Palmar Fibromatosis | Progressive Flexion Contracture
Tubiana Classification
Critical Must-Knows
- Myofibroblasts produce Type III collagen causing contracture
- Ring and little fingers most commonly affected (ulnar predominance)
- Spiral cord displaces NV bundle central and superficial - highest injury risk
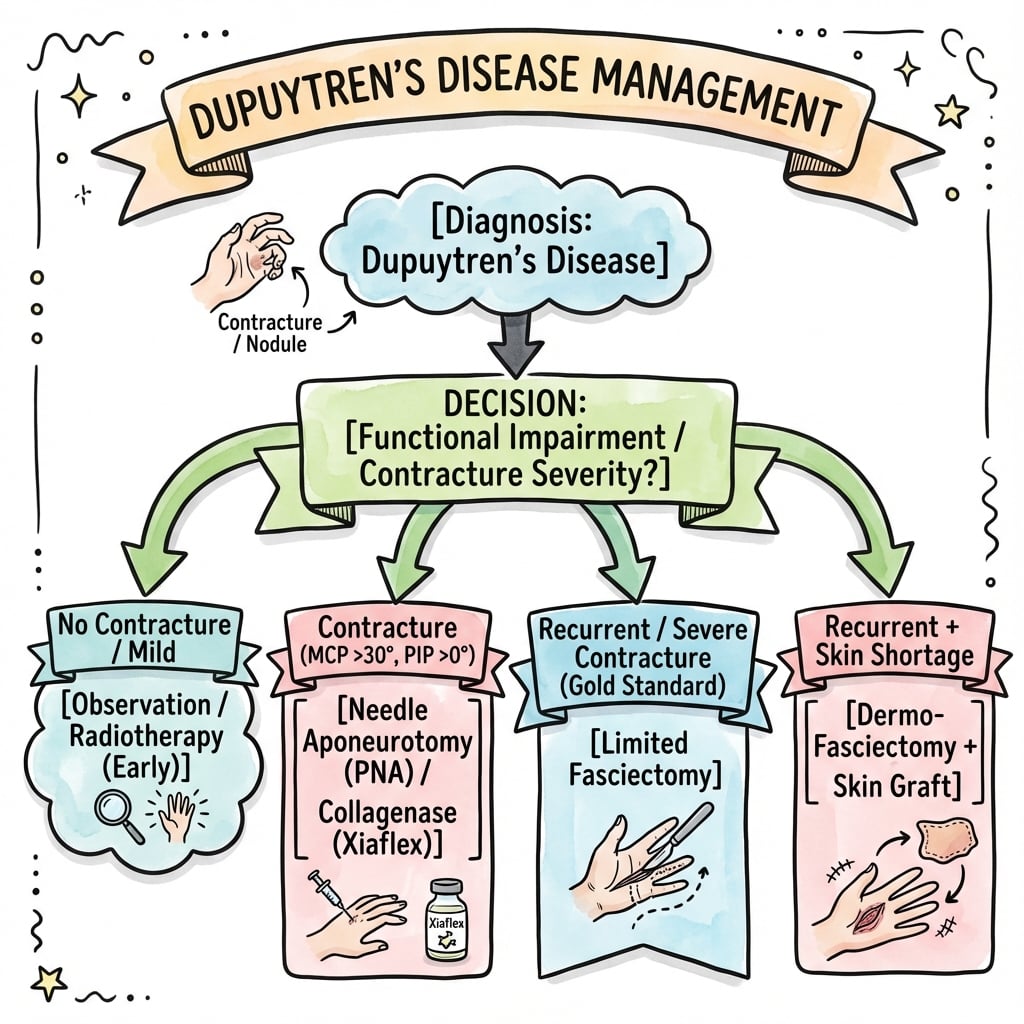
- Surgical indications: MCP greater than 30° or ANY PIP contracture
- Diathesis features: Young onset, bilateral, ectopic fibromatosis, family history
Clinical Pearls
- "Northern European/Celtic/Viking ancestry 15x risk
- "Diabetes: 20% prevalence (vs 4% general)
- "PIP contractures harder to correct - operate early
- "Recurrence vs extension: important distinction
Clinical Imaging
Imaging Gallery



Critical Dupuytren's Exam Points
Pathophysiology
Myofibroblast is the pathological cell - produces contractile force and Type III collagen. Three phases: Proliferative (nodules), Involutional (cord formation), Residual (mature contracture). TGF-beta pathway activation central to pathogenesis.
Spiral Cord Anatomy
Four components: Pretendinous band + Spiral band + Lateral digital sheet + Grayson ligament. Wraps around NV bundle displacing it central and superficial. Highest risk of iatrogenic nerve injury during dissection.
Surgical Indications
MCP contracture greater than 30 degrees OR ANY PIP contracture. Positive table-top test (Hueston). PIP contractures harder to correct - lower success than MCP. Operate earlier for PIP involvement.
Treatment Spectrum
Needle aponeurotomy: Percutaneous, fastest recovery, 60% recurrence at 5 years. Collagenase: Non-surgical enzyme injection. Limited fasciectomy: Gold standard surgery. Dermofasciectomy: With skin graft for aggressive recurrence or diathesis.
DASHEDDupuytren's Risk Factors
| D | Diabetes 20% prevalence in diabetics |
| A | Alcohol Hepatic fibrosis association |
| S | Smoking Microvascular changes |
| H | Hereditary/Northern European Viking disease - 15x increased risk |
| E | Epilepsy (phenytoin) Anti-epileptic medication effect |
| D | Disease (Peyronie, Ledderhose) Ectopic fibromatoses |
| D | Diabetes 20% prevalence in diabetics | S | Smoking Microvascular changes | E | Epilepsy (phenytoin) Anti-epileptic medication effect |
| A | Alcohol Hepatic fibrosis association | H | Hereditary/Northern European Viking disease - 15x increased risk | D | Disease (Peyronie, Ledderhose) Ectopic fibromatoses |
Hook:DASHED factors accelerate the disease! Northern European ancestry is the strongest predictor.
PSLGSpiral Cord Four Components
| P | Pretendinous band Longitudinal band in palm |
| S | Spiral band From natatory ligament around NV bundle |
| L | Lateral digital sheet Lateral to flexor sheath |
| G | Grayson ligament Volar to NV bundle |
| P | Pretendinous band Longitudinal band in palm | L | Lateral digital sheet Lateral to flexor sheath |
| S | Spiral band From natatory ligament around NV bundle | G | Grayson ligament Volar to NV bundle |
Hook:PSLG forms the Spiral cord - the most dangerous cord because it wraps around and displaces the neurovascular bundle!
YBEFDupuytren's Diathesis Features
| Y | Young onset Less than 40 years |
| B | Bilateral disease Both hands affected |
| E | Ectopic fibromatosis Peyronie, Ledderhose, Garrod pads |
| F | Family history Strong genetic component |
| Y | Young onset Less than 40 years | E | Ectopic fibromatosis Peyronie, Ledderhose, Garrod pads |
| B | Bilateral disease Both hands affected | F | Family history Strong genetic component |
Hook:YBEF predicts aggressive disease with higher recurrence - consider dermofasciectomy earlier!
NCFDTreatment Recurrence Rates - HIGH to LOW
| N | Needle fasciotomy 60-80% recurrence (highest) |
| C | Collagenase 35-65% recurrence |
| F | Fasciectomy 20-40% recurrence |
| D | Dermofasciectomy 10-20% recurrence (lowest) |
| N | Needle fasciotomy 60-80% recurrence (highest) | F | Fasciectomy 20-40% recurrence |
| C | Collagenase 35-65% recurrence | D | Dermofasciectomy 10-20% recurrence (lowest) |
Hook:NCFD: Needle worst, Dermo best for recurrence!
BRUNERSurgical Approach - BRUNER
| B | Bruner zigzag Incision design across creases |
| R | Respect NVB Identify before excision |
| U | Under loupe Magnification essential |
| N | No longitudinal Never cross crease with straight line |
| E | Excise diseased Remove pathological tissue only |
| R | Release contracture Achieve full extension if possible |
| B | Bruner zigzag Incision design across creases | U | Under loupe Magnification essential | E | Excise diseased Remove pathological tissue only |
| R | Respect NVB Identify before excision | N | No longitudinal Never cross crease with straight line | R | Release contracture Achieve full extension if possible |
Hook:BRUNER incision, Respect NVB, Under magnification, No straight lines, Excise disease, Release contracture
Overview and Epidemiology
The Viking Disease
Dupuytren's disease has the highest prevalence in populations of Northern European/Celtic/Viking descent. Prevalence reaches up to 30% in Norwegian men over 60 years, and pooled Western-population data show 12% at 55, 21% at 65 and 29% at 75 years. It is markedly rarer in African, East Asian and South Asian populations.
Definition
Dupuytren's disease is a benign fibroproliferative disorder affecting the palmar and digital fascia, resulting in progressive nodule and cord formation with flexion contracture of the digits. Named after Baron Guillaume Dupuytren who described surgical treatment in 1831.

Epidemiology
Population Prevalence:
- Western/European-ancestry pooled means: 12% (age 55), 21% (age 65), 29% (age 75)
- Northern European descent: up to 30% in men over 60
- Markedly lower in African, East Asian and South Asian populations
- Increases dramatically with age after 50 years
Demographics:
- Gender: Male to female ratio 7:1 in younger patients, equalizes after age 70
- Age: Peak presentation 50-60 years, can occur younger with diathesis
- Laterality: Right hand slightly more common, 40-60% bilateral
- Digit distribution: Ring greater than little greater than middle greater than index greater than thumb
Associated Risk Factors (DASHED):
- Diabetes mellitus: 20% prevalence (vs 4% general population)
- Alcohol consumption: Dose-dependent association, hepatic fibrosis link
- Smoking: 2-3x increased risk via microvascular effects
- Hereditary/Northern European: Strongest predictor, autosomal dominant pattern
- Epilepsy medications: Phenytoin, phenobarbital association
- Disease associations: Peyronie (penile), Ledderhose (plantar), Garrod pads (knuckles)
Dupuytren's Diathesis
Describes aggressive disease phenotype with poor prognosis:
- Young onset (less than 40 years)
- Bilateral hand involvement
- Ectopic fibromatoses (Peyronie, Ledderhose)
- Strong family history
- Radial side involvement (index, middle, thumb)
- Dorsal Garrod pads
Diathesis patients have higher recurrence rates (up to 70% at 5 years) and may benefit from more aggressive initial surgery (dermofasciectomy).
Pathophysiology
Cellular and Molecular Basis
The Myofibroblast is the central pathological cell in Dupuytren's disease:
- Modified fibroblast with smooth muscle-like contractile apparatus
- Contains alpha-smooth muscle actin (alpha-SMA) stress fibers
- Produces excessive Type III collagen (vs Type I in normal fascia)
- Generates contractile force via actin-myosin interaction
- Responds to TGF-beta and mechanical stress signals
Molecular Pathways:
- TGF-beta signaling: Central driver of myofibroblast differentiation
- Wnt pathway: Promotes fibroblast to myofibroblast transformation
- Mechanical stress: Tension induces myofibroblast activation
- Hypoxia: Local tissue hypoxia may trigger fibrogenesis
- Free radicals: Oxidative stress in pathological tissue
Three Phase Disease Progression
Phase 1 - Proliferative:
- Active myofibroblast proliferation
- High cellularity with immature fibroblasts
- Nodule formation in palm and digits
- Type III collagen predominates
- May be painful, progressive
Phase 2 - Involutional:
- Myofibroblast alignment along stress lines
- Cord formation from palmar nodules extending to digits
- Contracture begins and progresses
- Transition from Type III to Type I collagen
- Less cellular, more organized collagen
Phase 3 - Residual:
- Mature, relatively acellular cord
- Dense Type I collagen bundles
- Established fixed contracture
- Minimal active disease
- Low recurrence risk if excised
Normal Palmar Fascial Anatomy
Longitudinal Components:
- Pretendinous bands: Four bands from palmaris longus to digits (ring and little most prominent)
- Natatory ligament: Connects pretendinous bands distally
- Spiral band: From natatory to lateral digital sheet
Transverse Components:
- Transverse palmar ligament: At MCP level
- Natatory ligament: Distal palm between web spaces
Vertical Components:
- Septa of Legueu and Juvara: Anchor fascia to skeleton
- Eight vertical septa create palmar compartments
Digital Fascia:
- Lateral digital sheet: Lateral to flexor sheath
- Grayson ligament: Volar to neurovascular bundle
- Cleland ligament: Dorsal to neurovascular bundle (not involved in Dupuytren's)
Cord Anatomy and Types
Spiral Cord and Neurovascular Bundle
The spiral cord is the most dangerous anatomically because it displaces the neurovascular bundle central and superficial. During dissection, the NV bundle is at high risk of injury as it lies in an abnormal position. Always identify the NV bundle before dividing any cords.
Four Major Cord Types
1. Pretendinous Cord (Most Common)
- From pretendinous band in palm
- Extends from distal palmar crease to base of digit
- Causes MCP joint contracture
- Neurovascular bundle remains in normal position
- Relatively safe to excise
2. Central Cord
- Continuation of pretendinous cord into digit
- Lies central in digit over flexor sheath
- Causes PIP joint contracture
- Neurovascular bundle in normal position
- Common in ring and little fingers
3. Spiral Cord (Most Dangerous)
- Four components (PSLG):
- Pretendinous band (palm)
- Spiral band (from natatory ligament)
- Lateral digital sheet (lateral to flexor sheath)
- Grayson ligament (volar to NV bundle)
- Spirals around and displaces NV bundle centrally and superficially
- NV bundle can be displaced up to 1cm from normal position
- Highest risk of iatrogenic nerve injury
- Requires careful dissection under loupe magnification
4. Lateral Cord
- From lateral digital sheet alone
- Causes PIP joint contracture
- Less common than other types
- NV bundle usually in normal position
5. Other Rare Cords:
- Retrovascular cord: Dorsal to NV bundle (very rare)
- Natatory cord: In web space, causes web space contracture
- Thumb cords: First web pretendinous, proximal commissural

Cord Type Comparison
| Cord Type | Location | Contracture | NV Bundle | Risk Level |
|---|---|---|---|---|
| Pretendinous | Palm to finger base | MCP | Normal position | Low |
| Central | Digit over flexor sheath | PIP | Normal position | Low |
| Spiral | Wraps around NV bundle | MCP and PIP | Central and superficial | HIGH |
| Lateral | Lateral digital sheet | PIP | Usually normal | Moderate |
Classification Systems
Tubiana Classification (Most Used)
Based on total passive extension deficit (TPED) - sum of MCP, PIP, DIP contractures for each digit.
| Stage | Total Flexion | Description | Treatment |
|---|---|---|---|
| Stage 0 | 0° | Nodules only, no contracture | Observation |
| Stage I | 0-45° | Mild contracture | Consider treatment if progressive |
| Stage II | 45-90° | Moderate contracture | Surgery indicated |
| Stage III | 90-135° | Severe contracture | Surgery, may need skin graft |
| Stage IV | Greater than 135° | Very severe contracture | Surgery, often dermofasciectomy |
Utility: Prognostic - higher stages have worse outcomes and higher recurrence.
Stages III-IV have significantly worse correction rates especially for PIP joints.
Clinical Presentation and Assessment
History
Chief Complaint:
- Progressive inability to fully extend fingers
- Difficulty placing hand flat on surfaces
- Functional impairment: hand hygiene, glove wearing, placing hand in pocket
- Usually painless (pain suggests active proliferative phase)
Timeline:
- Insidious onset, progressive over months to years
- May notice palmar nodule before contracture develops
- Periods of rapid progression alternating with stability
Functional Impact:
- Difficulty with fine motor tasks
- Problems with gripping tools/objects
- Cosmetic concerns
- Interference with occupation
Risk Factor Assessment:
- Ancestry (Northern European/Celtic)
- Diabetes status and control
- Alcohol consumption history
- Epilepsy medication use
- Family history of Dupuytren's
- Bilateral hand involvement
- Ectopic fibromatoses (Peyronie, Ledderhose, Garrod pads)

Examination
Inspection:
- Palmar nodules: Firm, subcutaneous, adherent to skin
- Skin pitting: Overlying involved cords
- Cords: Palpable longitudinal bands from palm to digits
- Contracture: Flexion deformity at MCP and/or PIP joints
- Digit distribution: Record which rays involved
- Skin condition: Check for previous surgical scars, skin quality
Palpation:
- Identify nodules and cords
- Distinguish from flexor tendons (cords don't move with finger flexion)
- Check consistency (hard mature cord vs soft nodule)
- Skin adherence and pitting
Contracture Measurement:
- MCP contracture: Measure with goniometer, record separately
- PIP contracture: Measure separately (most important for prognosis)
- Total passive extension deficit (TPED): Sum of all joint contractures
- Active vs passive: Document both (rule out joint pathology)
Table-Top Test (Hueston Test):
- Patient attempts to place palm flat on table surface
- Positive: Cannot achieve flat palm-to-table contact
- Indicates functionally significant contracture
- Traditional threshold for surgical intervention
Neurovascular Assessment:
- Digital sensation (light touch, 2-point discrimination)
- Capillary refill and color
- Allen test if vascular concern
- Document baseline before any intervention
Bilateral Assessment:
- Always examine both hands
- 40-60% have bilateral involvement
- May be asymmetric in severity
Diathesis Features:
- Age at onset (less than 40 years concerning)
- Garrod pads (dorsal PIP knuckle pads)
- Ectopic disease: Peyronie (penile), Ledderhose (plantar)
- Family history
Differential Diagnosis
Differential Diagnosis of Palmar Nodule / Finger Contracture
| Condition | Key Distinguishing Feature | Cord/Contracture | Clue |
|---|---|---|---|
| Dupuytren's disease | Firm palmar cord/nodule, skin pitting | Yes — MCP/PIP flexion | Ulnar digits, NV bundle displaced by spiral cord |
| Stenosing tenosynovitis (trigger finger) | Triggering/locking with active flexion | No fixed contracture | Nodule moves WITH tendon on flexion |
| Camptodactyly | Congenital, painless PIP flexion | No palmar cord | Present from childhood, little finger |
| Epithelioid sarcoma | Persistent firm mass, may ulcerate | Mass not cord | Young adult, suspicious mass — biopsy if atypical |
| Inclusion cyst / foreign-body granuloma | Discrete mass, history of trauma | No cord | Localised, no fascial band |
| Intrinsic joint contracture / OA | Joint-line tenderness, radiographic changes | Fixed but no palmar cord | X-ray shows joint pathology |
The Key Bedside Discriminator
A Dupuytren's cord does NOT move when the finger flexes (it is fascial, not tendinous), whereas a trigger-finger nodule moves with the flexor tendon. Skin pitting/tethering over the cord is pathognomonic of Dupuytren's.
Investigations
Dupuytren's is a Clinical Diagnosis
No routine investigations required. Diagnosis is clinical based on characteristic palmar nodules and cords with flexion contracture. Imaging only if diagnostic uncertainty or planning complex revision surgery.
Blood Tests
Screening for Risk Factors:
- HbA1c or fasting glucose: Screen for diabetes if not known
- Liver function tests: If alcohol history suggests hepatic disease
- No specific blood test for Dupuytren's disease
Imaging
Radiographs (X-rays):
- Not routinely indicated for primary diagnosis
- Consider if joint pathology suspected (arthritis, previous fracture)
- Pre-operative in severe contractures to assess joint integrity
- Fixed PIP contracture: X-ray to check for secondary joint changes
Ultrasound:
- High-resolution ultrasound can demonstrate:
- Thickened palmar fascia
- Cord identification and extent
- Relationship to neurovascular structures
- Mainly research tool, not routine clinical practice
- May help distinguish Dupuytren's from other masses
MRI:
- Rarely indicated in primary disease
- Useful for complex cases or diagnostic uncertainty
- Can show:
- Full extent of fascial involvement
- Relationship to tendons, NV bundles, joints
- Secondary joint pathology
- T1: Low signal cords
- T2: Variable signal depending on cellularity/phase
Histopathology
Not required for diagnosis but if tissue obtained shows:
- Myofibroblasts with alpha-SMA immunostaining
- Type III collagen predominance (early)
- Transition to Type I collagen (late)
- Variable cellularity depending on phase
- No malignant features (benign process)
Pre-operative Assessment
Before Surgery:
- Document baseline contractures with goniometry
- Photograph hand
- Assess neurovascular status
- X-ray if severe PIP contracture or trauma history
- Optimize diabetes control if present
- Smoking cessation counseling
Management Algorithm
Conservative Management
Observation:
- Indications: Nodules without contracture, minimal contracture (less than 30° MCP, no PIP)
- Monitor progression every 6-12 months
- Patient education about disease natural history
- No proven method to prevent progression
Intralesional Corticosteroid Injection:
- May reduce nodule size in early disease
- Triamcinolone 10-40mg injected directly into nodule
- Evidence limited to case series
- Can cause fat pad atrophy and skin depigmentation
- Not effective for established cords
Radiotherapy:
- Low-dose radiation (superficial X-ray or electron beam)
- May slow progression in early nodular phase
- Evidence limited, not standard of care
- Used in parts of Europe (notably Germany); not widely adopted elsewhere
- Concerns about long-term radiation effects
Splinting:
- No role in preventing contracture progression
- May worsen disease via mechanical stress
- Post-operative extension splinting has role (see post-op care)
Non-Surgical Interventional Management
Collagenase Injection (Xiaflex)
Mechanism:
- Clostridium histolyticum collagenase
- Enzymatic breakdown of Type I and III collagen in cord
- Weakens cord allowing manipulation and rupture
Technique:
- Inject 0.58mg into palpable cord
- For MCP: Inject at distal palmar crease level
- For PIP: Inject at base/mid-proximal phalanx
- Patient returns next day (24-48 hours)
- Manipulation to rupture cord under local anesthetic
- Extension splinting for 4 months post-procedure
Indications:
- MCP contracture with palpable cord
- Single joint involvement preferred
- Patient preference for non-surgical option
- Comorbidity precluding surgery
Contraindications:
- Allergy to collagenase
- Anticoagulation (relative)
- Multiple joints in same finger (can treat sequentially)
Outcomes:
- Success rate: 60-70% achieve less than 5° contracture
- MCP joints: Better response than PIP
- Recurrence: Similar to needle aponeurotomy (approximately 50% at 5 years)
Complications:
- Skin tears (common, usually heal)
- Bruising, swelling, pain
- Lymphadenopathy
- Tendon rupture (rare but reported - flexor tendon)
- Allergic reaction
- CRPS (rare)
Global Availability:
- Region-dependent: FDA-approved in the US; withdrawn from UK/EU markets in 2020 for commercial reasons despite retained efficacy
- Where unavailable, needle fasciotomy fills the minimally invasive niche
- Cost remains a major access barrier in many health systems
This treatment option is appropriate for the non-surgical patient.
Surgical Management
Limited Fasciectomy (Gold Standard)
Definition: Excision of diseased fascia only, preserving normal fascia and all vital structures.
Indications:
- MCP contracture greater than 30 degrees
- Any PIP contracture
- Positive table-top test
- Failed conservative/needle/collagenase
- Primary surgical treatment
Pre-operative Planning:
- Document contractures, photos
- Discuss realistic expectations (PIP harder to correct)
- Counsel on risks: nerve injury, recurrence, stiffness, CRPS
- Optimize medical comorbidities
- Smoking cessation
Surgical Technique:
Anesthesia:
- General anesthetic or regional block (axillary)
- Local anesthetic with adrenaline (vasoconstriction)
- Tourniquet control
Incisions:
- Bruner zigzag: Alternating transverse and oblique limbs
- Midlateral: For isolated cords
- Avoid straight longitudinal (contracture risk)
- Extend into palm as needed
- Z-plasties to lengthen skin if deficient
Dissection:
- Elevate skin flaps carefully (fascia adherent to skin)
- Identify diseased fascia (white, firm cords and nodules)
- Identify neurovascular bundles (displaced by spiral cord)
- Trace NV bundles proximally and distally to define safe zones
- Use loupe magnification for digital dissection
- Excise diseased fascia by careful sharp dissection
- Trace cords to their insertion into flexor sheath, skeleton
- Excise completely but preserve normal structures
Critical Structures to Preserve:
- Digital nerves (displaced by spiral cord)
- Digital arteries
- Flexor tendons
- PIP joint capsule (avoid destabilizing)
- Normal fascial bands
Closure:
- Leave wounds open (healing by secondary intention) OR
- Z-plasty closure if adequate skin
- Skin graft if skin deficient (dermofasciectomy)
- Bulky dressing with splint in extension
Post-operative:
- Elevate hand
- Early finger mobilization (day 1-2)
- Extension splinting at night for 3-6 months
- Hand therapy essential
- Return to normal activity 6-12 weeks
Outcomes:
- MCP correction: 90-95% success, low recurrence
- PIP correction: 60-80% success, higher recurrence
- Recurrence: Approximately 30-50% at 5 years (varies by diathesis)
- Satisfaction: 80-90% despite recurrence risk
The standard surgical treatment balancing efficacy and morbidity.
Complications
Digital Nerve Injury
Most important complication to avoid. Spiral cord displaces nerve centrally and superficially. Always identify and protect neurovascular bundles throughout dissection. Use loupe magnification. If nerve injured, repair primarily or graft if gap.
Intra-operative Complications
Neurovascular Injury:
- Incidence: 1-5% (higher with spiral cord, revision surgery)
- Digital nerve: Most common, spiral cord anatomy
- Digital artery: Can occur, bleeding may be only sign
- Prevention: Identify NV bundles, loupe magnification, gentle dissection
- Management:
- Nerve: Primary repair with 8-0 or 9-0 nylon, nerve graft if gap
- Artery: Repair if possible, ligate if necessary (check perfusion)
Flexor Tendon Injury:
- Rare (less than 1%)
- Occurs during dissection of cords from flexor sheath
- Repair primarily if identified
Skin Flap Necrosis:
- Skin adherent to diseased fascia
- Thin flaps at risk
- Handle gently, preserve blood supply
Early Post-operative Complications (Less than 6 weeks)
Hematoma:
- Incidence: 2-5%
- Prevention: Meticulous hemostasis, tourniquet deflation before closure, pressure dressing
- Management: Small = observation, large = evacuation
Wound Healing Problems:
- Delayed healing: Common with open palm technique (healing by secondary intention)
- Wound breakdown: 5-10%, especially over PIP
- Infection: 1-2% (rare with proper technique)
- Management: Regular dressings, hand therapy, antibiotics if infected
Skin Graft Failure (Dermofasciectomy):
- Partial loss in 5-10%
- Complete loss rare (less than 2%)
- Prevention: Adequate hemostasis, secure bolster dressing, immobilization
- Management: Allow granulation, split skin graft if needed
Late Complications (Greater than 6 weeks)
Recurrence:
- Definition: Return of disease in previously treated area
- Incidence:
- Limited fasciectomy: 30-50% at 5 years
- Needle aponeurotomy: 50-60% at 5 years
- Dermofasciectomy: 10-20% at 5 years
- Risk factors: Diathesis features, young age, PIP involvement
- Management: Observation if mild, repeat intervention if symptomatic
Extension:
- Definition: New disease in previously unaffected area
- Different from true recurrence
- Represents disease progression
- Managed as primary disease
Stiffness and Loss of Motion:
- Some loss of flexion common post-operatively
- Active mobilization and hand therapy essential
- Pre-operative PIP contractures may not fully correct
- Realistic expectations important
Complex Regional Pain Syndrome (CRPS):
- Incidence: 5-10% (varies by definition)
- Risk factors: Extensive surgery, prolonged immobilization, nerve injury
- Prevention: Early mobilization, gentle surgery
- Management: Hand therapy, pain management, CRPS protocols
Sensory Changes:
- Numbness in distribution of affected nerves
- Usually improves over 6-12 months
- Permanent if nerve injured
Scar Contracture:
- Can occur with inadequate skin coverage
- Z-plasty technique reduces risk
- Skin graft for deficiency
- Hand therapy with scar massage
Chronic Pain:
- Neuropathic pain if nerve injured
- Scar tenderness common initially
- Usually resolves over time
Complication Rates by Procedure
| Complication | Needle Aponeurotomy | Collagenase | Limited Fasciectomy | Dermofasciectomy |
|---|---|---|---|---|
| Nerve injury | Less than 1% | Less than 1% | 1-5% | 2-6% |
| Recurrence (5yr) | 50-60% | 50% | 30-50% | 10-20% |
| Infection | Rare | Rare | 1-2% | 2-3% |
| CRPS | Rare | Rare | 5-10% | 5-10% |
Management of Recurrent Disease
Assessment:
- Distinguish recurrence (same area) from extension (new area)
- Assess severity, functional impact
- Review previous operative notes if available
- Consider diathesis features
Treatment Options:
- Observation: If minimal, asymptomatic
- Needle aponeurotomy: Can repeat, useful for recurrent MCP
- Repeat fasciectomy: Technically challenging, higher nerve injury risk
- Dermofasciectomy: Lower recurrence, consider in young patients
- Amputation: Salvage for repeatedly recurrent, non-functional digit
Post-operative Care and Rehabilitation
Immediate Post-operative (0-2 weeks)
Dressing:
- Bulky dressing with extension splint
- Elevate hand (reduce edema)
- Monitor neurovascular status
- Pain control (oral analgesia usually sufficient)
Wound Care:
- Dressing change at 2-3 days if excessive drainage
- Leave wounds open OR remove sutures at 2 weeks
- Open palm technique: regular dressings until healed (4-6 weeks)
Early Mobilization:
- Start day 1-2 post-operatively
- Active flexion exercises to prevent stiffness
- Gentle extension (don't force)
- Critical for outcome
Rehabilitation Phase (2-12 weeks)
Hand Therapy:
- Essential component of treatment
- Active range of motion exercises
- Scar massage (once wounds healed)
- Edema control (compression, elevation)
- Strengthening exercises (progressive)
Splinting:
- Extension splinting at night: 3-6 months
- Maintains correction while healing
- Evidence for reducing recurrence unclear but commonly practiced
- Custom thermoplastic splint
Return to Activities:
- Light activities: 2-4 weeks
- Heavy activities: 6-12 weeks
- Individualize based on occupation, healing
Long-term Follow-up
Monitoring:
- 6 weeks, 3 months, 6 months, 12 months post-op
- Assess range of motion, scar, function
- Monitor for recurrence (distinguish from extension)
- Patient education about recurrence risk
Outcomes:
- Full outcome assessment at 12 months
- MCP contractures: Excellent correction, low recurrence
- PIP contractures: More variable correction, higher recurrence
- Patient satisfaction generally high despite recurrence risk
Evidence Base
- Prospective double-blind placebo-controlled RCT, 308 patients, contractures of 20° or more
- Collagenase achieved reduction to 0-5° in 64.0% of cords vs 6.8% placebo (p less than 0.001)
- Range of motion improved 43.9° to 80.7° vs 45.3° to 49.5° with placebo
- 3 treatment-related serious events: 2 tendon ruptures, 1 CRPS; no nerve injuries
- 111 patients randomised to needle fasciotomy vs limited fasciectomy, minimum 30° deficit
- 5-year recurrence (defined as TPED increase greater than 30°): 84.9% needle vs 20.9% fasciectomy (p less than 0.001)
- Recurrence occurred sooner with needle fasciotomy; older age reduced recurrence
- Satisfaction high in both groups but greater after fasciectomy; 53% preferred needle if recurrence
- 5-year non-interventional follow-up of 644 collagenase-treated patients (1081 joints)
- Recurrence (20° or more worsening with palpable cord) in 47% of successfully treated joints
- MCP recurrence 39% vs PIP recurrence 66% at 5 years
- Only one mild treatment-related late adverse event; recurrence comparable to surgery
- Genome-wide association study, 2325 cases and 11,562 controls (Dutch/German/UK)
- Nine susceptibility loci identified at genome-wide significance
- Six of nine loci harbour Wnt-signalling genes (WNT4, SFRP4, WNT2, RSPO2, SULF1, WNT7B)
- Implicates aberrant Wnt signalling as central to the fibromatosis
- Systematic review and meta-analysis of 23 studies in Western populations
- Reported prevalence ranged widely from 0.6% to 31.6%
- Mean prevalence rises with age: 12% at 55, 21% at 65, 29% at 75 years
- Strong age and male-sex relationship across populations
- Delphi consensus of 24 hand surgeons from 17 countries
- Recurrence defined as PED greater than 20° in a treated joint with a palpable cord vs the time-0 result
- Nodules or cords without contracture do NOT constitute recurrence
- Recurrence should be reported per joint, not by Tubiana stage or per ray
- Seminal anatomical study of diseased digital fascia in Dupuytren's contracture
- Defined patterns of cord formation and the spiral cord
- Documented displacement of the neurovascular bundle by diseased fascia
- Foundation for modern safe surgical dissection
Controversies & Areas of Uncertainty
Recurrence definitions are not comparable
Historical recurrence figures (10% to 85%) largely reflect different definitions, not different biology. The Felici consensus (PED greater than 20° at a treated joint with palpable cord) is now standard but older literature must be read with caution.
Collagenase vs needle fasciotomy
Both are minimally invasive; head-to-head data are limited and short-term outcomes are broadly similar for MCP cords. With collagenase withdrawn from several markets, needle fasciotomy is the default minimally invasive option in many regions.
Dermofasciectomy as primary surgery
Skin grafting clearly lowers recurrence, but whether it should be used primarily in diathesis (vs reserved for recurrence) is debated — graft morbidity and longer recovery must be weighed against recurrence reduction.
Night splinting after surgery
Routine post-operative night extension splinting is widely practised but RCT evidence that it reduces recurrence or improves outcome is weak; it is often used selectively rather than for all patients.
Radiotherapy for early disease
Low-dose radiotherapy may slow early nodular disease in some series, but evidence is low quality and it is not standard of care outside a few European centres; long-term safety concerns persist.
PIP correction ceiling
Fixed PIP contractures frequently fail to fully correct regardless of technique because of secondary capsular and check-rein changes — managing patient expectations is as important as the operation chosen.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Primary Dupuytren's Contracture
"A 58-year-old man of Scottish ancestry presents with progressive ring finger contracture over 2 years. On examination, he has 40° MCP and 30° PIP contracture with palpable cords. Positive table-top test. How would you manage this patient?"
Scenario 2: Dupuytren's Diathesis
"A 35-year-old man presents with bilateral Dupuytren's affecting multiple digits. He has a strong family history and Peyronie's disease. What features make this case high-risk and how does this influence management?"
Scenario 3: Recurrent Dupuytren's
"A 62-year-old man had limited fasciectomy 3 years ago for ring finger Dupuytren's. He now has 35° recurrent MCP contracture in the same finger. Discuss management."
MCQ Practice Points
Pathological Cell
Q: What is the pathological cell in Dupuytren's disease and what does it produce? A: Myofibroblast - modified fibroblast with contractile apparatus containing alpha-smooth muscle actin. Produces excessive Type III collagen in early phases, transitioning to Type I in mature disease. Generates contractile force via actin-myosin interaction.
Surgical Indications
Q: What are the surgical indications for Dupuytren's disease? A: MCP contracture greater than 30 degrees OR ANY PIP contracture OR Positive table-top test. PIP contractures are harder to correct so intervene earlier. This is the most commonly tested point about Dupuytren's.
Spiral Cord Anatomy
Q: What makes the spiral cord dangerous and what are its four components? A: The spiral cord displaces the neurovascular bundle central and superficial creating high risk of iatrogenic nerve injury. Four components (PSLG): Pretendinous band, Spiral band, Lateral digital sheet, Grayson ligament. Always identify NV bundle before dividing cords.
Recurrence Rates
Q: What are the recurrence rates for different Dupuytren's treatments at 5 years? A: Needle aponeurotomy: 50-60%; Collagenase: approximately 50%; Limited fasciectomy: 30-50%; Dermofasciectomy: 10-20%. Lower recurrence comes at cost of greater surgical morbidity.
Diathesis Features
Q: What are the features of Dupuytren's diathesis and why do they matter? A: YBEF: Young onset (less than 40), Bilateral disease, Ectopic fibromatosis (Peyronie, Ledderhose, Garrod pads), Family history. These patients have recurrence rates up to 70% and may benefit from dermofasciectomy for lower recurrence.
Guidelines, Registries & Global Practice
Global Epidemiology
- Western/European-ancestry meta-analysis: mean prevalence 12% at age 55, 21% at 65, 29% at 75 (Lanting 2014)
- Highest rates in Scandinavian/Celtic populations; Norwegian men over 60 up to 30%
- Markedly lower in African, East Asian and South Asian populations
- Male predominance (up to 7:1 in younger cohorts), narrowing with age
Side-by-Side Guidance
| Body / Source | Position on intervention | Notes |
|---|---|---|
| AAOS (US) — CCH labelling/AUC | Collagenase and surgery both endorsed for palpable cords | FDA-approved CCH (2010); MCP responds better than PIP |
| BSSH / BAPRAS (UK) | Fasciectomy, needle fasciotomy and CCH all options; therapy-led service | UK NICE previously appraised CCH; NHS access has varied over time |
| EFORT / European hand societies | Stepwise approach by cord type, joint and recurrence risk | Strong emphasis on PIP being harder to correct |
| International consensus (Felici) | Recurrence = PED greater than 20° at a treated joint with palpable cord | Standardises outcome reporting worldwide |
Note: collagenase clostridium histolyticum (Xiapex/Xiaflex) was withdrawn from several markets including the UK and EU in 2020 for commercial reasons, despite retained efficacy — availability is now region-dependent.
Registry and Outcome Notes
- No dedicated international Dupuytren implant registry exists (no implant involved)
- Best comparative long-term data come from RCTs (van Rijssen) and pharmacovigilance cohorts (CORDLESS)
- National hand-surgery audits increasingly track recurrence using the Felici per-joint definition
High- vs Limited-Resource Practice
- Well-resourced settings: full menu — needle fasciotomy, collagenase (where available), limited fasciectomy, dermofasciectomy, hand-therapy-led rehabilitation
- Limited-resource settings: open fasciectomy under regional/local anaesthesia is the mainstay; collagenase often unavailable due to cost; emphasis on single definitive procedure
- Constitutional, not occupational: generally regarded as a heritable/constitutional disease; heavy manual vibration exposure is at most a weak contributory factor
DUPUYTREN'S DISEASE
Clinical summary
Pathophysiology Essentials
- •Myofibroblast = pathological cell (alpha-SMA positive)
- •Type III collagen predominates (early), transitions to Type I (late)
- •3 phases: Proliferative → Involutional → Residual
- •TGF-beta pathway central to pathogenesis
- •Ring and little fingers most affected (ulnar predominance)
Spiral Cord Anatomy (PSLG)
- •P = Pretendinous band (palm)
- •S = Spiral band (from natatory ligament)
- •L = Lateral digital sheet
- •G = Grayson ligament (volar to NV bundle)
- •Displaces NV bundle CENTRAL and SUPERFICIAL
- •Highest risk of iatrogenic nerve injury
Surgical Indications (30-ANY)
- •MCP contracture greater than 30 degrees
- •ANY PIP contracture (harder to correct, operate earlier)
- •Positive table-top test (Hueston)
- •Progressive disease with functional limitation
Treatment Options and Recurrence
- •Needle aponeurotomy: 50-60% recurrence at 5y
- •Collagenase injection: ~50% recurrence at 5y
- •Limited fasciectomy: 30-50% recurrence at 5y (gold standard)
- •Dermofasciectomy + skin graft: 10-20% recurrence at 5y
Diathesis Features (YBEF)
- •Y = Young onset (less than 40 years)
- •B = Bilateral hand involvement
- •E = Ectopic fibromatosis (Peyronie, Ledderhose, Garrod)
- •F = Family history (autosomal dominant pattern)
- •Predicts 70% recurrence - consider dermofasciectomy
Risk Factors (DASHED)
- •D = Diabetes (20% prevalence)
- •A = Alcohol (dose-dependent)
- •S = Smoking (2-3x risk)
- •H = Hereditary/Northern European (15x risk)
- •E = Epilepsy medications (phenytoin)
- •D = Disease associations (Peyronie, Ledderhose)
Key Complications to Know
- •Digital nerve injury: 1-5% (higher with spiral cord)
- •Recurrence: Most common long-term issue
- •CRPS: 5-10% (early mobilization reduces risk)
- •PIP contractures: Harder to correct than MCP
- •Distinguish recurrence (same area) from extension (new area)
Post-operative Essentials
- •Early mobilization from day 1-2 (critical)
- •Night extension splinting for 3-6 months
- •Hand therapy mandatory for optimal outcome
- •MCP correction: 90-95% success
- •PIP correction: 60-80% success (more variable)