Dermatomes, Myotomes & Spinal Nerve Root Anatomy
Weak great-toe extension (EHL) and dorsiflexion/foot inversion-eversion; sensory change over the dorsum of the foot / great toe; weak hip abduction; reflexes usually preserved. (Often a far-out or paracentral L4/5 disc.)
Weak ankle plantarflexion (calf), sensory change over the lateral border and sole/heel of the foot, and a reduced/absent Achilles (ankle) reflex. (Often an L5/S1 disc.)
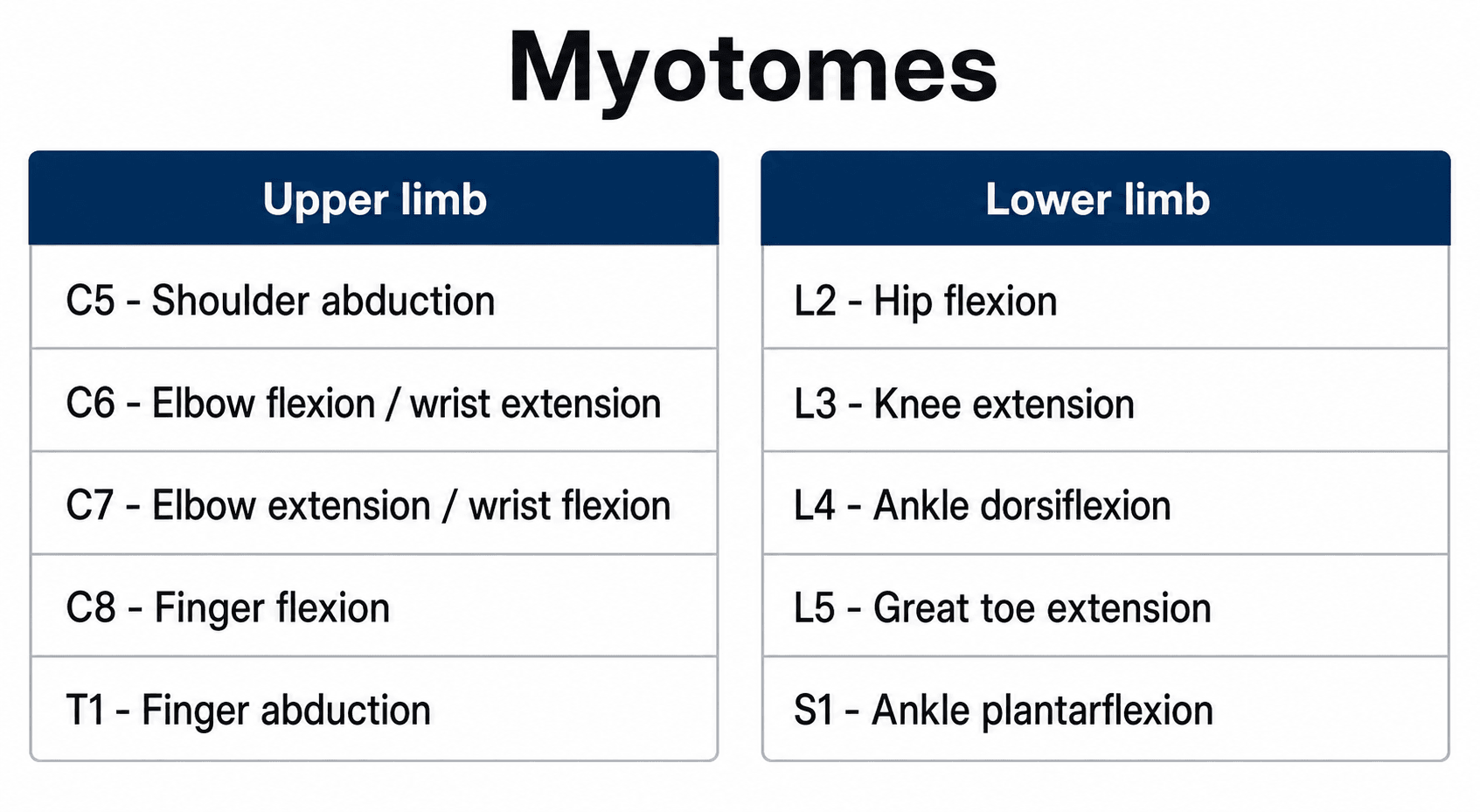
C5-T1Upper-Limb Myotomes (count down the arm)
Hook:Down the arm C5→T1: flex elbow, extend wrist, extend elbow, flex fingers, spread fingers. Pair with the lower-limb L2→S1 card.
Overview
Dermatome and myotome knowledge is the backbone of the neurological examination in orthopaedics and spine practice — it is how you turn "leg weakness and numbness" into "an L5 root lesion" or "a T6 sensory level". The two facts that make it clinically usable are that segments overlap (sensory loss is a fuzzy band, weakness is partial) and that the body has been standardised by the ISNCSCI into reproducible key sensory points and key muscles. Approach the topic in three layers: the maps (which level supplies which skin, muscle and reflex), the localisation logic (combine three findings to pinpoint a root), and the two big applications — distinguishing the common lumbar radiculopathies and performing the ASIA examination that grades and prognosticates a spinal cord injury.
Definitions & Principles
Dermatome vs Myotome
- Dermatome: the area of skin supplied by a single spinal (dorsal root) nerve.
- Myotome: the group of muscles supplied by a single spinal nerve root (most muscles are supplied by more than one root).
- Sclerotome / viscerotome: bone and viscera supplied by a segment (less examined).
The Key Maps
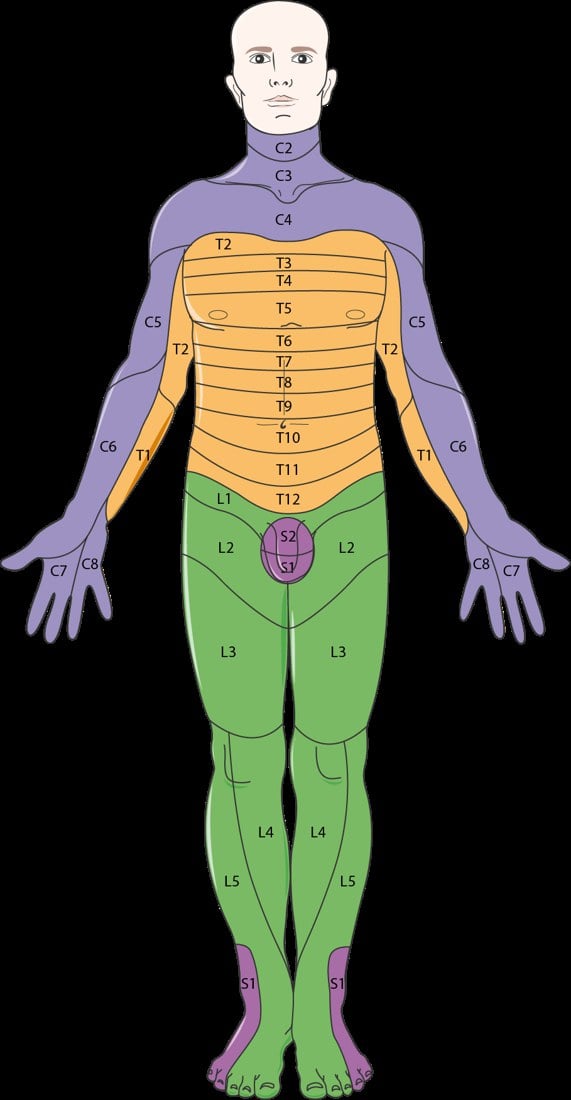
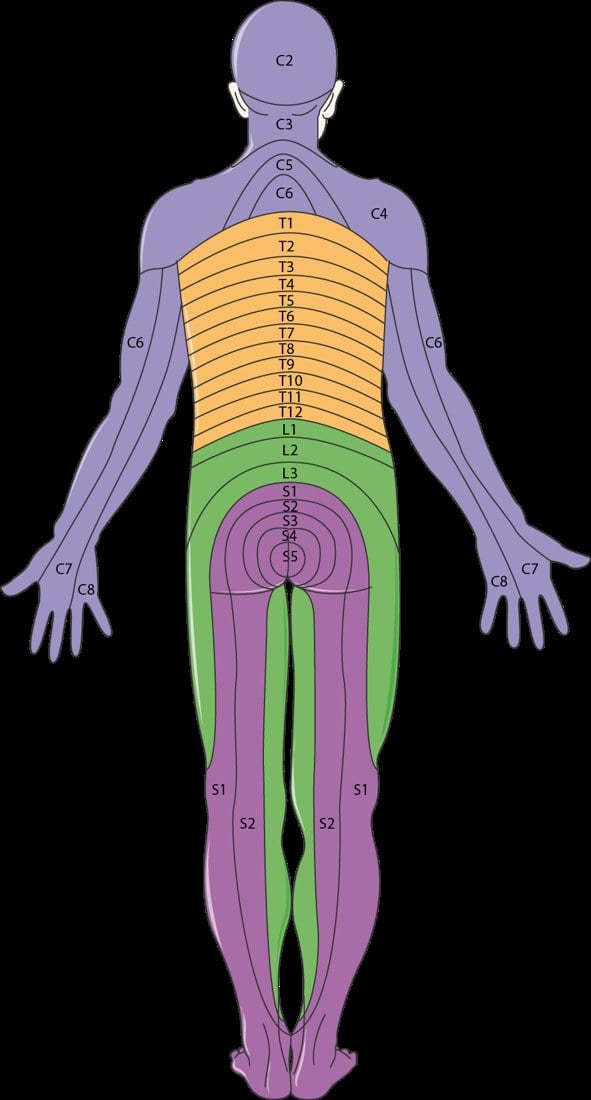
Landmark Dermatomes (ISNCSCI key points)
- C2 occiput - C3 posterior neck/supraclavicular fossa - C4 acromioclavicular joint
- C5 lateral antecubital fossa (lateral arm) - C6 thumb - C7 middle finger - C8 little finger - T1 medial antecubital fossa (medial forearm)
- T4 nipple - T6 xiphisternum - T10 umbilicus - L1 inguinal region/groin
- L2 anterior mid-thigh - L3 medial femoral condyle (medial knee) - L4 medial malleolus - L5 dorsum of the foot at the 3rd MTP joint / great toe - S1 lateral heel
- S2 popliteal fossa - S3 ischial tuberosity - S4-5 perianal
L2-S2Lower-Limb Myotomes (count up the leg)
Hook:Up the back of the leg: L2 flex hip, L3 straighten knee, L4 lift foot, L5 lift toe, S1 push off.
Nerve Root Reflex Levels and Grading
The deep tendon reflexes pin a few roots precisely and are an independent third data point alongside the myotome and dermatome:
- Root level
- C5–C6
- Root level
- C6
- Root level
- C7
- Root level
- L3–L4
- Root level
- S1
In the ISNCSCI/ASIA examination each key muscle is graded 0–5 (the MRC scale: 0 none → 3 movement against gravity → 5 normal) and each key sensory point 0–2 (0 absent, 1 impaired/altered, 2 normal) for light touch and pin-prick. Summing these yields the motor and sensory scores, the sensory and motor levels, and the single neurological level of injury (the most caudal level with normal sensory AND at least antigravity motor function, with the level above intact).
The same reflex that localises a root also flags a cord lesion — by whether it is reduced or exaggerated, the single most important interpretive step examiners test:
- Radiculopathy = a LOWER motor neuron pattern at the level: the affected reflex is diminished or absent, with hypotonia, segmental wasting and fasciculations and weakness in that myotome (e.g. an absent Achilles in S1, an absent biceps jerk in C5-6).
- Myelopathy / cord compression = an UPPER motor neuron pattern BELOW the level: reflexes are brisk/exaggerated, with clonus, spasticity, an up-going plantar (Babinski), a positive Hoffmann sign (flicking the middle-finger nail flexes the thumb/index), and Lhermitte's phenomenon — while a single root at the level of the cord lesion may still be LMN (a wasted, areflexic segment with brisk reflexes below it).
- The inverted supinator (radial) reflex is the classic crossover sign: tapping brachioradialis gives little brachioradialis contraction but brisk finger flexion, localising a C5-C6 cord/myelopathic level (the C5-6 LMN arc is interrupted while C8 below is disinhibited) — a peripheral musculocutaneous/C6 lesion does NOT do this.
So a "depressed reflex" is a root sign, a "brisk reflex with clonus/Babinski/Hoffmann" is a cord (UMN) sign, and the two can coexist at the compressed cervical level — distinguishing radiculopathy, myelopathy and myeloradiculopathy from the same examination.
Clinical Application
Localising a Radiculopathy
- Combine the key muscle (myotome) + dermatome + reflex to localise the level.
- C6: weak wrist extension/elbow flexion, thumb sensation, reduced brachioradialis reflex.
- C7: weak elbow extension (triceps), middle-finger sensation, reduced triceps reflex.
- L4: weak dorsiflexion, medial-malleolus sensation, reduced knee reflex.
- L5: weak great-toe extension, dorsum-of-foot sensation, reflexes preserved.
- S1: weak plantarflexion, lateral-foot sensation, reduced Achilles reflex.
ASIA Impairment Scale and Cauda Equina
The ASIA Impairment Scale (AIS)
The completeness and severity of a spinal cord injury are graded A–E, anchored on sacral sparing:
- Definition
- No motor or sensory function preserved in the sacral segments S4–S5 (no sacral sparing)
- Definition
- Sensory but not motor function preserved below the neurological level, including the sacral segments S4–S5
- Definition
- Motor function preserved below the level, with more than half the key muscles below the level grading less than 3
- Definition
- Motor function preserved below the level, with at least half the key muscles below the level grading 3 or more
- Definition
- Sensory and motor function normal in all segments (in a patient who had prior deficits)
The crucial conceptual point is that sacral sparing distinguishes complete (A) from incomplete (B–D) injuries — which is why the perianal examination (S4–5 light touch/pin-prick, deep anal pressure and voluntary anal contraction) is mandatory and never omitted. Spinal shock (transient areflexia) must resolve — confirmed by return of the bulbocavernosus reflex — before a complete injury is declared.
"Incomplete" (AIS B-D) is not one thing: the dermatome/myotome map plus the three long tracts (corticospinal = motor, dorsal columns = proprioception/vibration/light touch, spinothalamic = pain/temperature) define recognisable syndromes the exam expects you to name:
- Central cord syndrome — the commonest incomplete injury; a hyperextension injury in an older patient with cervical spondylosis (often without fracture). Upper limbs (especially the hands) are weaker than the lower limbs (medial-to-lateral somatotopy of the corticospinal tract), with variable "cape" sensory loss and usual sacral sparing. Generally managed without emergent surgery; most regain ambulation, hand recovery is least.
- Brown-Séquard (cord hemisection) — penetrating/lateral mass injury: ipsilateral loss of motor (corticospinal) and dorsal-column (proprioception/vibration) function, with contralateral loss of pain and temperature (spinothalamic) beginning a few levels below (fibres decussate within 1-2 segments). Best prognosis of the incomplete syndromes.
- Anterior cord syndrome — anterior spinal artery territory / flexion-compression: loss of motor and pain/temperature with PRESERVED proprioception, vibration and light touch (dorsal columns spared). Worst prognosis.
- Posterior cord syndrome — rare: isolated dorsal-column loss (proprioception/vibration → sensory ataxia and a positive Romberg) with motor and pain/temperature preserved.
Conus medullaris vs cauda equina (both involve the lumbosacral roots/segments and saddle anaesthesia, but localise differently): the conus (cord segments around L1-L2) gives an early, symmetrical, severe bladder/bowel and saddle deficit with mixed UMN + LMN signs (an up-going plantar can persist), relatively symmetric and less radicular pain; the cauda equina (roots below the conus) gives an asymmetric, LMN picture with prominent radicular pain, areflexia and a later but progressive bladder dysfunction. Both demand urgent MRI; cauda equina compression is the classic decompression emergency.
Cauda equina syndrome
The same lumbosacral roots that the dermatome/myotome map describes form the cauda equina below the conus (which ends at about L1–L2 in adults). Compression — classically a large central lumbar disc — produces cauda equina syndrome, a surgical emergency: bilateral sciatica, saddle (S2–4) anaesthesia, bladder dysfunction (retention with overflow), bowel/faecal incontinence, and reduced anal tone. It is the lower-limb counterpart of the sacral-sparing concept and demands urgent MRI and decompression (the evidence favours early surgery to optimise recovery of continence). Always check perianal sensation, anal tone and post-void residual in any patient with bilateral leg symptoms or new urinary dysfunction.
Guidelines, Registries & Global Practice
Global Practice Picture
Dermatome and myotome mapping is universal clinical knowledge, standardised internationally by the ISNCSCI (ASIA) for spinal cord injury and used everywhere to localise radiculopathy. The key sensory points and key muscles provide a common, reproducible language across clinicians and registries.
Side-by-Side Synthesis
- Key muscle (myotome)
- Elbow flexion (biceps)
- Key sensory point (dermatome)
- Lateral arm
- Reflex
- Biceps (C5-6)
- Key muscle (myotome)
- Wrist extension
- Key sensory point (dermatome)
- Thumb
- Reflex
- Brachioradialis
- Key muscle (myotome)
- Elbow extension (triceps)
- Key sensory point (dermatome)
- Middle finger
- Reflex
- Triceps
- Key muscle (myotome)
- Finger flexion
- Key sensory point (dermatome)
- Little finger
- Reflex
- -
- Key muscle (myotome)
- Ankle dorsiflexion
- Key sensory point (dermatome)
- Medial malleolus
- Reflex
- Knee (L3-4)
- Key muscle (myotome)
- Great toe extension (EHL)
- Key sensory point (dermatome)
- Dorsum great toe
- Reflex
- -
- Key muscle (myotome)
- Ankle plantarflexion
- Key sensory point (dermatome)
- Lateral foot/heel
- Reflex
- Achilles
Evidence Base
The dermatome/myotome maps themselves are settled anatomy; the modern evidence (both papers below checked against PubMed) concerns the ISNCSCI examination built on them. Kirshblum confirms the standardised key-sensory-point/key-muscle exam is the predominant tool for classifying and prognosticating spinal cord injury (most recovery in the first 3–9 months), and Walden shows it is reproducible enough to be computerised and used worldwide. The practical message: the value is in performing the exam consistently — the maps are only as useful as the disciplined application that turns them into a level and an AIS grade.
Characterizing Natural Recovery after Traumatic Spinal Cord Injury
- The ISNCSCI (with the ASIA Impairment Scale) is the predominant tool to classify and predict outcomes after traumatic spinal cord injury
- Completeness is defined by the sacral sparing definition
- Most AIS conversion and motor recovery occurs within the first 6-9 months, fastest in the first 3 months
- Initial AIS grade and zone of partial preservation influence prognosis
Computer International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) algorithms: a review
- Reviews validated computerised ISNCSCI algorithms (EMSCI and Praxis Spinal Cord Institute)
- Algorithms support education, clinical documentation, and consistent classification worldwide
- Over half of surveyed users apply the algorithm regularly in their workflow
- They support, not replace, trained clinicians and allow reclassification with updated ISNCSCI versions