Diagnosis | Imaging | Medical Management | Surgical Indications
ANATOMICAL PATTERNS
Critical Must-Knows
- Thoracolumbar junction (T10-L2) is most common site
- Disc preservation early distinguishes from pyogenic infection
- Cold abscess does not contain pus - caseous material
- MRI is the imaging modality of choice - high sensitivity, detects marrow, abscess and cord involvement
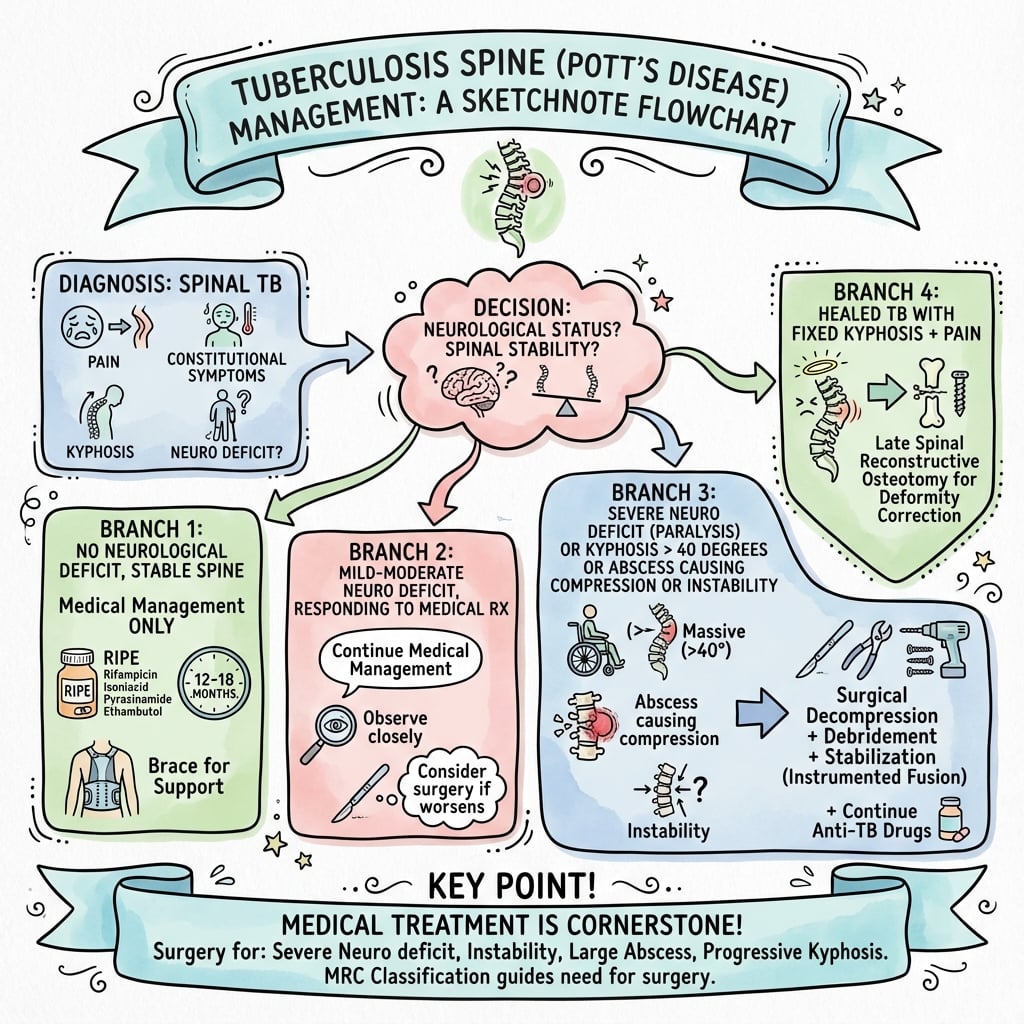
- Medical treatment first - surgery for specific indications
Clinical Pearls
- "Paradiscal type is most common - adjacent vertebrae + disc involvement
- "Skip lesions in 10-15% - always image whole spine
- "Psoas abscess is pathognomonic when combined with spine findings
- "Neurological deficit from granulation tissue, abscess, or kyphosis
Clinical Imaging
Imaging Gallery

Critical Spinal TB Exam Points
Disc Preservation
Early TB preserves the disc while pyogenic infection destroys it early. This is a key differentiating feature. However, late-stage TB can involve the disc. Always compare with clinical tempo - TB is insidious, pyogenic is acute.
Cold Abscess
Cold abscess is characteristic of TB - it lacks acute inflammatory features and contains caseous material, not pus. It can track along fascial planes (psoas abscess). The absence of local warmth and systemic toxicity distinguishes it from pyogenic abscess.
Imaging Sensitivity
MRI is essential - high sensitivity for marrow oedema, paravertebral and epidural abscess, and cord compression, and earlier than plain films. X-rays become positive only once substantial trabecular bone is destroyed (months of delay). Always image the whole spine for skip lesions.
Medical First
Medical treatment is primary - 85-90% respond to antitubercular therapy (ATT) alone. Surgery reserved for: progressive neurology, instability, failure of medical treatment, severe kyphosis. Even with neurology, medical treatment often effective.
Spinal TB vs Pyogenic Spondylitis (MRI feature frequencies from meta-analysis)
| Feature | Tuberculosis | Pyogenic |
|---|---|---|
| Onset | Insidious (weeks-months) | Acute (days-weeks) |
| Subligamentous spread | Common (93%) | Uncommon (24%) |
| Thin, smooth abscess wall | 94% | 18% |
| Epidural extension | 77% | 25% |
| Vertebral collapse | 68% | 24% |
| Disc height loss | 22% | 59% |
| Disc signal change | 82% | 95% |
COLD ABSCESS - TB FCOLD ABSCESS - TB Features
| C | Caseous necrosis Cheese-like material, not pus |
| O | Oligosymptomatic Minimal local inflammatory signs |
| L | Long duration Insidious onset over months |
| D | Disc spared early Unlike pyogenic infection |
| A | Abscess tracking Along fascial planes (psoas) |
| B | Bone destruction gradual Less explosive than pyogenic |
| S | Skip lesions possible Non-contiguous involvement |
| C | Calcification present Pathognomonic feature |
| E | ESR elevated Often very high (more than 50) |
| S | Slow response Takes weeks for improvement |
| S | Subligamentous spread Under anterior longitudinal ligament |
| C | Caseous necrosis Cheese-like material, not pus | D | Disc spared early Unlike pyogenic infection | S | Skip lesions possible Non-contiguous involvement | S | Slow response Takes weeks for improvement |
| O | Oligosymptomatic Minimal local inflammatory signs | A | Abscess tracking Along fascial planes (psoas) | C | Calcification present Pathognomonic feature | S | Subligamentous spread Under anterior longitudinal ligament |
| L | Long duration Insidious onset over months | B | Bone destruction gradual Less explosive than pyogenic | E | ESR elevated Often very high (more than 50) |
Hook:COLD ABSCESSES lack heat, redness, and acute toxicity - unlike pyogenic
SPINE TB - ISPINE TB - Imaging Findings
| S | Skip lesions Non-contiguous vertebral involvement |
| P | Preservation of disc (early) Key differentiator from pyogenic |
| I | Intraosseous abscess Within vertebral body |
| N | Narrow disc (late) Secondary to collapse |
| E | Epidural extension Causing cord compression |
| T | Thin-walled abscess Smooth margins |
| B | Bilateral psoas abscess Characteristic tracking |
| S | Skip lesions Non-contiguous vertebral involvement | N | Narrow disc (late) Secondary to collapse | B | Bilateral psoas abscess Characteristic tracking |
| P | Preservation of disc (early) Key differentiator from pyogenic | E | Epidural extension Causing cord compression | ||
| I | Intraosseous abscess Within vertebral body | T | Thin-walled abscess Smooth margins |
Hook:MRI is imaging modality of choice - high sensitivity for marrow, abscess and cord
SURGERY - ISURGERY - Indications for Surgery
| S | Severe kyphosis More than 40-50 degrees |
| U | Unstable spine Progressive deformity |
| R | Resistant TB MDR-TB considerations |
| G | Granulation tissue Compressing cord/roots |
| E | Extensive abscess Large cold abscess |
| R | Regressing neurology Progressive deficit despite ATT |
| Y | Yield diagnosis Biopsy for confirmation |
| S | Severe kyphosis More than 40-50 degrees | G | Granulation tissue Compressing cord/roots | Y | Yield diagnosis Biopsy for confirmation |
| U | Unstable spine Progressive deformity | E | Extensive abscess Large cold abscess | ||
| R | Resistant TB MDR-TB considerations | R | Regressing neurology Progressive deficit despite ATT |
Hook:Most patients (85-90%) respond to medical treatment alone
Overview and Epidemiology
Spinal tuberculosis (Pott's disease) is the most common form of skeletal tuberculosis, first described by Percivall Pott in 1779. It represents a significant cause of morbidity, particularly in endemic regions, and remains important in the Australian context due to immigration patterns.
Epidemiology:
- Spinal TB accounts for 50% of all skeletal TB cases
- Second most common form of extrapulmonary TB
- Thoracolumbar junction (T10-L2) is most commonly affected
- Approximately 10-15% have skip lesions (non-contiguous involvement)
- Male to female ratio approximately 1.5:1
- Can occur at any age but peaks in second and third decades
Global Burden:
| Region | Estimated Incidence | Risk Factors |
|---|---|---|
| High endemic | More than 100/100,000 | Crowding, poverty, HIV |
| Intermediate | 10-100/100,000 | Immigration, immunosuppression |
| Low endemic | Less than 10/100,000 | Imported cases, reactivation |
Australian Context:
Australia has low TB incidence overall, but overseas-born individuals (particularly from high-burden countries) account for the majority of cases. Spinal TB may present in immigrants, refugees, or travelers, often as reactivation of latent infection years after initial exposure.
Immigration Pattern
In Australia, maintain high suspicion for spinal TB in patients from endemic regions (South Asia, Southeast Asia, Sub-Saharan Africa, Pacific Islands) presenting with chronic back pain and constitutional symptoms, even years after migration.
Pathophysiology and Anatomy
Route of Infection
Primary Infection:
- Haematogenous spread from pulmonary focus (most common)
- Arterial dissemination to vertebral bodies
- Paradiscal arteries supply adjacent vertebrae (paradiscal type)
- Batson's venous plexus may facilitate spread
Secondary Spread:
- Subligamentous extension under ALL
- Epidural spread causing cord compression
- Paravertebral spread forming cold abscess
- Psoas tracking along muscle sheath
Anatomical Patterns of Involvement
1. Paradiscal Type (50-75%):
- Most common pattern
- Involves adjacent vertebral bodies and intervening disc
- Arterial spread via paradiscal arteries
- Late disc destruction (unlike pyogenic)
- May extend to multiple levels
2. Central Type:
- Isolated vertebral body involvement
- Concertina collapse
- May produce ivory vertebra
- Spares disc initially
3. Anterior Subligamentous Type:
- Spreads under anterior longitudinal ligament
- Multi-level involvement with anterior scalloping
- Can produce skip lesions
- Extensive yet may spare vertebral integrity initially
4. Posterior Type (2-10%):
- Involves neural arch (pedicle, lamina, spinous process)
- More common in lower lumbar spine
- May cause early neurological deficit
Pathological Changes
Bone Changes:
- Granulomatous inflammation
- Caseous necrosis
- Bone destruction and sequestration
- Minimal new bone formation (unlike pyogenic)
Soft Tissue:
- Cold abscess formation (paravertebral, epidural, psoas)
- Granulation tissue proliferation
- Fibrosis with healing
Neurological Compression:
- Early: Epidural granulation tissue, abscess
- Late: Bony compression from kyphotic deformity
Classification Systems
Kumar Classification (Neurological Status)
| Stage | Description | Neurological Findings |
|---|---|---|
| I | No deficit | Normal |
| II | Sensory | Sensory loss only |
| III | Motor - ambulatory | Motor weakness, can walk |
| IV | Motor - non-ambulatory | Cannot walk |
| V | Complete paraplegia | No function below lesion |
Tuli Classification (Paraplegia Type)
Type A: Active Disease with Paraplegia
- A1: Minimal bone loss, severe deficit
- A2: Moderate bone loss, severe deficit
- A3: Extensive bone loss with deficit
Type B: Healed Disease with Paraplegia
- B1: Cord compression from healed kyphosis
- B2: Reactivation in previously healed lesion
This classification guides surgical approach and prognosis for neurological recovery.
Clinical Assessment
History
Presenting Symptoms:
| Symptom | Frequency | Characteristics |
|---|---|---|
| Back pain | 90-95% | Insidious, localized, constant |
| Constitutional | 50-70% | Weight loss, night sweats, fever |
| Neurological | 20-30% | Weakness, sensory changes |
| Deformity | 30-40% | Visible kyphosis (gibbus) |
| Abscess | 20-30% | Swelling (groin, flank) |
Key History Elements:
- Duration of symptoms (typically weeks to months)
- Constitutional symptoms (weight loss, night sweats, low-grade fever)
- Neurological symptoms (weakness, numbness, bowel/bladder)
- Contact history (TB exposure)
- Country of origin and travel
- Immunocompromise (HIV, diabetes, immunosuppressants)
- Previous TB treatment
Physical Examination
Spinal Assessment:
- Gibbus deformity (angular kyphosis)
- Localized tenderness
- Paraspinal muscle spasm
- Restricted range of motion
- Cold abscess (paravertebral, groin, flank)
Neurological Examination:
- Motor power (myotomes)
- Sensory level
- Reflexes
- Long tract signs (spasticity, clonus, Babinski)
- Bladder/bowel function
- Gait assessment
Systemic Examination:
- Lymphadenopathy
- Pulmonary findings (primary TB)
- Peripheral cold abscess
- Signs of other organ involvement
Cold Abscess Features
A cold abscess lacks the cardinal signs of inflammation (calor, rubor, dolor, tumor). It presents as a non-tender, fluctuant swelling that may track to distant sites (groin in psoas abscess). The absence of acute inflammatory features is characteristic.
Red Flags
- Rapidly progressive neurological deficit
- Complete paraplegia
- Bladder/bowel dysfunction
- Respiratory compromise (cervical lesions)
- Signs of MDR-TB or treatment failure
Investigations
Laboratory Investigations
Essential Tests:
| Test | Expected Finding | Notes |
|---|---|---|
| ESR | Elevated (often more than 50) | Useful for monitoring |
| CRP | Elevated | Less specific than ESR |
| Mantoux/IGRA | Usually positive | Does not confirm active disease |
| Sputum AFB | May be positive | If pulmonary involvement |
| HIV serology | Rule out coinfection | Important for management |
Imaging Protocol
Plain Radiographs:
- First-line imaging
- Positive only when 50% trabecular bone destroyed
- May take 4-6 months to show changes
- Shows: vertebral destruction, collapse, kyphosis
MRI (modality of choice):
- High sensitivity; detects disease earlier than plain radiographs
- Essential for soft tissue assessment
- Detects epidural extension and cord compression
- Identifies skip lesions
MRI Findings:
- T1: Hypointense marrow signal
- T2/STIR: Hyperintense marrow edema
- Contrast: Rim enhancement of abscess
- Epidural extension
- Skip lesions
- Psoas/paravertebral abscess
CT Scan:
- Superior bone detail
- Calcification within soft tissue (pathognomonic)
- Bony destruction pattern
- CT-guided biopsy assistance
Tissue Diagnosis
Biopsy Indications:
- Atypical presentation
- Negative Mantoux/IGRA
- MDR-TB suspected
- Exclude malignancy
- Failed empirical treatment
Methods:
- CT-guided percutaneous biopsy
- Open surgical biopsy
- Abscess aspiration
Histopathology:
- Caseous necrosis
- Epithelioid granulomas
- Langhans giant cells
- AFB staining
- PCR (GeneXpert)
Differential Diagnosis
Differential Diagnosis of a Destructive Vertebral Lesion
| Diagnosis | Discriminating features | Key test |
|---|---|---|
| Spinal TB | Insidious, subligamentous spread, disc relatively spared early, thin-walled cold abscess, calcification | Biopsy: caseating granuloma, Xpert/culture |
| Pyogenic spondylodiscitis | Acute, high fever, early disc destruction, thick irregular abscess wall | Blood cultures, biopsy culture |
| Brucellar spondylitis | Endemic / livestock contact, lower lumbar, gas in disc, little deformity | Serology, blood culture |
| Metastasis / myeloma | Older, disc characteristically spared, posterior element / pedicle destruction, no abscess | MRI, biopsy, serum electrophoresis |
| Fungal spondylitis | Immunocompromised, indolent, can mimic TB | Biopsy fungal stain/culture |
A key trap is that metastatic disease and myeloma also spare the disc, so disc preservation alone does not confirm infection; the presence of a paravertebral cold abscess and subligamentous spread points to TB, whereas pedicle destruction without abscess favours malignancy.
Management
Antitubercular Therapy (ATT)
Standard Regimen (WHO):
| Phase | Duration | Drugs |
|---|---|---|
| Intensive | 2 months | HRZE (4 drugs) |
| Continuation | 4-10 months | HR (2 drugs) |
Drug Dosages:
- H (Isoniazid): 5 mg/kg (max 300 mg)
- R (Rifampicin): 10 mg/kg (max 600 mg)
- Z (Pyrazinamide): 25 mg/kg (max 2 g)
- E (Ethambutol): 15 mg/kg (max 1.2 g)
Duration Controversy:
- WHO endorses a 6-month regimen for drug-susceptible disease, supported by the MRC ambulant-chemotherapy RCT, in which 6 months of isoniazid plus rifampicin gave a 94% favourable outcome at 10 years
- CNS/spinal-focused guidance (e.g. British Infection Society) recommends 12 months: 2 months of four drugs then at least 10 months of isoniazid and rifampicin
- Many spinal units extend to 9-12 months in extensive or slow-responding disease
- Drug-resistant disease requires substantially longer, specialist-directed regimens
Monitoring:
- Baseline: LFTs, uric acid, visual acuity
- Monthly: LFTs during intensive phase
- Clinical response assessment
- Radiological healing (MRI at 6 months)
- ESR trending
Drug-Resistant TB:
- MDR-TB requires specialist management
- Second-line drugs (fluoroquinolones, injectables)
- Extended duration (18-24 months)
- Specialist input essential
Hepatotoxicity Risk
Monitor LFTs closely during ATT. Risk factors for hepatotoxicity include age more than 35, pre-existing liver disease, alcohol use, and concurrent hepatotoxic medications. Stop ATT if ALT rises more than 5x ULN or symptoms develop.
Medical therapy alone achieves good outcomes in 85-90% of cases when neurological deficit is not severe.
Complications
Disease-Related Complications
| Complication | Incidence | Management |
|---|---|---|
| Kyphosis | 30-50% | Surgical correction if severe |
| Paraplegia | 20-30% | Decompression ± steroids |
| Cold abscess | 20-30% | Drainage if large |
| Sinus formation | 5-10% | Debridement, prolonged ATT |
| Spinal instability | Variable | Instrumented fusion |
Neurological Complications
Pott's Paraplegia:
- Early onset (active disease): Better prognosis
- Late onset (healed disease): Worse prognosis
- Causes: Abscess, granulation tissue, bony compression
Prognosis Factors:
- Duration of deficit (shorter = better)
- Completeness (incomplete = better)
- Age (younger = better)
- Vertebral destruction extent
Treatment-Related Complications
Medical:
- Hepatotoxicity (2-10%)
- Drug reactions
- Drug interactions
- MDR development
Surgical:
- Infection
- Neurological injury
- Hardware failure
- Pseudarthrosis
- Recurrence
Long-Term Sequelae
- Residual kyphosis
- Chronic pain
- Residual neurological deficit
- Adjacent segment disease
- Growth disturbance (paediatric)
Kyphosis Prevention
Early recognition and appropriate treatment can prevent severe kyphosis. Children are at higher risk of progressive deformity. Consider early surgery in children with significant vertebral destruction to prevent late kyphotic deformity.
Outcomes and Prognosis
Neurological Recovery
Prognosis by Presentation:
| Presentation | Recovery Rate | Timeframe |
|---|---|---|
| Early/mild deficit | 70-80% | 3-6 months |
| Moderate deficit | 50-70% | 6-12 months |
| Complete paraplegia | 20-30% | Variable |
Favourable Factors:
- Short duration of deficit
- Incomplete paraplegia
- Younger age
- Compression by soft tissue (not bone)
- Early treatment initiation
Treatment Outcomes
Medical Treatment Alone:
- Success rate: 85-90%
- Healing time: 6-12 months
- Residual kyphosis: 30-50%
Combined Medical + Surgical:
- Neurological improvement: 70-90%
- Fusion rate: 90-95%
- Deformity correction maintained
Long-Term Prognosis
Factors Affecting Outcome:
- Extent of initial disease
- Timing of treatment
- Adequacy of ATT
- Surgical technique
- Patient compliance
Return to Activity:
- Light activities: 3-6 months
- Full activities: 6-12 months
- Depends on neurological status
Outcome Summary
With appropriate treatment, most patients with spinal TB achieve good outcomes. Medical treatment alone is sufficient in 85-90%. Neurological recovery is expected in 70-80% of those with incomplete deficits. Surgery improves outcomes in selected cases with specific indications.
Evidence and Guidelines
MRC Trial: Ambulant Chemotherapy vs Radical Surgery (10-Year Report)
- Randomised trial of 235 patients without paraplegia, three arms: radical anterior resection + 6 months HR (Rad6), ambulant 6 months HR (Amb6), ambulant 9 months HR (Amb9)
- At 10 years a favourable outcome was reached in 90% (Rad6), 94% (Amb6) and 99% (Amb9)
- Ambulant 6-month isoniazid plus rifampicin was effective for spinal TB without paraplegia
- Exception: children under 15 with an initial kyphosis angle over 30 degrees, in whom kyphosis increased substantially
Comprehensive Review for the Modern Spine Surgeon
- Skeletal TB affects roughly 10% of those with active disease; infection begins in the anterior vertebral body
- Tissue diagnosis (culture, histology, PCR) is the gold standard for confirmation
- Multidrug chemotherapy is the cornerstone of management and can be curative with minimal residual kyphosis
- Surgery is reserved for neurological deficit or severe kyphosis: debridement, deformity correction and stable fusion
MRI Features Differentiating Tuberculous from Pyogenic Spondylitis (Meta-analysis)
- 32 studies pooled; subligamentous spread far more common in TB (93% vs 24%)
- Thin and regular abscess wall favours TB (94% vs 18%); epidural extension also favours TB (77% vs 25%)
- Vertebral collapse (68% vs 24%) and kyphosis (39% vs 3%) favour TB
- Disc signal change (82% vs 95%) and disc height loss (22% vs 59%) favour pyogenic infection
Xpert MTB/RIF on Bone Specimens for Spinal TB
- Prospective study of 106 patients with suspected spinal TB using a composite reference standard
- Xpert MTB/RIF alone: sensitivity 63.3% against the composite standard, with high specificity
- Combining Xpert with histopathology raised pooled sensitivity to 95% and specificity to 97.8%
- Xpert simultaneously detects rifampicin resistance, aiding rapid identification of MDR disease
Prediction of Final Gibbus Deformity (Rajasekaran Formula)
- 90 patients with thoracic and thoracolumbar lesions followed for 6 years
- Initial vertebral body loss correlated strongly with final gibbus angle (correlation coefficient 0.83)
- Final kyphosis was predictable with about 90% accuracy in non-operatively treated patients
- Allows selection of patients who need radical resection and grafting to prevent severe kyphosis
Single-Stage Anterior Decompression with Posterior Instrumentation
- 38 patients with panvertebral disease, deficit or severe kyphosis treated via an anterolateral extrapleural approach
- Single-stage anterior decompression, posterior instrumentation and circumferential grafting avoided staged surgery
- Mean kyphosis corrected by 25 degrees in those operated for deformity
- All but one patient with a neurological deficit recovered complete motor and sensory function
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Classic Pott's Disease Presentation
"A 35-year-old man from India presents with 4 months of progressive back pain, night sweats, and weight loss. He has low-grade fever and difficulty walking due to leg weakness. MRI shows T11-12 vertebral destruction with anterior soft tissue collection."
Spinal TB vs Pyogenic Infection
"A 50-year-old man presents with back pain and low-grade fever. MRI shows L3-4 vertebral body involvement with disc changes and paravertebral collection. Both TB and pyogenic infection are being considered."
Pott's Paraplegia Management
"A 28-year-old woman presents with complete paraplegia of 2 weeks duration. MRI shows T7-8 vertebral destruction with large epidural collection causing severe cord compression. She has confirmed pulmonary TB on sputum."
MCQ Practice Points
Most Common Location
Q: What is the most common location for spinal tuberculosis?
A: The thoracolumbar junction (T10-L2) is the most common site for spinal TB. The thoracic spine is involved in approximately 50% of cases, lumbar in 35%, and cervical in 15%. The paradiscal region is the most common pattern of involvement.
Disc Preservation
Q: Which feature distinguishes spinal TB from pyogenic spondylitis?
A: Early disc preservation distinguishes TB from pyogenic infection. In pyogenic spondylitis, the disc is destroyed early as bacteria can survive in disc tissue. In TB, the avascular disc is relatively resistant to mycobacterial infection, though late TB can involve the disc.
Imaging Discriminators
Q: Which MRI features best distinguish tuberculous from pyogenic spondylitis?
A: A pooled meta-analysis found subligamentous spread (93% vs 24%), a thin, smooth-walled abscess (94% vs 18%) and epidural extension (77% vs 25%) favour TB, whereas disc signal change and disc height loss are more common in pyogenic infection. MRI is the modality of choice because it detects disease far earlier than plain films, which become positive only once substantial trabecular bone is destroyed.
Skip Lesions
Q: What percentage of spinal TB patients have skip lesions?
A: 10-15% of patients have skip lesions (non-contiguous vertebral involvement). This is why whole spine imaging with MRI is recommended in all suspected cases of spinal TB to detect all levels of involvement.
Treatment Response
Q: What percentage of patients with uncomplicated spinal TB respond to medical treatment alone?
A: 85-90% of patients with uncomplicated spinal TB respond to antitubercular therapy alone without surgery. Surgery is reserved for specific indications including progressive neurology, instability, and failure of medical treatment.
Guidelines, Registries & Global Practice
Global Epidemiology
Tuberculosis remains a leading infectious cause of death worldwide, with around 1.3 million deaths annually. Spinal TB is the most common musculoskeletal manifestation, affecting roughly 1 to 2% of all cases of TB, and skeletal involvement occurs in approximately 10% of those with active disease. Burden is concentrated in South and South-East Asia, Sub-Saharan Africa and the Western Pacific. In low-incidence high-income settings, the overwhelming majority of cases are in people born in high-burden countries, frequently presenting as reactivation of latent infection years after migration. HIV co-infection, which is endemic in parts of Sub-Saharan Africa, adds substantially to both the burden and complexity of management.
Major Guidance Side-by-Side
Drug Regimen and Surgical Triggers Across Guidance
| Body / Evidence | Drug regimen | Surgical trigger |
|---|---|---|
| WHO (drug-susceptible TB) | 2 months HRZE then 4 months HR (6 months total) | Not a surgical body; medical cure expected in uncomplicated disease |
| British Infection Society (CNS / spinal TB) | 4 drugs for 2 months then isoniazid + rifampicin for at least 10 months (12 months total) | Decompression for cord compression with deficit |
| MRC Working Party RCT evidence | Ambulant 6-9 months HR adequate without paraplegia | Routine radical surgery confers no healing benefit in uncomplicated disease |
| AO Spine / contemporary surgical reviews | Chemotherapy continued through and after surgery | Deficit, instability, severe / progressive kyphosis, failed medical therapy, diagnostic doubt |
The most important guideline divergence to recognise is duration: WHO endorses a 6-month regimen for drug-susceptible disease (supported by the MRC ambulant-chemotherapy RCT), whereas neurological/CNS-focused guidance such as the British Infection Society recommends a longer 12-month course (2 months of four drugs then at least 10 months of isoniazid and rifampicin) for spinal and CNS disease. Many spinal units extend treatment to 9-12 months in extensive or slow-responding disease.
Diagnostic Standards
A tissue diagnosis (culture, histology and nucleic-acid amplification) is the worldwide gold standard before committing a patient to prolonged therapy, and is especially important in low-prevalence settings and to detect drug resistance. Xpert MTB/RIF on bone or abscess material gives rapid results and simultaneously reports rifampicin resistance, but its sensitivity on bone is only moderate when used alone, so it should be paired with histopathology and culture rather than replacing them.
Practice Variation by Resource Setting
| Setting | Diagnosis | Surgery |
|---|---|---|
| High-resource, low-incidence | MRI plus image-guided biopsy with Xpert and culture; drug-susceptibility testing routine | Instrumented single- or two-stage reconstruction; titanium implants |
| High-burden, limited-resource | Often clinical/radiographic diagnosis; empirical ATT where confirmation is impractical | Middle-path regimen; surgery rationed to deficit and major deformity |
In resource-limited high-burden regions, empirical antitubercular therapy on clinical and radiographic grounds is common where biopsy is impractical, and a conservative "middle-path" approach (chemotherapy with selective surgery) predominates. In low-incidence settings, mandatory public-health notification, contact tracing, directly observed therapy for adherence, and multidisciplinary input from infectious diseases, spinal surgery, radiology and rehabilitation are standard.
SPINAL TUBERCULOSIS (POTT'S DISEASE)
Clinical summary
Key Facts
- •50% of skeletal TB is spinal
- •T10-L2 most common location
- •Paradiscal type most common (50-75%)
- •Skip lesions in 10-15% - image whole spine
TB vs Pyogenic
- •TB: Insidious onset, low-grade fever, disc spared early
- •Pyogenic: Acute onset, high fever, early disc destruction
- •TB: Thin smooth abscess wall, calcification
- •Pyogenic: Thick irregular wall, no calcification
Imaging
- •MRI gold standard: 96% sensitivity, 93% specificity
- •Changes visible on MRI in 3-5 days
- •X-ray: positive only when 50% bone destroyed (4-6 months)
- •Always image whole spine for skip lesions
Management
- •Medical first: 85-90% respond to ATT alone
- •ATT: HRZE 2 months, then HR 4-10 months
- •Surgery: progressive neurology, instability, large abscess
- •Combined approach for complex cases
Surgical Indications (SURGERY)
- •Severe kyphosis (more than 40-50 degrees)
- •Unstable spine
- •Resistant (MDR) TB
- •Granulation tissue compressing cord
- •Extensive abscess
- •Regressing neurology despite ATT