Caisson Disease | Nitrogen Bubble Bone Death | Divers and Compressed-Air Workers
- Cause is decompression - inert gas (nitrogen) bubbles form in fatty marrow during ascent and reduce blood flow, causing sterile bone death
- Two target groups - divers (especially indigenous/artisanal and technical divers) and compressed-air (caisson/tunnel) workers
- Humeral and femoral heads are the sites that matter - juxta-articular lesions cause pain and collapse
- Often silent for years - many lesions are found on screening or only declare once the joint surface collapses
- Prevention beats treatment - safe decompression schedules and medical surveillance dramatically lower risk
- “Dysbaric osteonecrosis is a form of avascular necrosis where the insult is decompression, not steroids, alcohol, or trauma
- “Shaft (diaphyseal) infarcts are usually harmless; juxta-articular head lesions are the ones that disable the patient
- “MRI is the most sensitive test and can detect pre-radiographic disease
- “Strict, well-monitored diving (e.g. many military programmes) shows very low rates - this is a largely preventable occupational disease
Dysbaric osteonecrosis (DON) is osteonecrosis caused by decompression. The final common pathway is identical to any avascular necrosis - ischaemia, osteocyte death, attempted repair, and (at the joint surface) collapse - but the trigger is inert gas bubbles forming in bone after a rapid reduction in ambient pressure. Always frame it as a named cause within the broader osteonecrosis differential.
Divers and compressed-air (caisson/tunnel) workers. The historical name "caisson disease" comes from the pressurised caissons used to build bridge foundations. Modern cases cluster in indigenous and artisanal diving fishermen who dive deep and often without safe decompression, and increasingly in deep technical recreational divers.
Juxta-articular head lesions matter; shaft lesions usually do not. Lesions of the humeral or femoral head can progress to subchondral collapse and disabling arthritis. Diaphyseal (shaft) bone infarcts are usually an incidental, asymptomatic finding.
DON is often asymptomatic until late and is commonly bilateral and multifocal because the whole skeleton was exposed to the same decompression stress. Always image both shoulders and both hips when DON is suspected.
- Dysbaric Osteonecrosis
- Decompression (nitrogen bubbles in marrow)
- Steroid/Alcohol Osteonecrosis
- Marrow fat hypertrophy and fat emboli
- Post-traumatic Osteonecrosis
- Direct disruption of blood supply
- Dysbaric Osteonecrosis
- Humeral head, femoral head, long-bone shafts
- Steroid/Alcohol Osteonecrosis
- Femoral head (often bilateral)
- Post-traumatic Osteonecrosis
- Femoral head, scaphoid, talus
- Dysbaric Osteonecrosis
- Divers and compressed-air workers
- Steroid/Alcohol Osteonecrosis
- Patients on steroids or heavy alcohol use
- Post-traumatic Osteonecrosis
- Patients after fracture or dislocation
- Dysbaric Osteonecrosis
- Common and usually harmless
- Steroid/Alcohol Osteonecrosis
- Can occur
- Post-traumatic Osteonecrosis
- Uncommon
- Dysbaric Osteonecrosis
- Safe decompression and surveillance - largely preventable
- Steroid/Alcohol Osteonecrosis
- Minimise steroid/alcohol exposure
- Post-traumatic Osteonecrosis
- Anatomic reduction, urgent dislocation reduction
FATTYWhy Bone Is Vulnerable to Inert Gas
Hook:FATTY marrow is a nitrogen sponge in a rigid box with a poor blood supply - the perfect setup for bubble-driven necrosis.
Overview and Epidemiology
Dysbaric osteonecrosis is a favourite basic-science and viva linking topic. It lets an examiner test decompression physiology (Henry's law, inert gas solubility), bone blood supply, the general principles of osteonecrosis, occupational medicine, and imaging - all from one diagnosis. The key narrative is simple: a rapid drop in ambient pressure lets nitrogen come out of solution as bubbles in fatty marrow; these bubbles cut off blood flow; bone dies; and at the joint surface the dead bone eventually collapses. According to PubMed, the disease remains a recognised occupational hazard for divers and compressed-air workers despite falling rates where safe decompression and surveillance are practised DOI.
Compressed-air workers: caisson and tunnel workers historically gave the disease its name ("caisson disease")
Commercial and military divers: risk is low where strict decompression and medical surveillance are enforced
Indigenous and artisanal diving fishermen: among the highest reported rates worldwide, reflecting deep, repetitive, poorly decompressed diving
Technical (deep mixed-gas) recreational divers: an emerging at-risk group as deep diving becomes more popular
Wide reported range: prevalence in professional divers has been reported anywhere from 0% to roughly 70%, depending heavily on the population and how strict their decompression practice is DOI
Highest-risk cohorts: in unsupervised artisanal diving fishermen, radiographic dysbaric osteonecrosis has been found in around three-quarters of those examined DOI
Well-monitored groups: experienced military divers following strict rules can show no excess of bone lesions compared with non-divers DOI
The striking spread of reported prevalence - from essentially zero in disciplined, surveilled diving programmes to very high rates in unregulated artisanal diving - is itself the exam message. Dysbaric osteonecrosis is driven by exposure and decompression practice, so safe dive profiles, decompression stops, depth and bottom-time limits, and periodic medical screening are the most effective interventions. Treatment of established juxta-articular collapse is far less satisfactory than prevention.
Mechanism and Pathophysiology: From Bubbles to Bone Death
At depth the body dissolves extra nitrogen into tissues; if ascent is too rapid, that nitrogen comes out of solution as bubbles, and bubbles forming in fatty bone marrow obstruct blood flow and raise intramedullary pressure, causing ischaemic (avascular) death of bone. This is why dysbaric osteonecrosis is a true osteonecrosis whose specific trigger is decompression rather than steroids, alcohol, or trauma.
Step-by-Step Mechanism

How Decompression Leads to Osteonecrosis
Under increased ambient pressure, more inert gas (usually nitrogen) dissolves into the body's tissues in proportion to the partial pressure (Henry's law). Fatty bone marrow takes up a disproportionate amount because nitrogen is far more soluble in fat than in water. The deeper and longer the dive, the greater the gas load.
As the diver or worker returns toward surface pressure, dissolved gas must be carried back to the lungs and exhaled. If ascent is faster than the tissues can offload gas, tissues become supersaturated and gas comes out of solution as bubbles - the same process that causes decompression sickness.
Bubbles nucleate within the fat-rich, poorly expansile marrow of long bones. Because bone is a rigid, closed compartment, even small volumes of gas can raise intramedullary pressure and compress the thin-walled sinusoidal vessels, while intravascular bubbles can directly obstruct flow.
Reduced perfusion starves osteocytes and marrow cells of oxygen. Osteocyte death produces the empty lacunae seen histologically - a sterile (non-infective) process. Subchondral bone, with its limited collateral supply, is especially vulnerable.
Surviving bone at the margin attempts revascularisation and lays down new bone on dead trabeculae, producing the sclerotic rim seen radiologically. This reparative process transiently weakens the necrotic segment.
For juxta-articular lesions, the weakened subchondral bone can fracture and collapse, giving a crescent sign and loss of the spherical joint surface, followed by secondary osteoarthritis. Shaft lesions, lacking an articular surface to fail, usually remain asymptomatic infarcts.
The single most testable physiological point is inert gas solubility in fat. Nitrogen is several times more soluble in lipid than in aqueous tissue, so the fatty marrow of the proximal humerus and femur loads heavily with nitrogen at depth and is then the place where bubbles preferentially form on ascent. Combine that with bone being a rigid compartment (so gas raises pressure rather than expanding) and a relatively end-arterial subchondral blood supply, and you have the precise anatomical and physiological recipe for dysbaric osteonecrosis DOI.
Lesion Distribution and Classification
Site-Based Description (the practical classification)
Dysbaric osteonecrosis lesions are traditionally described by where they lie in the long bone, because site predicts whether the lesion will cause symptoms.
- Location
- Subchondral bone of humeral head and femoral head
- Typical behaviour
- Can collapse, causing pain and secondary arthritis
- Clinical importance
- High - these are the disabling lesions
- Location
- Diaphysis and metaphysis of humerus, femur, tibia
- Typical behaviour
- Usually a stable, asymptomatic bone infarct
- Clinical importance
- Low - often an incidental finding
According to PubMed, lesions predominate in the proximal humerus and proximal femur, and in the majority of cases they progress despite the absence of further dysbaric exposure DOI - that is, stopping diving does not reliably reverse an established juxta-articular lesion.
BUBBLEPathophysiology Sequence
Hook:The whole disease is a BUBBLE problem: gas in, ascend too fast, gas out, bone dies.
Clinical Relevance, Presentation and Investigations
Occupational history is the key - depth, dive frequency, bottom times, decompression practice, years diving, and any past decompression sickness
Often asymptomatic - many shaft lesions and even some early head lesions cause no symptoms and are found on screening
Symptomatic head lesions present with deep shoulder or groin/hip pain, worse on loading, with progressive stiffness as the joint surface fails
Past decompression sickness, especially musculoskeletal "limb bends", should prompt suspicion of later bone lesions
Examine both shoulders and both hips - DON is frequently bilateral and multifocal
Shoulder: painful, restricted rotation; later, crepitus and fixed loss of movement with collapse
Hip: painful, restricted internal rotation; antalgic gait once the head collapses
Exclude other causes of osteonecrosis (steroids, alcohol, sickle cell, prior trauma) - DON is a diagnosis made in the right exposure context
Imaging
Imaging Approach to Suspected Dysbaric Osteonecrosis
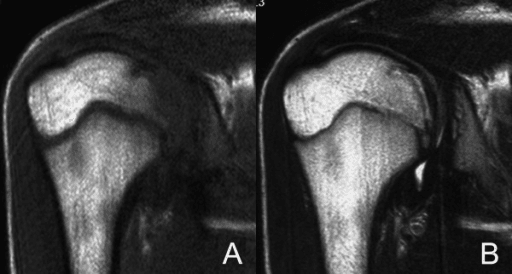
MRI detects pre-radiographic disease and is the most sensitive test for marrow change and early necrosis. It shows the geographic necrotic segment and the low-signal reactive interface ("band") and can survey several joints. Because it has no ionising radiation, it is also used for surveillance where indicated. A controlled study using MRI found that in well-disciplined military divers the prevalence of osteonecrosis was no higher than in matched non-divers, underlining that exposure practice, not diving per se, drives risk DOI.
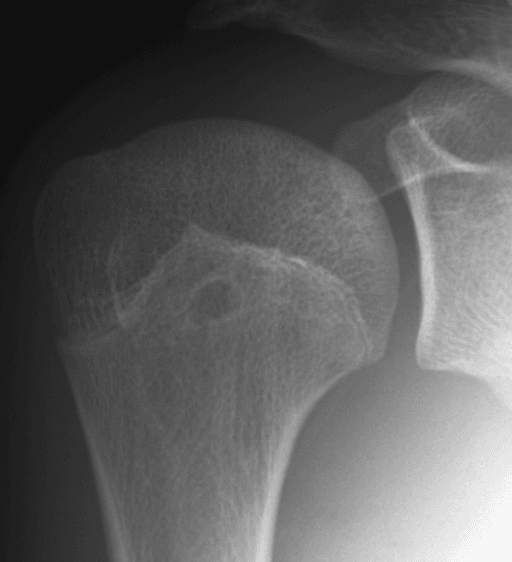
Radiographs of both shoulders, both hips, and the knees are the traditional screening and staging tool. They show sclerosis, cysts, bone islands, shaft infarct calcification, the crescent sign, and head flattening. Large historical occupational surveys used skeletal radiography to map lesion prevalence and distribution.
CT can clarify the extent of a lesion and detect a subchondral fracture (crescent) better than plain films, and is useful for surgical planning. Axial CT through the proximal humerus can show the mottled lucency, sclerosis, and crescentic subchondral lucency of an established head lesion.
Investigations to exclude alternative causes of osteonecrosis (for example, haemoglobinopathy screen if relevant) and to characterise the joint before any surgery. Remember that dysbaric and non-dysbaric osteonecrosis can coexist.

Management Principles
Prevention Is the Real Treatment
- Safe decompression schedules with appropriate ascent rates and decompression stops
- Depth and bottom-time discipline, avoiding provocative repetitive deep profiles
- Medical surveillance of at-risk workers and divers, with education for high-risk artisanal communities
- Prompt, correct treatment of decompression sickness (recompression and hyperbaric oxygen)
- Fitness-to-dive review - established juxta-articular DON may render a person unfit to continue diving
The contrast between strictly regulated diving (very low rates) and unsupervised artisanal diving (very high rates) is the strongest evidence that DON is preventable DOI DOI.
For juxta-articular dysbaric osteonecrosis, treat the joint as you would any osteonecrotic head - joint preservation before collapse, arthroplasty after. But the genuinely high-yield answer in a viva is to emphasise that prevention through safe decompression and surveillance is the only intervention that reliably changes the disease, because established head lesions tend to progress even after dysbaric exposure stops.
Classifying and Grading the Lesions: the Juxta-articular 'A' vs Head-Neck-Shaft 'B' Scheme
The One-Pager and the site-based table label lesions Type A and Type B, and the artisanal-fishermen study counts joints as affected at Grade II or higher - but neither the classification nor the grading has been defined so far. In diving and occupational medicine, dysbaric osteonecrosis lesions are grouped by site into two families, and severity within a joint is then graded radiographically. The characteristic radiographic vocabulary is common to both groups: decalcification, cystic lesions, osteosclerotic patterns, non-traumatic fractures, bone islands and a subchondral crescent sign DOI.
Subchondral bone of the humeral and femoral heads. Radiographically they run from dense (sclerotic) areas, segmental or linear opacities, and cystic lucencies with an intact articular cortex, through to structural failure - a subchondral translucent band (the crescent), sequestration, flattening and secondary osteoarthritis. Only these lesions threaten the joint surface, so they are the ones that cause pain, collapse and arthritis.
Medullary infarcts of the metaphysis and diaphysis of the humerus, femur and tibia, seen as dense areas, irregular serpentine ('smoke up a chimney') calcification, and translucent areas or cysts. Because they lie away from any articular surface, they are usually stable, asymptomatic infarcts found incidentally - important mainly as markers of exposure and for the rare late risk covered in the next section.
The artisanal-fishermen survey counted a joint as diseased only at Grade II or higher and still found dysbaric osteonecrosis in 76.9% of divers DOI. The catch for exams is that plain-film grading is blind to pre-radiographic disease, so radiograph-based figures under-report the true burden, whereas MRI detects marrow change before any film abnormality and is far more sensitive. That single methodological point explains much of the notorious 0-70% prevalence range: MRI surveys of disciplined military divers find no excess over non-divers, while radiograph surveys of unregulated deep divers approach three-quarters affected DOI.
Malignant Transformation of a Bone Infarct: the Rare but Lethal Late Risk
Twice above, the advice for an asymptomatic diaphyseal infarct is to observe and to "counsel about the very rare risk of malignant change." That warning deserves substance, because it converts an otherwise benign finding into a diagnosis you must not miss. A long-standing medullary bone infarct - including the shaft infarcts of dysbaric osteonecrosis - can, rarely, give rise to a sarcoma.
In a classic review of 16 infarct-associated sarcomas, the tumour was usually a fibrosarcoma or malignant fibrous histiocytoma (now termed undifferentiated pleomorphic sarcoma); patients were typically older men, lesions arose most often in the tibia and femur, and - directly relevant here - four of the sixteen patients had caisson disease. The risk appeared greatest in infarcts with a large medullary component, and the outcome was frequently rapidly fatal DOI.
Suspect malignant change when a previously stable, quiescent infarct becomes painful, or when imaging shows a new destructive lytic area, cortical destruction or a soft-tissue mass. That patient needs MRI, biopsy and staging - not reassurance. Dysbarism is among the recognised causes of the bone infarcts in which this transformation has been documented DOI.
The shaft infarct is not entirely benign: new or increasing pain, or a destructive lesion, in a long-standing bone infarct is malignant transformation until proven otherwise. According to PubMed, sarcoma arising in a bone infarct is rare, is usually a malignant fibrous histiocytoma or fibrosarcoma, has been documented specifically in caisson-disease (dysbaric) infarcts, and carries a poor prognosis DOI DOI.
DIVERSRisk Factors for Dysbaric Osteonecrosis
Hook:DIVERS who go too deep, too often, and ascend too fast grow bone infarcts.
Guidelines, Registries & Global Practice
Worldwide Burden and Demographics
Historical caisson work: bridge and tunnel construction in compressed air gave "caisson disease" its name and the first large case series
Highest modern rates: indigenous and artisanal diving fishermen (for example in parts of Mexico and South-East Asia), where surface-supplied deep diving is common and decompression is often unsafe DOI
Lowest rates: disciplined military and commercial diving programmes with enforced decompression and surveillance DOI
Emerging group: deep technical recreational divers DOI
Exposure dose: number of joints affected correlates with lifetime maximum depth and average bottom time DOI
Decompression practice: inadequate or absent decompression is the dominant modifiable driver
Prior decompression sickness: associated with later bone lesions
Age and career length: longer exposure histories carry more lesions DOI
MCQ Practice Points
Q: Why does fatty bone marrow play a central role in dysbaric osteonecrosis? A: Because nitrogen is far more soluble in fat than in water, so at depth the fat-rich marrow of long bones loads with a disproportionate amount of dissolved inert gas. On rapid ascent this marrow becomes supersaturated and bubbles form preferentially there. Within the rigid bony compartment the bubbles raise intramedullary pressure and obstruct sinusoidal blood flow, producing the ischaemia that kills bone. The combination of high fat solubility, a non-expansile compartment, and a relatively end-arterial subchondral supply explains why long-bone heads are targeted DOI.
Q: A diver has a calcified medullary infarct in the femoral shaft and a separate lesion in the femoral head. Which matters more and why? A: The femoral head (juxta-articular) lesion matters more. Juxta-articular lesions can undergo subchondral fracture and collapse, leading to pain and secondary arthritis, whereas diaphyseal shaft infarcts have no articular surface to fail and are usually stable, asymptomatic, and managed by observation. According to PubMed, lesions cluster in the proximal humerus and femur, and it is the head lesions that drive the disability DOI.
Q: Why does reported prevalence of dysbaric osteonecrosis range from 0% to about 70%? A: Because prevalence is driven by decompression discipline and surveillance, not by diving alone. Strictly regulated military divers following decompression rules and undergoing periodic examination can show no excess of bone lesions over non-divers, while unregulated artisanal diving fishermen who dive deep, often, and without safe decompression show some of the highest rates recorded - around three-quarters in one radiographic series. The wide range is the exam's way of saying the disease is largely preventable DOI DOI.
Q: Which imaging test detects dysbaric osteonecrosis earliest? A: MRI. It detects marrow change and the reactive low-signal interface band before any abnormality appears on plain radiographs, and it allows several joints to be surveyed without ionising radiation. Radiographs are used for staging (sclerosis, cysts, bone islands, crescent sign, head flattening) and CT helps define lesion extent and detect a subchondral fracture before surgery DOI.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A diver is found to have osteonecrosis of the humeral head. Explain to me, from first principles, how diving could have caused this.”
“A 45-year-old artisanal diving fisherman presents with chronic right shoulder pain. He has dived deep on surface-supplied air for over 20 years and has had several episodes of joint pains after dives. How would you assess and investigate him?”
Core Concept
- Osteonecrosis caused by decompression - nitrogen bubbles in fatty marrow cut off blood flow
- Same final pathway as any avascular necrosis; the trigger is decompression, not steroids/alcohol/trauma
- Henry's law plus high fat-solubility of nitrogen = fatty marrow loads heavily at depth
- Bone is a rigid compartment - bubbles raise intramedullary pressure and obstruct sinusoids
Who and Where
- Divers (artisanal/indigenous highest risk; technical divers emerging) and compressed-air/caisson workers
- Sites that matter: humeral head and femoral head (juxta-articular)
- Shaft (diaphyseal) infarcts are usually asymptomatic and observed
- Frequently bilateral and multifocal - image both shoulders and both hips
Diagnosis
- MRI most sensitive - detects pre-radiographic disease and the reactive band
- Radiographs stage: sclerosis, cysts, bone islands, shaft infarct calcification, crescent sign, flattening
- CT defines lesion extent and detects the subchondral fracture (crescent)
- Crescent sign is the watershed between salvageable and unsalvageable joints
Management
- Prevention is the real treatment: safe decompression, depth/bottom-time limits, surveillance, prompt DCS treatment
- Asymptomatic shaft lesions: observe and reassure
- Pre-collapse head lesions: core decompression, free vascularised fibular graft
- Post-collapse / secondary arthritis: arthroplasty of the affected joint
Exam Triggers
- Prevalence 0% to about 70% - driven by decompression discipline, not diving itself
- Disciplined military divers may show no excess over non-divers (preventable disease)
- Established juxta-articular lesions often progress even after diving stops
- Address fitness to dive once juxta-articular disease is confirmed
Evidence Base and Key Literature
Dysbaric Osteonecrosis: Pathophysiology, Presentation and Management - Literature Review
- Dysbaric osteonecrosis is associated with prolonged hyperbaric exposure and rapid decompression that drive nitrogen bubbles into fatty marrow-containing shafts of long bones, reducing blood flow and causing osteonecrosis
- Patients are frequently asymptomatic; typical radiographic findings are decalcification, cystic lesions, osteosclerotic patterns, non-traumatic fractures, bone islands and a subchondral crescent sign
- Surgical options include core decompression and free vascularised fibular graft; non-surgical options include monitoring, physical therapy and bisphosphonate therapy
- Incidence has fallen markedly over recent decades but delayed diagnosis and suboptimal management keep the condition relevant
Dysbaric Osteonecrosis Among Professional Divers: A Literature Review
- Reported prevalence of dysbaric osteonecrosis in professional divers ranges from 0% to 70.6%, highest in settings such as Turkey, Hawaii, Korea and Japan and dependent on activity and medical monitoring
- Risk is very low for military divers who strictly follow decompression rules and undergo periodic medical examination
- Lesions predominate in the proximal femur and proximal humerus
- In the majority of cases lesions progress despite the absence of further dysbaric exposure