INI1/SMARCB1-Deficient Soft Tissue Sarcoma | The Great Mimic | Distal Upper Limb of Young Adults
- Most common soft tissue sarcoma of the hand and distal forearm in young adults - the classic exam trap
- Loss of nuclear INI1 (SMARCB1) on immunohistochemistry is present in over 90% and is the key diagnostic clue
- Notorious mimic of benign disease (granuloma, abscess, Dupuytren nodule, wart, ulcer) causing long diagnostic delay
- Spreads by three routes: local recurrence, regional lymph nodes (unusual for a sarcoma), and lung
- Treatment is wide excision with negative margins plus radiotherapy; tazemetostat (EZH2 inhibitor) is an option in advanced disease
- “A non-healing ulcer or firm nodule on the hand or forearm of a young adult is epithelioid sarcoma until proven otherwise
- “Unlike most sarcomas, regional lymph node metastasis is a recognised pattern - examine and image the nodes
- “INI1 loss is shared with malignant rhabdoid tumour and epithelioid MPNST, so correlate with morphology and clinical context
- “Late local and distant recurrence is common - this tumour needs prolonged surveillance, not just 5 years
A persistent nodule or non-healing ulcer on the hand/forearm of a young adult is epithelioid sarcoma until proven otherwise. It is repeatedly misdiagnosed as a granuloma, abscess, wart, Dupuytren nodule or chronic ulcer, causing dangerous delay. Biopsy any unexplained persistent lesion.
Loss of nuclear INI1 (SMARCB1) is present in over 90% and is the single most useful diagnostic marker. It is shared with malignant rhabdoid tumour and epithelioid MPNST, so it confirms the family but morphology and context define the diagnosis.
Local recurrence, lymph node and lung. Unlike most soft tissue sarcomas, regional nodal metastasis is a recognised route of spread. Always examine and stage the draining nodes; do not assume sarcomas never go to nodes.
Distal (classic) type affects young adults in the distal limb; proximal (large-cell) type affects older patients in the pelvis/perineum, shows rhabdoid cells, and behaves more aggressively with earlier metastasis.
MIMICKEREpithelioid Sarcoma Key Features
Hook:Epithelioid sarcoma is the great MIMICKER of the hand - benign-looking but lethal.
DAPDistal vs Proximal Variant
Hook:DAP - Distal is classic, Aggressive Proximal type is worse.
LNLRoutes of Spread and Adverse Factors
Hook:LNL - the three exits for epithelioid sarcoma: Local, Nodes, Lung.
Overview and Epidemiology
Epithelioid sarcoma is a rare malignant soft tissue tumour of uncertain differentiation. It is best known as the most common soft tissue sarcoma of the hand and distal forearm in young adults, and as a notorious mimic of benign disease. According to PubMed, the World Health Organization now classifies it as an INI1 (SMARCB1)-deficient tumour, reflecting the loss of nuclear INI1 expression seen in the large majority of cases.
Epithelioid sarcoma is repeatedly mistaken for benign conditions - a granuloma, a chronic abscess, a wart, a Dupuytren nodule or a non-healing ulcer. Because it grows slowly and looks unremarkable, patients are often treated for benign disease for months to years. Any persistent, firm, or ulcerating lesion of the distal limb in a young adult must be biopsied rather than observed.
- Frequency: Under 1% of all soft tissue sarcomas (very rare)
- Age: Distal (classic) type typically 20-40 years; proximal type tends to be older
- Sex: Male predominance in most series
- Distal type: A leading soft tissue sarcoma of the hand and forearm in young adults
- Distal upper limb: Hand, fingers, forearm (classic type)
- Distal lower limb: Foot, ankle, lower leg
- Proximal/axial: Pelvis, perineum, genitalia, buttock (proximal type)
- Often superficial: Dermal or subcutaneous, tracking along fascia and tendon
Distal versus Proximal Type
According to PubMed, Guillou and colleagues defined the proximal-type variant as a distinctive, more aggressive neoplasm showing rhabdoid features, which contrasts with the conventional distal type.
- Distal (classic) type
- Young adults (20-40 years)
- Proximal (large-cell) type
- Older adults (often over 40)
- Distal (classic) type
- Hand, fingers, forearm, foot
- Proximal (large-cell) type
- Pelvis, perineum, genitalia, buttock, deep proximal soft tissue
- Distal (classic) type
- Nodular, granuloma-like with central necrosis
- Proximal (large-cell) type
- Sheets of large rhabdoid/epithelioid cells, multinodular
- Distal (classic) type
- Bland to moderately atypical epithelioid and spindle cells
- Proximal (large-cell) type
- Marked atypia, prominent rhabdoid cells
- Distal (classic) type
- Slow but relentless; high local recurrence
- Proximal (large-cell) type
- More aggressive; earlier and more frequent metastasis
Pathophysiology and Histology
Cellular Origin and the SWI/SNF Complex
Epithelioid sarcoma is a tumour of uncertain differentiation that shows partial epithelial differentiation (it co-expresses keratins and the mesenchymal marker vimentin). The defining molecular event is loss of function of SMARCB1 (INI1), a core subunit of the SWI/SNF chromatin-remodelling complex that normally acts as a tumour suppressor.
The molecular hallmark:
- SMARCB1 (also called INI1, SNF5, BAF47) is a core SWI/SNF subunit
- Biallelic inactivation leads to loss of nuclear INI1 protein
- Demonstrable as loss of nuclear staining on immunohistochemistry in over 90%
- The same loss occurs in malignant rhabdoid tumour and a subset of epithelioid MPNST
Why the loss is targetable:
- SMARCB1 loss removes the normal antagonism of EZH2
- The tumour becomes oncogenically dependent on EZH2 (a transcriptional repressor)
- This is the rationale for the EZH2 inhibitor tazemetostat
- A minority of cases retain INI1, where other SWI/SNF subunits may be abnormal
Loss of nuclear INI1 strongly supports epithelioid sarcoma in the right context, but it is not unique to it. Malignant rhabdoid tumour, epithelioid MPNST and a few carcinomas also show INI1 loss. Diagnosis therefore rests on the combination of clinical setting, morphology (epithelioid and rhabdoid cells), keratin/EMA and CD34 co-expression, and INI1 loss together.
Histological Pattern
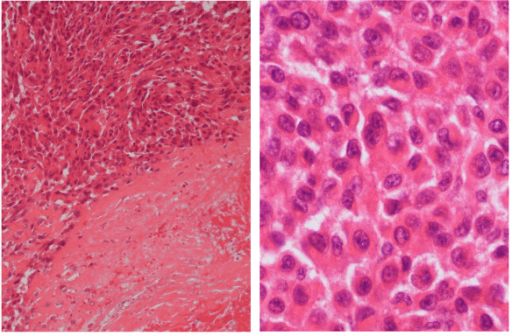
Distal (Classic) Type Histology
Nodular, granuloma-like architecture is the classic appearance.
- Nodules of tumour cells with central necrosis
- Resembles a necrotising granuloma at low power (a key trap)
- Cells track along fascia, tendon sheaths and dermis
- Slow infiltrative spread explains high recurrence
- Mixture of epithelioid and spindle cells
- Eosinophilic cytoplasm, relatively bland to moderate atypia
- Transition between epithelioid and spindled forms
- Mitoses present but may be inconspicuous
The nodules with central necrosis can be mistaken for a necrotising granuloma (for example, a rheumatoid nodule or infection). A young adult with a firm hand nodule reported as granulomatous inflammation deserves a second look with INI1 immunohistochemistry.
Differential Diagnosis
- Overlapping Features
- Nodular pattern with central necrosis
- Key Discriminator
- No cytological atypia, no keratin/CD34, INI1 retained
- Overlapping Features
- Keratin and EMA positive, epithelioid cells
- Key Discriminator
- Carcinomas are usually CD34 negative and retain INI1
- Overlapping Features
- Rhabdoid cells, INI1 loss
- Key Discriminator
- Younger children, deep/axial, no granuloma-like pattern
- Overlapping Features
- Epithelioid cells, can lose INI1
- Key Discriminator
- Arises from nerve/neurofibromatosis, S100 often positive
- Overlapping Features
- Epithelioid cells, atypia
- Key Discriminator
- S100, SOX10 and melanocytic markers positive; INI1 retained
- Overlapping Features
- Epithelioid cells, can express keratin
- Key Discriminator
- Vascular markers (CD31, ERG) positive; INI1 retained
Clinical Presentation
History
- Firm, painless nodule in skin or subcutis (most common)
- Non-healing ulcer over a nodule (classic and often misleading)
- Distal upper limb in young adults (hand, fingers, forearm)
- Slowly enlarging, sometimes multiple satellite nodules
- Long symptom duration before diagnosis (months to years)
- Previously "treated" as wart, abscess, granuloma or Dupuytren disease
- Recurrence after presumed benign excision
- Palpable regional lymph nodes (a warning of nodal spread)
Marginal or piecemeal excision of an unsuspected epithelioid sarcoma is a disaster - it leaves contaminated tissue, seeds the field, and compromises later limb-salvage surgery. Any indeterminate persistent hand or forearm lesion should be imaged and biopsied with a planned tract before any excision is contemplated.
Physical Examination
Examination Approach
- Skin nodule(s), ulceration or scar from prior excision
- Site (distal limb favours classic type)
- Satellite lesions along lymphatics or fascia
- Firm to hard consistency, fixed to deep tissue if infiltrative
- Tenderness usually mild
- Relationship to tendons and neurovascular structures
- Always examine the draining lymph nodes (epitrochlear, axillary, inguinal)
- Nodal metastasis is a recognised pattern in this tumour
- Document any palpable nodes for staging and biopsy
- Neurovascular status distal to the mass
- Joint range of movement and hand function
- Baseline function for reconstruction planning
Investigations and Imaging
Imaging Protocol
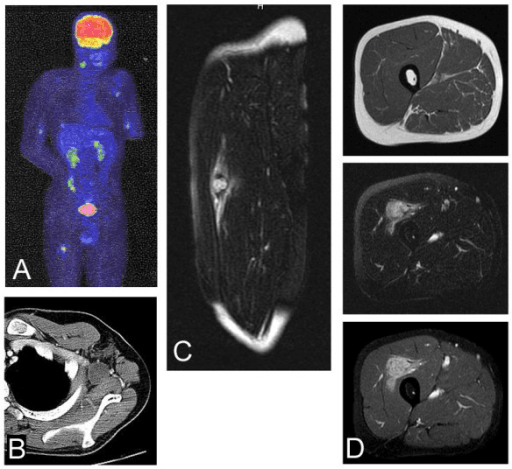
MRI (Local Staging)
MRI of the whole compartment is the standard for local staging of any suspected soft tissue sarcoma.
- T1: anatomical detail, tumour extent, relation to tendons and neurovascular bundle
- T2 with fat suppression: usually intermediate to high signal, heterogeneous
- Post-contrast: heterogeneous enhancement, may show nodular/multifocal pattern
- Look for satellite nodules and tracking along fascia - a clue to infiltrative spread
MRI also guides a safe biopsy tract and the eventual resection plan.
Biopsy and Diagnosis
Core needle biopsy at (or after discussion with) a specialist sarcoma centre is the standard.
- Plan the biopsy tract so it can be excised en bloc at definitive surgery
- Use a longitudinal approach on the limb; avoid transverse incisions
- Provide adequate tissue for morphology and immunohistochemistry (including INI1)
- Request INI1/SMARCB1 staining when epithelioid sarcoma is considered
- Never perform an unplanned marginal excision of an undiagnosed lesion
Putting the Diagnosis Together
- Epithelioid and spindle cells; nodular pattern with necrosis (distal type)
- Large rhabdoid cells in sheets (proximal type)
- Keratin/EMA positive, vimentin positive, CD34 positive in around half
- INI1 (SMARCB1) lost in over 90%
- S100 negative (helps exclude melanoma and nerve sheath tumours)
Grading and Staging
- How it is assessed
- FNCLCC grade (differentiation, mitoses, necrosis)
- Note for epithelioid sarcoma
- Many tumours are high grade, especially proximal type
- How it is assessed
- Size and depth
- Note for epithelioid sarcoma
- Often superficial but infiltrative; size is prognostic
- How it is assessed
- Regional lymph nodes
- Note for epithelioid sarcoma
- Nodal disease (N1) is a recognised pattern and upstages prognosis
- How it is assessed
- Distant disease, chiefly lung
- Note for epithelioid sarcoma
- Lung is the dominant distant site
For most soft tissue sarcomas, lymph node spread is rare and is treated as advanced disease. Epithelioid sarcoma is one of the classic exceptions (with clear cell sarcoma, rhabdomyosarcoma and angiosarcoma) where nodal metastasis genuinely occurs - so nodal assessment is part of routine staging here.
In the AJCC 8th edition staging of extremity and trunk soft tissue sarcoma, regional lymph node involvement (N1) is classified as Stage IV — node-positive disease is staged as advanced disease, the same category as distant metastasis. That is why nodal status is decisive in epithelioid sarcoma. The handful of sarcomas that genuinely metastasise to nodes are worth memorising as a group (mnemonic "CARE"): Clear cell sarcoma, Angiosarcoma (including epithelioid variants), Rhabdomyosarcoma, Epithelioid sarcoma — with synovial sarcoma sometimes added. For all of these, nodal examination and imaging are an explicit part of staging, unlike the great majority of soft tissue sarcomas in which nodes are rarely involved.
Because epithelioid sarcoma spreads to nodes, the natural question is whether the clinically and radiologically node-negative patient should have a sentinel lymph node biopsy (SLNB). SLNB is technically feasible and has been studied in the node-metastasising sarcomas (epithelioid and clear cell sarcoma, rhabdomyosarcoma), and it does identify occult nodal disease in a proportion of patients. However, the evidence that it improves survival is weak, it is not part of routine soft-tissue-sarcoma staging, and major guidelines (ESMO, NCCN) do not mandate it. The pragmatic position is meticulous clinical and cross-sectional nodal staging for every patient, biopsy of any suspicious node, and SLNB considered only selectively (often within a sarcoma centre or trial). Confirmed nodal disease is then managed with therapeutic dissection rather than routine elective node clearance.
Management
Core Principles
Complete surgical removal with negative margins offers the best chance of cure. Because epithelioid sarcoma infiltrates and recurs locally, wide excision is preferred and radiotherapy is added for most deep, large or marginally resected tumours. Systemic therapy is reserved largely for advanced or metastatic disease.
Treatment fundamentals:
- Surgery: Wide local excision with negative margins (the priority)
- Radiotherapy: Adjuvant for high-risk features or close/positive margins
- Nodal disease: Biopsy-proven nodes managed with regional node dissection at a sarcoma centre
- Systemic therapy: For unresectable, metastatic or relapsed disease
Systemic Therapy and the EZH2 Target
According to PubMed, the dependence of INI1-deficient epithelioid sarcoma on EZH2 has been translated into a licensed targeted therapy. The EZH2 inhibitor tazemetostat produced durable responses in advanced INI1-negative epithelioid sarcoma in an international phase 2 basket study and was well tolerated, leading to regulatory approval for advanced disease not amenable to complete resection. Conventional anthracycline-based chemotherapy is also used, but response rates are modest.
Complications and Surveillance
Patterns of Failure
- Frequency / Pattern
- Common, often repeated
- Drivers
- Infiltrative growth, marginal excision, satellite nodules
- Management
- Re-excision with wider margins; amputation if limb salvage fails
- Frequency / Pattern
- Recognised pattern (unusual for a sarcoma)
- Drivers
- Aggressive biology, proximal type, high grade
- Management
- Node biopsy and therapeutic dissection; adjuvant therapy
- Frequency / Pattern
- Dominant distant site
- Drivers
- High-risk and proximal-type tumours
- Management
- Systemic therapy; metastasectomy in selected oligometastatic cases
- Frequency / Pattern
- May occur years after treatment
- Drivers
- Indolent component of tumour biology
- Management
- Prolonged surveillance beyond the usual 5 years
Surveillance Principle
Surveillance must include the regional nodal basin (clinical and imaging) as well as the local site and the chest, because of the triple spread pattern. Late recurrences mean follow-up should continue well beyond five years.
Prognosis and Outcomes
According to PubMed, multi-institutional and tertiary-centre series consistently show that nodal and distant metastasis are the strongest adverse prognostic factors, and that the proximal type carries a worse outcome than the classic distal type.
- Favourable
- Distal (classic) type
- Unfavourable
- Proximal (large-cell) type
- Favourable
- Node negative (N0)
- Unfavourable
- Node positive (N1)
- Favourable
- No metastases
- Unfavourable
- Metastatic (M1)
- Favourable
- Wide negative margin
- Unfavourable
- Marginal/positive margin
- Favourable
- Superficial, small
- Unfavourable
- Deep, large
- Favourable
- Lower grade
- Unfavourable
- High grade with rhabdoid cells
Across series, lymph node or distant metastasis has the most critical impact on survival, and proximal-type disease behaves more aggressively with earlier metastasis and poorer overall survival than the classic distal type.
Guidelines, Registries & Global Practice
Global Epidemiology
- Rarity: Under 1% of all soft tissue sarcomas worldwide
- Age: Distal type peaks in young adults; proximal type tends to be older
- Sex: Male predominance in most reported series
- Distal type: A leading hand and forearm soft tissue sarcoma in young adults
- Triple spread: Local recurrence, regional nodes and lung
- Nodal metastasis: Reported in roughly a third of localized cases in tertiary series
- Late relapse: Disease-specific survival falls substantially between 5 and 10 years
- Variant matters: Proximal type carries worse outcomes than distal type
Side-by-Side Principles from Major Sarcoma Frameworks
- Diagnosis
- Refer to a sarcoma centre before biopsy; confirm INI1 loss
- Local Treatment
- Wide excision with radiotherapy for deep/larger tumours; assess nodes
- Systemic / Advanced Disease
- Anthracycline-based chemotherapy; targeted EZH2 inhibition for INI1-deficient disease
- Diagnosis
- Image-guided core biopsy at a sarcoma centre; INI1 testing
- Local Treatment
- Limb-sparing wide excision plus radiotherapy; re-excision for positive margins
- Systemic / Advanced Disease
- Tazemetostat is an option for advanced INI1-deficient epithelioid sarcoma
- Diagnosis
- Mandatory specialist sarcoma MDT before definitive treatment
- Local Treatment
- Centralized surgery and radiotherapy at designated centres
- Systemic / Advanced Disease
- Systemic therapy and trials for advanced disease at specialist centres
Every major framework agrees: any persistent or enlarging deep/atypical soft tissue lesion should be referred to a specialist sarcoma centre before biopsy, diagnosis should include INI1/SMARCB1 testing, and definitive management should be planned by a multidisciplinary sarcoma team. For epithelioid sarcoma specifically, nodal assessment is an explicit part of staging.
High- vs Limited-Resource Practice Variation
- Routine INI1 immunohistochemistry and molecular confirmation
- Centralized sarcoma MDTs with limb-salvage surgery and reconstruction
- MRI staging, CT chest and FDG-PET access
- Availability of tazemetostat for advanced INI1-deficient disease
- Diagnosis may rely on morphology and a limited immunopanel; INI1 not always available
- Later presentation with larger tumours and higher amputation rates
- Restricted radiotherapy and targeted-therapy access
- Telepathology and regional referral networks help bridge expertise gaps
Applicable in any health system:
- Document a clear investigation pathway for any persistent distal-limb nodule or non-healing ulcer (the common delayed-diagnosis pitfall)
- Confirm pre-biopsy staging and that biopsy was planned with the definitive surgeon
- Record that INI1/SMARCB1 testing and nodal assessment were performed
- Evidence of sarcoma MDT discussion before definitive treatment
- Informed consent covering wide excision, possible amputation, radiotherapy and recurrence/metastatic risk
- A written long-term surveillance plan that extends beyond 5 years given late relapse
MCQ Practice Points
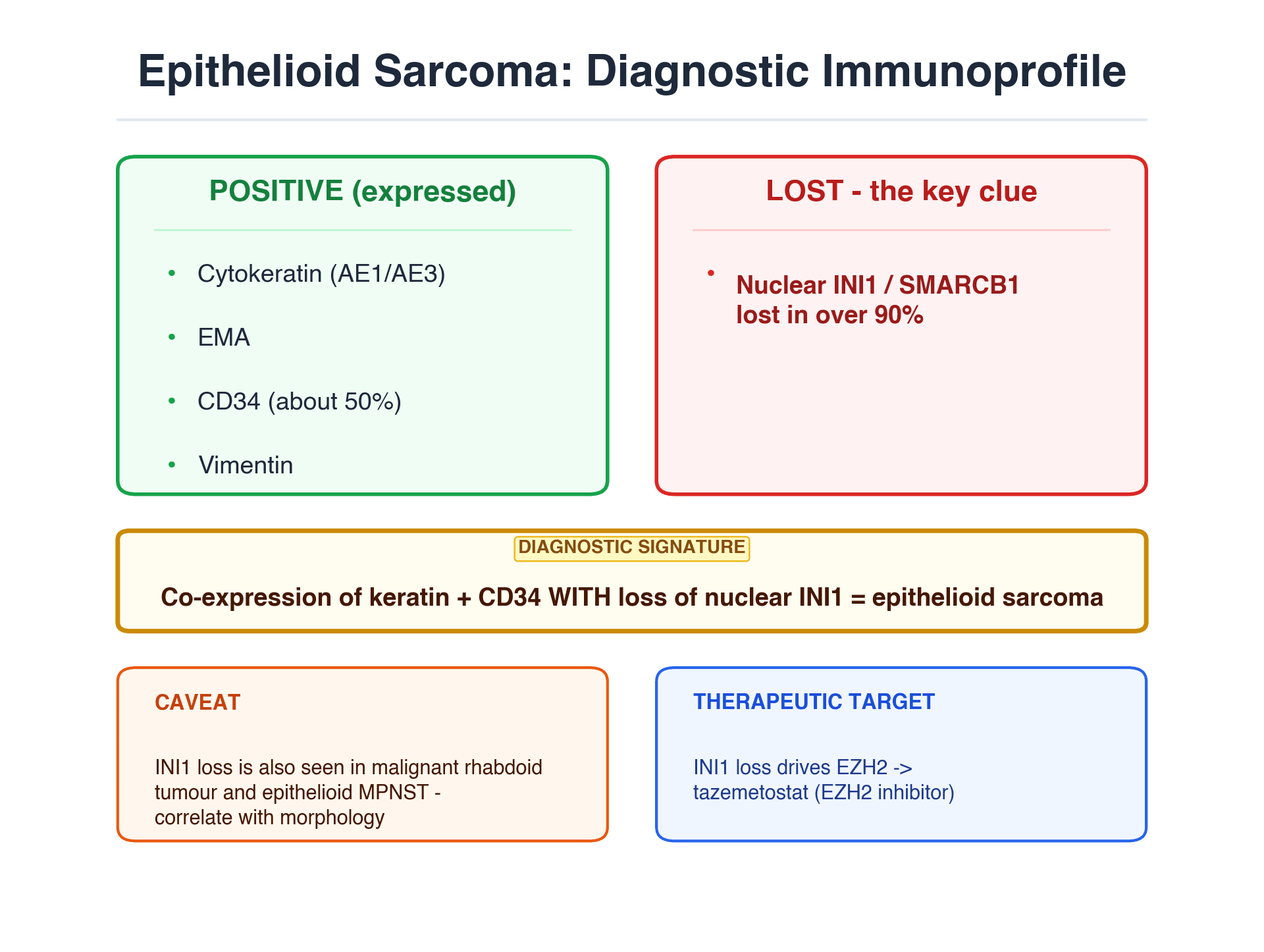
Q: What is the characteristic immunohistochemical finding in epithelioid sarcoma? A: Loss of nuclear INI1 (SMARCB1) in over 90% of cases, together with co-expression of cytokeratin/EMA and CD34. CD34 positivity helps distinguish it from carcinoma, which is usually CD34 negative. INI1 loss is shared with malignant rhabdoid tumour and epithelioid MPNST.
Q: What is the most common soft tissue sarcoma of the hand and distal forearm in a young adult? A: Epithelioid sarcoma (distal/classic type). It is the great mimic, often misdiagnosed as a granuloma, abscess, wart or non-healing ulcer, leading to long diagnostic delay.
Q: How does the metastatic pattern of epithelioid sarcoma differ from most soft tissue sarcomas? A: It shows a triple pattern - local recurrence, regional lymph nodes, and lung. Nodal spread is unusual for sarcomas but a recognised feature here, so nodal staging is part of routine workup.
Q: Which targeted agent is approved for advanced INI1-deficient epithelioid sarcoma and why? A: Tazemetostat, an EZH2 inhibitor. Loss of SMARCB1 makes the tumour oncogenically dependent on EZH2, and a phase 2 basket study showed durable responses with good tolerability in advanced disease.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 26-year-old man is referred with a firm 2 cm nodule on the volar aspect of his forearm that has been present for over a year. It was treated as a wart and then a chronic abscess. There is now superficial ulceration. How do you approach this?”
“A 48-year-old woman has a biopsy-proven epithelioid sarcoma of the buttock and perineal region, 9 cm, deep, with rhabdoid cells and loss of INI1. She has a palpable, firm inguinal lymph node. How do you manage her?”
“A 31-year-old man had a finger nodule excised elsewhere and the histology now reports epithelioid sarcoma with positive margins. He has re-presented six months later with new nodules near the scar. How do you proceed?”
Key Epidemiology
- Under 1% of all soft tissue sarcomas - very rare
- Most common soft tissue sarcoma of the hand and distal forearm in young adults (distal type)
- Male predominance; distal type peaks 20-40 years, proximal type older
- The great mimic - often misdiagnosed as granuloma, abscess, wart or non-healing ulcer
Two Variants
- Distal (classic): young adults, hand/forearm, nodular granuloma-like pattern with necrosis
- Proximal (large-cell): older patients, pelvis/perineum/genitalia, rhabdoid cells, more aggressive
- Proximal type metastasises earlier and has worse prognosis
Pathology and Diagnosis
- Loss of nuclear INI1 (SMARCB1) in over 90% - key diagnostic clue
- Co-expression of cytokeratin/EMA and vimentin; CD34 positive in around half
- CD34 positivity helps distinguish from carcinoma (usually CD34 negative)
- INI1 loss is shared with malignant rhabdoid tumour and epithelioid MPNST - correlate with context
Spread and Staging
- Triple pattern: local recurrence, regional lymph nodes, and lung
- Nodal metastasis is unusual for a sarcoma but a recognised feature here - stage the nodes
- MRI of the compartment for local staging; CT chest for lung; FDG-PET in selected cases
- Nodal (N1) and distant (M1) disease are the strongest adverse prognostic factors
Treatment
- Wide local excision with negative margins is the backbone of cure
- Adjuvant radiotherapy for deep/large tumours or close/positive margins
- Therapeutic lymph node dissection for biopsy-proven nodal disease
- Tazemetostat (EZH2 inhibitor) for advanced INI1-deficient disease; anthracycline chemotherapy an alternative
- Avoid unplanned marginal excision - it drives recurrence and compromises limb salvage
Prognosis and Surveillance
- Outcome driven by nodal/distant spread and by variant (proximal worse than distal)
- High local recurrence rate, often repeated
- Late relapse occurs - disease-specific survival falls further beyond 5 years
- Surveillance must cover the local site, the nodal basin and the chest, and continue beyond 5 years
Evidence Base and Key Studies
Definition of Proximal-Type Epithelioid Sarcoma
- Described 18 cases of a distinctive aggressive neoplasm with epithelioid and rhabdoid features, median age 35.5 years
- Most tumours arose in proximal/axial sites (pelvis, perineum, pubic and vulvar region, buttock)
- Cells co-expressed cytokeratin, EMA and vimentin; many were CD34 positive, defining the immunoprofile
- Follow-up showed metastatic dissemination in 6 of 14 patients leading to death in 5, supporting aggressive behaviour
Prognostic Variables in Epithelioid Sarcoma (44 Patients)
- Multi-institutional retrospective study of 44 patients (26 classic-type, 18 proximal-type)
- Overall survival at 5 years was 45% for the whole cohort
- Lymph node (N1) and distant (M1) metastasis were the strongest independent predictors of poor distant metastasis-free and overall survival
- Superficial location and N1 disease independently predicted local recurrence-free survival; proximal subtype trended to worse outcome
Clinical Behaviour and Molecular Markers (116 Patients)
- Database of 116 epithelioid sarcoma and unclassified sarcoma with epithelioid features patients treated since 1992
- Localized epithelioid sarcoma showed 22% local recurrence, 35% nodal metastasis and 41% distant metastasis rates
- Five- and ten-year disease-specific survival were 88% and 43%, underlining a propensity for late relapse
- INI1 loss was significantly more common in epithelioid sarcoma than in unclassified epithelioid sarcomas