High-risk site in distance runners and military recruits | Classify tension vs compression side | MRI when X-ray is normal | Tension side is an orthopaedic emergency
FULLERTON CLASSIFICATION
Critical Must-Knows
- Tension-side fracture is an orthopaedic emergency: the superior cortex is under tensile load and fractures here can displace rapidly, cutting off the femoral head blood supply - urgent fixation is mandatory.
- A normal plain X-ray does not exclude the diagnosis: up to half of femoral neck stress fractures are invisible on initial radiographs. If clinical suspicion is present, proceed directly to MRI.
- Know who gets this: distance runners (especially female), military recruits undergoing rapid training escalation, and individuals with low bone density from relative energy deficiency in sport (formerly called the female athlete triad).
- Compression-side fractures are not always safe: if more than 50% of the inferior cortex is involved on MRI, or if any displacement appears on follow-up imaging, surgical fixation becomes necessary.
- AVN is the feared complication: the femoral head blood supply runs along the femoral neck; a displaced fracture or an ischaemic event at this level can interrupt it permanently.
Clinical Pearls
- "The Fullerton classification divides fractures into tension (superior, high-risk) versus compression (inferior, lower-risk) side - the side determines management.
- "The classic history: a female distance runner with groin or anterior hip pain, worse on activity, with a normal plain X-ray - next step is urgent MRI.
- "Fixation options for tension-side fractures: three parallel cannulated cancellous screws (inverted triangle) or a dynamic hip screw with or without an anti-rotation screw.
- "Return to sport after compression-side non-operative treatment is typically 6 to 12 weeks; after tension-side surgical fixation, at least 4 to 6 months with radiographic union.
Clinical Imaging
Imaging findings across the spectrum
Critical Exam Points: Femoral Neck Stress Fracture
Tension Side = Emergency
A fracture on the superior (tensile) cortex of the femoral neck can displace rapidly and interrupt the blood supply to the femoral head. This is an orthopaedic emergency requiring urgent surgical fixation. It is catastrophically wrong to treat a tension-side fracture with simple rest. The examiner will probe whether you know this distinction.
MRI When X-Ray is Normal
Plain radiographs are normal in up to 50% of early femoral neck stress fractures. A normal X-ray in a runner or recruit with persistent hip or groin pain does not exclude the diagnosis. The correct next step is urgent MRI - it detects bone marrow oedema and fracture lines before any radiographic change appears.
Female Athlete Triad / RED-S
The female athlete triad - low energy availability, menstrual dysfunction, and low bone density - significantly amplifies stress fracture risk. Distance runners and gymnasts are the classic groups. Ask about menstrual irregularity, dietary restriction, and training load. The broader concept is now Relative Energy Deficiency in Sport (RED-S) and applies to male athletes too.
AVN Is the Catastrophic Complication
Avascular necrosis of the femoral head is the most feared outcome, occurring when the lateral epiphyseal vessels supplying the femoral head are disrupted by a displaced fracture or a vascular insult. Risk increases sharply with displacement and delay to treatment. Emphasise urgency at every step - delayed diagnosis, delayed MRI, and delayed fixation all increase AVN risk.
Memory aids
TENSETension-Side Danger Signs
| T | Top (superior) cortex involved Lucency on the superior femoral neck - the high-risk tension side |
| E | Emergency - do not delay Urgent surgical fixation; any wait risks displacement and AVN |
| N | Never treat non-operatively Resting a tension-side fracture without fixing it is wrong |
| S | Screws in - cannulated cancellous Three parallel cannulated screws or a dynamic hip screw |
| E | End result if missed: AVN Avascular necrosis of the femoral head - the catastrophic outcome |
| T | Top (superior) cortex involved Lucency on the superior femoral neck - the high-risk tension side | S | Screws in - cannulated cancellous Three parallel cannulated screws or a dynamic hip screw |
| E | Emergency - do not delay Urgent surgical fixation; any wait risks displacement and AVN | E | End result if missed: AVN Avascular necrosis of the femoral head - the catastrophic outcome |
| N | Never treat non-operatively Resting a tension-side fracture without fixing it is wrong |
Hook:Stay TENSE about the tension side - the superior cortex fracture is the one that kills the femoral head if you miss it.
DRAMSWho Gets Femoral Neck Stress Fractures
| D | Distance runners The most common group - especially those rapidly escalating mileage |
| R | Recruits (military) Rapid increase in repetitive loading in basic training |
| A | Athlete triad / RED-S Low energy, amenorrhoea, low bone density - amplifies all stress fracture risk |
| M | Metabolic bone disease Osteoporosis, osteomalacia, vitamin D deficiency - insufficiency fractures |
| S | Sudden training escalation Too much, too soon - the biomechanical root of all fatigue fractures |
| D | Distance runners The most common group - especially those rapidly escalating mileage | M | Metabolic bone disease Osteoporosis, osteomalacia, vitamin D deficiency - insufficiency fractures |
| R | Recruits (military) Rapid increase in repetitive loading in basic training | S | Sudden training escalation Too much, too soon - the biomechanical root of all fatigue fractures |
| A | Athlete triad / RED-S Low energy, amenorrhoea, low bone density - amplifies all stress fracture risk |
Hook:Think DRAMS when taking the history - identify which risk bucket your patient falls into and address the cause, not just the fracture.
CUFFManagement Decision Framework
| C | Compression side Inferior cortex: protected weight bearing and close MRI follow-up if less than 50% cortex |
| U | Urgent fix if tension side Superior cortex: do not delay - cannulated screws or DHS same admission |
| F | Follow-up with MRI, not X-ray Track healing with MRI; plain films lag well behind the biological response |
| F | Fix the cause - screen for triad/RED-S Address energy availability, bone health, and training load or you will see a recurrence |
| C | Compression side Inferior cortex: protected weight bearing and close MRI follow-up if less than 50% cortex | F | Follow-up with MRI, not X-ray Track healing with MRI; plain films lag well behind the biological response |
| U | Urgent fix if tension side Superior cortex: do not delay - cannulated screws or DHS same admission | F | Fix the cause - screen for triad/RED-S Address energy availability, bone health, and training load or you will see a recurrence |
Hook:Think CUFF - like the hip capsule: Compression-side conservative, Urgent fix for tension-side, Follow-up with MRI, Fix the underlying cause.
Overview
A femoral neck stress fracture is a fatigue fracture that occurs when repetitive submaximal loading overwhelms the bone's ability to remodel and repair. Unlike a traumatic fracture from a single high-energy event, a stress fracture develops gradually through a cycle of microdamage accumulation, and the femoral neck is one of the highest-risk and most clinically consequential sites in the body.
The condition is encountered primarily in distance runners, military recruits, and individuals with relative energy deficiency in sport (RED-S), formerly described as the female athlete triad. The reason the femoral neck is so dangerous compared with, for example, a tibial stress fracture, is that a complete or displaced fracture at this location directly threatens the blood supply to the femoral head - meaning that delayed or incorrect management can lead to avascular necrosis (AVN), a catastrophic outcome in a young, active person.
For the exam, three themes dominate: how to classify the fracture (tension versus compression side using the Fullerton system), how to investigate (the central role of MRI when plain X-rays are normal), and how to manage (particularly the emergency nature of tension-side fractures). The examiner will test whether you know that a normal X-ray does not exclude the diagnosis, and whether you know that a tension-side fracture must be fixed urgently.
Anatomy
Relevant anatomy
The femoral neck is a short, angled bridge of bone connecting the femoral head to the shaft. It is oriented at approximately 125 to 135 degrees of neck-shaft angle to the shaft (valgus), and approximately 10 to 15 degrees of anteversion. Its cortex is thicker inferiorly (compression side) and thinner superiorly (tension side).
Blood supply to the femoral head - the critical anatomical concern at this site:
- The medial femoral circumflex artery (MFCA) is the dominant supplier. Its lateral epiphyseal branches travel along the posterosuperior femoral neck inside the retinacular vessels (Weitbrecht's retinaculum).
- The lateral femoral circumflex artery contributes via the anteroinferior vessels.
- The artery of the ligamentum teres (foveal artery) supplies a small central region and is insufficient alone to sustain the femoral head.
A displaced femoral neck fracture - including one that starts as a stress fracture - can tear or kink the retinacular vessels, interrupting femoral head perfusion and causing AVN. This is the anatomical basis for treating tension-side fractures as an emergency.
Mechanical loading at the femoral neck
During stance phase of running, the femoral neck experiences:
- Compressive (bending) stress on the inferior (medial) cortex from body weight transmitted through the hip joint above.
- Tensile stress on the superior (lateral) cortex from the hip abductor muscles pulling on the greater trochanter, which bends the neck upward.
This explains why stress fractures occur on two distinct surfaces with different risk profiles:
- Compression-side fractures (inferior cortex) are more common and are inherently stable - the impacted cortex resists displacement.
- Tension-side fractures (superior cortex) are less common but inherently unstable - tensile forces act to pull the fracture apart, risking rapid displacement.
The tension versus compression distinction is the anatomical foundation of the Fullerton classification and drives every management decision at this site.
Pathophysiology
Bone constantly remodels in response to loading through the coupled process of osteoclast resorption followed by osteoblast formation. When loading exceeds the rate of repair - through sudden training escalation, inadequate energy availability, or compromised bone density - microcracks accumulate faster than they are repaired. The result is a stress reaction initially (bone marrow oedema visible on MRI) that progresses to a frank stress fracture (cortical break or complete fracture line).
The fatigue-insufficiency spectrum
Stress fractures fall on a spectrum:
- Fatigue fractures occur in bone with normal strength and density when mechanical load is excessive or training escalation is too rapid. Distance runners and military recruits typically fall in this category.
- Insufficiency fractures occur when normal loading acts on pathologically weakened bone - from osteoporosis, osteomalacia, vitamin D deficiency, or relative energy deficiency in sport. Older patients and those with metabolic bone disease fall here.
Both subtypes present identically - the distinction matters for bone health management, not for acute orthopaedic decisions.
Relative energy deficiency in sport (RED-S) and the female athlete triad
The female athlete triad describes the interrelated syndrome of:
- Low energy availability (insufficient caloric intake relative to exercise demands).
- Menstrual dysfunction (functional hypothalamic amenorrhoea driven by energy deficiency).
- Low bone mineral density (consequence of oestrogen deficiency and suppressed bone formation).
The broader concept - RED-S - extends this to male athletes and encompasses cardiovascular, immunological, and psychological consequences beyond bone health. Any athlete presenting with a femoral neck stress fracture should be systematically screened for RED-S.
Clinical Pearl
The lateral epiphyseal vessels of the MFCA travel in the retinacular tissue along the posterosuperior femoral neck - they are the critical blood supply to the femoral head and the anatomical reason why tension-side and displaced femoral neck stress fractures are orthopaedic emergencies.
Classification
The Fullerton classification is the key system for femoral neck stress fractures and the one most tested in vivas. It divides fractures by the cortex primarily affected, which directly dictates management.
Fullerton Classification of Femoral Neck Stress Fractures
| Type | Location | X-ray appearance | Mechanism | Risk | Management |
|---|---|---|---|---|---|
| Compression-side | Inferior (medial) cortex | Hazy sclerotic line or endosteal callus on the inferior neck | Compressive loading in stance phase - fracture is impacted | Lower - inherently stable; tends not to displace | Protected weight bearing; surgery if greater than 50% cortex involved or any displacement |
| Tension-side | Superior (lateral) cortex | Lucent (black) transverse line on the superior neck - may be subtle | Tensile loading from abductor pull - fracture pulled apart | High - can displace rapidly and without warning | Urgent surgical fixation - cannulated screws or DHS same admission |
| Displaced (complete) | Full-thickness, any cortex | Obvious femoral neck fracture with displacement of femoral head | Complete failure - often after prolonged ignored pain | Highest - blood supply already at severe risk | Emergency surgical fixation; anatomical reduction mandatory; high AVN rate even with correct treatment |
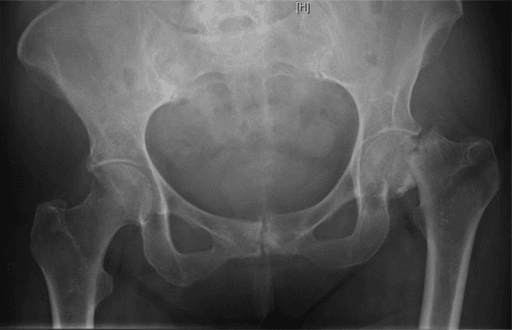
How to remember the X-ray signs
On an anteroposterior hip radiograph:
- Compression side: look at the inferior (medial, lower) surface of the femoral neck - a faint hazy sclerotic (white) line or a band of callus is the hallmark. This represents impacted bone and callus forming along the compressed cortex.
- Tension side: look at the superior (lateral, upper) surface of the femoral neck - a transverse lucent (dark) crack indicates the fracture line being pulled open. This sign is often subtle or even invisible, which is exactly why MRI is mandatory when clinical suspicion is present.
Clinical Pearl
In practice, the tension-side radiographic lucency is frequently invisible on plain X-rays - this is not a reason to be reassured. If the history is right (active individual, insidious groin pain, worse with loading), MRI is the mandatory next step regardless of what the plain film shows.
The Fullerton system is the primary classification in clinical practice and the one to lead with in any orthopaedic examination.
Clinical Presentation
History
The typical history is one of insidious onset anterior hip or groin pain in a runner or recruit that:
- Begins after a period of increased training load (new season, longer race preparation, military basic training).
- Is initially present only during activity and relieved by rest.
- Progressively worsens until pain occurs at rest, at night, or with ordinary walking.
- May be associated with a aching quality or a sensation of hip fatigue rather than sharp focal pain.
Critically, some patients report a history of groin pain that was initially ignored or attributed to a muscle strain before the fracture completed and displaced. This is the pathway to catastrophe.
Key risk factor questions to ask:
- Training volume and recent escalation in mileage or intensity.
- Running surface, footwear, and biomechanical issues.
- Dietary intake, weight, and menstrual history (screen for RED-S/female athlete triad).
- Previous stress fractures.
- Bone health: previous DEXA scan, calcium and vitamin D intake.
Examination
Examination findings are often subtle in an undisplaced fracture:
- Gait: the patient may walk with a slight antalgic limp or protective hip posture.
- Look: no visible deformity in undisplaced fractures; rotational deformity and shortening if displaced.
- Feel: deep groin tenderness on palpation. There is usually no bony tenderness over the greater trochanter or lateral hip (which would suggest trochanteric bursitis or ITB syndrome).
- Move: restricted range of motion - particularly limited and painful internal rotation and flexion. This is different from a trochanteric problem where external rotation is more restricted.
- Special tests:
Fulcrum Test
The examiner places their forearm under the patient's thigh as a fulcrum, then presses gently down on the knee to apply a bending force across the femoral neck. A positive test reproduces the groin pain and indicates a stress fracture. Sensitivity is moderate but it is a useful bedside test in the right clinical context.
Single-Leg Stance (Trendelenburg)
The patient stands on the affected limb. Pain or a positive Trendelenburg sign (contralateral pelvis drop) suggests hip pathology. In an early stress fracture, the patient may simply be unable to single-leg stand without pain - this indicates significant load-sensitive pathology.
Hop Test
The patient attempts a single-leg hop on the affected side. In a suspected stress fracture, this test should be performed with extreme caution - a high-grade tension-side fracture could displace with the load of hopping. Many clinicians omit this test in favour of MRI once clinical suspicion is high.
Internal Rotation Pain
Passive internal rotation of the hip - with the hip flexed to 90 degrees (the FADIR position) - typically reproduces or worsens the pain. Any intra-articular or femoral neck pathology tends to be painful in this position. Compare both sides and note the range restriction.
Clinical Pearl
The single most important examination finding is restricted and painful internal rotation of the hip in a runner with groin pain. Combine this with the history of training escalation and the diagnosis of femoral neck stress fracture should be high on your differential until MRI proves otherwise.
Investigations
Plain radiography: order but do not rely on
An anteroposterior pelvis and a lateral hip view (frog-leg or true lateral) should be the first investigation. However:
- Plain X-rays are normal in up to 50% of femoral neck stress fractures, particularly early in the course.
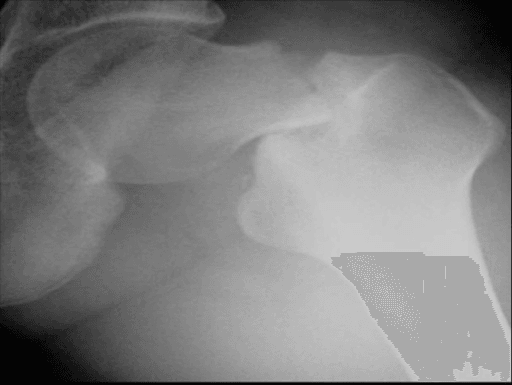
- When positive, look for a sclerotic (white) band on the inferior neck (compression side) or a transverse lucent line on the superior neck (tension side).
- A displaced fracture will be obvious, but by the time it is visible on X-ray the situation is already an emergency.
The key rule: a normal X-ray does not exclude a femoral neck stress fracture. Proceed to MRI in any patient with the right clinical picture.
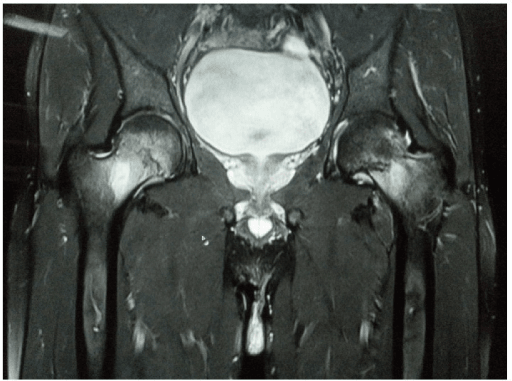
MRI: the gold-standard investigation
MRI is the investigation of choice. It should be requested urgently when clinical suspicion is present - do not wait for a formal elective slot.
- STIR (short-tau inversion recovery) or fat-saturated T2 sequences: show bone marrow oedema as high signal within the femoral neck. This is the earliest sign of stress injury and can be present before any cortical abnormality is visible.
- T1-weighted sequences: show a low-signal fracture line within the otherwise bright (fatty) marrow - this is the definitive finding of a cortical stress fracture.
- Coronal sequences through both hips: essential to look for bilateral involvement (more common than expected, especially with the female athlete triad).
Imaging Modalities for Femoral Neck Stress Fracture
| Modality | Sensitivity | Specificity | What it shows | When to use |
|---|---|---|---|---|
| Plain X-ray (AP pelvis + lateral hip) | Approximately 50% early; higher if displaced | High if positive | Sclerotic line (compression), lucent line (tension), or obvious displaced fracture | Always first - but a normal result does not exclude the diagnosis |
| MRI (STIR + T1) | Greater than 95% | High | Bone marrow oedema (STIR) and fracture line (T1) - earliest detection | Gold standard - urgent if clinical suspicion is present |
| Bone scintigraphy (isotope bone scan) | High overall | Lower than MRI | Focal increased uptake at the fracture site | Second line if MRI is unavailable or contraindicated - lower specificity |
| CT scan | Moderate for stress fractures | High if cortical break visible | Cortical breaks and fracture lines clearly - useful for operative planning | Useful to characterise displacement pre-operatively; not for initial diagnosis |
What to do with the MRI result
Once MRI confirms a femoral neck stress fracture, the key decision is tension side versus compression side:
- Compression-side, less than 50% cortical involvement, no displacement: admission for protected weight bearing, activity modification, repeat MRI in 4 to 6 weeks to confirm non-progression.
- Tension-side (any grade), greater than 50% cortical involvement on either side, or any displacement: immediate surgical referral for fixation on the next available theatre list. Do not send the patient home to await an outpatient appointment.
Blood tests and bone health screen
In any patient with a femoral neck stress fracture, especially outside the expected demographic (e.g. older, less athletic, bilateral), perform:
- Full blood count, renal function, liver function, bone profile (calcium, phosphate, alkaline phosphatase).
- Vitamin D level (25-OH vitamin D).
- Consider parathyroid hormone, DEXA scan, and endocrinology referral if an underlying metabolic bone disease is suspected.
- In female athletes, document menstrual history and consider RED-S/female athlete triad workup.
Do Not Miss Bilateral Involvement
Bilateral femoral neck stress fractures occur in up to 15% of cases, particularly in individuals with relative energy deficiency, metabolic bone disease, or military recruits. Always image both hips with MRI. Missing the contralateral side can lead to a second disaster.
Management
Management is dictated primarily by the Fullerton type. The overriding principle is: do not allow a tension-side or high-grade fracture to displace. Prevention of displacement is prevention of AVN.
Non-operative: Compression-Side, Low-Grade
- Admit or immediately restrict weight bearing - non-weight bearing or protected weight bearing on crutches.
- Analgesia and modification of all impact activity.
- Correct any underlying cause: optimise vitamin D, calcium, and energy availability; address training errors.
- Repeat MRI at 4 to 6 weeks: if no progression and improving symptoms, gradual return to activity. If worsening MRI or any displacement appears, proceed to surgery.
- Typical return to running: 6 to 12 weeks for low-grade compression-side fractures.
Urgent Surgery: Tension-Side and High-Grade
- Admit and place on strict non-weight bearing immediately.
- Inform the on-call orthopaedic team - this is an urgent surgical case.
- Operate on the next available list; do not delay overnight unnecessarily.
- Fixation options: three parallel cannulated cancellous screws (inverted triangle configuration) or a dynamic hip screw (DHS) with or without an anti-rotation screw.
- Post-operatively: non-weight bearing for 6 weeks, then progressive weight bearing as healing confirms on X-ray or CT. Return to sport typically after 4 to 6 months with confirmed radiographic union.
Complications
Complications of Femoral Neck Stress Fracture
| Complication | Mechanism | Risk factors | Prevention / management |
|---|---|---|---|
| Avascular necrosis (AVN) of femoral head | Interruption of the retinacular (lateral epiphyseal) vessels by displacement, haematoma, or intracapsular pressure | Displacement, delay to treatment, high-energy injury, older age | Urgent fixation to prevent displacement; anatomical reduction if displaced; monitor with serial MRI post-op |
| Nonunion | Failure of fracture healing - often from inadequate fixation, poor biology, or continued loading | Poor bone quality, displaced fracture, inadequate fixation, nutritional deficiency | Rigid fixation, address bone health, non-weight bearing compliance; valgus osteotomy or total hip replacement in established nonunion |
| Implant failure / hardware complication | Screw cutout, migration, or breakage - typically from collapse in poor bone | Poor bone density, technical error, early loading | Careful screw placement, appropriate post-op weight bearing restriction, confirm union before removing restriction |
| Displacement after non-operative treatment | Compression-side fracture progresses and displaces - converts from low-risk to high-risk | Underestimated fracture grade, non-compliance, premature return to activity, progression missed on follow-up imaging | Strict non-weight bearing, close MRI follow-up, low threshold for fixation if any worsening |
| Recurrence / contralateral fracture | Second stress fracture due to uncorrected biomechanical, nutritional, or metabolic cause | RED-S, untreated osteoporosis, return to same training errors | Mandatory metabolic and nutritional assessment; bilateral MRI imaging; graduated return to sport |
| Hip osteoarthritis (late) | Post-traumatic arthritis secondary to AVN with collapse, nonunion, or joint incongruity | AVN, malunion, delayed treatment | Prevention by avoiding AVN; monitor long-term; total hip replacement if end-stage |
Avascular necrosis in detail
AVN is the complication that defines the severity and urgency of femoral neck stress fractures. The risk is directly proportional to the degree of displacement and the delay between injury and treatment:
- In undisplaced fractures treated promptly, AVN risk is low (less than 5% with appropriate management).
- In displaced fractures, AVN rates of 20 to 30% or higher are reported even with prompt surgical fixation - the blood supply may already have been compromised at the time of displacement.
- MRI is the most sensitive investigation for early AVN post-operatively, showing decreased perfusion signal in the femoral head before any collapse is apparent on plain radiographs.
The practical lesson: prevention through early diagnosis and urgent fixation of high-risk fractures is far more effective than any treatment for established AVN.
Nonunion
Nonunion at the femoral neck after stress fracture is less common than after acute traumatic fractures but is a recognised complication, especially if:
- Fixation was inadequate.
- The patient returned to loading too early.
- Underlying metabolic bone disease or nutritional deficiency was not corrected.
Established nonunion in a young patient is managed with valgus intertrochanteric osteotomy to redirect forces and stimulate healing. In older patients or those with concurrent AVN, total hip replacement may be the more pragmatic solution.
Clinical Relevance
Femoral neck stress fractures sit at the intersection of sports medicine, trauma, and basic science - exactly the domains examiners explore in depth. The topic tests whether a candidate can recognise a high-risk diagnosis from an atypical history, interpret normal and abnormal imaging correctly, make a time-sensitive management decision, and understand the anatomical basis for the most feared complication.
In sports medicine practice, this is one of the diagnoses where missing it - or downgrading it from tension-side to compression-side without adequate imaging - can destroy a young person's hip. The story of a runner whose groin pain was attributed to a muscle strain for several weeks before a complete displaced fracture was found is not rare. The lesson is embedded in every guideline: persistent groin pain in an active individual requires MRI.
In surgical practice, the internal fixation of an undisplaced tension-side fracture is a relatively straightforward percutaneous procedure - but it must be done urgently, correctly, and with post-operative non-weight bearing enforced. Get the screws into the calcar and the femoral head. Confirm no articular penetration. Keep the patient on crutches until the imaging confirms union.
In basic science vivas, the anatomy of the femoral head blood supply and the biomechanics of tension versus compression loading at the femoral neck are classical questions. Know the medial femoral circumflex artery, its lateral epiphyseal branches, and why displacement compromises them.
Evidence
Landmark Classification: Tension vs Compression Side Femoral Neck Stress Fractures
- Retrospective case series establishing the clinical and radiographic classification of femoral neck stress fractures into tension-side (superior cortex) and compression-side (inferior cortex) types
- Tension-side fractures carry a high risk of displacement and should be treated with urgent internal fixation - non-operative management risks catastrophic displacement
- Compression-side fractures with less than 50% cortical involvement in young athletes with normal bone can initially be managed non-operatively with protected weight bearing and close follow-up
- Displaced femoral neck stress fractures carry a high rate of avascular necrosis even with prompt surgical fixation
- This paper established the management principles that remain the foundation of current practice
Displaced Femoral Neck Stress Fracture in a Female Distance Runner with the Female Athlete Triad
- Case report of a displaced femoral neck stress fracture in an adolescent female distance runner with all three components of the female athlete triad: low body weight, amenorrhoea, and low bone density
- Initial presentation was with groin pain attributed to muscle strain - a common diagnostic delay scenario
- Internal fixation was performed urgently; postoperative MRI at 6 months showed early signs of avascular necrosis (low signal on T1-weighted imaging) alongside healing at the fracture site
- Bone scintigraphy at 6 months showed uptake at both the fracture site and the femoral head, confirming vascular insult
- Highlights the importance of recognising the female athlete triad as a major risk amplifier and the need for urgent action when displacement occurs
Simultaneous Bilateral Femoral Neck Stress Fracture: MRI Diagnosis and Dynamic Hip Screw Fixation
- Case report of simultaneous bilateral femoral neck stress fractures in a 24-year-old male stone mason with high repetitive occupational loading
- Initial plain radiograph showed only a faint fracture line in the left femoral neck; MRI confirmed bilateral fractures with T2 signal change in both femoral necks
- Both hips were fixed with dynamic hip screws (three-holed plate); postoperative radiographs showed satisfactory implant position
- Follow-up at 6 months showed progressive radiographic union bilaterally
- Illustrates that stress fractures are not exclusive to classical athletic populations; bilateral involvement is real and MRI of both hips is essential
Femoral Neck Stress Fractures: Review of Classification and Management in Athletes
- Review article consolidating evidence on femoral neck stress fractures in the athletic population, supporting the tension versus compression side classification
- Tension-side fractures in athletes should be treated with prophylactic internal fixation to prevent displacement and its sequelae
- Compression-side fractures in athletes with normal bone can be managed with protected weight bearing, but require close follow-up as progression to displacement has been reported
- MRI was highlighted as superior to plain radiography and bone scintigraphy for early detection and accurate characterisation of fracture type
- Return to sport after non-operative management of compression-side fractures is typically possible at 6 to 12 weeks with symptomatic and radiographic resolution
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Runner with Groin Pain and a Normal X-ray (~4 min)
"A 22-year-old female elite marathon runner presents with a 3-week history of right groin pain that is worse during and after running. She has recently doubled her weekly training mileage. Examination shows painful and limited internal rotation of the right hip. Her plain radiographs are reported as normal. What do you do next?"
Impression and urgency: This presentation is highly suspicious for a femoral neck stress fracture. I take it seriously - this is one of the high-risk stress fracture sites and a missed tension-side fracture can lead to displacement and avascular necrosis. I would not be falsely reassured by the normal X-ray, as up to 50% of femoral neck stress fractures are radiographically occult early on.
Investigation: I would arrange urgent MRI of the hip with coronal STIR and T1 sequences through both hips. I would not send her home to wait for an outpatient MRI - I would arrange this urgently, ideally within 24 to 48 hours. If MRI is unavailable, bone scintigraphy is an alternative, though with lower specificity.
While waiting: I would advise immediate cessation of running and all impact activities. Depending on the clinical picture, I might keep her non-weight bearing with crutches while awaiting the scan, particularly if the history is convincing.
If MRI confirms a femoral neck stress fracture: I then classify it as tension-side or compression-side. A compression-side low-grade fracture could be managed non-operatively with protected weight bearing and close MRI follow-up. A tension-side fracture requires urgent surgical fixation - I would admit her and arrange fixation on the next available list.
I would also screen for relative energy deficiency in sport (RED-S) and the female athlete triad - asking about dietary restriction, menstrual regularity, and energy availability. Vitamin D and bone density testing should be arranged.
Tension-Side Stress Fracture: Urgent Fixation Decision (~5 min)
"MRI of the runner from the previous scenario shows a transverse low-signal line on T1-weighted imaging along the superior cortex of the femoral neck, with extensive bone marrow oedema on STIR. There is no displacement. The registrar on call tells you the fracture can wait for an elective list next week because it is not displaced yet. Do you agree?"
I do not agree. This is a tension-side femoral neck stress fracture - a fracture on the superior cortex that is under tensile loading from the hip abductor muscles. Unlike a compression-side fracture, which is inherently stable because the fractured surfaces are being pushed together, a tension-side fracture is being pulled apart by physiological forces. It can displace suddenly and without warning, even during low-load activities like walking.
The consequence of displacement is disruption of the retinacular vessels - the lateral epiphyseal branches of the medial femoral circumflex artery - which supply the femoral head. Avascular necrosis in a 22-year-old athlete would be a catastrophic outcome. The rate of AVN rises significantly with any delay in treatment.
My decision: This patient should be admitted for strict non-weight bearing immediately and listed for internal fixation on the next available theatre list - ideally today or tomorrow, not next week. I would escalate to the on-call consultant if necessary.
Surgical plan: I would perform percutaneous cannulated cancellous screw fixation. Under fluoroscopic guidance, I would place three parallel partially threaded screws in an inverted triangle configuration - one along the calcar inferiorly and two superior screws. The smooth shank crosses the fracture site and the threads are in the femoral head, providing compression at the fracture site.
Post-operatively: Non-weight bearing on crutches for 6 weeks, then progressive loading with radiographic confirmation of union before returning to full weight bearing. Return to running would not be before 4 to 6 months and only with confirmed radiographic union.
Young Female with Bilateral Femoral Neck Fractures and Metabolic History (~5 min)
"A 19-year-old female gymnast is brought to the emergency department after her right hip gave way while dismounting from the beam. Plain radiographs show a displaced right femoral neck fracture. On further questioning she reports 6 months of bilateral hip pain. She has not had a period in 18 months, weighs 42 kg, and her vitamin D level comes back at 18 nmol/L. What are your priorities and what further imaging do you order?"
Immediate orthopaedic priority: The displaced right femoral neck fracture is an emergency. I ensure the patient is immediately non-weight bearing, provide adequate analgesia, and inform the on-call consultant for urgent surgical planning. Anatomical reduction and internal fixation should proceed as soon as the patient is medically optimised - the longer we wait, the higher the risk of avascular necrosis.
However, I am also very concerned about the left hip: She reports 6 months of bilateral hip pain. A displaced fracture on one side following a minor mechanism in a 19-year-old with very low body weight, amenorrhoea, and severe vitamin D deficiency strongly suggests that the left hip may also have an unrecognised stress fracture. I would urgently order an MRI of the left hip alongside the right.
Diagnosis of the female athlete triad (or RED-S): This patient has all three components: low energy availability (42 kg, restricted diet in gymnastics), menstrual dysfunction (18 months amenorrhoea), and low bone density (implicit from the vitamin D deficiency and fragility fracture). I would arrange a DEXA scan, full bone metabolism blood panel, and refer to a sports medicine physician and a dietitian.
Surgical planning for the right hip: Closed or open reduction on the fracture table followed by cannulated screw fixation or a dynamic hip screw. Given the poor bone quality from the metabolic context, I would discuss with the consultant whether supplementary bone health optimisation is needed post-operatively.
If the left MRI shows a tension-side stress fracture: I would recommend bilateral fixation - right hip urgently for the displaced fracture, and prophylactic or therapeutic fixation of the left. Bilateral staged or simultaneous surgery under the same anaesthetic may be appropriate.
Long-term: Address the root cause - energy availability, bone health, hormonal status, and return-to-sport planning with the gymnastic coaching team.
FEMORAL NECK STRESS FRACTURE
Clinical summary
Who Gets It
- •Distance runners, military recruits, gymnasts
- •Female athlete triad / RED-S: low energy, amenorrhoea, low bone density
- •Sudden training escalation - too much too soon
- •Metabolic bone disease: osteomalacia, vitamin D deficiency
Classification (Fullerton)
- •Compression side (inferior cortex): sclerotic/white line, stable, non-op if low-grade
- •Tension side (superior cortex): lucent/black line, unstable, URGENT FIXATION
- •Displaced (complete): emergency fixation, high AVN risk even with perfect surgery
Investigations
- •AP pelvis + lateral hip: first - but normal in up to 50% of cases
- •MRI (STIR + T1): gold standard - book urgently, do not wait for elective
- •Image both hips: bilateral involvement is underappreciated and must be excluded
- •Bone profile, vitamin D, DEXA scan: essential in any atypical or recurrent case
Management
- •Compression side, less than 50% cortex: protected weight bearing + MRI follow-up
- •Tension side (any grade): urgent surgical fixation - not next week, this admission
- •Fixation: 3 cannulated screws (inverted triangle) or dynamic hip screw
- •Post-op: non-weight bearing 6 weeks; return to sport 4 to 6 months with union confirmed
Complications
- •AVN (avascular necrosis): the catastrophic complication - proportional to delay and displacement
- •Nonunion: poor bone quality, inadequate fixation, premature loading
- •Bilateral involvement: missed contralateral fracture is a preventable disaster
- •Late osteoarthritis: sequela of AVN with femoral head collapse
Guidelines, Registries and Global Practice
-
No single international guideline specifically governs the management of femoral neck stress fractures. Practice is guided by expert consensus, landmark case series (particularly Fullerton and Snowdy 1988), and sports medicine society position statements on high-risk stress fractures.
-
American Orthopaedic Society for Sports Medicine (AOSSM) and British Orthopaedic Association (BOA) guidance on stress fractures classifies the femoral neck as a high-risk site requiring urgent evaluation and surgical fixation for tension-side or displaced fractures - consistent with Fullerton principles.
-
Relative Energy Deficiency in Sport (RED-S): the International Olympic Committee (IOC) published its consensus statement on RED-S in 2014 and updated it in 2018 and 2023. This replaced the narrower concept of the female athlete triad and now applies to all athletes regardless of sex. Management of stress fractures in the context of RED-S requires multidisciplinary care: sports medicine, dietitian, endocrinology, and psychology.
-
Military populations: the US Department of Defense (DoD) and UK Armed Forces have specific protocols for stress fractures in recruits. Femoral neck stress fractures in military trainees are managed aggressively given the high-risk nature of the site. Recruits are typically medically downgraded and taken off training immediately.
-
Return to sport criteria vary by institution but broadly require: resolution of pain, confirmed radiographic union (X-ray or CT), full pain-free range of motion, and successful completion of a graduated loading programme. No major registry specifically tracks outcomes of femoral neck stress fractures at a population level.
-
Bilateral femoral neck stress fractures: reported in endurance athletes, recruits, and individuals with metabolic bone disease across multiple global case series. The consistent message from all regions is to image both hips with MRI when one side is confirmed, as missing the contralateral fracture leads to preventable catastrophe.
-
Vitamin D and bone health optimisation: globally recommended as part of the management of any stress fracture patient. Target 25-OH vitamin D levels are typically set at greater than 50 nmol/L (greater than 20 ng/mL) by most international societies, with supplementation for deficiency universally recommended.