Floating Knee Injury
Ipsilateral Femur + Tibia | Fraser Classification | High-Energy Polytrauma
Fraser Classification
Critical Must-Knows
- Fraser Classification: Type I (both extra-articular = best), IIA (tibial articular), IIB (femoral articular), IIC (both = worst)
- Ligamentous injury in 50%+ - often missed initially due to swelling/pain. Always reassess and MRI when stable
- Stabilise BOTH fractures - typically IM nails if extra-articular. Same sitting reduces complications
- Damage control if patient unstable: spanning external fixation of both, definitive fixation when resuscitated
- Vascular injury and compartment syndrome (thigh AND leg) must be assessed
Clinical Pearls
- "Femur first usually preferred - restores limb length, facilitates tibial reduction
- "Type IIC (both articular) has worst prognosis - complex surgical management required
- "Knee stiffness is common complication - early mobilisation essential
- "Open fractures common in this high-energy pattern
Clinical Imaging
Imaging Gallery


Exam Warning
Fraser Classification
Articular = Bad. Type I (Extra-articular) is best. Type IIC (Both articular) is worst.
Hidden Injury
Ligaments. Greater than 50% have ACL/PCL tears. Often missed due to swelling/pain.
Double Danger
Compartment Syndrome. Assess BOTH thigh and leg compartments closely.
At a Glance
Floating knee injury describes ipsilateral femur and tibia fractures creating an unstable knee segment disconnected from axial skeleton. It results from high-energy trauma (MVA, motorcycle accidents) with associated injuries in 80% and mortality of 5-15%. The Fraser classification determines prognosis: Type I (both extra-articular, best prognosis), Type IIA (tibial articular), Type IIB (femoral articular), Type IIC (both articular, worst prognosis). Management involves stabilization of both fractures, typically with intramedullary nailing if extra-articular. Critical associated injuries include ligamentous knee injury (greater than 50%, often missed initially), vascular injury requiring angiography, and compartment syndrome in both thigh and leg.
I-ABCFraser Classification
| I | Extra-articular Both Best prognosis - both IM nailable |
| A | Articular Tibia Type IIA - tibial plateau involvement |
| B | Bone (Femur) articular Type IIB - distal femur involvement |
| C | Combined Type IIC - both articular = worst |
| I | Extra-articular Both Best prognosis - both IM nailable | B | Bone (Femur) articular Type IIB - distal femur involvement |
| A | Articular Tibia Type IIA - tibial plateau involvement | C | Combined Type IIC - both articular = worst |
Hook:I-ABC: I for extra-articular (Individual bones), ABC for articular (A=tibia, B=femur, C=Combined)
CLVNFloating Knee Assessment
| C | Compartments Check BOTH thigh AND leg compartments |
| L | Ligaments 50%+ have knee ligament injury (often occult) |
| V | Vascular Popliteal artery at risk - assess DP/PT pulses |
| N | Nerve Peroneal nerve most vulnerable |
| C | Compartments Check BOTH thigh AND leg compartments | V | Vascular Popliteal artery at risk - assess DP/PT pulses |
| L | Ligaments 50%+ have knee ligament injury (often occult) | N | Nerve Peroneal nerve most vulnerable |
Hook:CLVN: Check Limbs, Vessels, Nerves for compartment and vascular safety
F-T-SManagement Sequence
| F | Femur First Restores limb length, facilitates tibial reduction |
| T | Tibia Second IM nail if extra-articular, ORIF if plateau |
| S | Same Sitting Reduces complications, shortens hospital stay |
| F | Femur First Restores limb length, facilitates tibial reduction |
| T | Tibia Second IM nail if extra-articular, ORIF if plateau |
| S | Same Sitting Reduces complications, shortens hospital stay |
Hook:F-T-S: Femur restores length, Tibia follows, Same sitting for efficiency
Overview
Floating knee injury describes ipsilateral fractures of the femur and tibia, creating an unstable knee segment that is disconnected from the axial skeleton. The term reflects the biomechanical reality that the knee "floats" free between two fracture sites.
Epidemiology
- Incidence: Accounts for 2-4% of lower extremity fractures
- Demographics: Male predominance (3:1), peak age 20-40 years
- Mechanism: High-energy trauma (MVA 70%, motorcycle 20%, pedestrian vs vehicle 5%)
- Polytrauma association: Present in 70-80% of cases
- Mortality: 5-15% (usually from associated injuries)
- Open fracture rate: 30-40%
Associated Injuries
| Injury Type | Incidence | Clinical Significance |
|---|---|---|
| Knee ligament injury | 50-70% | Often missed initially, affects rehabilitation |
| Vascular injury | 5-10% | Limb-threatening, requires urgent assessment |
| Compartment syndrome | 10-20% | Both thigh and leg at risk |
| Ipsilateral hip/ankle | 15-20% | Must image entire limb |
| Head/chest/abdominal | 40-60% | ATLS priorities |
Anatomy and Biomechanics
Relevant Anatomy
Knee as the "Floating" Segment:
- The knee joint and surrounding soft tissues become an unstable segment
- Disconnected superiorly by femur fracture and inferiorly by tibia fracture
- Popliteal vessels and nerves traverse this zone
Critical Vascular Anatomy:
- Popliteal artery: Fixed at adductor hiatus proximally and soleus arch distally
- Tethered position makes it vulnerable to traction injury
- Intimal tears may cause delayed thrombosis
Muscular Attachments:
- Quadriceps mechanism spans the femur fracture
- Gastrocnemius origin crosses the knee
- These contribute to deforming forces and stiffness
Biomechanical Considerations
Deforming Forces:
- Femur: Proximal fragment abducted and flexed (iliopsoas, abductors)
- Tibia: Variable depending on fracture level
- Knee tends toward flexion contracture if not mobilized early
Load Transmission:
- Normal: Axial load through femur → knee → tibia
- Floating knee: Complete loss of axial stability
- Requires fixation of BOTH fractures for weight-bearing
Classification Systems
Fraser Classification
| Type | Femur | Tibia | Prognosis |
|---|---|---|---|
| Type I | Shaft (Extra-articular) | Shaft (Extra-articular) | Best (75-85% Excellent) |
| Type IIA | Shaft | Articular (Plateau) | Moderate (60-70% Good) |
| Type IIB | Articular (Condyle) | Shaft | Poor (55-65% Good) |
| Type IIC | Articular (Condyle) | Articular (Plateau) | Worst (45-55% Good) |
The Fraser system remains the most widely used classification, but it describes only the bony pattern and has limited prognostic power because it ignores soft-tissue and extensor-mechanism injury (see Controversies).
Differential Diagnosis and Mimics
The diagnosis of a floating knee is radiographic (ipsilateral femur AND tibia fracture), so the real "differential" is recognising which adjacent injury patterns can masquerade as, accompany, or be mistaken for it. The table below contrasts the floating knee with the patterns it is most often confused with on initial trauma imaging.
Floating Knee vs Look-Alike Patterns
| Pattern | Distinguishing feature | Why it matters | Key action |
|---|---|---|---|
| Floating knee (true) | Fracture of BOTH ipsilateral femur and tibia | Knee segment isolated from axial skeleton | Stabilise both bones |
| Isolated femoral shaft fracture | Intact tibia on full-length film | Knee not isolated; standard nailing | Image whole limb to exclude second fracture |
| Floating hip (ipsilateral acetabulum + femur) | Pelvic/acetabular fracture, not tibia | Different proximal segment isolated | AP pelvis and CT pelvis |
| Knee dislocation / fracture-dislocation | Tibiofemoral malalignment, multiligament injury | High popliteal artery injury risk even without shaft fracture | Reduce, document pulses, ABI/CT angiogram |
| Floating knee in children (Letts-Ran) | Physeal involvement, remodelling potential | Different classification and growth implications | Use paediatric system; assess physes |
| Combined plateau + distal femur (no shaft) | Both articular but no diaphyseal break | Behaves like Fraser IIC for the joint | Anatomic ORIF of both articular surfaces |
The single commonest error is under-imaging: an obvious femoral shaft fracture distracts from a subtle proximal tibial or plateau fracture. Always obtain full-length femur AND tibia films plus dedicated knee views before excluding a floating knee.
Clinical Assessment
Initial Trauma Evaluation
ATLS Priorities:
- High-energy polytrauma focus
- Associated injuries in 80% (Head, Chest, Abdo)
- Hemodynamic stability assessment first
Limb Assessment:
- Obvious deformity and length discrepancy
- Skin integrity (open fractures common)
- Compartment Monitoring: Both thigh (3 compartments) and leg (4 compartments)
- Vascular Exam: Popliteal, DP, PT pulses; ABI if suspicious
- Neurological Exam: Peroneal nerve (most vulnerable)
Assessment of the "floating" segment is secondary to life-saving measures.
Investigations
Radiographic Series
Standard Trauma Series:
- Full-length femur (AP/Lateral)
- Full-length tibia (AP/Lateral)
- AP Pelvis (check for associated hip fractures)
- Dedicated Knee Series (AP/Lateral/Oblique)
Assessment checklist:
- Identify fracture location (diaphyseal vs articular)
- Assess for comminution
- Check joint congruity
A true lateral of the knee is essential to rule out occult subluxation.
Management Algorithm
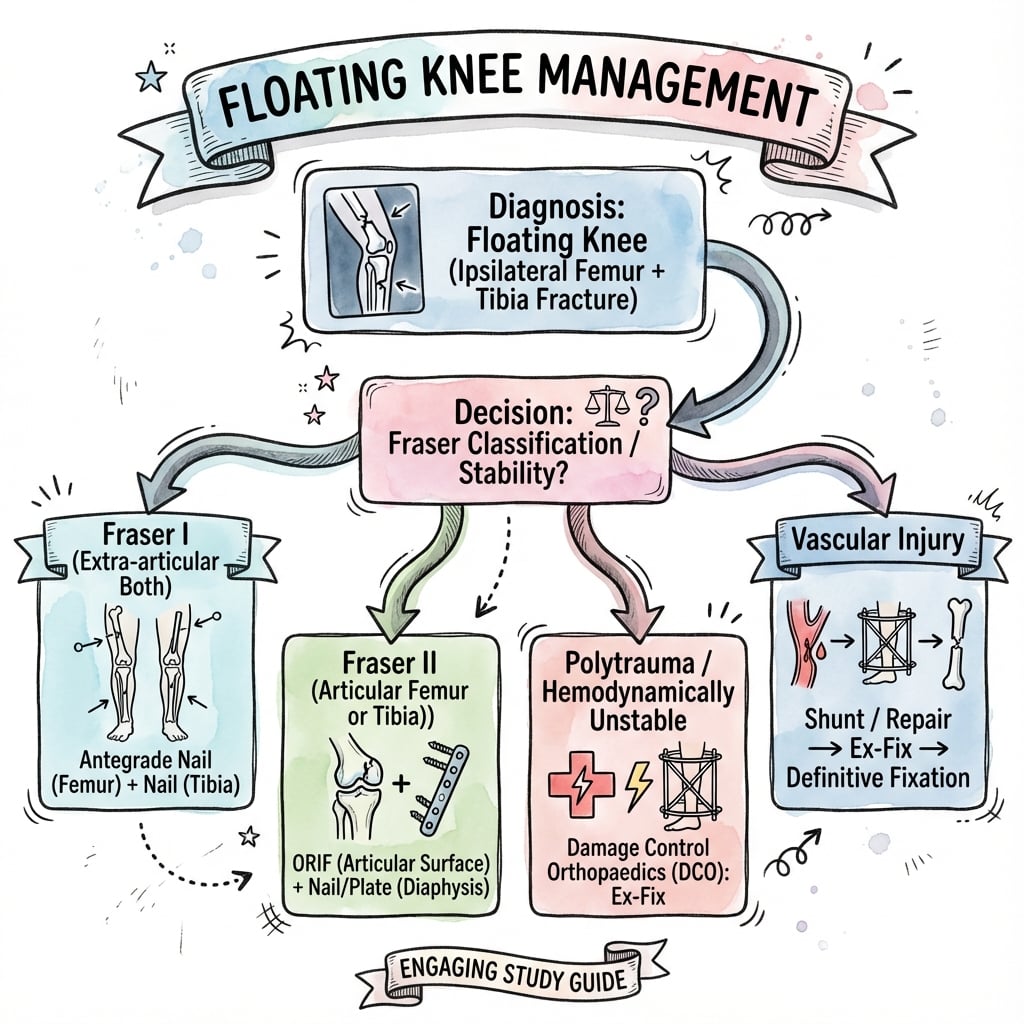
Algorithm should be interpreted in context of overall trauma status.
Ligamentous Injury
More than 50% of floating knee injuries have associated knee ligament damage, but this is often occult initially due to swelling and pain. Always assess the knee once fractures are stabilised and obtain MRI when appropriate.
Clinical Context: Ligamentous injury significantly affects rehabilitation and outcomes.
Management
Damage Control vs Definitive
Damage Control Phase (Unstable Patient):
- Spanning external fixation of both femur and tibia
- Temporary stabilisation to allow resuscitation
- Definitive fixation once physiological parameters normalise
Definitive Fixation (Stable Patient):
- Address both fractures at same sitting if possible
- Reduces hospital stay and allows early motion
Fixation Strategies by Fraser Type:
- Fraser Type I: Double IM nailing (Antegrade femur + Tibia)
- Fraser Type IIA: Femur nailing + Tibial plateau ORIF
- Fraser Type IIB: Distal femur ORIF + Tibial nailing
- Fraser Type IIC: Dual ORIF (Distal femur + Tibial plateau)
Fixation strategy must be tailored to specific fracture patterns.
Sequence of Fixation
Most surgeons prefer femur first:
- Restores limb length and gross alignment
- Facilitates subsequent tibial reduction
- More ergonomic patient positioning
Tibial fixation follows immediately to finalize the construct stability.
Surgical Technique
Femoral Techniques
Intramedullary Nailing:
- Entry: Piriformis or greater trochanteric
- Reamed nailing preferred for stability
- Interlocking screws to control rotation
ORIF (Distal Femur):
- Lateral parapatellar approach
- Anatomic articular reduction first
- Locking plate or retrograde nail depending on complexity
Bone quality and comminution dictate the final implant choice.
Complications
Early Complications
Compartment Syndrome (10-20%):
- Affects both thigh AND leg compartments
- Thigh contains 3 compartments (Often overlooked)
- Maintain high index of suspicion with serial evaluations
- Threshold for prophylactic fasciotomy should be low
Vascular Injury (5-10%):
- Popliteal artery most at risk due to tethered anatomy
- May present delayed due to intimal injury
- Requires immediate revascularization if diagnosed
- Limb viability window: 6-8 hours warm ischemia
Infection:
- Higher rates than isolated fractures (10-15%)
- Open fractures require debridement and antibiotics per Gustilo protocol
- External fixation pin site infections
Late Complications
Knee Stiffness (20-50%):
- Most common long-term problem
- Due to periarticular scarring and quadriceps adhesions
- Prevention: Early ROM, avoid prolonged immobilization
- Treatment: Aggressive physiotherapy, consider manipulation under anesthesia
Malunion/Nonunion:
- Both fracture sites at risk
- Smoking, diabetes, and infection increase risk
- May require revision fixation or bone grafting
Post-traumatic Arthritis:
- Particularly prevalent in Fraser Type II injuries
- Articular damage + ligament instability contribute
- May require total knee arthroplasty in the long term
Postoperative Care
Immediate Postoperative
Day 0-3:
- DVT prophylaxis (LMWH)
- Pain management (multimodal analgesia)
- Neurovascular monitoring
- Wound inspection
Early Mobilization:
- CPM or active-assisted ROM from day 1 if stable fixation
- Quadriceps setting exercises
- Ankle pumps
Weight-Bearing Protocol
| Fracture Pattern | Weight-Bearing Status | Duration |
|---|---|---|
| Type I (both IM nails) | Touch weight-bearing → progressive | 6-12 weeks |
| Type II (articular) | Non-weight-bearing → partial | 8-12 weeks |
| External fixation | Non-weight-bearing | Until definitive fixation |
Rehabilitation Phases
Phase 1 (0-6 weeks):
- ROM exercises (goal: 0-90° knee flexion)
- Quadriceps strengthening (isometric initially)
- Gait training with assistive devices
Phase 2 (6-12 weeks):
- Progressive weight-bearing
- Active ROM to full
- Closed chain exercises
- Aquatic therapy if available
Phase 3 (12+ weeks):
- Full weight-bearing
- Functional training
- Return to activity assessment
- Address remaining ligamentous instability
Outcomes
Functional Recovery
Return to Work:
- 60-70% return to pre-injury occupation
- Average time: 9-12 months
- Manual laborers typically have worse outcomes
Outcome Measures:
- Knee Society Score
- WOMAC
- SF-36
Prognostic Factors (AOA context): Type II injuries (articular) carry a significantly higher burden of post-traumatic OA.
Evidence Base
Original Fraser Classification (foundational)
- Original description of the floating knee and its type I / type II classification
- Type II (articular) injuries had significantly worse outcomes than type I
- Knee stiffness was the most common complication
- Early mobilisation improved functional results
Ipsilateral Fractures of the Femur and Tibia (57 cases)
- 57 consecutive ipsilateral femur/tibia fractures; 33 limbs were open and 21 patients had life-threatening injuries
- Best results when BOTH fractures were stabilised surgically
- Good or excellent functional result in approximately 80%; mean knee arc 129 degrees
- Complications: 3 deep infections, 4 nonunions, 1 below-knee amputation; fat embolism syndrome in 13%
Surgical Management of the Adult Floating Knee
- 15 adults (Fraser I-IIc) treated by fixation of both fractures; mean follow-up 2.2 years
- Karlstrom outcome: excellent 8, good 4, acceptable 2, poor 1
- Associated injuries and fracture type (open, intra-articular, comminution) were the key prognostic factors
- Intramedullary nailing of both bones plus early rehabilitation gave the best results
Fraser Type I Floating Knee: Function and Occult Ligament Injury
- 21 Fraser type I (both diaphyseal) patients after internal fixation of both bones
- Even this 'best' subtype had unsatisfactory function: large isokinetic deficits (61% knee extensor, 37% flexor peak-torque)
- MRI revealed occult ligament/meniscal injury: 3 partial ACL, 1 PCL, 3 meniscal tears
- Four nonunions and two cases of chronic osteomyelitis at follow-up
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Fraser Type I Floating Knee - Single-Stage Fixation
"A 28-year-old motorcyclist is brought to ED after a high-speed collision. He has obvious deformity of his left thigh and leg. X-rays show a mid-shaft femur fracture and a proximal tibial shaft fracture. He is haemodynamically stable. How do you manage this?"
Scenario 2: Fraser Type IIC - Complex Articular Injury
"A 35-year-old construction worker falls 4 meters from scaffolding landing on his left leg. X-rays show a comminuted distal femur fracture and a bicondylar tibial plateau fracture (Schatzker VI pattern). How would you approach this challenging injury?"
Scenario 3: Floating Knee with Popliteal Artery Injury - Limb Salvage
"A 42-year-old presents following a motor vehicle accident with a floating knee injury. His left leg is pale and cool with absent pulses. CT angiography confirms popliteal artery transection. How do you manage this?"
MCQ Practice Points
Clinical Pearl
Q: What is a floating knee injury and what is the Fraser classification?
A: Floating knee: Ipsilateral fractures of the femur and tibia, isolating the knee segment. Fraser classification: Type I: Diaphyseal fractures of both bones (extra-articular). Type IIa: Tibial plateau involvement (intra-articular tibia). Type IIb: Distal femur involvement (intra-articular femur). Type IIc: Both articular surfaces involved. Type II injuries have worse prognosis due to knee joint involvement.
Clinical Pearl
Q: What are the associated injuries to evaluate in floating knee?
A: Vascular injury: Popliteal artery (high risk) - check pulses, ABI, consider CT angiography. Knee ligamentous injury: Up to 50% have ligament damage; Assess after skeletal stabilization. Compartment syndrome: High index of suspicion for both thigh and leg. Soft tissue injury: Open fractures common (30-40%). Systemic trauma: Polytrauma evaluation (head, chest, abdomen) due to high-energy mechanism.
Clinical Pearl
Q: What is the surgical treatment strategy for floating knee injuries?
A: Damage control: Temporizing external fixation if hemodynamically unstable. Definitive fixation: Both fractures fixed when patient optimized. Femur first: Usually IMN for diaphyseal fractures. Tibia: IMN for shaft; Plates for plateau. Same-day fixation of both fractures preferred to allow early knee mobilization. Early motion critical to prevent knee stiffness.
Clinical Pearl
Q: What are the outcomes and complications specific to floating knee injuries?
A: Knee stiffness: Most common complication (20-50%). Malunion/nonunion: Both fracture sites at risk. Infection: Higher rates with open fractures. Vascular injury: Limb-threatening emergency. Long-term outcomes: Return to work only 60-70%. Knee arthrosis: Common in Type II injuries affecting articular surfaces.
Clinical Pearl
Q: When should external fixation be used for floating knee injuries?
A: Indications for temporary external fixation: Damage control orthopaedics - polytrauma, hemodynamic instability; Open fractures with severe contamination awaiting soft tissue healing; Vascular injury requiring restoration of length before vascular repair; Compartment syndrome - provides stability during fasciotomy management; Severe soft tissue swelling precluding safe internal fixation. Conversion to definitive fixation typically within 7-14 days when soft tissue and systemic conditions permit.
Controversies and Areas of Uncertainty
- Is Fraser still fit for purpose? Fraser describes only the bony pattern. A 2024 multicentre study of 168 floating knees found Fraser severity did not reliably predict function, whereas soft-tissue and extensor-mechanism damage did, and proposed a new prognostic system. Fraser remains the lingua franca for exams and communication, but is increasingly seen as prognostically weak.
- Early total care vs damage control. Single-stage fixation in the stable patient is well supported, but the threshold for damage control in the "borderline" physiology patient is debated. The EPOFF biological data favour temporising external fixation in borderline patients, while some high-performing trauma centres report good results with early total care in carefully selected borderline cases.
- Femur-first vs tibia-first. Femur-first (length and alignment) is the common teaching, but no high-level evidence proves superiority; some surgeons fix the simpler or more accessible fracture first, or fix the tibia first to allow knee extension for femoral nailing.
- Routine MRI of the knee. Occult ligament and meniscal injuries are common (and may dominate long-term disability), but the optimal timing and whether routine MRI changes management in the acute setting is unresolved; many units image selectively once the knee can be examined.
- How "best" is the best subtype? Even Fraser type I (both extra-articular) carries large isokinetic strength deficits and unsatisfactory function in some series, challenging the assumption that extra-articular equals good outcome.
Guidelines, Registries & Global Practice
Global Epidemiology
- The floating knee is uncommon, accounting for roughly 2-4% of lower-limb trauma; a contemporary single-centre series reported an incidence of 2.32% of all lower-limb injuries.
- Road traffic and motorcycle trauma dominate the mechanism worldwide; the burden is disproportionately high in low- and middle-income countries with rising motorisation and a young, male-predominant cohort.
- Outcomes are governed less by geography than by soft-tissue status and associated injuries, which are consistent across published series.
Side-by-Side Guideline Framework
| Body / Region | Relevant guidance | Practical emphasis |
|---|---|---|
| AO Foundation (global) | Principles of fracture management; damage control vs early total care | Choice of IM nail vs articular ORIF by fracture pattern |
| BOA / BOAST (UK) | Open fracture and severe lower-limb injury standards | Combined ortho-plastic care, early debridement, soft-tissue cover timing |
| AAOS (US) | Evidence-based polytrauma and femoral shaft guidance | Timely IM nailing in the physiologically stable patient |
| EFORT / European consensus | Polytrauma management and timing of fixation | Physiology-driven (borderline patient) decision-making |
Where these differ, the divergence is mainly on timing (early total care versus damage control) and is reconciled by patient physiology rather than by national preference.
Registry and Trauma-System Notes
- National joint replacement registries (NJR, AJRR, AOANJRR, SHAR, NZJR) capture the downstream burden of post-traumatic arthritis requiring arthroplasty after Fraser type II injuries, but no registry tracks the acute floating knee itself.
- Mature trauma systems with rapid pre-hospital retrieval and Level 1 centres favour single-stage early total care in stable patients; the EPOFF biological data underpin damage control where physiology is borderline.
High- vs Limited-Resource Practice Variation
- High-resource settings: combined ortho-plastic teams, CT angiography on demand, IM nailing of both bones in one sitting, and early MRI of the knee.
- Limited-resource settings: greater reliance on external fixation (limited implants, contaminated open injuries, delayed presentation), staged conversion, and clinical rather than imaging-based vascular assessment. The principle of stabilising both bones to permit early knee motion remains universal.
Floating Knee Quick Reference
Clinical summary
Fraser Classification
- •Type I: Both shafts (extra-articular) - best prognosis
- •Type IIA: Tibia articular (plateau)
- •Type IIB: Femur articular (distal femur)
- •Type IIC: Both articular - worst prognosis
Key Assessment
- •High-energy polytrauma focus
- •Knee ligament injury in 50%+
- •Compartment syndrome - thigh AND leg
- •Popliteal artery at risk
Fixation Order
- •Femur first (restores length/alignment)
- •IM nailing preferred for shafts
- •Anatomic reduction for articular components
- •Damage control if unstable
Complications
- •Knee stiffness (most common)
- •Ligament instability (often occult)
- •Compartment syndrome
- •Infection/Nonunion
References
- Fraser RD, Hunter GA, Waddell JP. Ipsilateral fracture of the femur and tibia. J Bone Joint Surg Br. 1978;60-B(4):510-515.
- Veith RG, Winquist RA, Hansen ST Jr. Ipsilateral fractures of the femur and tibia. J Bone Joint Surg Am. 1984;66(7):991-1002. PMID 6480657.
- Hegazy AM. Surgical management of ipsilateral fracture of the femur and tibia in adults (the floating knee). Clin Orthop Surg. 2011;3(2):133-139. PMID 21629474.
- Andrade-Silva FB, et al. Functional results and isokinetic muscle strength in Fraser type I floating knee. Injury. 2017;48 Suppl 4:S2-S5. PMID 29145963.
- Kenmegne GR, et al. The current issues and challenges in the management of floating knee injury. Front Surg. 2023;10:1164032. PMID 37206352.
- Pape HC, et al. (EPOFF Study Group). Impact of intramedullary instrumentation versus damage control for femoral fractures on immunoinflammatory parameters. J Trauma. 2003;55(1):7-13. PMID 12855874.
- Chouhan D, et al. Comparison of functional outcomes among subtypes of Fraser's type II floating knee. Chin J Traumatol. 2020;24(1):25-29. PMID 33339679.
- Meccariello L, et al. Floating knee: a new prognostic classification. Injury. 2024;55 Suppl 4:111471. PMID 39542575.