A Surgical Emergency: Delay in diagnosis leads to permanent paralysis.
Anatomical Location
Critical Must-Knows
- The 'Classic Triad' (Fever, Back Pain, Neurology) is rarely present (less than 15%).
- Back pain is the most consistent symptom (greater than 70%).
- Any patient with Back Pain + Fever + Risk Factors needs an MRI.
- Neurological deficit is an indication for EMERGENCY surgery.
- Paralysis can become permanent within hours.
Clinical Pearls
- "Paralysis is due to mechanical compression AND venous thrombosis (venous stasis).
- "Once paralysis sets in, less than 50% recover function even with surgery.
- "CRP is almost always elevated (greater than 90%), unlike WCC.
- "Lumbar Puncture is CONTRAINDICATED (risk of meningitis spreading).
Critical Errors
Delaying MRI
Negligence. Do not wait for neurological signs. Any high-risk patient with severe back pain needs an urgent MRI.
LP Contraindicated
Major Safety Violation. Do NOT puncture an infected site. Risk of seeding meningitis.
Medical Management
Strict Criteria. Only for: Neurologically Intact AND Identified Organism AND Stable. Close monitoring essential.
At a Glance
SEA vs Discitis
| Feature | Epidural Abscess | Discitis / Osteomyelitis |
|---|---|---|
| Urgency | Emergency (Hours) | Urgent (Days) |
| Main Risk | Cord Compression (Paralysis) | Instability / deformity |
| Location | Epidural Space | Disc & Endplate |
| Surgery | Decompression (Laminectomy) | Biopsy / Debridement / Fusion |
Mnemonics
RISKRisk Factors
| R | Renal / Diabetes Immunocompromised state |
| I | IV Drug Use Direct inoculation / S. aureus |
| S | Skin / Spine Recent infection or procedure |
| K | Known Infection Distant site (UTI, Pneumonia) |
| R | Renal / Diabetes Immunocompromised state | S | Skin / Spine Recent infection or procedure |
| I | IV Drug Use Direct inoculation / S. aureus | K | Known Infection Distant site (UTI, Pneumonia) |
Hook:Who gets SEA?
Pain - Shoot - Weak - ParalyzedHeusner's Stages
| 1 | Pain Focal back pain |
| 2 | Shoot Radicular pain (nerve root irritation) |
| 3 | Weak Motor weakness / Sensory loss |
| 4 | Paralysis Complete paraplegia (Irreversible) |
| 1 | Pain Focal back pain | 3 | Weak Motor weakness / Sensory loss |
| 2 | Shoot Radicular pain (nerve root irritation) | 4 | Paralysis Complete paraplegia (Irreversible) |
Hook:Progression of disease.
SECCommon Pathogens
| S | Staph aureus Most common (greater than 60%) (MSSA/MRSA) |
| E | E. coli Gram negatives from UTI |
| C | Coag-neg Staph Skin flora (epidermidis) |
| S | Staph aureus Most common (greater than 60%) (MSSA/MRSA) |
| E | E. coli Gram negatives from UTI |
| C | Coag-neg Staph Skin flora (epidermidis) |
Hook:Bugs.
Overview and Epidemiology
Definition A collection of pus (purulent material) within the epidural space of the spinal canal.
Epidemiology
- Incidence is rising (aging population, IVDU, spinal procedures).
- Common in men (2:1).
- Peak age 50-70.
Pathophysiology
- Bacteria enter the epidural space via hematogenous spread (skin, UTI) or direct extension (discitis).
- The infection causes mechanical compression of the cord/cauda equina.
- It also causes septic thrombophlebitis of the epidural veins → Venous congestion → Cord ischemia → Infarction.
Pathophysiology and Mechanisms
Epidural Space
- Potential space between the Dura Mater and the Periosteum/Ligamentum Flavum.
- Contains fat and the Batson's Venous Plexus.
Batson's Plexus
- Valveless venous system.
- Allows retrograde spread of infection from pelvic organs (e.g., during coughing/straining) to the spine.
- Explains why UTI is a common source.
Anterior vs Posterior
- Posterior: Most common in Thoracic/Lumbar spine (more epidural fat posteriorly).
- Anterior: Associated with Vertebral Osteomyelitis/Discitis (direct extension).
Classification Systems
Anatomical Classification Based on location relative to the Dura.
- Posterior: Behind the cord. (Majority). Easier to decompress via laminectomy.
- Anterior: In front of the cord. Harder to access. Often requires corpectomy or transpedicular approach.
- Circumferential: Surrounds the cord. High risk of ischemia.
Clinical Assessment
History
- Classic Triad: Fever + Back Pain + Neurology. (Only 10-15% sensivity).
- Back Pain: Most common symptom (greater than 75%). Severe, unrelenting, night pain.
- Fever: Only present in ~50%.
- History of: IVDU, Diabetes, Recent spinal injection, UTI.
Examination
- Spine: Focal percussion tenderness (Highly suspicious).
- Neurology:
- Assess Power (Myotomes).
- Assess Sensation (Fluid level? Saddle anesthesia?).
- Assess PR Tone/Sensation (Cauda Equina).
Red Flags
- New onset back pain in an IV Drug User = SEA until proven otherwise.
Imaging and Investigations
Diagnostic Protocol
- WCC: Elevated in ~60% (Unreliable).
- CRP/ESR: Elevated in greater than 95% (Highly Sensitive).
- Blood Cultures: Positive in ~60%. Guide antibiotic therapy.
- T1: Iso/Hypointense.
- T2: Hyperintense (High signal) fluid collection.
- T1+Gad: Peripheral enhancement (Ring enhancement) with central non-enhancing pus.
- Cord Signal: Look for T2 hyperintensity in the cord (Edema/Myelomalacia).
- Used if MRI contraindicated (Pacemaker).
- CT Myelogram is the alternative.
- Shows compression but misses cord signal changes.
Imaging Gallery

Management Algorithm
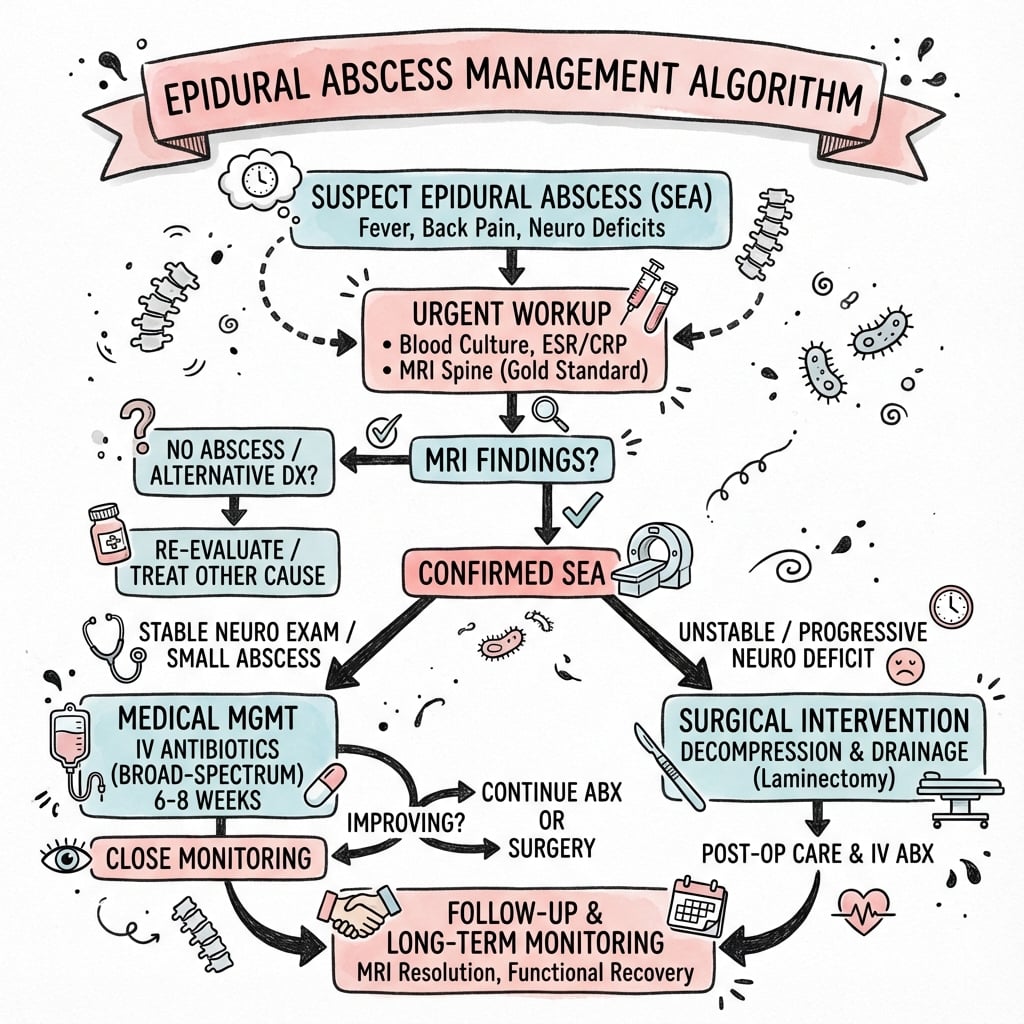
Treatment Protocols
Medical Management
- Reserved for:
- Neurologically intact patients.
- Known organism (Blood Cx or Biopsy positive).
- Too unfit for surgery.
- Complete paralysis greater than 48-72 hours (salvage unlikely).
- Antibiotics: Empiric (Vanc + Ceftriaxone) → Targeted.
- Monitoring: Daily neurological checks. Serial MRI if worsening.
Failure of Medical Management
- Defined as:
- New neurological deficit.
- Persistent fever/CRP elevation.
- Increasing pain.
- Enlargement of abscess on MRI.
Surgical Technique
Laminectomy
- Goal: Evacuate pus and decompress the neural elements.
- Technique:
- Midline approach.
- Wide Laminectomy (remove spinous process and lamina).
- Identifying the abscess (often epidural fat is inflamed/indurated).
- Irrigation and gentle suction.
- Drains: Leave large bore drains.
- Note: Culture the pus!
Complications
| Complication | Rate | Impact |
|---|---|---|
| Permanent Paralysis | 4-22% | Devastating. Predictor: Pre-op deficit severity. |
| Death | 5-15% | Due to Sepsis / Multi-organ failure. |
| Recurrence | 10% | Inadequate drainage or short antibiotic course. |
| Meningitis | Rare | Due to dural tear during surgery. |
Postoperative Rehab
Antibiotics
- Long term IV (usually 6-8 weeks).
- Oral suppression may be needed lifelong if implant retained (rare).
Rehabilitation
- Spinal Cord Injury protocol if deficit persists.
- Bladder/Bowel management.
- Pressure area care.
Outcomes and Prognosis
Prognostic Factors
- Pre-operative Neurology: The single most important factor.
- Duration of Deficit: Less than 36 hours has better prognosis.
- Age: Greater than 65 has worse outcome.
- Diabetes: Associated with higher mortality.
Recovery
- Complete recovery is rare if paralysis has set in.
- Early decompression (less than 24 hours) yields best results.
Evidence Base
Diagnostic Delay and the Myth of the Triad
- Case-control study: 63 SEA patients matched 2:1 to 126 controls with spine pain.
- The classic triad (fever, spine pain, neurology) was present in only 13% of SEA patients at the initial visit.
- One or more risk factors were present in 98% of SEA patients vs 21% of controls — risk-factor screening beats the triad.
- Diagnostic delays occurred in 75%; residual motor weakness rose from 13% (no delay) to 45% (delay), OR 5.65.
- ESR was more sensitive and specific than total white cell count as a screen.
Landmark Meta-Analysis (915 Patients)
- Pooled 915 published SEA cases (1954–1997); incidence 0.2–2 per 10,000 hospital admissions.
- Back pain was the initial symptom in 71% and fever in 66%; complete paralysis (stage 4) affected only 34%.
- Diabetes was the most common predisposing factor; Staphylococcus aureus the most common organism.
- MRI showed the greatest diagnostic accuracy; myelography is no longer recommended.
- Lumbar puncture risks seeding the subarachnoid space (meningitis) and should not be performed; mortality fell from 34% to 15%.
Antibiotics Alone vs Early Surgery
- 48 patients (median age 61); only 23/48 were febrile and WBC was frequently normal.
- Of 23 started on antibiotics alone, 11 deteriorated and required delayed surgery.
- Patients managed without early surgery had significantly more unfavourable outcomes (deterioration or death), P less than 0.005.
- IV drug abuse was the commonest risk factor; S. aureus the commonest organism.
Predictors of Failed Medical Management
- 355 patients; of those started non-operatively, 54 failed and 73 succeeded without surgery.
- Neurologic deficit (incomplete or complete cord injury) was the single most significant predictor of failure.
- Age over 65, diabetes and MRSA were also independent risk factors for failure.
- Patients with all four risk factors had a 99% predicted probability of failing antibiotics alone.
Authoritative Clinical Review (NEJM)
- Defines SEA as a neurosurgical emergency; gadolinium-enhanced MRI is the imaging modality of choice.
- Recommends prompt surgical decompression plus drainage combined with culture-directed antibiotics.
- Empirical cover should include staphylococci (incl. MRSA) and Gram-negative bacilli pending cultures.
- Outcome is dictated chiefly by the neurological status at the time of intervention.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Missed Diagnosis
"A 50M IVDU presents with severe back pain. Afebrile. Neuro intact. GP gave NSAIDs. Returns 2 days later with urinary retention. What happened?"
Medical Management
"65F with L3 SEA. S. aureus. Neuro intact. Unfit for surgery (Severe COPD). Can you treat medically?"
The Empirical Antibiotic Choice
"A septic patient with a thoracic SEA and an emerging paraparesis is going to theatre. The microbiology results are not yet back. What antibiotics do you start, and when?"
MCQ Practice Points
Diagnosis
Q: Most sensitive screening test for SEA? A: ESR / CRP (greater than 95% sensitivity). WCC is often normal.
Anatomy
Q: Which venous system facilitates spread from the pelvis to the spine? A: Batson's Venous Plexus (Valveless).
Management
Q: Absolute indication for surgery in SEA? A: Neurological Deficit (e.g., foot drop, retention).
Pathogen
Q: Most common causative organism? A: Staphylococcus aureus (greater than 60%).
Contraindication
Q: Which procedure is contraindicated in suspected SEA? A: Lumbar Puncture. Risk of introducing infection to the subarachnoid space (Meningitis).
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence is rising worldwide: historically 0.2–2 per 10,000 hospital admissions (Reihsaus), now commonly quoted at 2–8 per 10,000 in tertiary centres, driven by an ageing population, diabetes, injection drug use and increasing spinal instrumentation.
- Male predominance (roughly 1.5–2:1); peak age 50–70 years.
- Staphylococcus aureus causes 60–70% of cases; the proportion of MRSA varies markedly by region and rises where community-acquired MRSA is endemic. Gram-negative organisms (e.g. E. coli) point to a urinary source; consider Mycobacterium tuberculosis (Pott disease) and Brucella in high-prevalence and limited-resource settings.
Guidance — Areas of Broad International Agreement
Where Major Bodies Align
| Theme | Consensus Position | Source / Society |
|---|---|---|
| Imaging | Gadolinium-enhanced MRI of the whole spine is first-line; skip lengths are common, so image neuraxis if multifocal suspected | NEJM review; IDSA vertebral osteomyelitis guidance |
| Microbiological diagnosis | Obtain blood cultures and, where safe, image-guided or operative sampling BEFORE antibiotics unless septic/unstable | IDSA 2015 (vertebral osteomyelitis); BSAC |
| Surgery for deficit | Neurological deficit or deterioration mandates urgent decompression plus antibiotics | NEJM; NASS / spine society consensus |
| Antibiotic duration | Typically 6 weeks or more of culture-directed therapy, often IV-led; longer with concomitant osteomyelitis | IDSA 2015; BSAC |
Where Practice Genuinely Varies
- Empirical regimen: vancomycin (MRSA cover) plus a broad Gram-negative agent (e.g. ceftriaxone, cefepime or an antipseudomonal in IVDU/healthcare-associated cases) is widespread, but local antibiograms and MRSA prevalence drive the exact choice. Where MRSA is rare, an anti-staphylococcal penicillin may suffice.
- Initial non-operative trial: more readily adopted in high-resource centres with rapid MRI access and the ability to monitor with frequent neuro-obs and serial imaging; risky where MRI and theatre access are limited, so earlier surgery is often favoured.
- Source-setting differences: in TB-endemic and limited-resource regions, tuberculous epidural abscess is a major differential and changes both imaging interpretation and drug therapy.
Registry & Outcome Notes
- SEA is not tracked in arthroplasty registries; the evidence base is retrospective cohorts and meta-analyses (Reihsaus; Curry; Kim) rather than RCTs. No high-quality randomised data compares medical vs surgical management — a key limitation acknowledged across guidelines.
Controversies & Areas of Uncertainty
Who can be managed without surgery?
The biggest controversy. Selected neurologically intact patients with an identified organism can sometimes be treated with antibiotics alone, but failure rates approach 40% and rise to ~99% when age over 65, diabetes, MRSA and any deficit coexist (Kim et al). There is no RCT — decisions rest on cohort data and require vigilant monitoring.
Timing of surgery once paralysed
Complete deficits beyond ~24–72 hours have poor recovery, raising the question of whether late decompression helps. Practice varies: many still operate for source control and instability even when neurological salvage is unlikely. Earlier intervention consistently outperforms delayed surgery.
Instrumentation in active infection
Whether to instrument an actively infected spine is debated. Titanium implants and contemporary series suggest fusion can be safe with adequate debridement and antibiotics, but many surgeons avoid metalwork in frank pus unless instability or concurrent osteomyelitis demands it.
Antibiotic duration & route
The traditional 6+ weeks of IV therapy is being challenged. Oral switch trials in bone and joint infection (e.g. OVIVA) suggest oral therapy may be non-inferior in selected, stable patients, though SEA-specific data remain limited.
Exam Day Cheat Sheet
SEA Summary
Clinical summary
Classic Triad
- •Back Pain (100%)
- •Fever (50%)
- •Neurology (Late)
- •Tenderness (Focal)
Workup
- •MRI Gadolinium (Gold Std)
- •Blood Cx x3
- •ESR/CRP (Sensitive)
- •Look for Source (Echo)
Management
- •Decompression (If Neuro Deficit)
- •Antibiotics (6w+)
- •Monitor CRP
- •Stabilize if needed
Red Flags
- •IV Drug Use
- •Diabetes
- •Recent Procedure
- •Night Pain
Image Manifest
- [4-sagittal-view-of-t2-diffusion-mri-lumbar-spine-sho.png]: Lumbar Abscess T2
- [1-sagittal-t2-weighted-magnetic-resonance-imaging-mr.png]: Cervical Abscess T2
- [sea_algorithm.png]: Management Algorithm