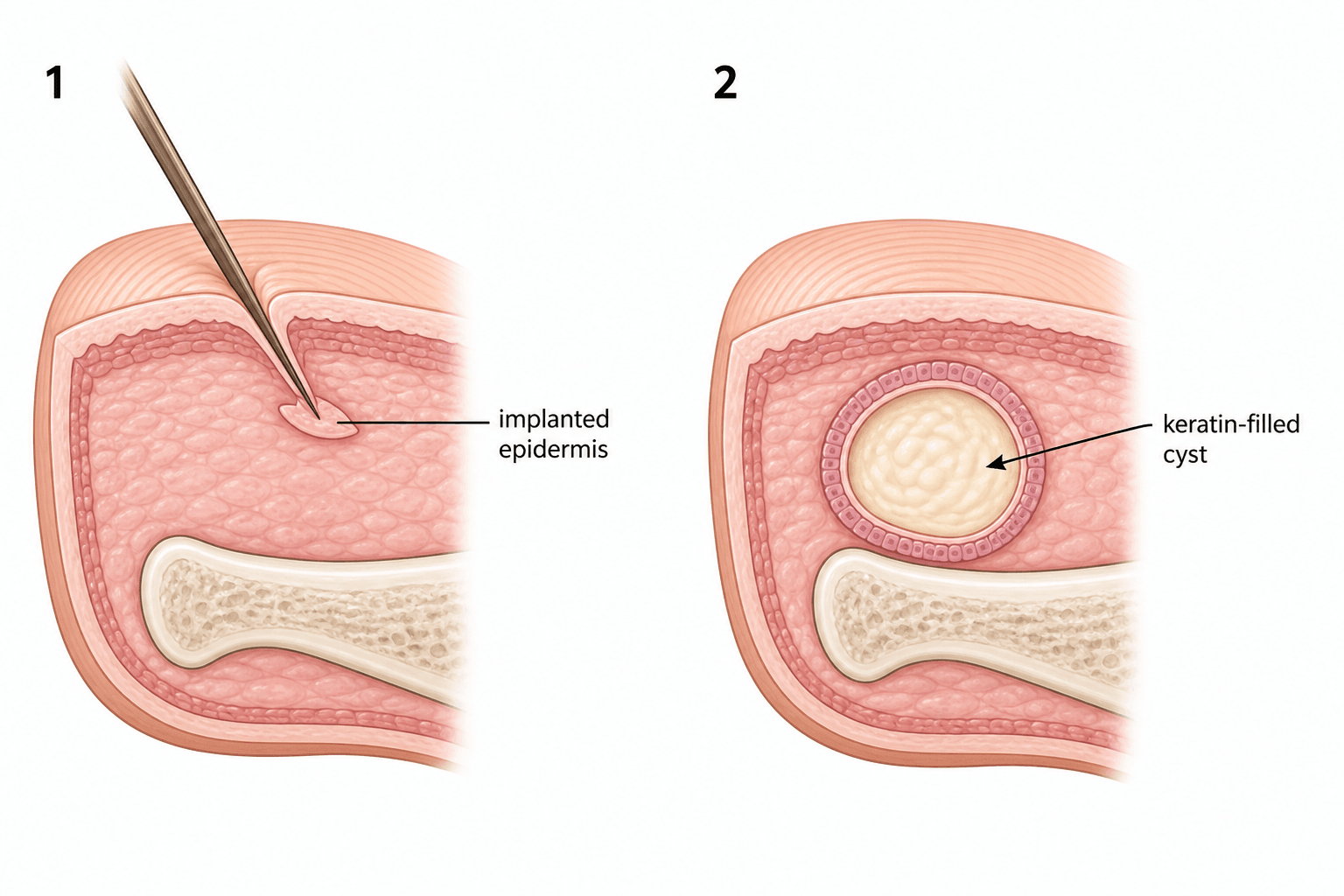
Implanted Epidermis -> a Keratin-Filled Cyst
- An epidermal inclusion cyst (epidermoid/implantation cyst) of the hand forms when keratinising SQUAMOUS EPIDERMIS is implanted into the deeper tissues, usually by PENETRATING TRAUMA or surgery; the implanted epithelium proliferates and produces KERATIN, creating a cyst lined by stratified squamous epithelium and filled with keratin debris.
- It typically presents as a FIRM, slowly enlarging, usually PAINLESS subcutaneous NODULE on the VOLAR fingertip/pulp or palm, often with a HISTORY OF TRAUMA (a puncture, laceration or prior surgery) weeks to years earlier; it can become tender or secondarily infected.
- A distinct INTRAOSSEOUS variant occurs in the DISTAL PHALANX (and the skull), appearing as a well-defined LYTIC lesion that may expand the bone or cause a pathological fracture - it is a recognised benign bone lesion of the hand.
- The DIFFERENTIAL of a hand mass includes a GANGLION (the commonest hand mass, transilluminates, near joint/tendon sheath), GIANT CELL TUMOUR OF THE TENDON SHEATH, foreign-body granuloma, glomus tumour (subungual, painful, cold-sensitive), and - for an intraosseous lytic lesion - ENCHONDROMA (the commonest bone tumour of the hand) and OSTEOMYELITIS (especially with a chronic digital wound, which can coexist with an epidermoid cyst).
- DIAGNOSIS is clinical (a firm nodule with a trauma history) supported by imaging - ultrasound shows a well-defined cyst; radiographs show an intraosseous lytic lesion with a sclerotic margin - but DEFINITIVE diagnosis is HISTOLOGICAL: a cyst lined by stratified squamous epithelium with laminated keratin and NO skin adnexa (which distinguishes it from a true dermoid cyst).
- TREATMENT is COMPLETE SURGICAL EXCISION of the soft-tissue cyst including its entire lining (incomplete removal -> RECURRENCE), or CURETTAGE (+/- bone graft/substitute) for the intraosseous form; where an epidermoid cyst coexists with osteomyelitis, thorough debridement/curettage plus antibiotics treats both.
- “Epidermal inclusion cyst = traumatic implantation of epidermis -> squamous-lined, KERATIN-FILLED cyst (no adnexa).
- “Firm painless volar finger/palm nodule with a trauma history; intraosseous variant = lytic distal phalanx lesion.
- “Differential: ganglion (commonest), GCTTS, glomus, enchondroma, osteomyelitis. Treat by COMPLETE excision/curettage - incomplete removal recurs.
Ganglion (commonest, transilluminates), giant cell tumour of tendon sheath, epidermal inclusion cyst (trauma history, keratin-filled), glomus tumour (subungual, painful).
Enchondroma (commonest hand bone tumour), intraosseous epidermoid cyst, osteomyelitis (chronic wound - can coexist with an epidermoid cyst). Image and biopsy.
Pathogenesis & Presentation
The fingertip and palm are frequently subject to penetrating injuries; if a fragment of surface epidermis is driven into the deeper tissue (or buried at surgery), the trapped keratinising epithelium continues to grow and shed keratin into an enclosing cyst. The result is a firm, well-circumscribed, slowly enlarging subcutaneous nodule, usually on the volar fingertip/pulp or palm, typically painless unless it is large, ruptures or becomes infected. A careful history often reveals a previous puncture, laceration or operation at the site, sometimes years earlier. An intraosseous epidermoid cyst of the distal phalanx presents instead as a localised lytic lesion, with swelling, nail changes or a pathological fracture.
Terminology, frequency and natural history
Two naming points are worth settling first, because both get asked. The lesion is not a "sebaceous cyst" - that term is a long-standing misnomer, since the cyst contains keratin, not sebum, and arises from keratinising epidermis rather than from sebaceous glands. And "epidermoid", "epidermal inclusion" and "implantation" cyst all describe the same thing in the hand; the last is the most honest name, because in the hand the mechanism is nearly always implantation rather than a spontaneously occluded follicle.
On frequency, be careful with the usual one-liner. Across hand and wrist masses overall the ganglion dominates and the epidermal inclusion cyst is one of the next commonest benign lesions, but the ranking shifts with the site studied: in series restricted to the fingers, giant cell tumour of the tendon sheath often comes first, and excision-only series under-count ganglia because so many are aspirated or simply observed rather than sent to pathology. The safe exam answer is that the ganglion is the commonest hand mass overall, with GCTTS and the epidermal inclusion cyst the other two names expected in the same breath - while noting that in the digit specifically GCTTS is at least as common.
The clinical course is slow and benign. Patients are typically middle-aged adults, more often men, reflecting the occupational penetrating injuries that cause it, and the latency between the injury and a noticeable lump is long - months to many years - so a patient who denies trauma has usually just forgotten a splinter, a needlestick or a minor laceration. Left alone the cyst enlarges very gradually; it does not regress, and the events that bring it to attention are usually rupture or secondary infection rather than size alone.
Investigation & Diagnosis
Ultrasound shows a well-defined, often hypoechoic cyst and helps distinguish it from a ganglion or solid tumour; radiographs are essential if an intraosseous lesion is suspected, showing a well-defined lytic lesion with a sclerotic margin in the distal phalanx (and exclude enchondroma/osteomyelitis); MRI can characterise deeper or recurrent lesions. On ultrasound the two features that actually earn their keep are posterior acoustic enhancement (confirming it is fluid/debris-filled rather than solid) and the absence of internal vascularity on Doppler - a giant cell tumour of the tendon sheath, the main solid mimic, shows internal flow. A cyst densely packed with keratin can look deceptively solid on greyscale alone, so it is the Doppler that separates them. The definitive diagnosis is histological: a cyst lined by stratified squamous epithelium with a granular layer producing laminated (lamellated) keratin, and - importantly - no skin adnexal structures (hair follicles/sebaceous glands), which distinguishes it from a true dermoid cyst. Always send excised tissue for histology, particularly to exclude an unexpected diagnosis.
The Histology: Telling the Keratinous Cysts Apart
The diagnosis rests on a squamous lining, laminated keratin and the absence of adnexa, which distinguishes it from a dermoid - but the whole family of keratinous cysts is sorted on histology. Three features separate them: whether the lining has a granular layer, the type of keratin, and the presence of skin adnexa - and whether there is an epithelial lining at all.
- Lining
- Stratified squamous epithelium WITH a granular layer
- Contents / adnexa
- Laminated ('dry') keratin; NO adnexa
- Clue
- Trauma/implantation history
- Lining
- Squamous epithelium WITH skin adnexa
- Contents / adnexa
- Keratin plus hair follicles / sebaceous glands
- Clue
- Congenital/developmental (e.g. midline, periorbital)
- Lining
- Squamous epithelium WITHOUT a granular layer
- Contents / adnexa
- Dense, compact ('wet') keratin
- Clue
- Scalp; often multiple/familial
- Lining
- NO epithelial lining (a pseudocyst)
- Contents / adnexa
- Clear mucin / myxoid fluid
- Clue
- Near a joint or tendon sheath; transilluminates
Epidermoid = squamous lining with a granular layer, dry laminated keratin, and NO adnexa. Add skin adnexa and it is a dermoid; lose the granular layer and it is a trichilemmal cyst; lose the epithelial lining altogether and it is a ganglion. Rarely, a long-standing epidermoid cyst harbours a squamous cell carcinoma, which is the deeper reason every excised cyst goes for histology.
Management
- Soft-tissue cyst: complete surgical EXCISION including the entire cyst lining/capsule - incomplete removal (or simple rupture/aspiration) leaves epithelium behind and leads to RECURRENCE; marsupialisation is inadequate.
- Intraosseous (distal phalanx): CURETTAGE of the lesion with removal of the lining, filling the cavity with bone graft or substitute as needed; outcomes are generally good with a low recurrence after thorough curettage.
- Coexisting osteomyelitis (chronic digital wound): debridement and curettage plus antibiotics (a bone substitute carrying antibiotic is one option) treats both entities; obtain histology and culture.
- Infected cyst: treat the infection, then excise the cyst electively once settled.
Does every cyst need an operation?
No, and it is worth being able to say so. A small, asymptomatic, confidently diagnosed cyst in a site that does not interfere with function may reasonably be observed, with the patient told what would change the plan: enlargement, pain, interference with grip or pinch, repeated inflammation, or any uncertainty about the diagnosis. Two qualifications keep that from becoming a soft option. The first is that observation is only defensible when the diagnosis is genuinely secure - a firm nodule that is assumed to be an inclusion cyst is the way a solid tumour gets watched. The second is that a cyst near the pulp or a pressure point tends to declare itself eventually through rupture or infection, and an elective excision on a quiet finger is a considerably better operation than an urgent one on an inflamed one, so waiting is not risk-free.
Operative Technique: Excising the Cyst Intact
Incomplete removal recurs, so how a complete removal is achieved is the examinable point - the cyst sits among the digital neurovascular structures and its contents provoke a reaction if spilled.
- Operate under tourniquet and loupe magnification; plan the incision to give access without crossing a flexion crease.
- Dissect the cyst out with its entire lining/capsule INTACT - rupture spills keratin, which both incites a foreign-body inflammatory reaction and risks leaving lining behind and recurrence.
- Protect the digital neurovascular bundles in the pulp. If the cyst ruptures, meticulously excise all visible lining and irrigate the wound.
- Make a cortical window, then thoroughly curette the lesion, removing the entire lining to a clean, bleeding cavity (a high-speed burr of the walls helps).
- Fill the cavity with bone graft or substitute as needed; send material for histology and culture.
- Recurrence is low after thorough curettage - it is incomplete curettage that recurs.
The operative goal is total removal of the epithelial lining: en-bloc excision without rupture for the soft-tissue cyst, thorough curettage to clean bone for the intraosseous form. Rupture-with-retained-lining (or simple aspiration/marsupialisation) is exactly why these recur.
Complications
The cyst itself is benign and the operation small, so the complications divide into what the untreated cyst does and what the excision costs.
- Rupture and foreign-body reaction. Extruded keratin is intensely irritant in the soft tissues, producing a painful, red, swollen digit that looks infected but is initially a sterile inflammatory reaction. It is the commonest reason an indolent lump suddenly becomes symptomatic, and it matters surgically because the inflamed, ruptured cyst has lost the clean plane that makes complete excision easy.
- Secondary infection and abscess, which may follow rupture or arise independently; a genuinely infected cyst is drained first and excised electively once quiet, since excision through infected tissue both fails to achieve a clean plane and risks a worse wound.
- Recurrence, essentially always from retained lining - after rupture during dissection, after aspiration, or after marsupialisation. This is the reason the technique above insists on removing the capsule intact.
- Digital nerve or artery injury, a real risk given how often these sit in the volar pulp among the neurovascular bundles; loupe magnification and tourniquet control are not optional refinements.
- Painful or adherent scar and pulp tenderness, particularly for a volar fingertip incision, which is why the incision is planned off the pinch surface and away from flexion creases.
- Bone involvement in the intraosseous form - progressive expansion, cortical thinning and pathological fracture of the distal phalanx, and nail deformity where the lesion abuts the germinal matrix.
- Malignant transformation, chiefly to squamous cell carcinoma, is genuinely rare but real and is the substantive reason every excised cyst goes to histology rather than into the bin. Suspect it in a long-standing cyst that grows rapidly, ulcerates, becomes fixed or recurs atypically.
Mnemonics & Memory Aids
KERATIN
Hook:KERATIN captures the epidermal inclusion cyst story.
GEEO (lytic distal phalanx)
Hook:Lytic distal phalanx? Think GEEO: Glomus, Enchondroma, Epidermoid, Osteomyelitis.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has a firm, painless nodule in the pulp of a finger and recalls a splinter injury there two years ago. What is the likely diagnosis and how would you confirm and treat it?”
“A radiograph shows a well-defined lytic lesion in the distal phalanx of a finger. How do you approach it?”
Pathogenesis
- Traumatic/surgical implantation of epidermis into deeper tissue
- Implanted epithelium makes keratin -> squamous-lined, keratin-filled cyst
- No skin adnexa (distinguishes from true dermoid)
Presentation
- Firm, slowly enlarging, usually painless nodule (volar finger/palm)
- History of prior puncture/laceration/surgery
- Intraosseous variant: lytic lesion of the distal phalanx (+/- pathological fracture)
Differential & diagnosis
- Soft tissue: ganglion (commonest), GCTTS, foreign-body granuloma, glomus
- Intraosseous lytic: enchondroma, epidermoid, osteomyelitis (can coexist)
- US/X-ray/MRI; DEFINITIVE = histology (squamous lining + keratin)
Treatment
- Soft tissue: COMPLETE excision of cyst + lining (incomplete -> recurrence)
- Intraosseous: curettage + lining removal +/- bone graft/substitute
- Coexisting osteomyelitis: debridement/curettage + antibiotics; always send histology
Evidence & Key Studies
Intraosseous epidermoid cyst discovered in the distal phalanx of a thumb: a case report
- Intraosseous epidermoid cyst is a rare benign inclusion cyst found mainly in the skull and phalanges.
- Once differentiated from similar lytic lesions, it can be treated with simple CURETTAGE, seldom needing additional procedures.
- The case was treated successfully without complication, illustrating the favourable outcome of the distal-phalanx variant.
Chronic digital wound: epidermoid cyst, osteomyelitis or both? Two cases and review
- Epidermoid bone cyst and osteomyelitis of the distal phalanx can coexist, and both are linked to previous trauma, nail alterations and chronic inflammatory signs.
- Definitive diagnosis requires histopathology, and good surgical debridement is needed to heal both entities.
- Curettage with filling of the bone defect using an antibiotic-loaded bone substitute is a good treatment option.
Clinicopathological analysis of soft-tissue tumours and tumour-like lesions of the fingers (134 patients)
- 134 finger masses excised over a decade in an industrial region: ALL were benign, mean age 47.6 years, with the third and first fingers most often affected.
- Giant cell tumour of the tendon sheath was the commonest lesion at 37.3%, ahead of ganglion cyst at 14.2% - a higher TSGCT share than usually reported, showing that the familiar 'ganglion is commonest' ranking shifts when the series is restricted to the fingers.
- Epidermal cysts were significantly more common in men (p = 0.039); clinical-pathological diagnostic concordance was 76.1%, so roughly one finger mass in four was not what it was clinically thought to be.
The rarity, distribution (skull/phalanges) and curettage treatment of the intraosseous epidermoid cyst come from the cited Shin case report; the coexistence with osteomyelitis, the link to prior trauma, and the need for histology and debridement/curettage from the cited Portes-Chiva report; and the finger-mass frequency distribution, the male predominance of epidermal cysts and the 76.1% clinical-pathological concordance from the cited Gok series. The traumatic-implantation mechanism, the keratin-filled squamous histology and the soft-tissue excision principle are standard hand-surgery teaching. (See also our Ganglion, Giant Cell Tumour of Tendon Sheath, Enchondroma and Hand Infections topics.)