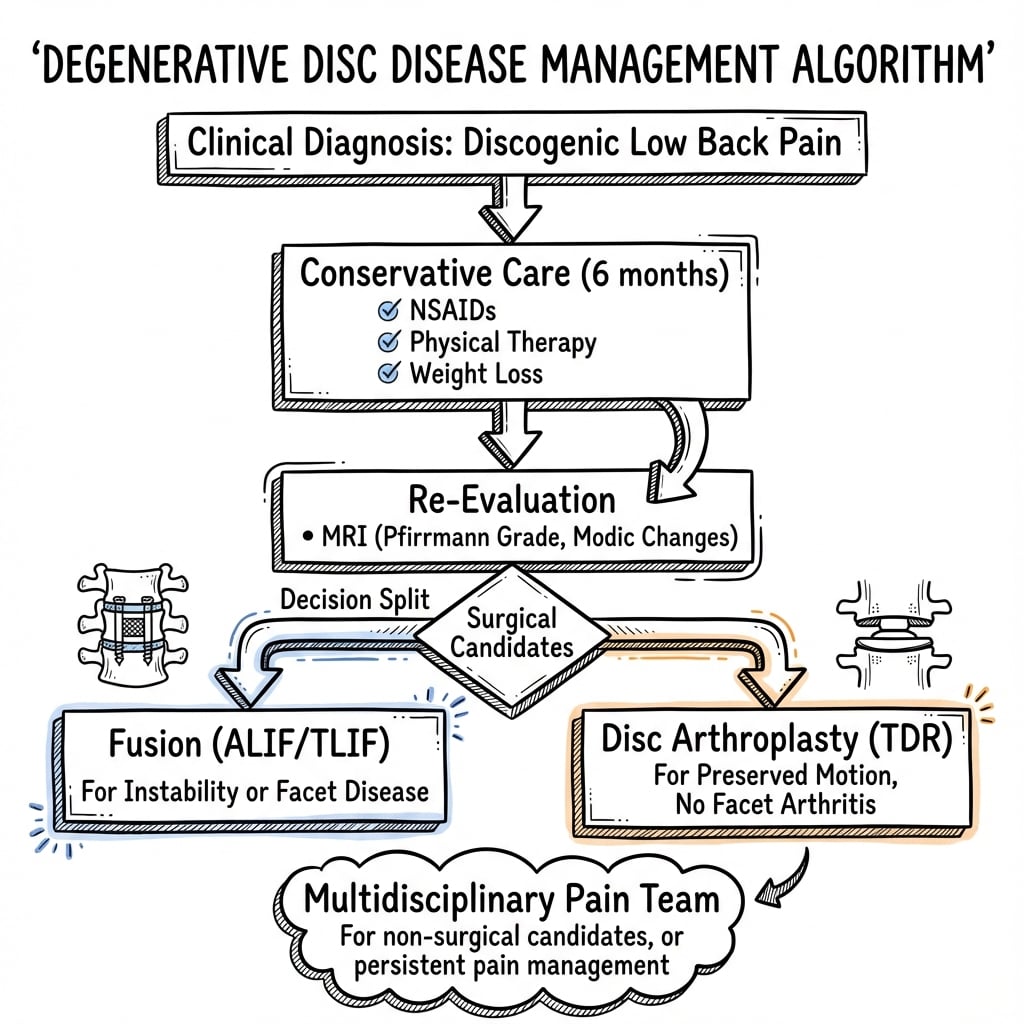
- Conservative First: 6-12 months of physio/NSAIDs before surgery
Clinical Pearls
- "Modic I indicates active inflammation and pain
- "MRI changes are not a diagnosis in isolation
- "Conservative management works for the vast majority
- "Surgery is a last resort for refractory disability
Clinical Imaging
Imaging Gallery




Exam Warning
MRI ≠ Diagnosis
30% of 20yr / 90% of 60yr olds have disc degeneration. A dark disc alone is not an indication for surgery.
Clinical Correlation
Pathology must correlate with concordant pain. Treating MRI findings without clinical correlation leads to poor outcomes.
At a Glance
Degenerative disc disease (DDD) is the aging process of intervertebral discs characterized by proteoglycan loss, dehydration, and annular tears. It presents as mechanical, flexion-aggravated axial back pain. MRI shows Modic changes (Type I = inflammation, Type II = fatty degeneration, Type III = sclerosis). Critical principle: imaging must correlate with concordant clinical pain - treating MRI findings alone leads to poor outcomes. Conservative management for 6-12 months is first-line. Surgery (fusion or arthroplasty) is reserved for single-level disease with intractable symptoms and positive provocative discography.
Key Facts
| Aspect | Key Information |
|---|---|
| Definition | Aging process of disc with loss of hydration/structure |
| Pain Pattern | Axial, mechanical, flexion-aggravated |
| Pathology | Proteoglycan loss, dehydration, annular tears |
| Key Sign | Modic Type I changes (inflammation) |
| Imaging | MRI is gold standard (high sensitivity, low specificity) |
| First Line | Conservative care (6-12 months) |
| Surgical Indication | Intractable pain, disability, single-level disease |
| Gold Standard Surgery | Fusion (Interbody) |
| Alternative | Disc Arthroplasty (in selected patients) |
I-II-IIIModic Types
| I | Inflammation Edema: T1 Dark, T2 Bright (Water) |
| II | Fat Fatty Marrow: T1 Bright, T2 Bright |
| III | Sclerosis Bone Sclerosis: T1 Dark, T2 Dark |
| I | Inflammation Edema: T1 Dark, T2 Bright (Water) |
| II | Fat Fatty Marrow: T1 Bright, T2 Bright |
| III | Sclerosis Bone Sclerosis: T1 Dark, T2 Dark |
Hook:I=Inflammation, II=Fat (Two=Tu=Tub of lard), III=Scar (Sclerosis)
DISKirkaldy-Willis Cascade
| D | Dysfunction Early tears, synovitis, minor herniation |
| I | Instability Disc resumption, laxity, subluxation |
| S | Stabilization Osteophytes, fibrosis, stiffening (less pain) |
| D | Dysfunction Early tears, synovitis, minor herniation |
| I | Instability Disc resumption, laxity, subluxation |
| S | Stabilization Osteophytes, fibrosis, stiffening (less pain) |
Hook:The disc goes DIS-functional
SADDiscogenic Pain Flags
| S | Sitting Worse with sitting (increased intradiscal pressure) |
| A | Axial Central back pain, not legs |
| D | Deep Deep, aching quality |
| S | Sitting Worse with sitting (increased intradiscal pressure) |
| A | Axial Central back pain, not legs |
| D | Deep Deep, aching quality |
Hook:Disc pain makes you SAD
Overview and Epidemiology
Degenerative Disc Disease (DDD) is a clinical syndrome characterized by pain and dysfunction stemming from the natural aging process of the intervertebral disc. It represents a continuum from physiological aging to pathological condition. The distinction between "aging" and "disease" is defined by the presence of symptoms, disproportionate loss of function, and quality of life impact.
Epidemiology
Prevalence
- Degeneration is ubiquitous with age. It is present in:
- 37% of asymptomatic 20-year-olds
- 80% of asymptomatic 50-year-olds
- 96% of asymptomatic 80-year-olds
- Symptomatic DDD is less common but is a leading cause of disability worldwide. Back pain is the single leading cause of disability globally.
- Genetic Influence: Genetics is the strongest predictor (70% heritability) of disc degeneration, far outweighing occupational factors. Key genes include Vitamin D receptor, Aggrecan, and Collagen IX polymorphisms.
Risk Factors
- Non-Modifiable: Genetics (Twin studies show strong concordance), Age.
- Modifiable:
- Smoking: Critically important. Nicotine inhibits chondrocyte proliferation and causes vasoconstriction of the subchondral vascular network, starving the disc.
- Obesity: Increases mechanical load and creates a systemic pro-inflammatory state.
- Occupation: Long-term whole-body vibration (truck driving) and heavy lifting.
- Diabetes: Microvascular disease impairs endplate nutrition.
Natural History
- The condition typically runs a relapsing-remitting course.
- There is a tendency for pain to improve over decades as the spine proceeds to the "Stabilization" phase (stiffening/restabilization).
- Exam Pearl: Elderly patients often have less back pain but signs of stenosis (neurogenic claudication) due to osteophytes.
Pathophysiology
Anatomy of the Disc
The intervertebral disc is the largest avascular structure in the body, relying on diffusion for nutrition.
- Nucleus Pulposus (NP):
- Central, gelatinous core.
- Composed of Type II Collagen and Proteoglycans (Aggrecan).
- Aggrecan is highly hydrophilic. The high water content (80% in youth) creates hydrostatic pressure to resist axial compression and distribute load.
- Annulus Fibrosus (AF):
- Peripheral, tough outer ring arranged in lamellar sheets.
- Type I Collagen dominates (tensile strength).
- Contains the nucleus and attaches to vertebral endplates via Sharpey's fibers.
- Vertebral Endplate:
- Hyaline cartilage interface between disc and bone.
- Critical for nutrition: Glucose and oxygen diffuse from vertebral body marrow capillaries through the endplate to the disc cells. Sclerosis of the endplate blocks this supply.
- Nutritional Failure: This is the 'Final Common Pathway' of degeneration. Factors impeding marrow diffusion include atherosclerosis, smoking (vasoconstriction), and vibration.
Disc Innervation
The sinuvertebral nerve (recurrent meningeal nerve) supplies the posterior longitudinal ligament and the outer 1/3 of the annulus fibrosus.
- Neoneurogenesis: In healthy discs, the inner annulus and nucleus are aneural. In painful DDD, nerve fibers accompanied by blood vessels (neovascularization) grow deep into the nucleus.
- Mechanism: This ingrowth is driven by Neurotrophins (NGF, BDNF) expressed by degenerative chondrocytes. This explains how a deeper structure can become the source of significant pain.
Biochemical Changes
Degeneration involves a shift from anabolic (building) to catabolic (breaking) metabolism:
- Proteoglycan Loss: Decreased aggrecan synthesis and fragmentation leads to reduced water-binding capacity. The nucleus loses turgor and height.
- Collagen Switch: Shift from Type II (cartilage-like) to Type I (fibrotic) collagen in the nucleus. The distinction between nucleus and annulus blurs.
- Enzymatic Degradation: Upregulation of MMPs (Matrix Metalloproteinases) and ADAMTS enzymes digests the matrix.
- Inflammation: Release of pro-inflammatory cytokines (TNF-alpha, IL-1beta, IL-6) from the degenerating nucleus can sensitize nerve endings (sinuvertebral nerve) in the outer annulus, causing pain even without compression.
The Kirkaldy-Willis Cascade
A classic three-stage model of spinal degeneration:
| Stage | Pathophysiology | Clinical Features | Imaging |
|---|---|---|---|
| 1. Dysfunction | Circumferential annular tears, endplate separation, synovitis. | Intermittent axial pain, "acute back strains". | Normal X-ray, MRI showing "black disc" (desiccation). |
| 2. Instability | Resorption of disc, loss of height, facet capsule laxity. | Catching pain, giving way, severe episodes. | Traction spurs, vacuum phenomenon, dynamic instability (translation). |
| 3. Stabilization | Osteophyte formation, fibrosis, stiffening. | Reduced back pain, developing stenosis symptoms from hypertrophy. | Bridging osteophytes, severe disc collapse, foraminal stenosis. |
Classification
Pfirrmann Classification (MRI T2 Weighting) Used to grade the degree of disc degeneration based on structure and signal intensity.
| Grade | Structure | Signal Intensity | Disc Height | Description |
|---|---|---|---|---|
| I | Homogeneous | Hyperintense (Bright) | Normal | Juvenile/Normal |
| II | Heterogeneous (Streak) | Hyperintense | Normal | Early Adult |
| III | Heterogeneous | Intermediate (Grey) | Normal/Slight loss | Degenerative |
| IV | Heterogeneous | Hypointense (Dark) | Moderate loss | "Black Disc" |
| V | Collapsed | Hypointense (Black) | Collapsed | End-stage |
Clinical Presentation
History
Cardinal Feature: Axial Low Back Pain (Midline).
- Nature: Deep, aching, dull. Quality can be severe ("toothache in the back"). Contrast this with sharp, electric radicular pain.
- Aggravating Factors (Loading):
- Flexion: Sitting, bending forward (increases intradiscal pressure).
- Axial Load: Lifting, standing static for long periods.
- Valsalva: Coughing/sneezing (increases intrathecal pressure - caution: also herniation feature).
- Relieving Factors (Unloading):
- Extension, lying supine, walking.
- Pattern:
- Often intermittent "flare-ups" lasting weeks, settling to baseline.
- Stiffness in mornings (gel phenomenon) lasting minutes.
- Biopsychosocial Factors: Screen for "Yellow Flags" (fear avoidance, catastrophizing, depression) as these are stronger predictors of disability than MRI findings.
Red Flags (Rule Out):
- Weight loss, night pain, history of cancer (Malignancy).
- Fever, IVDU, immunosuppression (Infection).
- Significant trauma (Fracture).
- Saddle anaesthesia, bladder dysfunction (Cauda Equina Syndrome).
Physical Examination
Findings in pure DDD are often non-specific. The exam is used to rule out other pathology (hips, roots).
- Inspection: Loss of lordosis (flat back) due to muscle spasm/guarding. Lateral shift (list).
- Palpation: Midline tenderness (spinous processes/interspinous). Paraspinal muscle spasm ("washboarding").
- Range of Motion:
- Flexion often limited and painful ("fingertip to floor" distance).
- Extension may be preserved (unless Facet Arthropathy present).
- Catching or "painful arc" during return from flexion suggests instability.
- Neurology:
- Usually normal in isolated DDD.
- Check for concordant radiculopathy (requires nerve root compression).
- Provocative Tests:
- Disc Loading: Axial compression may reproduce back pain.
- Straight Leg Raise: Usually negative in pure discogenic pain (unless HNP present).
Differential Diagnosis
Back pain is a symptom with many causes. Differentiating "Mechanical" from "Non-Mechanical" is key.
1. Mechanical Back Pain
- Facet Joint Arthropathy: Worse with extension/rotation. Paramedian tenderness.
- Spondylolisthesis: Instability pain, "step-off" on exam.
- Lumbar Strain: Acute muscle injury, self-limiting.
- Sacroiliac Joint Dysfunction: Pain below L5, Fortin's finger test positive, Patrick's FABER test.
2. Non-Mechanical Assessment
- Tumour: Multiple Myeloma, Metastases (Breast, Lung, Prostate, Kidney, Thyroid). Night pain.
- Infection: Discitis/Osteomyelitis. Fever, unremitting pain. Modic I changes can mimic infection.
- Inflammatory: Ankylosing Spondylitis. Morning stiffness greater than 30 mins, young male, bamboo spine.
3. Visceral Referral
- AAA: Pulsatile mass, cardiovascular risk factors.
- Renal: Kidney stones (colic), Pyelonephritis (fever/CVA tenderness).
- Pancreatitis: Penetrating back pain.
Investigations
Imaging
1. Plain Radiographs (X-ray)
- AP/Lateral: Assess alignment (Scoliosis, Lordosis).
- Findings:
- Loss of disc height (vacuum phenomenon).
- Endplate sclerosis.
- Vacuum phenomenon (nitrogen gas in clefts - sign of instability).
- Osteophytes (traction spurs).
- Flexion/Extension Views: Critical to rule out instability (Spondylolisthesis) prior to fusion surgery. (translation greater than 3mm or angulation greater than 10 degrees).
2. MRI (Gold Standard)
- T2 Sagittal: Best for hydration status (Pfirrmann grade).
- High Intensity Zone (HIZ): Bright spot in posterior annulus on T2. Correlates with annular tear. High specificity for discogenic pain (but controversial).
- Modic Changes: Endplate signal abnormalities.
- Features: "Black Disc", loss of height, bulging, nerve root compression.
3. Discography (Provocative)
- Injection of contrast/saline into disc nucleus under fluoroscopy.
- Positive Test: Reproduction of patient's exact familiar pain (concordant pain) + Morphological degeneration + Negative control level.
- Current Status: Highly controversial. High false-positive rate. Risk of damaging healthy discs (accelerated degeneration). Used rarely for indeterminate cases prior to fusion.
- Nuclear Medicine: SPECT-CT may show "hot" uptake at active degenerative levels, aiding localization.
Imaging Examples

Management
Complications
Surgical Complications
1. General Spinal Surgery risks:
- Infection (1-3%).
- Dural tear (CSF leak).
- Nerve root injury.
- DVT/PE.
2. Fusion Specific:
- Pseudarthrosis (Non-union): Failure of bone to fuse. Risk factors: Smoking, NSAIDs, Diabetes. Causes persistent pain leading to Revision.
- Adjacent Segment Disease (ASD): Accelerated degeneration at levels above/below fusion due to increased stress. Rate: 2-3% per year.
- Hardware Failure: Screw loosening, cage migration.
3. Arthroplasty Specific:
- Implant migration/subsidence.
- Heterotopic ossification (auto-fusion).
- Polyethylene wear debris (rare).
- Difficulty of revision (anterior approach scar tissue - "vascular disaster" risk on revision).
4. Anterior Approach Risks (ALIF/TDR):
- Vascular Injury: Iliac vein/artery (life-threatening).
- Retrograde Ejaculation: Injury to Superior Hypogastric Plexus (males). Rate 1-5%.
- Ureteral Injury: Rare.
Outcomes and Prognosis
- Natural History: Favorable. Many patients stabilize ("burn out") as the spine stiffens.
- Conservative Care: Good function executable for most.
- Fusion Results:
- Pain reduction: Typically 50-70% reduction (not 100%).
- Return to work: Variable.
- Satisfaction: 60-75% in well-selected patients.
- Predictors of Poor Outcome:
- Psychosocial factors (Yellow flags, Workers Comp, Depression).
- Smoking.
- Obesity.
- Multi-level disease.
Evidence Base
Swedish Lumbar Spine Study (2001 Volvo Award)
- RCT of 294 patients with severe chronic LBP and L4-S1 disc degeneration: fusion vs non-surgical care
- Back pain reduced 33% with fusion vs 7% non-surgical at 2 years (P=0.0002)
- 63% of surgical patients rated 'much better/better' vs 29% non-surgical (P less than 0.0001)
- Net back-to-work rate favoured surgery (36% vs 13%); early surgical complication rate 17%
ProDisc-L FDA IDE Trial
- RCT of 286 patients: ProDisc-L total disc replacement vs circumferential fusion for 1-level DDD (L3-S1)
- At 24 months ODI improvement in 91.8% of TDR vs 84.5% of fusion patients
- Neurological success and patient satisfaction superior in TDR group (P=0.034, P=0.015)
- Functional range of motion maintained in 93.7% of TDR patients (mean 7.7 degrees)
MRI Degeneration in Asymptomatic Individuals
- Systematic review of 33 studies, 3110 asymptomatic individuals
- Disc degeneration prevalence rose from 37% at age 20 to 96% at age 80
- Disc bulge prevalence rose from 30% at age 20 to 84% at age 80
- Degenerative imaging features are largely part of normal aging
Modic Endplate Changes Classification
- Defined Type I (T1 dark/T2 bright, edema-fibrovascular) and Type II (T1 bright, fatty marrow) endplate changes
- All endplate changes associated with degenerative disc disease at that level
- Type I converted to Type II over 14 months to 3 years in 5 of 6 patients followed
- Type II changes remained stable over 2-3 years
Kirkaldy-Willis Degenerative Cascade
- Described the three-phase model of segmental spinal degeneration
- Dysfunction phase: annular tears, facet synovitis, minor instability
- Instability phase: disc resorption, height loss, capsular laxity and abnormal motion
- Stabilization phase: osteophytosis and fibrosis reduce motion and often reduce axial pain
MCQ Practice Points
Discogenic Pain Localisation
Q: What MRI finding helps identify the symptomatic disc level in degenerative disc disease?
A: Modic Type I changes (bone marrow oedema appearing as T1 hypointense, T2 hyperintense) correlate most strongly with active inflammation and symptomatic disc degeneration. Type II (fatty replacement) and Type III (sclerosis) are less commonly associated with active symptoms.
Discography Role
Q: What is the role of provocative discography in degenerative disc disease?
A: Provocative discography identifies concordant pain (reproduction of typical symptoms) to localise the painful level before fusion. However, it has high false positive rates (up to 40% in asymptomatic individuals) and is controversial. Best used when imaging shows multi-level disease and clinical localisation is uncertain.
Fusion vs Non-Operative
Q: What does the evidence show for fusion surgery vs non-operative treatment in degenerative disc disease?
A: Systematic reviews show modest benefit at best. The SPORT trial showed minimal difference between surgical and non-surgical groups for discogenic pain. Intensive multidisciplinary rehabilitation is often equally effective. Surgery is reserved for patients with failed prolonged conservative treatment (greater than 6-12 months), confirmed single-level disease, and concordant pain on discography.
Motion Preservation
Q: When is disc arthroplasty (artificial disc replacement) indicated over fusion?
A: Disc arthroplasty is indicated for single-level disease, intact facet joints, no significant instability, and younger patients (typically less than 60 years). Contraindications include: multi-level disease, facet arthropathy, instability, osteoporosis, or previous posterior surgery at that level.
Guidelines, Registries & Global Practice
Global Epidemiology
- Low back pain is the single leading cause of years lived with disability worldwide (Global Burden of Disease).
- Disc degeneration on imaging rises with age (37% at 20 years to 96% at 80 years; Brinjikji 2015) and is largely asymptomatic - prevalence is similar across populations, so it is a global aging phenomenon rather than a regional disease.
- Genetics carries the strongest weight in heritability studies, outweighing occupational mechanical load.
Society Guidance (Side by Side)
| Body | Position on Imaging | Position on Surgery for Axial DDD |
|---|---|---|
| NICE (UK) | Do not routinely offer imaging in non-specialist settings; reserve MRI for suspected serious pathology or when result changes management | Do not offer spinal fusion for low back pain outside a randomised trial; emphasise exercise and combined physical/psychological programmes |
| NASS / AAOS (US) | MRI is the modality of choice when red flags or failed conservative care; degeneration alone is non-diagnostic | Fusion reserved for carefully selected refractory single/two-level disease after failed structured non-operative care |
| EFORT / European consensus | Correlate imaging strictly with concordant symptoms; discography controversial | Motion-preserving arthroplasty an option in young patients with intact facets and single-level disease |
Consistent global message: at least 3-6 months (commonly up to 12) of structured non-operative care; never operate on imaging alone; document concordant clinical correlation before any fusion or arthroplasty.
Registry & Outcome Notes
- Spine procedures are tracked in national registries such as the British Spine Registry, Swespine (Sweden) and the Norwegian (NORspine) registry. Registry data consistently show smaller, more variable benefit for fusion in pure axial discogenic pain than for radiculopathy or deformity.
- Adjacent segment disease accrues at roughly 2-3% per year after lumbar fusion in registry and cohort follow-up.
High- vs Limited-Resource Variation
- High-resource settings: ready MRI access (with attendant risk of over-imaging), multidisciplinary pain programmes, and access to arthroplasty implants.
- Limited-resource settings: emphasis on clinical diagnosis, exercise and analgesia; imaging and instrumented surgery rationed to red-flag or instability cases. Across all settings the core principle is unchanged: conservative-first, image only to change management, operate only on concordant refractory disease.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Chronic Low Back Pain assessment
"A 40-year-old labourer presents with 2 years of worsening mechanical back pain. MRI shows L5/S1 dark disc with Modic I changes. He wants a 'fusion' so he can return to heavy work."
MRI Findings: 'Dark disc' (desiccation) at L5/S1 indicates Pfirrmann IV/V degeneration. Modic I changes (marrow edema) suggest active inflammation and correlate with discogenic pain source.
Suitability Factors: psychosocial status (yellow flags), smoking status, obesity, response to conservative care, realistic expectations. Labourer job is a RISK factor for poor outcome.
Risks: Fusion alters biomechanics. Heavy labor increases stress on adjacent segments (ASD risk). Fusion may not provide 100% pain relief fitting for heavy duties.
Success Rate: Literature quotes 60-70% 'good/excellent' result. This means improvement, not cure. Return to heavy manual labor is essentially 50/50.
Adjacent Segment Disease
"A 65-year-old female had an L4/5 fusion 10 years ago. She presents with recurrence of back pain and new L3 radiculopathy (pain radiating to anterior thigh/knee)."
Diagnosis: Adjacent Segment Disease (ASD) at L3/4 (level above fusion).
Pathophysiology: Rigid fusion at L4/5 eliminates motion. Motion and stress are transferred to adjacent levels (L3/4), accelerating degeneration (hypertrophy, stenosis, instability). L3 radiculopathy suggests L3/4 pathology.
Incidence: Approximately 2-3% per year. At 10 years, ~25% risk of significant ASD.
Management: Initially conservative (as per primary DDD). If refractory, surgical extension of fusion (L3-5) or decompression alone if stable stenosis.
DEGENERATIVE DISC DISEASE
Clinical summary
Pathology Facts
- •**Water Loss**: Proteoglycan/Aggrecan loss leads to dehydration
- •**Collagen**: Type II (nucleus) replaced by Type I (fibrosis)
- •**Kirkaldy-Willis**: Dysfunction to Instability to Stabilization
Imaging & Signs
- •**Modic I**: Edema (T1 Dark, T2 Bright) - Painful
- •**Modic II**: Fat (Bright/Bright) - Stable
- •**Pfirrmann**: MRI Grading I-V of disc height/signal
- •**HIZ**: High Intensity Zone - Posterior annular tear
Management Rules
- •**First Line**: Conservative care for 6-12 months is mandatory
- •**Red Flag**: Don't operate on asymptomatic radiologic findings
- •**Gold Standard**: Fusion (ALIF/TLIF) for single-level refractory pain
- •**Alternative**: TDR (Arthroplasty) for young, motion preservation
- •**Outcome**: 60-70% pain improvement. Not a perfect cure.
Self-Assessment Quiz
References
- Fritzell P, Hagg O, Wessberg P, Nordwall A. 2001 Volvo Award Winner in Clinical Studies: Lumbar fusion versus nonsurgical treatment for chronic low back pain: a multicenter randomized controlled trial from the Swedish Lumbar Spine Study Group. Spine. 2001;26:2521-2532.
- Brinjikji W, Luetmer PH, Comstock B, et al. Systematic literature review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol. 2015;36(4):811-6.
- Modic MT, Steinberg PM, Ross JS, et al. Degenerative disk disease: assessment of changes in vertebral body marrow with MR imaging. Radiology. 1988;166:193-199.
- Kirkaldy-Willis WH, Farfan HF. Instability of the lumbar spine. Clin Orthop Relat Res. 1982;(165):110-23.
- Zigler J, Delamarter R, Spivak JM, et al. Results of the prospective, randomized, multicenter Food and Drug Administration investigational device exemption study of the ProDisc-L total disc replacement versus circumferential fusion for the treatment of 1-level degenerative disc disease. Spine. 2007;32:1155-1162.