Cervical Extensor Weakness | Chin-on-Chest Deformity | Multifactorial Etiology
CLASSIFICATION BY ETIOLOGY
Critical Must-Knows
- Chin-on-chest deformity with inability to extend neck against gravity
- INEM (isolated neck extensor myopathy) is non-inflammatory myopathy of elderly
- MRI shows fatty infiltration of paraspinal muscles, especially semispinalis cervicis
- Rule out MG and ALS before diagnosing INEM - these require different treatment
- Surgery indicated when conservative care fails and fixed deformity develops
Clinical Pearls
- "Check for ptosis, diplopia, limb weakness to exclude MG/ALS
- "EMG shows myopathic changes in neck extensors with normal limbs in INEM
- "Muscle biopsy shows non-inflammatory myopathy with fiber size variation
- "Posterior-only fusion may fail - often need combined anterior-posterior approach
Clinical Imaging
Imaging Gallery



Critical Dropped Head Syndrome Exam Points
Differential Diagnosis
Always exclude systemic causes: Myasthenia gravis (check AChR antibodies, ptosis, fatigability), ALS (check for fasciculations, hyperreflexia, tongue atrophy), inflammatory myopathy (check CK, muscle biopsy). INEM is a diagnosis of exclusion.
Clinical Examination
Key findings: Patient uses hand to support chin ("chin-on-hand sign"), horizontal gaze impaired, cannot extend neck against gravity, dysphagia common. Symptoms worse at end of day suggests MG.
Imaging Findings
MRI shows fatty infiltration of paraspinal muscles, especially semispinalis cervicis and capitis. T1 hyperintensity indicates fat replacement. May see secondary cervical kyphosis and cord compression.
Surgical Planning
Consider 360-degree approach: Posterior-only fusion has high failure rate due to poor muscle quality. Combined anterior release (if fixed) plus posterior instrumented fusion provides best correction and stability.
Differential Diagnosis of Dropped Head Syndrome
| Condition | Key Features | Investigations |
|---|---|---|
| INEM | Elderly, isolated to neck, non-inflammatory | EMG myopathic in neck, normal limbs, muscle biopsy |
| Myasthenia Gravis | Ptosis, diplopia, fatigability, fluctuating | AChR antibodies, repetitive nerve stimulation, Tensilon test |
| ALS | Fasciculations, hyperreflexia, tongue atrophy | EMG widespread denervation, normal sensory |
| Inflammatory Myopathy | Proximal weakness, elevated CK, rash (dermatomyositis) | CK, ANA, muscle biopsy with inflammation |
| Cervical Spondylosis | Myelopathy signs, radiculopathy, mechanical | MRI cord compression, CT osteophytes |
| Parkinson Disease | Rigidity, tremor, bradykinesia, anterocollis | Clinical diagnosis, response to L-dopa |
At a Glance
Dropped head syndrome (chin-on-chest deformity) results from weakness of cervical extensor muscles, most commonly due to isolated neck extensor myopathy (INEM)—a non-inflammatory myopathy of the elderly. Systemic causes must be excluded first: myasthenia gravis (ptosis, diplopia, fatigability, AChR antibodies), ALS (fasciculations, hyperreflexia, tongue atrophy), and inflammatory myopathy (elevated CK, proximal weakness). MRI demonstrates fatty infiltration of paraspinal muscles, particularly semispinalis cervicis, appearing hyperintense on T1. Patients cannot extend the neck against gravity and use the "chin-on-hand sign" for support. A 3-6 month conservative trial is appropriate; if fixed deformity develops, surgery is indicated—posterior-only fusion has high failure rate due to poor muscle quality, often requiring combined anterior release plus posterior instrumented fusion.
DROPPED - CDROPPED - Causes of Dropped Head
| D | Degenerative Cervical spondylosis, osteoporosis with compression fracture |
| R | Radiation/Rheumatologic Post-radiation myopathy, ankylosing spondylitis |
| O | Other myopathies INEM (isolated neck extensor myopathy) - most common |
| P | Parkinson/Psychiatric Anterocollis in Parkinson disease, camptocormia |
| P | Post-surgical After cervical laminectomy, multilevel decompression |
| E | Endocrine Hypothyroidism, Cushing syndrome |
| D | Disease - neuromuscular MG, ALS, inflammatory myopathy, muscular dystrophy |
| D | Degenerative Cervical spondylosis, osteoporosis with compression fracture | P | Parkinson/Psychiatric Anterocollis in Parkinson disease, camptocormia | D | Disease - neuromuscular MG, ALS, inflammatory myopathy, muscular dystrophy |
| R | Radiation/Rheumatologic Post-radiation myopathy, ankylosing spondylitis | P | Post-surgical After cervical laminectomy, multilevel decompression | ||
| O | Other myopathies INEM (isolated neck extensor myopathy) - most common | E | Endocrine Hypothyroidism, Cushing syndrome |
Hook:DROPPED head needs comprehensive workup - multiple causes exist
NECK - KNECK - Key Muscles Affected
| N | Neck extensors Semispinalis cervicis and capitis - primary muscles |
| E | Erector spinae Longissimus capitis and cervicis |
| C | Capitis muscles Splenius capitis, rectus capitis posterior |
| K | Key exam - resisted extension Test prone head lift against gravity |
| N | Neck extensors Semispinalis cervicis and capitis - primary muscles | C | Capitis muscles Splenius capitis, rectus capitis posterior |
| E | Erector spinae Longissimus capitis and cervicis | K | Key exam - resisted extension Test prone head lift against gravity |
Hook:Semispinalis cervicis is the KEY muscle - check T1 MRI for fatty infiltration
FIX - SFIX - Surgical Principles
| F | Fusion levels C2 to upper thoracic (T2-T4) for adequate anchor |
| I | Instrumentation Posterior screws with possible cement augmentation |
| X | eXtend to thoracic Upper thoracic extension prevents junctional kyphosis |
| F | Fusion levels C2 to upper thoracic (T2-T4) for adequate anchor |
| I | Instrumentation Posterior screws with possible cement augmentation |
| X | eXtend to thoracic Upper thoracic extension prevents junctional kyphosis |
Hook:Extend fusion to thoracic spine - posterior-only often insufficient
Overview and Epidemiology
Dropped Head Syndrome (DHS) refers to severe weakness of the neck extensor muscles resulting in an inability to hold the head up against gravity. The characteristic presentation is a "chin-on-chest" deformity with impaired horizontal gaze.
Terminology:
| Term | Definition |
|---|---|
| Dropped Head Syndrome | Clinical syndrome of neck extensor weakness |
| INEM | Isolated Neck Extensor Myopathy - the primary/idiopathic form |
| Head Drop | Alternative term for the same condition |
| Anterocollis | Similar deformity seen in Parkinson disease |
Epidemiology:
DHS is uncommon but increasingly recognized in the aging population. INEM specifically affects:
- Age typically over 65-70 years
- Female predominance (approximately 2:1)
- No racial predilection identified
Clinical Significance:
DHS significantly impacts quality of life due to impaired horizontal gaze, difficulty with eating and swallowing, respiratory compromise, and social embarrassment. Progressive cervical kyphosis can lead to myelopathy from cord compression.
INEM Definition
Isolated Neck Extensor Myopathy (INEM) was defined by Katz et al. (1996) as a non-inflammatory myopathy restricted to the paraspinal muscles of the neck. It is a diagnosis of exclusion after ruling out systemic neuromuscular disease.
Anatomy of Cervical Extensors
Primary Neck Extensor Muscles
Semispinalis Group (Most Important):
| Muscle | Origin | Insertion | Action |
|---|---|---|---|
| Semispinalis cervicis | T1-T6 transverse processes | C2-C5 spinous processes | Extends cervical spine |
| Semispinalis capitis | C7-T7 transverse processes | Occipital bone | Extends head |
The semispinalis cervicis is the PRIMARY muscle affected in INEM and is the most important for head extension.
Secondary Extensors:
| Muscle | Function |
|---|---|
| Splenius capitis | Extends and rotates head |
| Splenius cervicis | Extends and rotates cervical spine |
| Longissimus capitis | Extends head, lateral flexion |
| Trapezius (upper) | Extends head, elevates scapula |
| Levator scapulae | Assists extension when scapula fixed |
Muscle Layers
Superficial Layer:
- Trapezius
- Splenius capitis and cervicis
Intermediate Layer:
- Erector spinae (longissimus, iliocostalis)
Deep Layer:
- Semispinalis cervicis and capitis
- Multifidus
- Rotatores
Innervation
Posterior Rami of Cervical Nerves:
- Suboccipital nerve (C1) - suboccipital muscles
- Greater occipital nerve (C2) - semispinalis capitis
- Posterior rami C2-C7 - deep extensors
Biomechanics
Head Weight: The head weighs approximately 4-5 kg. The neck extensors must generate sufficient force to counteract this weight and maintain horizontal gaze. In DHS, extensor weakness shifts the center of gravity forward, creating a progressive kyphotic moment.
Compensatory Mechanisms:
- Use of hand to support chin (pathognomonic)
- Hyperextension of lumbar spine
- Shoulder elevation to provide passive support
Pathophysiology
Mechanisms of Muscle Weakness
INEM (Primary/Idiopathic):
The pathophysiology of isolated neck extensor myopathy involves:
- Selective muscle involvement - Semispinalis cervicis is preferentially affected
- Non-inflammatory myopathy - No immune infiltrate on biopsy
- Fiber size variation - Type 2 fiber atrophy predominates
- Fat replacement - Progressive fatty infiltration visible on MRI
Proposed Mechanisms:
| Mechanism | Evidence |
|---|---|
| Postural overload | Prolonged forward head posture (computer use) |
| Vascular compromise | Watershed zone between vertebral and occipital arteries |
| Mitochondrial dysfunction | Ragged red fibers on biopsy in some cases |
| Age-related sarcopenia | Accelerated in neck extensors |
Neuromuscular Causes
Myasthenia Gravis:
- Antibodies against acetylcholine receptors
- Fatigability of neuromuscular junction
- Neck extensors may be selectively vulnerable
- Responds to cholinesterase inhibitors
Amyotrophic Lateral Sclerosis (ALS):
- Motor neuron degeneration
- Combined upper and lower motor neuron signs
- Neck weakness may be early presentation
- Progressive, no specific treatment
Inflammatory Myopathy:
- Immune-mediated muscle destruction
- Dermatomyositis, polymyositis, inclusion body myositis
- Elevated CK, responds to immunosuppression
- May overlap with INEM
Secondary/Mechanical Causes
Post-Surgical:
- Extensive cervical laminectomy
- Loss of posterior tension band
- Extensor muscle denervation
Radiation:
- Fibrosis of paraspinal muscles
- Usually delayed onset (months to years)
- May be progressive
Cascade of Deformity
- Initial weakness - Difficulty holding head up at end of day
- Compensatory postures - Hand support, chin on chest
- Fixed kyphosis - Soft tissue contracture develops
- Secondary myelopathy - Cord compression from kyphosis
- Functional decline - Dysphagia, respiratory compromise
Progression Pattern
DHS typically progresses from "flexible" to "fixed" deformity over 3-6 months. Early intervention during the flexible phase may prevent fixed deformity. Once fixed, anterior release may be required for surgical correction.
Classification
Etiological Classification
Isolated Neck Extensor Myopathy
Diagnostic Criteria (Katz et al. 1996):
- Weakness limited to neck extensors
- No evidence of systemic neuromuscular disease
- EMG shows myopathic changes in neck muscles only
- Muscle biopsy: non-inflammatory myopathy
- Normal serum CK
- Negative autoantibodies
Characteristics: Age over 65 typically, female predominance, gradual onset over weeks to months, may stabilize or slowly progress.
Prognosis: Generally better than secondary causes. Some spontaneous improvement reported. Conservative management effective in early/mild cases.
Flexibility Classification
| Type | Definition | Clinical Implication |
|---|---|---|
| Flexible | Passively correctable | May respond to conservative care |
| Partially Fixed | Some passive correction possible | Soft tissue release may help |
| Fixed | No passive correction | Anterior release required |
Clinical Presentation
History
Presenting Symptoms:
- Difficulty holding head up, especially end of day
- Need to use hand to support chin
- Impaired horizontal gaze
- Difficulty with eating and drinking
- Social embarrassment
- Progressive over weeks to months
Important History Points:
| Question | Significance |
|---|---|
| Timing of symptoms | Morning improvement suggests MG |
| Limb weakness | Suggests systemic myopathy |
| Double vision | Suggests MG |
| Swallowing difficulty | Common in DHS, also suggests MG |
| Previous surgery | Post-surgical DHS |
| Radiation history | Post-radiation myopathy |
| Medications | Statins, steroids |
Physical Examination
Inspection:
- Chin-on-chest deformity
- Use of hand to support chin (pathognomonic)
- Compensatory lumbar hyperlordosis
- Shoulder elevation
Passive Range of Motion:
- Assess flexibility of deformity
- Gently extend neck to assess passive correction
- Note any fixed contracture
Active Range of Motion:
- Ask patient to extend neck actively
- Prone head lift test (extend neck against gravity)
- Sustained gaze test (maintain horizontal gaze for 60 seconds)
Neurological Examination:
| Component | Assessment |
|---|---|
| Cranial nerves | Ptosis, diplopia, facial weakness (MG) |
| Tongue | Atrophy, fasciculations (ALS) |
| Upper limbs | Proximal weakness (myopathy), fasciculations (ALS) |
| Lower limbs | Weakness, hyperreflexia (ALS) |
| Myelopathy | Hyperreflexia, Hoffman sign, gait |
Specific Tests:
- Ice pack test (improvement in ptosis suggests MG)
- Fatigability test (repeated arm abduction)
Red Flags
Red Flags Requiring Urgent Investigation
Rapidly progressive weakness, limb involvement, respiratory difficulty, bulbar symptoms (dysarthria, aspiration), or hyperreflexia require urgent neurology referral to exclude ALS or MG crisis. These conditions require different management than INEM.
Investigations
Laboratory Investigations
First-Line:
| Test | Purpose |
|---|---|
| CK (creatine kinase) | Elevated in inflammatory myopathy |
| ESR, CRP | Inflammatory markers |
| TFTs | Hypothyroidism can cause myopathy |
| AChR antibodies | Myasthenia gravis |
| Anti-MuSK antibodies | Seronegative MG |
Second-Line:
| Test | Indication |
|---|---|
| ANA, anti-Jo1 | Inflammatory myopathy |
| Genetic testing | Suspected muscular dystrophy |
| Paraneoplastic panel | Suspected paraneoplastic syndrome |
Electrodiagnostic Studies
EMG (Electromyography):
| Finding | Interpretation |
|---|---|
| Myopathic potentials in neck | Small, short, polyphasic |
| Normal limb EMG | Supports INEM |
| Widespread abnormalities | Suggests systemic disease |
| Fibrillations | Denervation (ALS, radiculopathy) |
Nerve Conduction Studies:
- Normal in INEM
- Decremental response in MG
- Helpful to exclude neuropathy
Imaging
X-ray:
- Assess degree of kyphosis
- Measure chin-brow vertical angle (CBVA)
- Evaluate for fracture or spondylosis
MRI:
- T1-weighted: Fatty infiltration appears hyperintense
- T2-weighted: Edema in acute phase
- Key muscles: Semispinalis cervicis, capitis
- Assess for cord compression
- Evaluate cord signal (myelomalacia)
CT:
- Bone detail for surgical planning
- Fusion assessment if prior surgery
- Fracture detection
Muscle Biopsy
Indications:
- Diagnosis uncertain after non-invasive workup
- Suspected inflammatory myopathy
- Atypical presentation
INEM Biopsy Findings:
- Fiber size variation
- Type 2 fiber atrophy
- No inflammation
- No necrosis
- Possible fatty replacement
Technique:
- Open biopsy of paraspinal muscle
- Usually semispinalis cervicis
- Sufficient sample for histology and special stains
Management
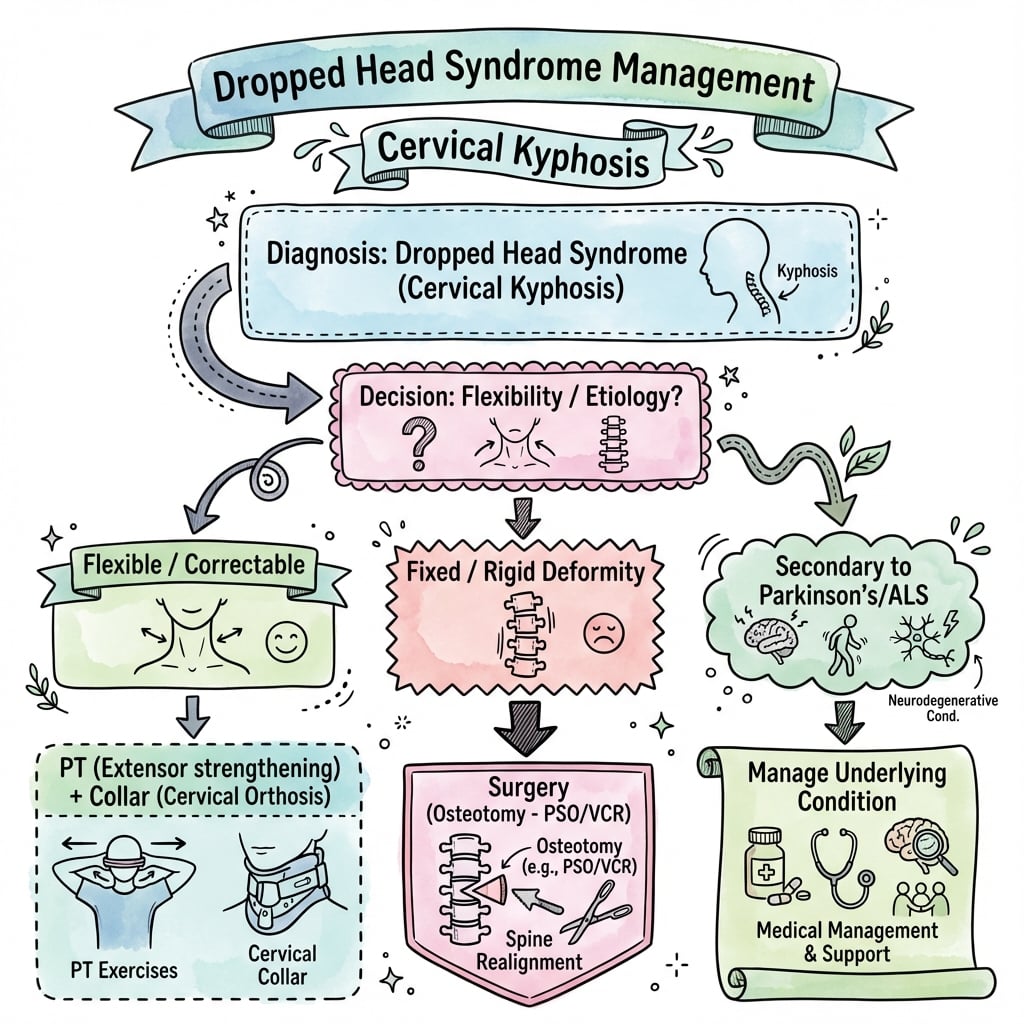
Treatment Algorithm
Initial Assessment:
- Complete history and examination
- Exclude systemic neuromuscular disease (MG, ALS)
- Imaging (X-ray, MRI)
- EMG and laboratory studies
Management by Phase:
Indications:
- Flexible deformity
- Early presentation (less than 3-6 months)
- Mild symptoms
- High surgical risk
Components:
Physical Therapy:
- Neck extensor strengthening exercises
- Postural retraining
- Stretching of anterior structures
- Aquatic therapy
Orthoses:
- Cervical collar (soft or rigid)
- Custom orthosis for chin support
- May not halt progression but provides comfort
Medications:
- Treat underlying condition (e.g., steroids for inflammatory myopathy)
- Pyridostigmine for MG
- No specific medication for INEM
Duration: Trial of 3-6 months of conservative management. If deformity progresses or becomes fixed, surgery is indicated.
Surgical Pearl
Posterior-only fusion has a high failure rate in DHS due to poor muscle quality and high mechanical demand. Extending fusion to T2-T4 and considering combined anterior-posterior surgery for fixed deformity improves outcomes. Always assess flexibility preoperatively.
Surgical Technique
Posterior Cervical Fusion for Dropped Head Syndrome
Surgical Goals
Primary Objectives:
- Restore horizontal gaze
- Stabilize cervical kyphotic deformity
- Decompress neural elements if myelopathy present
- Prevent progression of deformity
Patient Selection:
- Failed conservative management (3-6 months)
- Fixed or progressive deformity
- Functional goals: horizontal gaze, eating, ambulation
- Adequate bone quality for fixation
- Acceptable surgical risk profile
Preoperative Planning
Essential Workup:
- Full-length standing spine radiographs
- CT cervical spine (bone quality, anatomy)
- MRI if myelopathy suspected
- Neurological assessment
- Cardiopulmonary optimization
Positioning Considerations:
- Patient may not tolerate prone positioning initially
- May require staged correction
- Awake fiberoptic intubation often needed
- Careful head positioning to avoid further flexion
Surgical Approach
Positioning:
- Prone on Jackson table or Mayfield head holder
- Position head in as much correction as safely tolerated
- Neuromonitoring (SSEP, MEP) essential
- Fluoroscopy to confirm alignment
Exposure:
- Posterior midline approach
- Subperiosteal dissection to expose lateral masses
- Identify occiput if occipitocervical fusion planned
- Extend to upper thoracic if long construct needed
Fixation Options:
- Lateral mass screws (C3-C6)
- Pedicle screws (C2, C7, thoracic)
- Occipital plate if occipitocervical fusion
- Rods contoured to restore lordosis
Clinical Pearl
Exam Viva Point: "What are the key surgical considerations in dropped head syndrome?" Answer: Positioning is critical - patient may not tolerate prone initially. Require neuromonitoring. Long posterior fusion (often occiput to T2) to correct kyphosis. Staged correction if severe. High complication rates in elderly/comorbid patients.
Surgery aims to restore horizontal gaze and stabilize the cervical spine in corrected alignment.
Complications
Conservative Management Complications
Disease Progression:
- Fixed deformity development
- Secondary myelopathy
- Dysphagia and aspiration
- Skin breakdown under chin
Orthosis-Related:
- Skin pressure sores
- Discomfort and poor compliance
- May not prevent progression
Surgical Complications
Intraoperative:
| Complication | Prevention/Management |
|---|---|
| Cord injury | Careful positioning, neuromonitoring |
| Vascular injury (vertebral artery) | Anatomic knowledge, image guidance |
| Dural tear | Primary repair, dural sealant |
| Screw malposition | Image guidance, careful technique |
Early Postoperative:
| Complication | Management |
|---|---|
| Dysphagia | Speech therapy, swallow evaluation |
| Wound infection | Antibiotics, debridement if deep |
| Hardware prominence | Revision if symptomatic |
| Hematoma | Evacuation if neurological compromise |
Late Complications:
| Complication | Management |
|---|---|
| Pseudarthrosis | Revision fusion, extend levels |
| Adjacent segment disease | Monitor, extend fusion if symptomatic |
| Hardware failure | Revision, address pseudarthrosis |
| Junctional kyphosis | More common if stopped at C7, extend to thoracic |
| Persistent weakness | Expected due to underlying myopathy |
Specific Risks in DHS
Poor Bone Quality:
- Elderly population
- Consider cement augmentation
- Longer constructs for load sharing
Poor Muscle Quality:
- Reduces posterior tension band
- Higher construct demands
- May need anterior column support
High Complication Rates:
- Up to 30% complication rate in some series
- Related to patient age and comorbidities
- Careful patient selection important
Postoperative Care
Immediate Postoperative Care
Neurological Monitoring
Immediate Post-Op:
- Hourly neurological observations
- Upper and lower limb motor assessment
- Document any new deficits immediately
- Urgent imaging if deterioration
Warning Signs:
- New weakness or numbness
- Respiratory compromise
- Swallowing difficulty (airway edema)
- Wound hematoma
Immobilization
Cervical Collar:
- Rigid collar (Miami-J or Aspen type)
- Worn at all times except wound care
- Duration: 6-12 weeks until radiographic fusion
- May need custom collar if alignment specific
Positioning:
- Elevate head of bed 30 degrees
- Log-roll precautions
- Avoid excessive neck flexion or extension
- Soft collar for sleeping comfort (over rigid collar)
Early Postoperative Management
Wound Care:
- Check wound daily for hematoma, drainage
- Drain removal at 24-48 hours when output minimal
- Suture/staple removal at 2-3 weeks
Pain Management:
- Multimodal analgesia
- Avoid excessive opioids (respiratory depression)
- Muscle relaxants may help spasm
Mobilization:
- Sit upright day 1 if stable
- Walk with assistance day 1-2
- Physical therapy for gait and balance
- Avoid lifting greater than 2 kg for 6 weeks
Clinical Pearl
Exam Viva Point: "What is postoperative care after cervical fusion for dropped head syndrome?" Answer: Rigid cervical collar for 6-12 weeks. Close neurological monitoring. Early mobilization. Watch for wound hematoma and dysphagia. Serial radiographs to confirm fusion.
Close monitoring in the immediate postoperative period is essential given the high-risk nature of this surgery.
Outcomes
Clinical Outcomes
Outcome Measures
Expected Outcomes After Surgery
| Outcome Domain | Improvement Expected | Factors Affecting Outcome |
|---|---|---|
| Horizontal gaze restoration | 75-85% achieve improved forward gaze | Severity and flexibility of deformity preoperatively |
| Pain relief | Variable - 60-70% improvement | Underlying cause (INEM vs secondary DHS) |
| Dysphagia improvement | Often improves if due to chin-on-chest | May persist if unrelated cause |
| Function and ADLs | Improved eating, ambulation, social interaction | Patient goals and expectations |
| Quality of life | Significant improvement in most | Preoperative functional status |
What Surgery Achieves:
- Restores ability to look forward and see horizon
- Improves eating and swallowing (if due to chin-on-chest position)
- Enhances social interaction (eye contact)
- Reduces neck pain from chronic flexion
What Surgery Does NOT Achieve:
- Does not cure underlying neuromuscular disease
- Does not restore normal neck motion
- May not prevent progression of underlying condition
- Does not guarantee pain-free outcome
Clinical Pearl
Exam Viva Point: "What outcomes can a patient expect from surgery for dropped head syndrome?" Answer: 75-85% achieve improved horizontal gaze. Quality of life improves. However, neck motion is lost, pseudarthrosis occurs in 10-25%, and complications are common (20-40%). Surgery treats the deformity but not the underlying cause.
Patient expectations must be realistic - surgery improves alignment and function but does not cure the underlying condition.
Evidence Base
INEM Definition and Characterization (Landmark)
- Four patients with a non-progressive myopathy of severe neck extensor weakness
- Coined the term isolated neck extensor myopathy (INEM), preferred to dropped head syndrome
- INEM distinguished from more ominous neuromuscular disorders by electrophysiology, imaging and histology
- Muscle biopsy shows fibre-size variation without inflammation
DHS Case Series and Literature Review
- Seven patients with DHS presenting to a UK spinal unit (4 acute, 3 gradual onset)
- Six of seven were managed conservatively; one underwent surgery
- The single operated patient was dissatisfied with the surgical outcome
- Highlights that surgery must be considered cautiously, especially in elderly patients
DHS Etiology and Management Review
- DHS is most commonly associated with neuromuscular disorders; INEM is used when EMG/biopsy are unrevealing
- Most reports favour non-surgical interventions to stabilise the deformity initially
- Surgical outcomes in the literature are limited and mixed, ranging from poor to excellent
- Prevalence is expected to rise with increasing life expectancy
The Dropped Head Syndrome (Original Description)
- Four patients with relatively isolated neck extensor weakness
- EMG and muscle biopsy suggested a restrictive, non-inflammatory myopathy
- Cervical paraspinal muscles predominantly affected
- One of the earliest formal characterisations of the syndrome
Dropped Head Syndrome: A Systematic Review (Largest Pooled Cohort)
- 129 patients across 74 studies; mean age 63.6 years, 63% female
- Four diagnoses account for most cases: INEM 31.8%, Parkinson disease 20.2%, myasthenia gravis 12.4%, ALS 7.0%
- Overall positive response to treatment 64.3%; combined medical plus immunosuppression 87.5%
- Surgery successful in 93.8% when used after failed medical management
Cervical Spine Deformity Classification (Horizontal Gaze / CBVA)
- Expert Delphi-derived classification for cervical spine deformity with a deformity descriptor and five modifiers
- Chin-brow vertical angle (CBVA) formalised as the horizontal-gaze modifier, central to DHS planning
- Incorporates C2-7 SVA, T1 slope minus cervical lordosis, mJOA myelopathy and SRS-Schwab parameters
- Moderate inter- and intra-observer reliability across 20 deformity surgeons
DHS: Update on Etiology and Surgical Management
- DHS is a heterogeneous group with diverse etiologies producing a flexible anterior cervical curvature
- Causes include myasthenia gravis, ALS, Parkinson disease, radiotherapy, age-related change and idiopathic forms
- Non-operative care comprises orthotic bracing and physical therapy
- Surgical fusion carries a higher complication rate but most achieve favourable long-term outcomes
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Elderly Woman with Progressive Neck Weakness
"A 72-year-old woman presents with 3-month history of progressive difficulty holding her head up. She uses her hand to support her chin. No limb weakness, diplopia, or swallowing difficulty. No medication history. MRI shows fatty infiltration of the semispinalis cervicis."
Failed Conservative Management
"The same patient returns after 4 months of physical therapy and collar use. Her deformity is now partially fixed, with only 50% passive correction. She has difficulty eating and is socially isolated. MRI shows no cord compression."
DHS with Myelopathy
"A 68-year-old man with dropped head syndrome now develops progressive hand numbness and gait difficulty. Examination shows hyperreflexia, positive Hoffman sign, and difficulty with tandem gait. MRI shows severe cervical kyphosis with cord compression at C4-5."
Young Patient with Dropped Head
"A 45-year-old woman presents with 6-week history of dropped head syndrome. She also reports fatigue, double vision at the end of the day, and difficulty swallowing solids. Examination shows mild bilateral ptosis that worsens with sustained upgaze."
DROPPED HEAD SYNDROME
Clinical summary
Definition & Etiology
- •Severe weakness of neck extensors causing chin-on-chest deformity
- •INEM = Isolated Neck Extensor Myopathy (diagnosis of exclusion)
- •Must exclude: MG, ALS, inflammatory myopathy
- •Secondary causes: post-surgical, radiation, Parkinson
Clinical Features
- •Hand-to-chin support (pathognomonic)
- •Impaired horizontal gaze
- •Dysphagia common
- •Worse at end of day = think MG
- •Assess flexibility of deformity
Key Investigations
- •AChR antibodies - rule out MG
- •CK - elevated in inflammatory myopathy
- •EMG - myopathic in neck, normal limbs for INEM
- •MRI - fatty infiltration of semispinalis cervicis
- •X-ray - measure kyphosis
Management Principles
- •Conservative trial 3-6 months for flexible deformity
- •Physical therapy, collar, treat underlying cause
- •Surgery if failed conservative or fixed deformity
- •Posterior fusion for flexible, 360° for fixed
- •Extend to T2-T4 to prevent junctional kyphosis
Surgical Technique
- •C2 pars/pedicle screws superiorly
- •Lateral mass screws C3-C6
- •Pedicle screws upper thoracic
- •Anterior release if fixed
- •Consider cement augmentation
Exam Pearls
- •INEM = elderly, isolated to neck, non-inflammatory
- •MG = young/middle-age, fatigability, ptosis, diplopia
- •Semispinalis cervicis is KEY muscle affected
- •High complication rate (20-30%) - counsel appropriately
- •Posterior-only often insufficient - plan for combined
MCQ Practice Points
INEM Definition
Q: What is INEM and why is it a diagnosis of exclusion?
A: Isolated Neck Extensor Myopathy (INEM) is a non-inflammatory myopathy affecting only cervical extensors, predominantly in elderly patients. It is a diagnosis of exclusion because systemic causes (myasthenia gravis, ALS, inflammatory myopathy) must be ruled out first. EMG shows myopathic changes in neck extensors but normal limb muscles.
MRI Findings
Q: What is the characteristic MRI finding in dropped head syndrome due to INEM?
A: T1 hyperintensity (fatty infiltration) of the paraspinal muscles, especially semispinalis cervicis and capitis. This indicates chronic muscle degeneration with fat replacement. The splenius, multifidus, and deep extensors may also be involved.
Differential from MG
Q: What clinical features help differentiate myasthenia gravis from INEM as a cause of dropped head?
A: Myasthenia gravis:
- Fatigability (symptoms worsen with activity/end of day)
- Ptosis and diplopia (ocular involvement)
- Fluctuating weakness
- Positive AChR antibodies
INEM: Isolated to neck extensors, non-fatiguing, no ocular symptoms, negative antibodies.
Surgical Approach
Q: Why is a combined anterior-posterior approach often needed for surgical correction of dropped head syndrome?
A: Posterior-only fusion has high failure rates (up to 30-50%) due to poor extensor muscle quality and high mechanical demands. A 360-degree approach provides:
- Anterior release if fixed kyphosis
- Anterior structural support
- Posterior instrumented fusion for correction
- Better biomechanical stability
Guidelines, Registries & Global Practice
Global Epidemiology
Dropped head syndrome (DHS) is rare and predominantly affects older adults. The largest pooled cohort to date (systematic review of 129 patients across 74 studies) reports a mean age of 63.6 years and a 63% female predominance, with four diagnoses accounting for most cases.
| Parameter | Pooled estimate | Source |
|---|---|---|
| Mean age at presentation | 63.6 years | Drain 2019 (PMID 30844858) |
| Female proportion | ~63% | Drain 2019 (PMID 30844858) |
| INEM (idiopathic) | 31.8% of cases | Drain 2019 (PMID 30844858) |
| Parkinson disease | 20.2% of cases | Drain 2019 (PMID 30844858) |
| Myasthenia gravis | 12.4% of cases | Drain 2019 (PMID 30844858) |
| Amyotrophic lateral sclerosis | 7.0% of cases | Drain 2019 (PMID 30844858) |
Guidance Landscape (No Disease-Specific CPG)
There is no dedicated DHS clinical practice guideline from AAOS, NICE, BOA, AO Spine or EFORT. Practice is therefore derived from narrative reviews, consensus on cervical sagittal alignment and the underlying-disease guidelines that drive treatment.
| Body / Framework | Relevant guidance | Evidence basis |
|---|---|---|
| Ames/ISSG cervical deformity classification | CBVA (horizontal gaze), C2-7 SVA, TS-CL as planning/correction targets | Expert Delphi, moderate reliability (PMID 26273762) |
| AO Spine / deformity consensus | Restore horizontal gaze and sagittal balance; instrument to a stable caudal foundation (cervicothoracic junction) | Expert consensus / review (PMID 23203936) |
| Neuromuscular disease pathways (e.g. EFNS/AAN for MG, ALS) | Treat the causative neuromuscular disorder first; DHS often improves with disease control | Disease-specific guidelines |
| Pooled treatment evidence | Medical/immunomodulatory therapy first; surgery for non-responders | Systematic review, Level V (PMID 30844858) |
Registry Evidence
No national joint or spine registry captures DHS as a discrete diagnosis; arthroplasty registries (AOANJRR, NJR, AJRR) are not applicable to this cervical extensor disorder. The evidence base is limited to single-centre series, the pooled systematic review above and narrative updates (PMID 32105239), all Level IV-V. This evidentiary weakness should temper any strong treatment claims.
Practice Variation
- First-line emphasis varies by referral pathway: neurology-led services prioritise antibody/EMG-guided medical therapy, whereas spine-led referrals more readily consider deformity surgery.
- Surgical extent differs between centres, from subaxial constructs to occiput/C2-to-upper-thoracic fusions; extension across the cervicothoracic junction is increasingly favoured to limit junctional failure.
- Anterior release / circumferential surgery is reserved for fixed or biplanar deformity and is concentrated in high-volume deformity units (PMID 36106864).
Australian Context
Australian practice mirrors these international principles. Patients are typically referred to neurology for AChR/anti-MuSK antibody testing and electrodiagnostic studies (widely available through public and private pathology) to exclude myasthenia gravis, ALS and inflammatory myopathy before presumed INEM is treated. MRI of the cervical spine with attention to paraspinal muscle signal is standard. Complex deformity correction, including combined anterior-posterior surgery, is performed at major spinal units and discussed at multidisciplinary meetings with spine surgeons, neurologists and radiologists. Postoperative rehabilitation is coordinated through hospital and community physiotherapy, with speech pathology assessment for dysphagia.
References
- Katz JS, Wolfe GI, Burns DK, Bryan WW, Fleckenstein JL, Barohn RJ. Isolated neck extensor myopathy: a common cause of dropped head syndrome. Neurology. 1996;46(4):917-21. PMID 8780064. doi:10.1212/wnl.46.4.917
- Suarez GA, Kelly JJ Jr. The dropped head syndrome. Neurology. 1992;42(8):1625-7. PMID 1641161. doi:10.1212/wnl.42.8.1625
- Petheram TG, Hourigan PG, Emran IM, Weatherley CR. Dropped head syndrome: a case series and literature review. Spine (Phila Pa 1976). 2008;33(1):47-51. PMID 18165748. doi:10.1097/BRS.0b013e31815e38ec
- Sharan AD, Kaye D, Charles Malveaux WMS, Riew KD. Dropped head syndrome: etiology and management. J Am Acad Orthop Surg. 2012;20(12):766-74. PMID 23203936. doi:10.5435/JAAOS-20-12-766
- Drain JP, Virk SS, Jain N, Yu E. Dropped head syndrome: a systematic review. Clin Spine Surg. 2019;32(10):423-429. PMID 30844858. doi:10.1097/BSD.0000000000000811
- Brodell JD, Sulovari A, Bernstein DN, Mongiovi PC, Ciafaloni E, Rubery PT, Mesfin A. Dropped head syndrome: an update on etiology and surgical management. JBJS Rev. 2020;8(1):e0068. PMID 32105239. doi:10.2106/JBJS.RVW.19.00068
- Ames CP, Smith JS, Eastlack R, et al. Reliability assessment of a novel cervical spine deformity classification system. J Neurosurg Spine. 2015;23(6):673-83. PMID 26273762. doi:10.3171/2014.12.SPINE14780
- Li Y, Basil G, Vanni S. Dropped head syndrome in a patient with Parkinson's disease and inflammatory myopathy, treated with sternocleidomastoid release and circumferential cervical fusion. Br J Neurosurg. 2025;39(1):104-109. PMID 36106864. doi:10.1080/02688697.2022.2123892